




Influence of Concurrent Exercise Training on Ankle Muscle Activation during Static and Proactive Postural Control on Older Adults with Sarcopenic Obesity: A Multicenter, Randomized, and Controlled Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
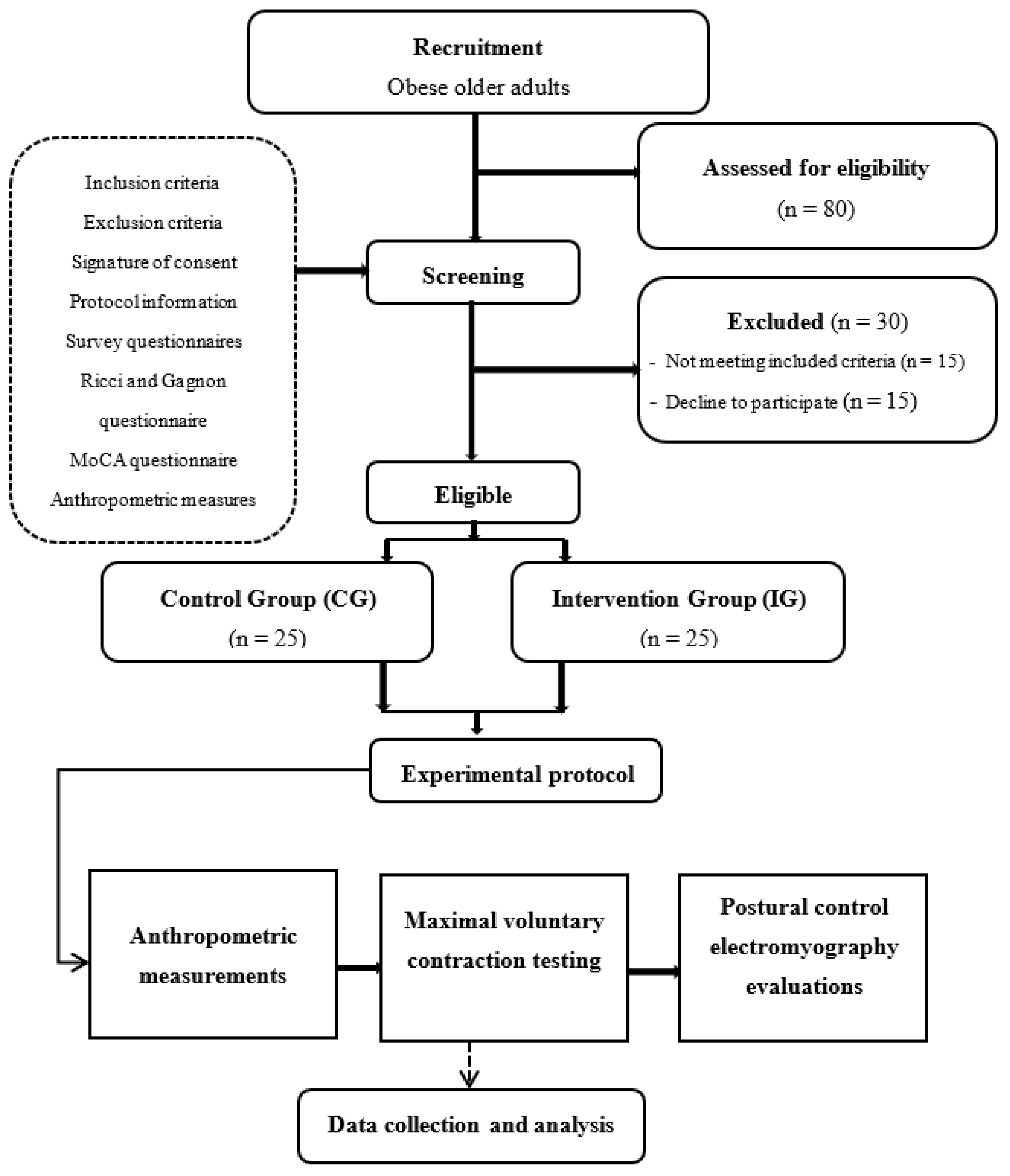
2.1. Experimental Design
2.2. Recruitment and Randomization
2.3. Intervention Program
2.4. Outcomes Measures
2.4.1. Steady-State and Proactive Postural Control
2.4.2. Anthropometric Measurement
2.4.3. Maximal Voluntary Contraction Testing Measurement
2.4.4. Postural Control Evaluation
2.4.5. Electromyography Evaluation
2.5. Statistical Analysis
2.5.1. Sample Size
2.5.2. Statistical Procedures
3. Results
3.1. Participants
3.2. Anthropometric Parameters
3.3. Maximal Voluntary Contraction Testing
3.4. Postural Control Evaluation
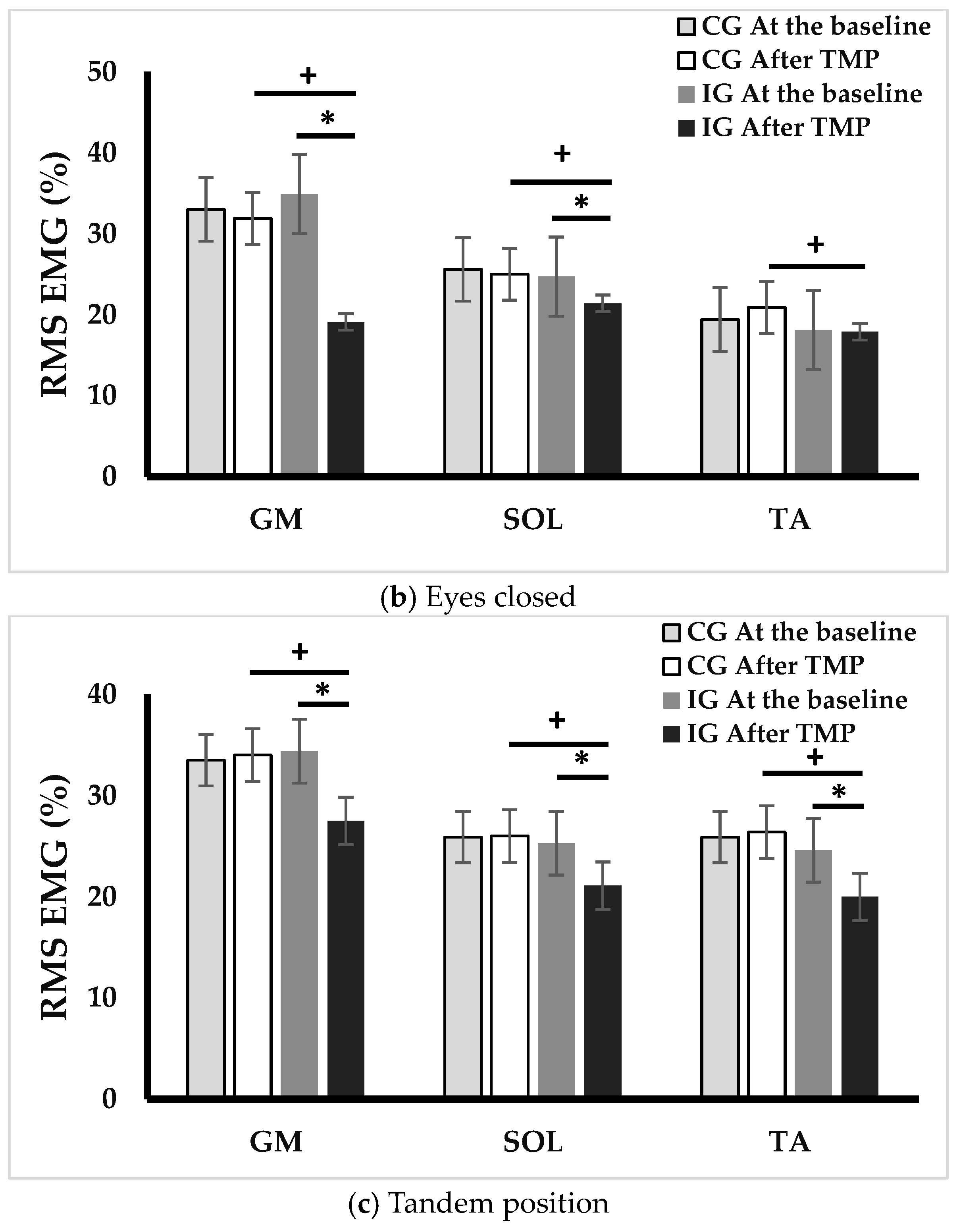
3.5. Electromyography Evaluation
3.6. Pearson’s Correlation Analysis
4. Discussion
Limitations and Perspectives
5. Conclusions
6. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; Jiménez-García, J.D.; Achalandabaso, A.; Sánchez-Montesinos, I.; de la Torre-Cruz, M.; Hita-Contreras, F. Sarcopenia and Sarcopenic Obesity in Spanish Community-Dwelling Middle-Aged and Older Women: Association with Balance Confidence, Fear of Falling and Fall Risk. Maturitas 2018, 107, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Combined Effects of Aging and Obesity on Postural Control, Muscle Activity and Maximal Voluntary Force of Muscles Mobilizing Ankle Joint. J. Biomech. 2018, 79, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Billot, M.; Simoneau, E.M.; Van Hoecke, J.; Martin, A. Age-Related Relative Increases in Electromyography Activity and Torque According to the Maximal Capacity during Upright Standing. Eur. J. Appl. Physiol. 2010, 109, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Macie, A.; Matson, T.; Schinkel-Ivy, A. Age Affects the Relationships between Kinematics and Postural Stability during Gait. Gait Posture 2023, 102, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.; Lo, O.-Y.; Olson, E.A.; Habtemariam, D.; Iloputaife, I.; Gagnon, M.M.; Manor, B.; Lipsitz, L.A. Functional Implications of Muscle Co-Contraction during Gait in Advanced Age. Gait Posture. 2017, 53, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, K.; Shyh-Chang, N.; Jiang, Z.; Liu, T.; Ma, S.; Luo, L.; Guang, L.; Liang, K.; Ma, W.; et al. Pathogenesis of Sarcopenia and the Relationship with Fat Mass: Descriptive review. J. Cachex-Sarcopenia Muscle 2022, 13, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, M.d.M.; Gouveia, R.; Gouveia, B.R.; Marques, A.; Martins, F.; Przednowek, K.; França, C.; Peralta, M.; Ihle, A. Associations of Gait Speed, Cadence, Gait Stability Ratio, and Body Balance with Falls in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 13926. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Lee, P.-H.; Lin, L.-F.; Liao, C.-D.; Liou, T.-H.; Huang, S.-W. Effects of Progressive Elastic Band Resistance Exercise for Aged Osteosarcopenic Adiposity Women. Exp. Gerontol. 2021, 147, 111272. [Google Scholar] [CrossRef]
- Andreato, L.V.; de Oliveira, D.V.; Follmer, B.; Bertolini, S.M.M.G. The Influence of Age and Overweight or Obesity on Foot Sensitivity and Postural Control: A Systematic Review. Australas. J. Ageing. 2020, 39, e251–e258. [Google Scholar] [CrossRef]
- Gonzalez, M.; Gates, D.H.; Rosenblatt, N.J. The Impact of Obesity on Gait Stability in Older Adults. J. Biomech. J. Biomech. 2020, 100, 109585. [Google Scholar] [CrossRef]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural Stability in the Elderly: A Comparison between Fallers and Non-Fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Gremeaux, V.; Martin, A. The Involvement of Ankle Muscles in Maintaining Balance in the Upright Posture Is Higher in Elderly Fallers. Exp. Gerontol. 2016, 77, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, Y.; Takahashi, M.; Shinkoda, K. Differences of Muscle Co-Contraction of the Ankle Joint between Young and Elderly Adults during Dynamic Postural Control at Different Speeds. J. Physiol. Anthropol. 2017, 36, 32. [Google Scholar] [CrossRef] [PubMed]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Van Hoecke, J.; Gremeaux, V.; Martin, A. Ankle Muscle Strength Discriminates Fallers from Non-Fallers. Front. Aging Neurosci. 2014, 6, 336. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.H.; Chou, L.S. Gait Balance Control after Fatigue: Effects of Age and Cognitive Demand. Gait Posture 2022, 95, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Melzer, I.; Oddsson, L.I.E. Altered Characteristics of Balance Control in Obese Older Adults. Obes. Res. Clin. Pract. 2016, 10, 151–158. [Google Scholar] [CrossRef]
- Gentier, I.; D’Hondt, E.; Shultz, S.; Deforche, B.; Augustijn, M.; Hoorne, S.; Verlaecke, K.; De Bourdeaudhuij, I.; Lenoir, M. Fine and Gross Motor Skills Differ between Healthy-Weight and Obese Children. Res. Dev. Disabil. 2013, 34, 4043–4051. [Google Scholar] [CrossRef]
- Corbeil, P.; Simoneau, M.; Rancourt, D.; Tremblay, A.; Teasdale, N. Increased Risk for Falling Associated with Obesity: Mathematical Modeling of Postural Control. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 126–136. [Google Scholar] [CrossRef]
- Handrigan, G.; Hue, O.; Simoneau, M.; Corbeil, P.; Marceau, P.; Marceau, S.; Tremblay, A.; Teasdale, N. Weight Loss and Muscular Strength Affect Static Balance Control. Int. J. Obes. 2010, 34, 936–942. [Google Scholar] [CrossRef]
- Handrigan, G.A.; Maltais, N.; Gagné, M.; Lamontagne, P.; Hamel, D.; Teasdale, N.; Hue, O.; Corbeil, P.; Brown, J.P.; Jean, S. Sex-Specific Association between Obesity and Self-Reported Falls and Injuries among Community-Dwelling Canadians Aged 65 Years and Older. Osteoporos. Int. 2017, 28, 483–494. [Google Scholar] [CrossRef]
- Handrigan, G.A.; Simoneau, M.; Teasdale, N.; Corbeil, P. The Effects of Added Mass on Plantar Sole Sensitivity in Upright Standing. J. Biomech. 2012, 45, S233. [Google Scholar] [CrossRef]
- Wu, X.; Madigan, M.L. Impaired Plantar Sensitivity among the Obese Is Associated with Increased Postural Sway. Neurosci. Lett. 2014, 583, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Finch, A.; Solnik, S.; Rider, P.; De Vita, P. Association between Muscle Activation and Metabolic Cost of Walking in Young and Old Adults. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2011, 66A, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Pajoutan, M.; Mehta, R.K.; Cavuoto, L.A. The Effect of Obesity on Central Activation Failure during Ankle Fatigue: A Pilot Investigation. Fatigue Biomed. Health Behav. 2016, 4, 115–126. [Google Scholar] [CrossRef]
- Pajoutan, M.; Ghesmaty Sangachin, M.; Cavuoto, L.A. Central and Peripheral Fatigue Development in the Shoulder Muscle with Obesity during an Isometric Endurance Task. BMC Musculoskelet. Disord. 2017, 18, 314. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Mackenzie, T.A.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, Sarcopenic Obesity, and Functional Impairments in Older Adults: National Health and Nutrition Examination Surveys 1999–2004. Nutr. Res. 2015, 35, 1031–1039. [Google Scholar] [CrossRef]
- Maktouf, W.; Durand, S.; Beaune, B.; Boyas, S. Influence of Obesity and Impact of a Physical Activity Program on Postural Control and Functional and Physical Capacities in Institutionalized Older Adults: A Pilot Study. J. Phys. Act. Health 2019, 17, 169–176. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 152, 26–32. [Google Scholar] [CrossRef]
- Ferhi, H.; Chortane, S.G.; Durand, S.; Beaune, B.; Boyas, S.; Maktouf, W. Effects of Physical Activity Program on Body Composition, Physical Performance, and Neuromuscular Strategies during Walking in Older Adults with Sarcopenic Obesity: Randomized Controlled Trial. Healthcare 2023, 11, 2294. [Google Scholar] [CrossRef]
- Cadore, E.L.; Rodríguez-Mañas, L.; Sinclair, A.; Izquierdo, M. Effects of Different Exercise Interventions on Risk of Falls, Gait Ability, and Balance in Physically Frail Older Adults: A Systematic Review. Rejuvenation Res. 2013, 16, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodriguez-Mañas, L.; Izquierdo, M. Multicomponent Exercises Including Muscle Power Training Enhance Muscle Mass, Power Output, and Functional Outcomes in Institutionalized Frail Nonagenarians. Age 2014, 36, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Dutil, M.; Handrigan, G.A.; Corbeil, P.; Cantin, V.; Simoneau, M.; Teasdale, N.; Hue, O. The Impact of Obesity on Balance Control in Community-Dwelling Older Women. Age 2013, 35, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Simoneau, M.; Teasdale, N. Balance Control Impairment in Obese Individuals Is Caused by Larger Balance Motor Commands Variability. Gait Posture 2015, 41, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Berrigan, F.; Simoneau, M.; Tremblay, A.; Hue, O.; Teasdale, N. Influence of Obesity on Accurate and Rapid Arm Movement Performed from a Standing Posture. Int. J. Obes. 2006, 30, 1750–1757. [Google Scholar] [CrossRef] [PubMed]
- Frontera, W.R. Physiologic Changes of the Musculoskeletal System with Aging: A Brief Review. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 705–711. [Google Scholar] [CrossRef]
- Maktouf, W.; Durand, S.; Boyas, S.; Pouliquen, C.; Beaune, B. Interactions among Obesity and Age-Related Effects on the Gait Pattern and Muscle Activity across the Ankle Joint. Exp. Gerontol. 2020, 140, 111054. [Google Scholar] [CrossRef]
- Hammond, K.G.; Pfeiffer, R.F.; LeDoux, M.S.; Schilling, B.K. Neuromuscular Rate of Force Development Deficit in Parkinson Disease. Clin. Biomech. 2017, 45, 14–18. [Google Scholar] [CrossRef]
- Erskine, R.M.; Tomlinson, D.J.; Morse, C.I.; Winwood, K.; Hampson, P.; Lord, J.M.; Onambélé, G.L. The Individual and Combined Effects of Obesity- and Ageing-Induced Systemic Inflammation on Human Skeletal Muscle Properties. Int. J. Obes. 2017, 41, 102–111. [Google Scholar] [CrossRef]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Winwood, K.; Onambélé-Pearson, G. The Impact of Obesity on Skeletal Muscle Strength and Structure through Adolescence to Old Age. Biogerontology 2016, 17, 467–483. [Google Scholar] [CrossRef]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Winwood, K.; Onambélé-Pearson, G.L. Combined Effects of Body Composition and Ageing on Joint Torque, Muscle Activation and Co-Contraction in Sedentary Women. Age 2014, 36, 9652. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Description and Replication (TIDieR) Guidelines | |
|---|---|
| Name | The TMP program. |
| Why | To enhance steady-state and proactive postural control in older adults with SO (n = 25). |
| Materials | Diverse range of physical materials: chairs, balls, markers, slats, cups, hoops, elastic bands, and weighted bags, foam rollers, balance boards, resistance tubes and bands, exercise mats, medicine balls, step platforms, cones, kettlebells, and step platforms. |
| Procedures | The TMP program was conducted over a 16-week duration, comprising three 60-min sessions per week, for a total of 48 sessions over the course of the intervention. Each session adhered to a structured protocol, commencing with a 10-min warm-up. The central component of each session encompassed motor skill exercises and exercises emphasizing strength and posture, with the duration determined by the prescribed training volume.Motor skill exercises:
|
| Who | Conducted by a specialized kinesiologist in adapted physical activity. |
| How | Collective sessions. |
| Where | In the rehabilitation spaces. |
| How much | Forty-eight sessions. Each session had a duration of 60 min. The design of the exercise types within the program was customized to suit the training load of each session and was based on predefined training intensity and volume for individual sessions. Each exercise regimen included 1 to 5 sets, with repetitions varying from a minimum of 3 to a maximum of 15 per set. |
| Tailoring | Modifications to the training intensity were assessed after each session using the Rating of Perceived Exertion (RPE) scale, as outlined in the study by Ferhi et al. [30]. |
| Modifications | Adjustments were made during each session, following the guidelines provided in the study by Ferhi et al. [30]. |
| How planned | The TMP program comprised three micro-cycles, as outlined in Ferhi et al. [30]. |
| Actual | All participants completed the TMP program. |
| CG n = 25 | IG n = 25 | CG n = 25 | IG n = 25 | |||
|---|---|---|---|---|---|---|
| At Baseline | p-Value | After the Intervention | p-Value | |||
| Anthropometric characteristics | Anthropometric parameters | |||||
| Age (years) | 75.9 ± 5.4 | 76.3 ± 3.5 | NS | 76.3 ± 5.4 | 76.7 ± 3.5 | NS |
| Body height (cm) | 163.2 ± 4.2 | 165.7 ± 4.9 | NS | 163.2 ± 4.2 | 165.7 ± 4.9 | NS |
| Body mass (kg) | 92.1 ± 6.4 | 94.2 ± 5.1 | NS | 90.9 ± 5.4 | 92.6 ± 6.4 *+ | NS |
| BMI (kg/m2) | 34.7 ± 2.3 | 34.5 ± 4.0 | NS | 33.4 ± 2.4 | 31.9 ± 1.4 | NS |
| Body fat (%) | 40.0 ± 4.3 | 39.0 ± 4.5 | NS | 40.4 ± 7.1 | 32.6 ± 4.5 *+ | <0.01 |
| FBM (kg) | 31.9 ± 3.6 | 36.7 ± 5.5 | NS | 36.8 ± 3.6 | 30.2 ± 5.5 *+ | <0.05 |
| LBM (kg) | 60.1 ± 4.2 | 57.5 ± 6.4 | NS | 54.2 ± 4.2 | 62.4 ± 3.4 *+ | <0.05 |
| Waist circumference (cm) | 94.8 ± 4.9 | 89.3 ± 4.8 | NS | 94.2 ± 4.1 | 85.4 ± 4.9 | NS |
| Hip circumference (cm) | 92.0 ± 6.5 | 98.9 ± 4.6 | NS | 92.4 ± 6.1 | 96.5 ± 6.0 | NS |
| Hand grip (N) | 13.7 ± 3.2 | 13.0 ± 2.5 | NS | 13.3 ± 3.0 | 16.3 ± 3.3 *+ | <0.05 |
| Maximal gait speed (m/s) | 0.8 ± 0.2 | 0.7 ± 0.3 | NS | 0.8 ± 0.2 | 1.1 ± 0.4 *+ | <0.05 |
| Tests | Balance parameters | |||||
| Time Up and Go (s) | 12.9 ± 1.9 | 14.1 ± 2.1 | NS | 13.1 ± 1.64 | 11.9 ± 1.34 | <0.05 |
| Romberg test (s) | 13.7 ± 3.2 | 13.3 ± 3.0 | NS | 14.3 ± 2.37 | 17.9 ± 2.32 | <0.01 |
| Intervention Group | ||||||
|---|---|---|---|---|---|---|
| Conditions | Group | CoP Parameters | Baseline | After TMP | Δ (%) | p-Value |
| EO | IG | Area (cm2) | 8.4 ± 3.2 | 5.2 ± 2.9 *+ | −26 | <0.001 |
| CG | 8.1 ± 5.4 | 8.6 ± 7.2 | +6 | NS | ||
| IG | Velocity (mm/s) | 24.9 ± 10.6 | 17.0 ± 4.2 *+ | −31 | <0.01 | |
| CG | 22.9 ± 8.6 | 23.4 ± 6.2 | +3 | NS | ||
| EC | IG | Area (cm2) | 10.7 ± 3.7 | 7.8 ± 3.6 *+ | −27 | <0.01 |
| CG | 10.1 ± 4.9 | 10.5 ± 6.6 | +4 | NS | ||
| IG | Velocity (mm/s) | 32.6 ± 10.2 | 26.5 ± 7.6 *+ | −19 | <0.05 | |
| CG | 29.1 ± 8.2 | 31.6 ± 8.9 | +9 | NS | ||
| TC | IG | Area (cm2) | 24.8 ± 5.1 | 16.4 ± 4.5 *+ | −34 | <0.01 |
| CG | 27.1 ± 9.1 | 25.9 ± 11.1 | −4 | NS | ||
| IG | Velocity (mm /s) | 54.9 ± 14.1 | 34.4 ± 6.3 *+ | −37 | <0.05 | |
| CG | 53.4 ± 10.1 | 55.9 ± 12.1 | +5 | NS | ||
| Intervention Group | ||||||
|---|---|---|---|---|---|---|
| EO | EC | TC | ||||
| Ϫ Area | Ϫ Velocity | Ϫ Area | Ϫ Velocity | Ϫ Area | Ϫ Velocity | |
| Ϫ PF relative | 0.71 * | 0.69 * | 0.62 * | 0.55 * | 0.37 | 0.39 |
| Ϫ DF relative | 0.42 * | 0.54 * | 0.51 * | 0.49 * | 0.39 | 0.42 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magtouf, E.; Chortane, S.G.; Chortane, O.G.; Boyas, S.; Beaune, B.; Durand, S.; Maktouf, W. Influence of Concurrent Exercise Training on Ankle Muscle Activation during Static and Proactive Postural Control on Older Adults with Sarcopenic Obesity: A Multicenter, Randomized, and Controlled Trial. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2779-2794. https://doi.org/10.3390/ejihpe13120192
Magtouf E, Chortane SG, Chortane OG, Boyas S, Beaune B, Durand S, Maktouf W. Influence of Concurrent Exercise Training on Ankle Muscle Activation during Static and Proactive Postural Control on Older Adults with Sarcopenic Obesity: A Multicenter, Randomized, and Controlled Trial. European Journal of Investigation in Health, Psychology and Education. 2023; 13(12):2779-2794. https://doi.org/10.3390/ejihpe13120192
Chicago/Turabian StyleMagtouf, Elmoetez, Sabri Gaied Chortane, Oussema Gaied Chortane, Sébastien Boyas, Bruno Beaune, Sylvain Durand, and Wael Maktouf. 2023. "Influence of Concurrent Exercise Training on Ankle Muscle Activation during Static and Proactive Postural Control on Older Adults with Sarcopenic Obesity: A Multicenter, Randomized, and Controlled Trial" European Journal of Investigation in Health, Psychology and Education 13, no. 12: 2779-2794. https://doi.org/10.3390/ejihpe13120192
APA StyleMagtouf, E., Chortane, S. G., Chortane, O. G., Boyas, S., Beaune, B., Durand, S., & Maktouf, W. (2023). Influence of Concurrent Exercise Training on Ankle Muscle Activation during Static and Proactive Postural Control on Older Adults with Sarcopenic Obesity: A Multicenter, Randomized, and Controlled Trial. European Journal of Investigation in Health, Psychology and Education, 13(12), 2779-2794. https://doi.org/10.3390/ejihpe13120192