
A Self-Adaptive and Efficient Context-Aware Healthcare Model for COPD Diseases



Abstract
:1. Introduction
2. Context Awareness and Self-Adaptive Systems
2.1. Background
2.2. Self-Adaptation Frameworks
2.2.1. FUSION
2.2.2. CASA
- the CASA framework, an integrated framework to develop adaptive applications;
- CASA runtime, which provides resource awareness and dynamic adaptability to applications in a transparent way.
2.2.3. SSOA
- Parametric adaptation, which modifies the value of an existing parameter or service;
- Functional adaptation, which replaces one function implementation with another, leaving the interfaces unchanged;
- Behavioural adaptation, which changes how a service acts and possibly its interface;
- Structural adaptation, which modifies the composition of services inside an application;
- Environmental adaptation, which allows the outside world of the application to be changed (service migration).
- Single service;
- Composition of services in one application;
- Several applications running on heterogeneous service-oriented platforms.
2.2.4. CAreDroid
2.2.5. Self-OSGi
- The belief model, which describes information about the environment and internal state;
- The goal model, which describes the goals an agent may have and how these goals can be achieved;
- The plan model, which describes the plan available to the agent for the purpose of achieving its goals.
2.2.6. Dynamic Pervasive Healthcare System for COPD
2.3. Limitations of Adaptation Frameworks
3. System Requirements and Self-Adaptation Characteristics and Taxonomy
3.1. Requirements Extraction and Gathering
- Where: Determines where the change needs to be implemented;
- When: Addresses temporal aspects of change;
- What: Identifies what attributes or artifacts of the system can be changed through adaptation actions and what needs to be changed in each situation;
- Why: Deals with the motivations for building a self-adaptive software application;
- Who: Addresses the level of automation and human involvement in self-adaptive software;
- How: Determines how adaptable artifacts can be changed and which adaptation action(s) are appropriate for application in a given condition.
3.2. Adaptation Characteristics and Taxonomy
3.2.1. Time
3.2.2. Reason
3.2.3. Level
3.2.4. Technique
3.2.5. Adaptation Control
- Monitor: The monitoring phase extracts information—i.e., properties or states—from the managed element.
- Analyze: This phase determines whether something has gone wrong in the system, usually because a system property exhibited a value outside of expected bounds or has a degrading trend.
- Plan: This stage determines a set of actions to adapt the managed element when a problem is detected.
- Execute: This phase applies a chosen set of actions to effect changes in the system.
4. Self-Adaptive Healthcare System for COPD
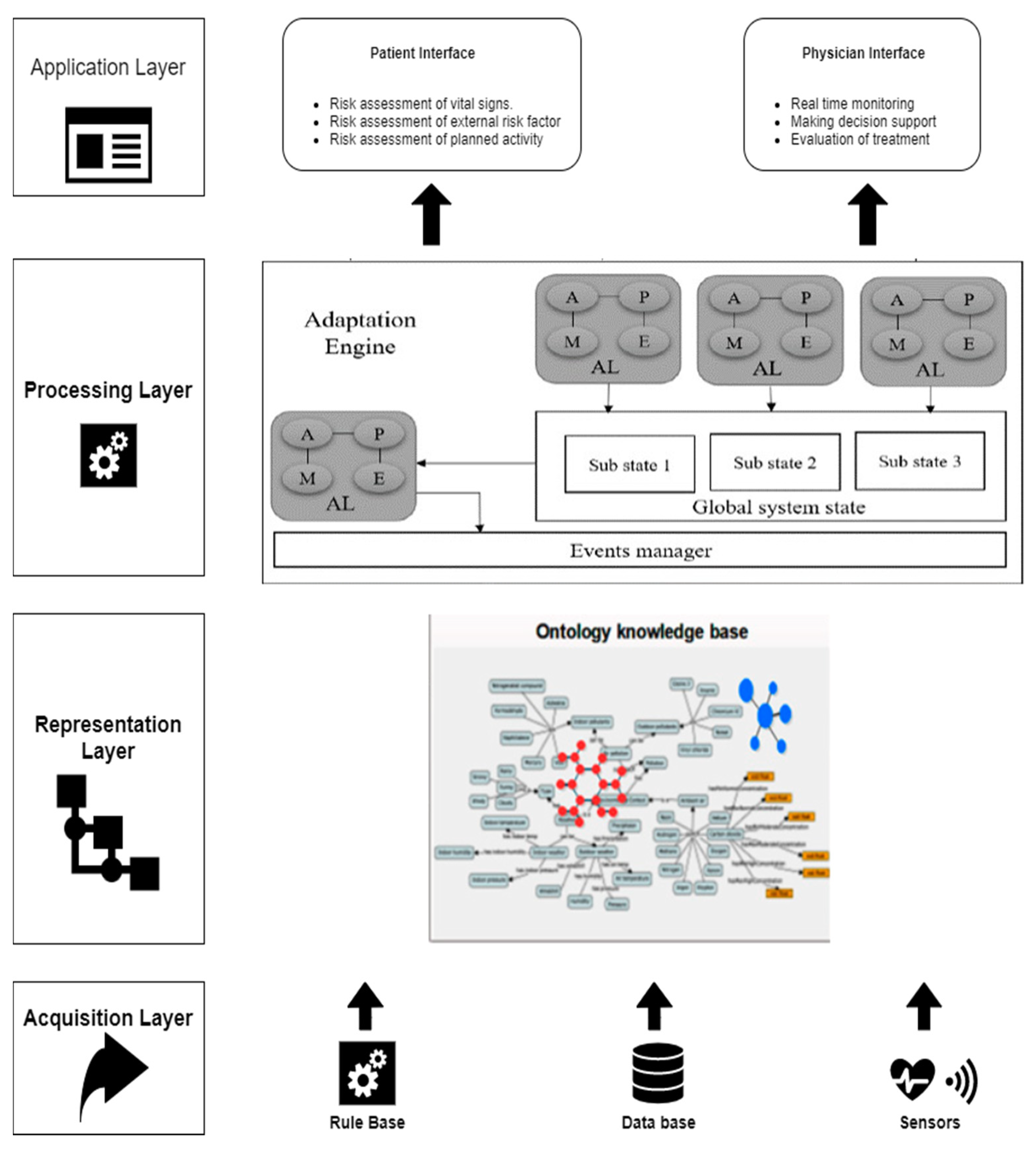
4.1. Pervasive Healthcare System for COPD Patients
- In the acquisition layer, different sorts of data—such as the medical profiles of COPD patients, biomarkers and environmental information—are collected and transmitted from monitoring sensors and wearable devices.
- The semantic layer translates the real context of the patient into machine-understandable and accessible language.
- The processing layer aims to detect all possible hazardous events that could influence the COPD patient. In the healthcare system, we provided rules expressed in SWRL to describe all implications and consequences. These rules are used by an inference engine to derive new facts, detect events and predict potential risk factors.
- The application layer is divided into two parts (a patient interface and a physician interface). Each part provides a set of functionalities and services related to the patient health state, risk assessment for vital signs and external risk factors, and many more.
- The end user application should provide needed services for both patient and physician, such as:
- Alerting both the patient and physician to any exacerbation of vital signs (body temperature, blood pressure, heart rate, partial pressure oxygen [PaO2], oxygen saturation [SpO2], partial pressure carbon dioxide [PaCO2], oxygen consumption [VO2], respiration rate, blood pH, bicarbonate [HCO3] and FEV1);
- Providing recommendations and alerts to the patient related to conditions in the external surrounding environment and the patient’s physical activities (e.g., warning the patient when the weather temperature and humidity exceed a certain range for a long duration; suggesting that the patient stop a certain physical activity, like walking, when their biomarkers indicate an abnormal situation);
- Continuously adapting the acceptable ranges for patient biomarkers and external conditions;
- When a grave situation is detected, alerting emergency personnel or informing both the patient and physician about the need for an urgent appointment.
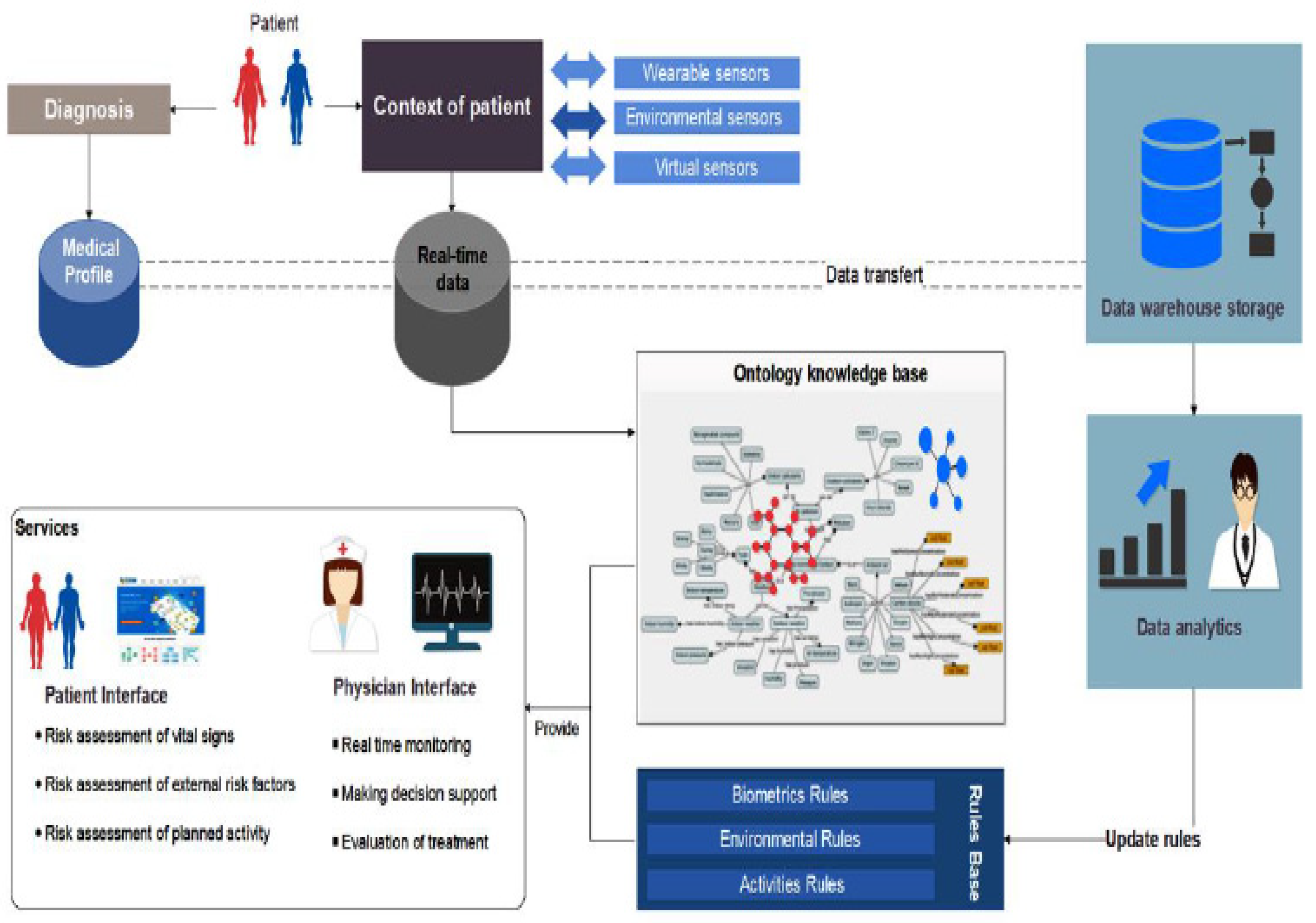
- The data sources (sensors and patient records) provide a continuous stream of contextual data and historical data about the patient.
- The rule base serves as the knowledge base for our system. These rules (20,308 rules) are generated and identified based on the literature of COPD diseases and validated by 20 physicians to verify the profile of patients, detect their location, evaluate the status of patients and offer the recommendation services [12].
4.2. Adaptation Approach
4.3. Adaptation Life Cycle
- Single source of truth: The system state is the only place in the system where the data are stored, and any system component that needs to read those data or receive the latest updates must be listening to it. In addition, any update in the data is directly reflected in the state.
- One-way data flow: There is one and only one way for data to be transferred to other parts of the system. This means that system units cannot directly send changes to each other. In addition, one system component cannot directly call any function or modify any variable in another component.
- One way to change the state: The data stored in the system state can be changed only by using predefined functions called “actions.” Therefore, no individual system component can immediately update the state. For example, if it were necessary to update the safe range for outdoor temperature, the system would need to use the predefined action “updateOutdoorTemperatureSafeRange”.
4.4. Decentralization and Separation of Concerns
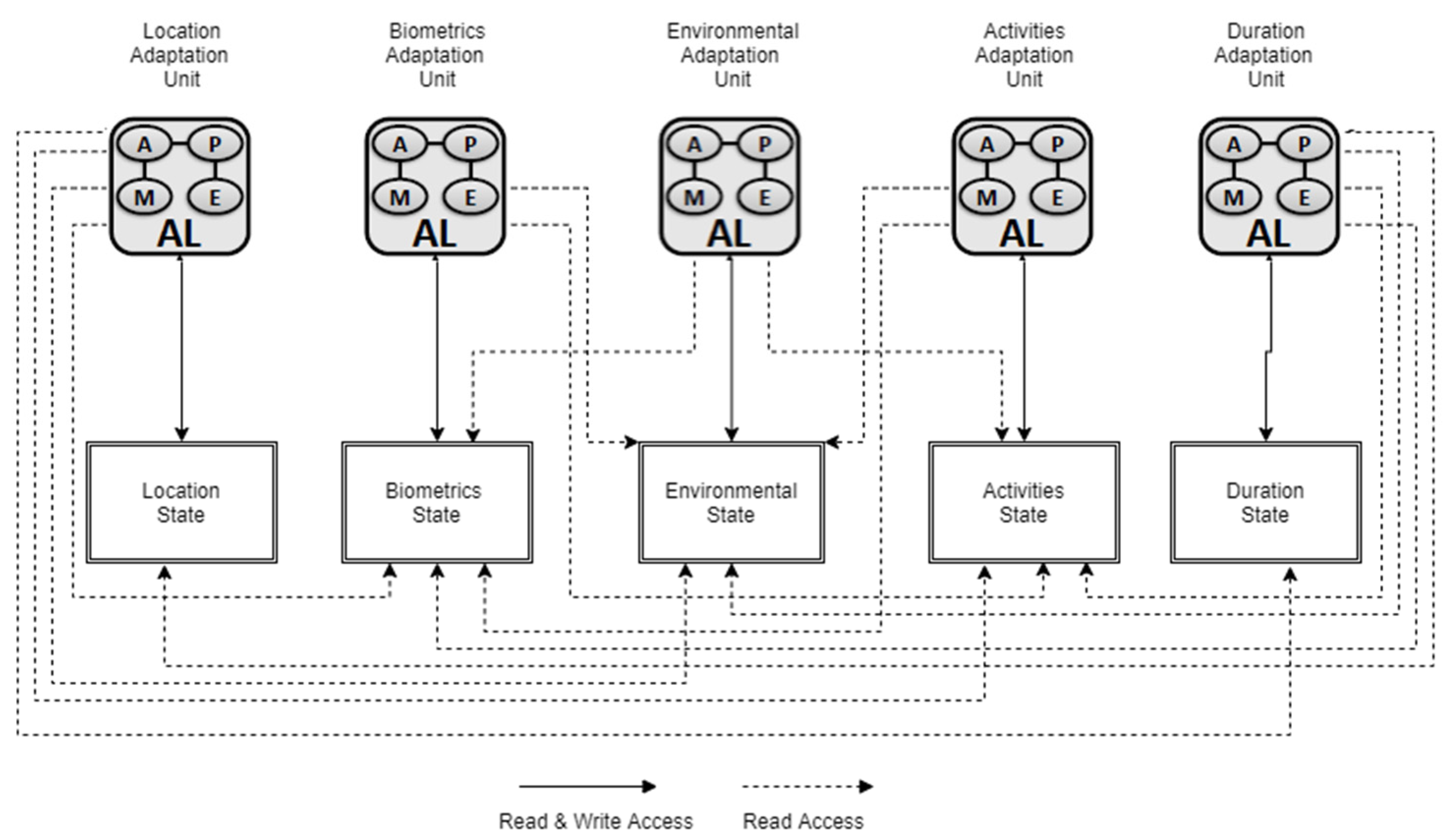
- Multiple adaptation units: Each unit is responsible for handling the monitoring process for a specific type of contextual data and updating a set of system parameters associated with the same type of monitored data.
- Shared memory unit: This unit, called the global state, consists of multiple substates, each of which saves system parameters, such as environmental and biometrics safe ranges, as well as functional parameters, which are responsible for triggering services.
- Central adaptation unit: This unit is responsible for monitoring the updated system parameters saved in the global state and triggering the required services accordingly.
4.5. Adaptation Engine and Monitoring Units
- Biometrics unit;
- Environmental unit;
- Activities unit;
- Location unit;
- Duration unit (time unit).
5. Validation of Adaptation Model’s Performance
5.1. Implementation and Tools
5.1.1. Rules Engine Implementation
5.1.2. State Units Implementation
5.2. Case Scenarios for Understanding the Separation of Units and the Efficient Execution of the Subset of Rules Based on Changed Attributes
5.3. Results and Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 3 June 2017).
- Chronic Respiratory Diseases. Available online: www.who.int/respiratory (accessed on 15 July 2018).
- Casas, A.; Troosters, T.; Garcia-Aymerich, J.; Roca, J.; Hernández, C.; Alonso, A.; del Pozo, F.; de Toledo, P.; Antó, J.M.; Rodríguez-Roisín, R.; et al. Integrated care prevents hospitalisations for exacerbations in COPD patients. Eur. Respir. J. 2006, 28, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Strategy for the Diagnosis Management and Prevention of COPD. Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2011. Available online: http://www.goldcopd.org/ (accessed on 13 January 2021).
- McKinstry, B. The use of remote monitoring technologies in managing chronic obstructive pulmonary disease. QJM 2013. [Google Scholar] [CrossRef] [PubMed]
- Bolton, C.E.; Waters, C.S.; Peirce, S.; Elwyn, G. Insufficient evidence of benefit: A systematic review of home telemonitoring for COPD. J. Eval. Clin. Pract. 2010, 17, 1216–1222. [Google Scholar] [CrossRef]
- Polisena, J.; Tran, K.; Cimon, K.; Hutton, B.; McGill, S.; Palmer, K.; Scott, R.E. Home telehealth for chronic obstructive pulmonary disease: A systematic review and meta-analysis. J. Telemed. Telecare 2010, 16, 120–127. [Google Scholar] [CrossRef]
- Jaana, M.; Pare, G.; Sicotte, C. Home telemonitoring forrespiratory conditions: A systematic review. Am. J. Manag. Care 2009, 15, 313–320. [Google Scholar] [PubMed]
- Bartoli, L.; Zanaboni, P.; Masella, C.; Ursini, N. Systematicreview of telemedicine services for patients affected by Chronic Obstructive Pulmonary Disease (COPD). Telemed. J. E-Health 2009, 15, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Mcheick, H.; Saleh, L.; Ajami, H.; Mili, H. Context Relevant Prediction Model for COPD Domain Using Bayesian Belief Network. Sensors 2017, 17, 1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajami, H.; Mcheick, H. Ontology-Based Model to Support Ubiquitous Healthcare Systems for COPD Patients. Electronics 2018, 7, 371. [Google Scholar] [CrossRef] [Green Version]
- Ajami, H.; Mcheick, H.; Mustapha, K. A Pervasive Healthcare System for COPD Patients. Diagnostics 2019, 9, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ajami, H.; Mcheick, H.; Mustapha, K. Ubiquitous Healthcare Systems and Medical Rules in COPD Domain. In How AI Impacts Urban Living and Public Health ICOST 2019. Lecture Notes in Computer Science; Pagán, J., Mokhtari, M., Aloulou, H., Abdulrazak, B., Cabrera, M., Eds.; Springer: Cham, Switzerland, 2019; Volume 11862. [Google Scholar]
- Krupitzer, C.; Roth, F.M.; VanSyckel, S.; Schiele, G.; Becker, C. A survey on engineering approaches for self-adaptive systems. Pervasive Mob. Comput. J. 2015, 17 Pt B, 184–206. [Google Scholar] [CrossRef]
- Oreizy, P.; Gorlick, M.M.; Taylor, R.N.; Heimhigner, D.; Johnson, G.; Medvidovic, N.; Quilici, A.; Rosenblum, D.S.; Wolf, A.L. An Architecture-Based Approach to Self-Adaptive Software. IEEE Intell. Syst. 1999, 14, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Elkhodary, A.; Esfahani, N.; Malek, S. FUSION: A Framework for Engineering Self-tuning Self-adaptive Software Systems. In Proceedings of the Eighteenth ACM SIGSOFT International Symposium on Foundations of Software Engineering, Santa Fe, NM, USA, 7–11 November 2010; pp. 7–14. [Google Scholar]
- Mukhija, A.; Glinz, M. CASA A Contract-based Adaptive Software Architecture Framework. In Proceedings of the 3rd IEEE Workshop on Applications and Services in Wireless Networks (ASWN 2003), Berne, Switzerland, 2–4 July 2003; pp. 275–286. [Google Scholar]
- André, F.; Daubert, E.; Gauvrit, G. Towards a Generic Context-Aware Framework for Self-Adaptation of Service-Oriented Architectures. In Proceedings of the Fifth International Conference on Internet and Web Applications and Services, Barcelona, Spain, 9–15 May 2010; pp. 309–314. [Google Scholar]
- Elmalaki, S.; Wanner, L.; Srivastava, M. CAreDroid: Adaptation Framework for Android Context-Aware Applications. In Proceedings of the 21st Annual International Conference on Mobile Computing and Networking, Paris, France, 7–11 September 2015. [Google Scholar]
- Dragone, M. Building Self-adaptive Software Systems with Component, Services & Agents Technologies: Self-OSGi. In International Conference on Agents and Artificial Intelligence; Springer: Berlin/Heidelberg, Germany, 2013; Volume 358, pp. 300–316. [Google Scholar] [CrossRef]
- Mukabunani, A. Ontology-Based Clinical Decision Support System Applied on Diabetes. Master’s Thesis, University of Agder, Kristiansand, Norway, 2017. [Google Scholar]
- Humphries, S.M.; Notary, A.M.; Centeno, J.P.; Strand, M.J.; Crapo, J.D.; Silverman, E.K.; Genetic Epidemiology of COPD (COPDGene) Investigators. DL enables automatic classification of emphysema pattern at CT. Radiology 2020, 294, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Ying, J.; Dutta, J.; Guo, N.; Hu, C.; Zhou, D.; Sitek, A.; Li, Q. Classification of Exacerbation Frequency in the COPD Gene Cohort Using DL with Deep Belief Networks. IEEE J. Biomed. Health Inform. 2020, 24, 1805–1813. [Google Scholar] [CrossRef] [PubMed]
- Gaasbeek, J.R.; Martin, J.N. Getting to Requirements: The W5H Challenge. In Proceedings of the 11th International Symposium of the International Council on Systems Engineering, Tel Aviv-Yafo, Israel, 16–17 March 2001. [Google Scholar]
- Handte, M.; Schiele, G.; Matjuntke, V.; Becker, C.; Marrón, P.J. 3PC: System Support for Adaptive Peer-to-Peer Pervasive Computing. ACM Trans. Auton. Adapt. Syst. 2012, 7, 1–19. [Google Scholar] [CrossRef]
- Lieberman, H.; Selker, T. Out of context: Computer systems that adapt to, and learn from, context. IBM Syst. J. 2000, 39, 617–632. [Google Scholar] [CrossRef]
- McKinley, P.K.; Sadjadi, S.M.; Kasten, E.P.; Cheng, B.H. Composing Adaptive Software. IEEE Comput. 2004, 37, 56–64. [Google Scholar] [CrossRef]
- IBM. An Architectural Blueprint for Autonomic Computing; IBM: Armonk, NY, USA, 2004. [Google Scholar]
- Redux Fundamentals, Part 2: Concepts and Data Flow. Available online: https://redux.js.org/basics/data-flow (accessed on 8 May 2021).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Context Requirement | Description |
|---|---|
| Where | Where do we need to make a change inside our system when a context changes? In the model presented by Ajami and Mcheick [11], change needs to take place in the application layer on both sides: user interface and physician interface. |
| When | When do we need to make these changes? Changes should take place whenever an urgent update occurs in user contextual data, such as vital signs, environmental risk factors and planned activities, or periodical changes, such as treatment evaluation and decision support suggestions. |
| What | What do we need to change? We need to update some system attributes that present the system state. These attributes could in turn trigger new functions or activate new components. |
| Why | Why are these changes required? In healthcare monitoring applications, especially these related to chronic diseases, taking preventive action is a crucial component of treatment plans. In addition, the ability to notify the patient and medical experts about any threatening situation or abnormal signs makes these applications more efficient. |
| Who | Is any human intervention required in the adaptation process? On the patient side, all biomedical data and surrounding environmental data are collected from sensors. However, because physical activities affect COPD patients’ states, patients need to be able to specify their planned physical activity (e.g., running, swimming) and the system needs to be able to detect these activities. |
| How | How should we determine what changes and actions are needed in the adaptation process? Ajami and Mcheick [11] provided a rule-based reasoning engine. All required actions and changes can be deduced based on these generated rules. |
| Biometrics | Environmental | Activities | Location | Duration | |
|---|---|---|---|---|---|
| Data | Biometrics Data | Environmental Data | Activities Data | Location Data | Duration Data |
| Rules | Biometrics Rules | Environmental Rules | Activities Rules | Location Rules | Duration Rules |
| Services | Biometrics Services | Environmental Services | Activities Services | Location Services | Duration Services |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mcheick, H.; Sayegh, J. A Self-Adaptive and Efficient Context-Aware Healthcare Model for COPD Diseases. Informatics 2021, 8, 41. https://doi.org/10.3390/informatics8030041
Mcheick H, Sayegh J. A Self-Adaptive and Efficient Context-Aware Healthcare Model for COPD Diseases. Informatics. 2021; 8(3):41. https://doi.org/10.3390/informatics8030041
Chicago/Turabian StyleMcheick, Hamid, and John Sayegh. 2021. "A Self-Adaptive and Efficient Context-Aware Healthcare Model for COPD Diseases" Informatics 8, no. 3: 41. https://doi.org/10.3390/informatics8030041
APA StyleMcheick, H., & Sayegh, J. (2021). A Self-Adaptive and Efficient Context-Aware Healthcare Model for COPD Diseases. Informatics, 8(3), 41. https://doi.org/10.3390/informatics8030041