




Measuring Vulnerability in Grief: The Psychometric Properties of the Italian Adult Attitude to Grief Scale

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
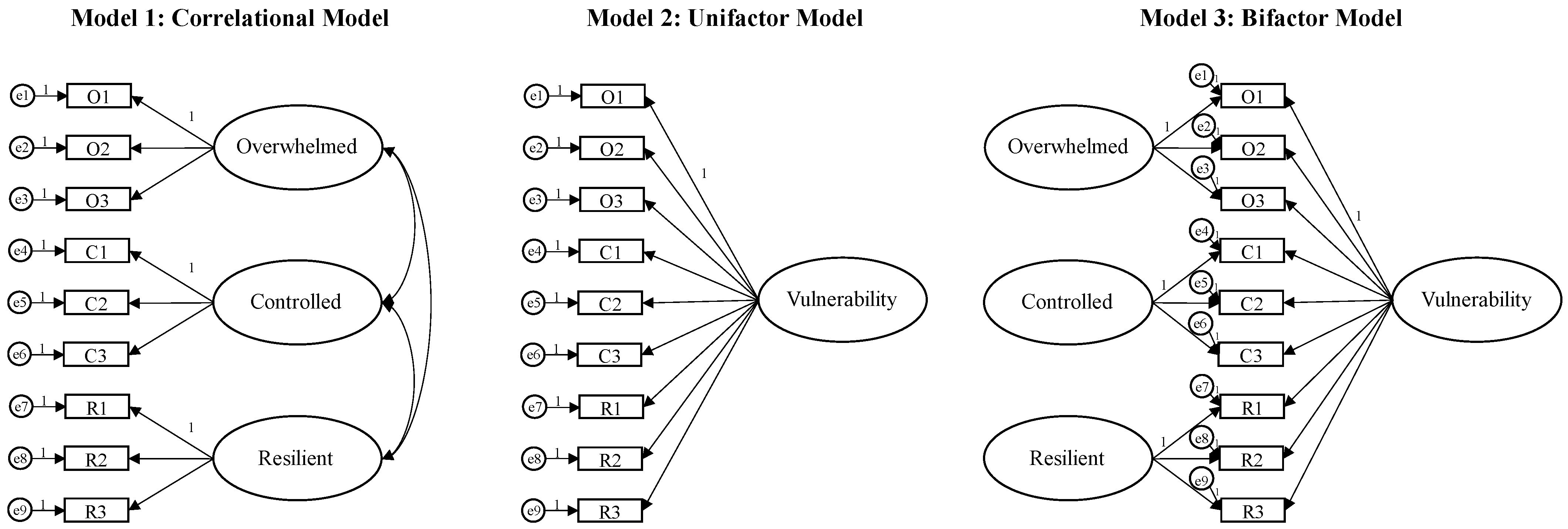
1.1. The Adult Attitude to Grief Scale
- The “overwhelmed” factor, indicating a feeling of being overcome with grief, being stressed, and having lost the meaning of life.
- The “control” factor, indicating instinctive mechanisms to resist pain and maintain autonomy by avoiding full engagement with the loss.
- The “resilient” factor, indicating the perception of having resources to cope with the grief and the hope of overcoming it.
1.2. Aim and Hypothesis
2. Materials and Methods
2.1. Participants
2.2. Procedure and Ethics
2.3. Measures
2.3.1. Adult Attitude to Grief Scale (AAG)
2.3.2. Forty-Item Defense Style Questionnaire (DSQ-40)
2.3.3. Impact of Event Scale—Revised (IES-R)
2.3.4. Beck Depression Inventory-II (BDI-II)
2.4. Data Analysis
3. Results
4. Discussion
Limitations and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. The Adult Attitude to Grief Scale—Italian Version
| Fortemente D’accordo | D’accordo | Né D’accordo né in Disaccordo | In Disaccordo | Fortemente in Disaccordo |
| 4 | 3 | 2 | 1 | 0 |
| 1. Mi sento in grado di affrontare il dolore che deriva dalla perdita. | 4 | 3 | 2 | 1 | 0 |
| 2. Per me, è difficile reprimere i pensieri sulla persona che ho perso. | 4 | 3 | 2 | 1 | 0 |
| 3. Mi sento molto consapevole della mia forza interiore quando affronto il dolore. | 4 | 3 | 2 | 1 | 0 |
| 4. Credo di dover essere coraggioso nell’affrontare la perdita. | 4 | 3 | 2 | 1 | 0 |
| 5. Sento che porterò sempre con me il dolore della sofferenza. | 4 | 3 | 2 | 1 | 0 |
| 6. Per me, è importante tenere sotto controllo il mio dolore. | 4 | 3 | 2 | 1 | 0 |
| 7. La vita ha meno significato per me dopo questa perdita. | 4 | 3 | 2 | 1 | 0 |
| 8. Penso che sia meglio andare avanti con la vita e non soffermarsi su questa perdita. | 4 | 3 | 2 | 1 | 0 |
| 9. Potrebbe non sempre sembrare così, ma credo che supererò questa esperienza di dolore. | 4 | 3 | 2 | 1 | 0 |
References
- Talerico, K.A. Grief & older adults: Differences, issues, and clinical approaches. J. Psychosoc. Nurs. Ment. Health Serv. 2023, 41, 12–16. [Google Scholar] [CrossRef]
- Stroebe, M.S.; Hansson, R.O.; Stroebe, W.; Schut, H.E. Handbook of Bereavement Research: Consequences, Coping, and Care; American Psychological Association: Washington, DC, USA, 2001. [Google Scholar]
- Rando, T.A. Grief and mourning: Accommodating to loss. In Dying: Facing the Facts; Wass, H., Neimeyer, R.A., Eds.; Taylor & Francis: Washington, DC, USA, 2018; pp. 211–241. [Google Scholar]
- Rosenblatt, P.C. Researching grief: Cultural, relational, and individual possibilities. J. Loss Trauma 2017, 22, 617–630. [Google Scholar] [CrossRef]
- Rosenblatt, P.C. Grief across cultures: A review and research agenda. In Handbook of Bereavement Research and Practice: Advances in Theory and Intervention; Stroebe, M.S., Hansson, R.O., Schut, H., Stroebe, W., Eds.; American Psychological Association: Washington, DC, USA, 2008; pp. 207–222. [Google Scholar] [CrossRef]
- Strada, E.A. Grief, demoralization, and depression: Diagnostic challenges and treatment modalities. Prim. Psychiatry 2009, 16, 49–55. [Google Scholar]
- Boelen, P.A.; Smid, G.E. Disturbed grief: Prolonged grief disorder and persistent complex bereavement disorder. BMJ 2017, 357, j2016. [Google Scholar] [CrossRef]
- Boelen, P.A. Improving the understanding and treatment of complex grief: An important issue for psychotraumatology. Eur. J. Psychotraumatol. 2016, 7, 32609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottington, E.M.; Matthews, K.A.; Talbott, E.; Kuller, L.H. Environmental events preceding sudden death in women. Psychosom Med. 1980, 42, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, T.C. Immunity and health after bereavement in relation to coping. Scand. J. Psychol. 1997, 38, 253–259. [Google Scholar] [CrossRef]
- Espinosa, J.; Evans, W.N. Heightened mortality after the death of a spouse: Marriage protection or marriage selection? J. Health Econ. 2008, 27, 1326–1342. [Google Scholar] [CrossRef]
- Ajdacic-Gross, V.; Ring, M.; Gadola, E.; Lauber, C.; Bopp, M.; Gutzwiller, F.; Rössler, W. Suicide after bereavement: An overlooked problem. Psychol. Med. 2008, 38, 673–676. [Google Scholar] [CrossRef] [Green Version]
- Comtesse, H.; Rosner, R. Prolonged grief disorder among asylum seekers in Germany: The influence of losses and residence status. Eur. J. Psychotraumatol. 2019, 10, 1591330. [Google Scholar] [CrossRef] [Green Version]
- Komischke-Konnerup, K.B.; Zachariae, R.; Johannsen, M.; Nielsen, L.D.; O’Connor, M. Co-occurrence of prolonged grief symptoms and symptoms of depression, anxiety, and posttraumatic stress in bereaved adults: A systematic review and meta-analysis. J. Affect. Disord. Rep. 2021, 4, 100140. [Google Scholar] [CrossRef]
- Djelantik, A.M.J.; Smid, G.E.; Kleber, R.J.; Boelen, P.A. Symptoms of prolonged grief, post-traumatic stress, and depression after loss in a Dutch community sample: A latent class analysis. Psychiatry Res. 2017, 247, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Harrison, O.; Windmann, S.; Rosner, R.; Steil, R. Interpersonal problems and cooperative behavior in patients suffering from prolonged grief disorder as compared to bereaved healthy controls. J. Clin. Psychol. 2022, 78, 1912–1924. [Google Scholar] [CrossRef] [PubMed]
- Thompson, N.; Lund, D.A. Loss, Grief, and Trauma in the Workplace; Routledge: New York, NY, USA, 2017. [Google Scholar]
- Treml, J.; Linde, K.; Engel, C.; Glaesmer, H.; Hinz, A.; Luck, T.; Riedel-Hellere, S.; Sander, C.; Kersting, A. Loss and grief in elderly people: Results from the LIFE-Adult-Study. Death Stud. 2022, 46, 1621–1630. [Google Scholar] [CrossRef]
- Prigerson, H.G.; Maciejewski, P.K.; Reynolds, C.F., 3rd; Bierhals, A.J.; Newsom, J.T.; Fasiczka, A.; Frank, E.; Doman, J.; Miller, M. Inventory of Complicated Grief: A scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995, 59, 65–79. [Google Scholar] [CrossRef]
- Prigerson, H.G.; Boelen, P.A.; Xu, J.; Smith, K.V.; Maciejewski, P.K. Validation of the new DSM-5-TR criteria for prolonged grief disorder and the PG-13-Revised (PG-13-R) scale. World Psychiatry 2021, 20, 96–106. [Google Scholar] [CrossRef]
- Shear, K.M.; Jackson, C.T.; Essock, S.M.; Donahue, S.A.; Felton, C.J. Brief Grief Questionnaire [Database Record]; APA PsycTests: Washington, DC, USA, 2006. [Google Scholar] [CrossRef]
- Sim, J.; Machin, L.; Bartlam, B. Identifying vulnerability in grief: Psychometric properties of the Adult Attitude to Grief Scale. Qual. Life Res. 2014, 23, 1211–1220. [Google Scholar] [CrossRef]
- Machin, L.; Bartlam, R.; Bartlam, B. Identifying levels of vulnerability in grief using the Adult Attitude to Grief scale: From theory to practice. Bereave. Care 2015, 34, 59–68. [Google Scholar] [CrossRef]
- Machin, L. Working with Loss and Grief: A New Model for Practitioners; Sage: London, UK, 2008. [Google Scholar]
- Machin, L. Working with Loss and Grief: A Theoretical and Practical Approach, 2nd ed.; Sage: London, UK, 2014. [Google Scholar]
- Diamond, H.; Llewelyn, S.; Relf, M.; Bruce, C. Helpful aspects of bereavement support for adults following an expected death: Volunteers’ and bereaved people’s perspectives. Death Stud. 2012, 36, 541–564. [Google Scholar] [CrossRef]
- Selman, L.E.; Farnell, D.J.; Longo, M.; Goss, S.; Torrens-Burton, A.; Seddon, K.; Mayland, C.R.; Machin, L.; Byrne, A.; Harrop, E.J. Factors associated with higher levels of grief and support needs among people bereaved during the pandemic: Results from a national online survey. Omega Westport 2022. advanced online publication. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.F.M. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, G.; Singh, M.; Bond, M. The Defense Style Questionnaire. J. Nerv. Ment. Dis. 1993, 181, 246–256. [Google Scholar] [CrossRef]
- Cortinovis, I.; Farma, T. Misurare i meccanismi di diffesa attraverso il “Defense Style Questionnaire” a 40 item. Attendibilita’ dello strumento e suo utilizzo nel contesto Italiano [Measuring defense mechanism through the 40 items of the “Defense Style Questionnaire.“ Reliability of the instrument and its use in the Italian context]. Ric. Di Psicol. 2000, 24, 127–144. [Google Scholar]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale—Revised. In Assessing Psychological Trauma and PTSD; Wilson, J.P., Keane, T.M., Eds.; Guilford Press: New York, NY, USA, 1996; pp. 399–411. [Google Scholar]
- Craparo, G.; Faraci, P.; Rotondo, G.; Gori, A. The Impact of Event Scale—Revised: Psychometric properties of the Italian version in a sample of flood victims. Neuropsychiatr. Dis. Treat. 2013, 9, 1427–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. BDI-II. Beck Depression Inventory; The Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar] [CrossRef]
- Ghisi, M.; Flebus, G.B.; Montano, A.; Sanavio, E.; Sica, C. Beck Depression Inventory-II. Manuale italiano; Giunti Organizzazioni Speciali: Florence, Italy, 2006. [Google Scholar]
- Sica, C.; Ghisi, M. The Italian versions of the Beck Anxiety Inventory and the Beck Depression Inventory-II: Psychometric properties and discriminant power. In Leading-Edge Psychological Tests and Testing Research; Lange, M.A., Ed.; Nova Science Publishers: New York, NY, USA, 2007; pp. 27–50. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows (Version 21.0) [Computer Software]; IBM Corp.: Armonk, NY, USA, 2012. [Google Scholar]
- Arbuckle, J.L. IBM SPSS Amos 24 User’s Guide; Amos Development Corporation: Meadville, PA, USA, 2016. [Google Scholar]
- JASP Team. JASP (Version 0.17.2) [Computer Software]; JASP Team: Amsterdam, The Netherlands, 2023. [Google Scholar]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef]
- Mulaik, S.A. Foundations of Factor Analysis; CRC Press: Boca Raton, FL, USA, 2009. [Google Scholar]
- Marsh, H.W.; Hocevar, D. Application of confirmatory factor analysis to the study of self-concept: First- and higher order factor models and their invariance across groups. Psychol. Bull. 1985, 97, 562–582. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modeling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–59. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Marsh, H.W.; Hau, K.T.; Wen, Z. In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Struct. Equ. Model. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Wegener, D.T.; MacCallum, R.C.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming, 2nd ed.; Taylor and Francis Group: New York, NY, USA, 2010. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- McDonald, R.P. Test Theory: A Unified Treatment; Psychology Press: London, UK, 2013. [Google Scholar]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Gaskin, J.; James, M. HTMT Plugin for AMOS. 2019. Available online: https://statwiki.kolobkreations.com/index.php?title=Plugins (accessed on 29 February 2020).
- Prigerson, H.G.; Jacobs, S.C. Traumatic grief as a distinct disorder: A rationale, consensus criteria, and a preliminary empirical test. In Handbook of Bereavement Research: Consequences, Coping and Care; Stroebe, M.S., Hansson, R.O., Stroebe, W., Schut, H., Eds.; American Psychological Association: Washington, DC, USA, 2001; pp. 613–645. [Google Scholar]
- Prigerson, H.G.; Kakarala, S.; Gang, J.; Maciejewski, P.K. History and status of prolonged grief disorder as a psychiatric diagnosis. Annu. Rev. Clin. Psychol. 2021, 17, 109–126. [Google Scholar] [CrossRef]
- Prigerson, H.G.; Shear, M.K.; Reynolds, C.F. Prolonged grief disorder diagnostic criteria—Helping those with maladaptive grief responses. JAMA Psychiatry 2022, 79, 277–278. [Google Scholar] [CrossRef]
- Larsen, L.H.; Guldberg, A.; Kring, V. A group therapy program for parentally bereaved young adults with grief complications: Rationale, method and case examples. Omega Westport 2021, 88, 1212–1234. [Google Scholar] [CrossRef]
- Linde, K.; Treml, J.; Steinig, J.; Nagl, M.; Kersting, A. Grief interventions for people bereaved by suicide: A systematic review. PLoS ONE 2017, 12, e0179496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzinger, K.J.M.; Swineford, F. The bi-factor method. Psychometrika 1937, 2, 41–54. [Google Scholar] [CrossRef]
- Mansolf, M.; Reise, S.P. When and why the second-order and bifactor models are distinguishable. Intelligence 2017, 61, 120–129. [Google Scholar] [CrossRef]
- Reise, S.P. The rediscovery of bifactor measurement models. Multivariate Behav. Res. 2012, 47, 667–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, J.; Zhao, Y.; Feng, X.; Wang, Y.; Yu, Z.; Hua, L.; Wang, S.; Li, J. How is fatalistic determinism linked to depression? The mediating role of self-control and resilience. Pers. Individ. Dif. 2021, 180, 110992. [Google Scholar] [CrossRef]
- Brosowsky, N.P.; Smith, A.C.; Smilek, D.; Seli, P. On the relation between mind wandering, PTSD symptomology, and self-control. Conscious. Cogn. 2022, 99, 103288. [Google Scholar] [CrossRef] [PubMed]
- Lindner, C.; Kotta, I.; Marschalko, E.E.; Szabo, K.; Kalcza-Janosi, K.; Retelsdorf, J. Increased risk perception, distress intolerance and health anxiety in stricter lockdowns: Self-control as a key protective factor in early response to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 5098. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Musetti, A.; Giannini, M.; Grotto, R.L.; Svicher, A.; Di Fabio, A. The protective role of mature defense mechanisms on satisfaction with life in the COVID-19 era: A moderated mediation analysis. Behav. Sci. 2022, 12, 290. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Caretti, V. The impact of COVID-19 lockdown on perceived stress: The role of defence mechanisms and coping strategies. J. Conting. Crisis Manag. 2022, 30, 379–390. [Google Scholar] [CrossRef]
- Altwaijri, N.; Abualait, T.; Aljumaan, M.; Albaradie, R.; Arain, Z.; Bashir, S. Defense mechanism responses to COVID-19. PeerJ 2022, 10, e12811. [Google Scholar] [CrossRef]
- Cramer, P. Protecting the Self: Defense Mechanisms in Action; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Boelen, P.A.; Reijntjes, A.; Djelantik, A.M.J.; Smid, G.E. Prolonged grief and depression after unnatural loss: Latent class analyses and cognitive correlates. Psychiatry Res. 2016, 240, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, A.; Liddell, B.J.; Maccallum, F.; Steel, Z.; Silove, D.; Bryant, R.A. Posttraumatic stress disorder and prolonged grief in refugees exposed to trauma and loss. BMC Psychiatry 2014, 14, 106. [Google Scholar] [CrossRef] [Green Version]
- Skalski, S.; Konaszewski, K.; Dobrakowski, P.; Surzykiewicz, J.; Lee, S.A. Pandemic grief in Poland: Adaptation of a measure and its relationship with social support and resilience. Curr. Psychol. 2022, 41, 7393–7401. [Google Scholar] [CrossRef] [PubMed]
- Dodd, A.; Guerin, S.; Delaney, S.; Dodd, P. Complicated grief: Knowledge, attitudes, skills and training of mental health professionals: A systematic review. Patient Educ. Couns. 2017, 100, 1447–1458. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Topino, E.; Musetti, A. The relationship among anxiety, worry, perceived stress, defense mechanisms, and high levels of post-traumatic stress symptoms: A discriminant analytic approach. J. Pers. Med. 2023, 13, 237. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E.; Musetti, A. Pathways towards posttraumatic stress symptomatology: A moderated mediation model including perceived stress, worry, and defense mechanisms. Psychol. Trauma. 2023. advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Ferrajão, P.; Dias, J.; Elklit, A. Defense mechanisms mediate associations between exposure to adverse childhood experiences and anxiety and depression in Kenyan adolescents. Traumatology 2022. advance online publication. [Google Scholar] [CrossRef]
- Vaillant, G.E. Involuntary coping mechanisms: A psychodynamic perspective. Dialogues Clin. Neurosci. 2011, 13, 366–370. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; text revision; American Psychiatric Publishing: Washington, DC, USA, 2022. [Google Scholar]


{kind=link}
| Characteristics | M ± SD | n | % | |
|---|---|---|---|---|
| Age | 30.44 ± 11.206 | |||
| Sex | ||||
| Females | 285 | 77.7 | ||
| Males | 82 | 22.3 | ||
| Marital status | ||||
| Single | 261 | 71.1 | ||
| Married | 55 | 15 | ||
| Cohabiting | 39 | 10.6 | ||
| Divorced | 9 | 2.5 | ||
| Separated | 2 | 0.5 | ||
| Widowed | 1 | 0.3 | ||
| Education | ||||
| Elementary school | 1 | 0.3 | ||
| Middle School diploma | 30 | 8.2 | ||
| High School diploma | 123 | 33.5 | ||
| University degree | 125 | 34.1 | ||
| Master’s degree | 64 | 17.4 | ||
| Post-lauream specialization | 24 | 6.5 | ||
| Occupation | ||||
| Student | 134 | 36.5 | ||
| Working-student | 55 | 15 | ||
| Employee | 85 | 23.2 | ||
| Freelance | 30 | 8.2 | ||
| Entrepreneur | 11 | 3 | ||
| Manager | 5 | 1.4 | ||
| Artisan | 7 | 1.9 | ||
| Trader | 6 | 1.6 | ||
| Retired | 7 | 1.9 | ||
| Unemployed | 27 | 7.4 | ||
| Experience of loss | ||||
| Mourning | 219 | 59.7 | ||
| Separation from important people (e.g., friends, family, partner) | 114 | 31.1 | ||
| Loss of work, job opportunities, or important occasions. | 34 | 9.3 | ||
| χ2 | df | p | NFI | TLI | CFI | RMSEA | SRMR | Model Comparisons | Δχ2 | Δdf | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Correlational model | 66.171 | 21 | <0.001 | 0.930 | 0.914 | 0.950 | 0.077 | 0.056 | ||||
| - | - | - | - | |||||||||
| Unifactor model | 236.913 | 24 | <0.001 | 0.748 | 0.647 | 0.765 | 0.155 | 0.109 | ||||
| M1-M2 | 170.742 | 3 | <0.001 | |||||||||
| Bifactor model | 19.905 | 11 | <0.05 | 0.979 | 0.968 | 0.990 | 0.047 | 0.018 | ||||
| M1-M3 | 46.266 | 10 | <0.001 |
| 1 | 2 | 3 | |
|---|---|---|---|
| 1. Overwhelmed | — | 0.037 | 0.359 |
| 2. Controlled | –0.035 (0.052) | — | 0.790 |
| 3. Resilient | –0.267 (0.050) | 0.567 (0.043) | — |
| α | 0.701 | 0.638 | 0.793 |
| ω | 0.703 | 0.643 | 0.800 |
| AAG Total Score: Vulnerability | Overwhelmed | Controlled | Resilient | ||
|---|---|---|---|---|---|
| Defense mechanisms | |||||
| Mature | −0.187 *** (0.386) | −0.008 (0.023) | 0.195 *** (0.331) | 0.223 *** (0.362) | |
| Neurotic | 0.094 (0.248) | 0.224 *** (0.328) | 0.080 (0.157) | –0.025 (0.025) | |
| Immature | 0.110 * (0.180) | 0.219 *** (0.277) | 0.107 * (0.159) | –0.089 (0.090) | |
| Post-traumatic symptoms | |||||
| Total score | 0.391 *** (0.248) | 0.336 *** (0.413) | −0.152 ** (0.185) | −0.339 *** (0.393) | |
| Intrusion | 0.289 *** (0.059) | 0.266 *** (0.347) | −0.058 (0.069) | −0.278 *** (0.343) | |
| Avoidance | 0.400 *** (0.128) | 0.338 *** (0.423) | −0.203 *** (0.255) | −0.312 *** (0.369) | |
| Hyperarousal | 0.374 *** (0.130) | 0.310 *** (0.394) | −0.141 ** (0.181) | −0.339 *** (0.406) | |
| Depressive symptoms | |||||
| Total score | 0.435 *** (0.248) | 0.298 *** (0.362) | −0.202 *** (0.262) | −0.431 *** (0.500) | |
| Somatic and Affective | 0.388 *** (0.205) | 0.277 *** (0.343) | −0.173 *** (0.226) | −0.377 *** (0.444) | |
| Cognitive | 0.436 *** (0.281) | 0.285 *** (0.356) | −0.210 *** (0.284) | −0.441 *** (0.528) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gori, A.; Topino, E.; Imperatore, P.; Musetti, A.; Sim, J.; Machin, L. Measuring Vulnerability in Grief: The Psychometric Properties of the Italian Adult Attitude to Grief Scale. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 975-985. https://doi.org/10.3390/ejihpe13060074
Gori A, Topino E, Imperatore P, Musetti A, Sim J, Machin L. Measuring Vulnerability in Grief: The Psychometric Properties of the Italian Adult Attitude to Grief Scale. European Journal of Investigation in Health, Psychology and Education. 2023; 13(6):975-985. https://doi.org/10.3390/ejihpe13060074
Chicago/Turabian StyleGori, Alessio, Eleonora Topino, Pierluigi Imperatore, Alessandro Musetti, Julius Sim, and Linda Machin. 2023. "Measuring Vulnerability in Grief: The Psychometric Properties of the Italian Adult Attitude to Grief Scale" European Journal of Investigation in Health, Psychology and Education 13, no. 6: 975-985. https://doi.org/10.3390/ejihpe13060074
APA StyleGori, A., Topino, E., Imperatore, P., Musetti, A., Sim, J., & Machin, L. (2023). Measuring Vulnerability in Grief: The Psychometric Properties of the Italian Adult Attitude to Grief Scale. European Journal of Investigation in Health, Psychology and Education, 13(6), 975-985. https://doi.org/10.3390/ejihpe13060074