
Chronic Olfactory Dysfunction in Children with Long COVID: A Retrospective Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Statistical Analysis
2.3. Ethics Statement
3. Results
3.1. Characteristics of the Population
3.2. Families’ Voices
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, E.A. The immunology and immunopathology of COVID-19. Science 1127, 375, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021, 110, 2208–2211. [Google Scholar] [CrossRef] [PubMed]
- Roge, I.; Smane, L.; Kivite-Urtane, A.; Pucuka, Z.; Racko, I.; Klavina, L.; Pavare, J. Comparison of Persistent Symptoms after COVID-19 and Other Non-SARS-CoV-2 Infections in Children. Front. Pediatr. 2021, 9, 752385. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, E.J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Stephenson, T.; Allin, B.; Nugawela, M.D.; Rojas, N.; Dalrymple, E.; Pinto Pereira, S.; Soni, M.; Knight, M.; Cheung, E.Y.; Heyman, I.; et al. Long COVID (post-COVID-19 condition) in children: A modified Delphi process. Arch. Dis. Child 2022, 107. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Surda, P.; Vaira, L.A.; Lechien, J.R.; Safarian, M.; Saussez, S.; Kumar, N. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinol. J. 2020, 59, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Boscolo-Rizzo, P.; Guida, F.; Polesel, J.; Marcuzzo, A.V.; Antonucci, P.; Capriotti, V.; Sacchet, E.; Cragnolini, F.; D’Alessandro, A.; Zanelli, E.; et al. Self-reported smell and taste recovery in coronavirus disease 2019 patients: A one-year prospective study. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Zazhytska, M.; Kodra, A.; Hoagland, D.A.; Frere, J.; Fullard, J.F.; Shayya, H.; McArthur, N.G.; Moeller, R.; Uhl, S.; Omer, A.D.; et al. Non-cell-autonomous disruption of nuclear architecture as a potential cause of COVID-19-induced anosmia. Cell 2022, 185, 1052–1064.e12. [Google Scholar] [CrossRef] [PubMed]
- Keshavarz, P.; Haseli, S.; Yazdanpanah, F.; Bagheri, F.; Raygani, N.; Karimi-Galougahi, e.M. A Systematic Review of Imaging Studies in Olfactory Dysfunction Secondary to COVID-19. Acad. Radiol. 2021, 28, 1530–1540. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Yousefi-Koma, A.; Bakhshayeshkaram, M.; Raad, N.; Haseli, e.S. (18)FDG PET/CT Scan Reveals Hypoactive Orbitofrontal Cortex in Anosmia of COVID-19. Acad. Radiol. 1043, 27, 1042–1043. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.J.; Yu, A.C.; Lee, e.J.T. Management of post-COVID-19 olfactory dysfunction. Curr. Treat. Options Allergy 2022, 9, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Parri, N.; de Rose, C.; Valentini, e.P. Toward a clinically based classification of disease severity for paediatric COVID-19. Lancet Infect. Dis. 2021, 21, 22. [Google Scholar] [CrossRef]
- Elvan-Tuz, A.; Karadag-Oncel, E.; Kiran, S.; Kanik-Yuksek, S.; Gulhan, B.; Hacimustafaoglu, M.; Ozdem-Alatas, S.; Kuyucu, N.; Ozdemir, H.; Egil, O.; et al. Prevalence of Anosmia in 10.157 Pediatric COVID-19 Cases: Multicenter Study from Turkey. Pediatr. Infect. Dis. J. 2022, 41, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Resendiz, K.J.G.; Benitez-Trinidad, A.B.; Covantes-Rosales, C.E.; Toledo-Ibarra, G.A.; Ortiz-Lazareno, P.C.; Girón-Pérez, D.A.; Bueno-Durán, A.Y.; Pérez-Díaz, D.A.; Barcelos-García, R.G.; Girón-Pérez, M.I. Loss of mitochondrial membrane potential (Δ Ψ m ) in leucocytes as post-COVID-19 sequelae. J. Leukoc. Biol. 2022, 112, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Di Gennaro, L.; De Rose, C.; Morello, R.; D’Ilario, F.; Zampino, G.; Piazza, M.; Boner, A.L.; Iraci, C.; O’Connell, S.; et al. Long-term outcomes of pediatric infections: From traditional infectious diseases to long Covid. Future Microbiol. 2022, 17, 551–571. [Google Scholar] [CrossRef] [PubMed]
- Long COVID and kids: More research is urgently needed. Nature 2022, 602, 183. [CrossRef] [PubMed]
- Tan, B.K.J.; Han, R.; Zhao, J.J.; Tan, N.K.W.; Quah, E.S.H.; Tan, C.J.; Chan, Y.H.; Teo, N.W.Y.; Charn, T.C.; See, A.; et al. Prognosis and persistence of smell and taste dysfunction in patients with covid-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022, 378, e069503. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef] [PubMed]
- Printza, A.; Katotomichelakis, M.; Valsamidis, K.; Metallidis, S.; Panagopoulos, P.; Panopoulou, M.; Petrakis, V.; Con-stantinidis, J. Smell and Taste Loss Recovery Time in COVID-19 Patients and Disease Severity. J. Clin. Med. 2021, 10, 966. [Google Scholar] [CrossRef] [PubMed]
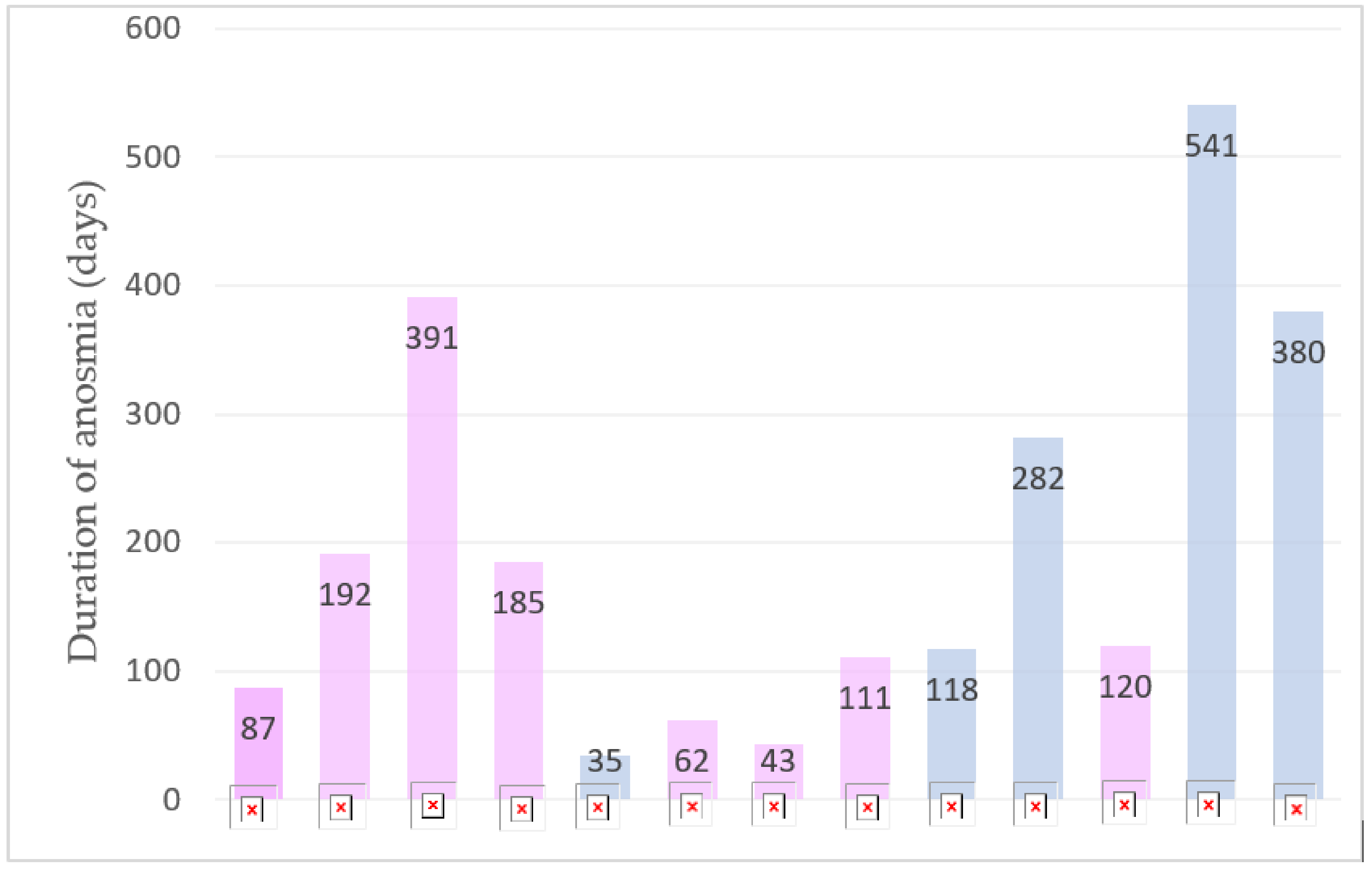
 : It’s the patient number, 1-2-3-4 etc.
: It’s the patient number, 1-2-3-4 etc.

{kind=link}
| Children aged 0–18 years |
| The child sought/needed primary or secondary medical care for COVID-19 |
| Laboratory (RT-PCR) diagnosis of acute COVID-19 |
| At least 28 days from the onset of COVID-19 symptoms |
| Parent’s/carer’s/guardian’s consent to participate |
| 1 | When was your child diagnosed with SARS-CoV-2 infection? |
| 2 | Did your child report smell disorders? If yes, since when? |
| 3 | Did your child report taste disorders? If yes, since when? |
| 4 | If your child had smell disorders, how long did they last? |
| 5 | If your child had taste disorders, how long did they last? |
| 6 | Could you tell us how your child describes smell and taste disorders? |
| 7 | Could you tell us how these disorders impact on your child’s daily routine? |
| 8 | As a parent, do these disorders impact on your daily routine or mood, too? If yes, describe us some examples. |
| 9 | As a parent, what do you expect from the scientific community and media about these problems? |
| All | Persistent Anosmia | Non-Persistent Anosmia | p Value | |
|---|---|---|---|---|
| N (%) | 784 (100) | 13 (1.7) | 771 (98.3) | |
| Age at first SARS-CoV-2 infection (years) N (%) | ||||
| 0–9 years | 530 (67.6) | 1 (7.7) | 529 (68.6) | |
| 10–18 years | 254 (32.4) | 12 (92.3) | 242 (31.4) | |
| Median age (years) IQR | 7.99 4.6–10.8 | 13.86 11.6–14.5 | 7.83 4.55–10.7 | <0.05 |
| Gender N (%) | 0.24 | |||
| Male | 427 (54.5) | 5 (38.5) | 422 (54.7) | |
| Female | 357 (45.5) | 8 (61.5) | 349 (45.3) | |
| Nationality N (%) | <0.05 | |||
| Italy | 778 (99.2) | 12 (92.3) | 766 (99.4) | |
| Other countries | 6 (0.8) | 1 (7.7) | 5 (0.6) | |
| COVID-19 Vaccination status N (%) | 0.78 | |||
| Non vaccinated | 648 (82.7) | 10 (76.9) | 638 (82.7) | |
| Vaccinated with 1 dose | 56 (7.1) | 1 (7.7) | 55 (7.1) | |
| Fully vaccinated | 73 (9.3) | 2 (15.4) | 71 (9.2) | |
| Vaccinated with booster dose | 7 (0.9) | 0 (0) | 7 (0.9) | |
| Comorbidities N (%) | 0.18 | |||
| Yes | 89 (11.4) | 3 (23.1) | 86 (11.2) | |
| No | 695 (88.6) | 10 (76.9) | 685 (88.8) | |
| Allergic Asthma | 15 (1.9) | 1 (7.7) | 14 (1.8) | |
| Asthmatic Bronchitis | 15 (1.9) | 0 | 15 (1.9) | |
| Autism Spectrum disorders | 12 (1.5) | 0 | 12 (1.6) | |
| Allergies | 8 (1.0) | 2 (15.3) | 6 (0.8) | |
| Atopic dermatitis | 8 (1.0) | 0 | 8 (1.0) | |
| Adenotonsillar hypertrophy | 5 (0.6) | 0 | 5 (0.6) | |
| Recurrent respiratory infections | 4 (0.5) | 0 | 4 (0.5) | |
| Prematurity | 4 (0.5) | 0 | 4 (0.5) | |
| Gastroesophageal reflux | 2 (0.3) | 0 | 2 (0.3) | |
| Celiac disease | 2 (0.3) | 0 | 2 (0.3) | |
| Epilepsy | 2 (0.3) | 0 | 2 (0.3) | |
| Migraine | 2 (0.3) | 0 | 2 (0.3) | |
| D. Duchenne | 2 (0.3) | 0 | 2 (0.3) | |
| Henoch–Schonlein Purpura | 2 (0.3) | 0 | 2 (0.3) | |
| Obesity | 2 (0.3) | 0 | 2 (0.3) | |
| Down syndrome | 2 (0.3) | 0 | 2 (0.3) | |
| Noonan syndrome | 1 (0.1) | 0 | 1 (0.1) | |
| Klinefelter syndrome | 1 (0.1) | 0 | 1 (0.1) | |
| Turner syndrome | 1 (0.1) | 0 | 1 (0.1) | |
| Arnold–Chiari malformation | 1 (0.1) | 0 | 1 (0.1) | |
| Charcot–Marie–Tooth syndrome | 1 (0.1) | 0 | 1 (0.1) | |
| Primary ciliary dyskinesia | 1 (0.1) | 0 | 1 (0.1) | |
| Solitary kidney | 1 (0.1) | 0 | 1 (0.1) | |
| No comorbidities | 690 (88.0) | 10 (77.0) | 680 (88.2) | |
| Acute disease severity N (%) | 0.78 | |||
| Asymptomatic | 39 (5.0) | 0 | 39 (5.1) | |
| Mild | 724 (92.3) | 13 (100) | 711 (92.2) | |
| Moderate | 19 (2.4) | 0 | 19 (2.5) | |
| Severe- MISC | 2 (0.3) | 0 | 2 (0.3) | |
| Hospital admission N (%) | 0.33 | |||
| Yes | 24 (3.1) | 1 (7.7) | 23 (3.0) | |
| No | 760 (96.9) | 12 (92.3) | 748 (97.0) | |
| PICU admission N(%) | 0.79 | |||
| Yes | 4 (0.5) | 0 | 4 (0.5) | |
| No | 780 (99.5) | 13 (100) | 767 (99.5) | |
| FUP | ||||
| Mean (days) IQR | 106.9 61–120 | 132.0 62–185 | 106.7 61–119 | 0.43 |
| Post-acute infection symptoms | ||||
| Yes | 287 (36.6) | 13 (100) | 274 (35.5) | |
| No | 497 (63.4) | 0 | 497 (64.5) | |
| Fever | 11 (1.4) | 0 | 11 (1.4) | 0.66 |
| Nasal congestion/rhinorrhea | 25 (3.2) | 1 (7.7) | 24 (3.1) | 0.35 |
| Altered taste | 11 (1.4) | 7 (53.8) | 4 (0.5) | <0.05 |
| Cough | 33 (4.2) | 1 (7.7) | 32 (4.2) | 0.528 |
| Dyspnea at rest | 7 (0.9) | 1 (7.7) | 6 (0.8) | <0.05 |
| Dyspnea on exertion | 66 (8.4) | 6 (46.2) | 60 (7.8) | <0.05 |
| Asthma | 10 (1.3) | 0 | 10 (1.3) | 0.68 |
| Chest pain | 33 (4.2) | 1 (7.7) | 32 (4.2) | <0.05 |
| Palpitations | 21 (2.7) | 2 (15.4) | 19 (2.5) | <0.05 |
| Joint pain | 35 (4.5) | 3 (15.4) | 32 (4.2) | <0.05 |
| Muscle pain | 50 (6.4) | 2 (15.4) | 48 (6.2) | 0.18 |
| Headache | 72 (9.2) | 3 (23.1) | 69 (8.9) | 0.08 |
| Asthenia | 107 (13.6) | 3 (23.1) | 104 (13.5) | 0.32 |
| Gastrointestinal symptoms | 48 (6.1) | 1 (7.7) | 47 (6.1) | 0.81 |
| Rash | 18 (2.3) | 1 (7.7) | 17 (2.2) | 0.19 |
| Other: yes | 75 (9.6) | 3 (23.1) | 72 (9.3) | 0.09 |
| Patient 1 | Anosmia, dyspnea on exertion, chest pain, palpitations, joint pain, rash. |
| Patient 2 | Anosmia, altered taste, asthenia. |
| Patient 3 | Anosmia, altered taste, dyspnea on exertion, palpitations. |
| Patient 4 | Anosmia, concentration and memory disorders. |
| Patient 5 | Anosmia, altered taste, joint and muscle pain, headache, gastrointestinal symptoms, asthenia. |
| Patient 6 | Anosmia, dyspnea on exertion. |
| Patient 7 | Anosmia, nasal congestion, dyspnea on exertion, muscle pain, asthenia. |
| Patient 8 | Anosmia and altered taste. |
| Patient 9 | Anosmia and altered taste. |
| Patient 10 | Anosmia and altered taste. |
| Patient 11 | Anosmia, altered taste, cough, dyspnea on exertion, headache. |
| Patient 12 | Anosmia. |
| Patient 13 | Anosmia, dyspnea at rest, dyspnea on exertion, chest pains, joint pain, headache, altered sleep–wake rhythm. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buonsenso, D.; Martino, L.; Morello, R.; De Rose, C.; Valentini, P. Chronic Olfactory Dysfunction in Children with Long COVID: A Retrospective Study. Children 2022, 9, 1251. https://doi.org/10.3390/children9081251
Buonsenso D, Martino L, Morello R, De Rose C, Valentini P. Chronic Olfactory Dysfunction in Children with Long COVID: A Retrospective Study. Children. 2022; 9(8):1251. https://doi.org/10.3390/children9081251
Chicago/Turabian StyleBuonsenso, Danilo, Laura Martino, Rosa Morello, Cristina De Rose, and Piero Valentini. 2022. "Chronic Olfactory Dysfunction in Children with Long COVID: A Retrospective Study" Children 9, no. 8: 1251. https://doi.org/10.3390/children9081251
APA StyleBuonsenso, D., Martino, L., Morello, R., De Rose, C., & Valentini, P. (2022). Chronic Olfactory Dysfunction in Children with Long COVID: A Retrospective Study. Children, 9(8), 1251. https://doi.org/10.3390/children9081251