




Associations of Mental Health Issues with Health Literacy and Vaccination Readiness against COVID-19 in Long-Term Care Facilities—A Cross-Sectional Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
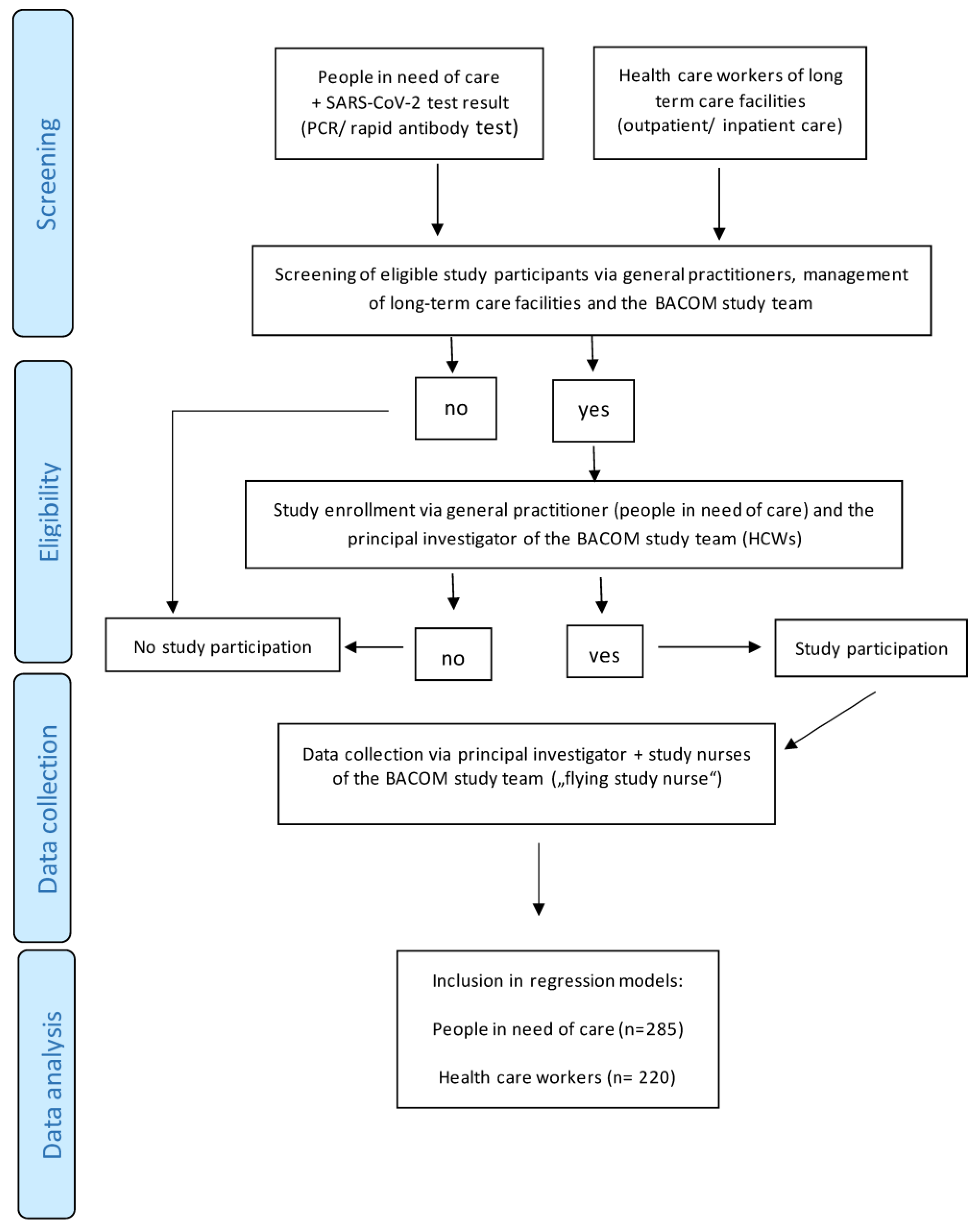
2.1. Study Design and Setting
2.2. Participants
2.2.1. Eligibility Criteria for Patients
2.2.2. Eligibility Criteria for Participating HCWs
2.3. Variables
2.3.1. Parameters of Interest among People in Need of Care
2.3.2. Parameters of Interest among HCWs
2.4. Data Sources/Measurement
2.5. Bias
2.6. Study Size
2.7. Quantitative Variables
2.8. Statistical Methods
3. Results
3.1. Participants
3.2. Descriptive Data, Outcome Data, and Main Results
3.2.1. People in Need of Care
3.2.2. Healthcare Workers (HCWs)
4. Discussion
4.1. Key Results
4.2. Strength and Limitations
4.3. Interpretation
4.4. Implications for Research and Practice
4.5. Generalizability
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations (in Alphabetical Order)
| BaCoM | Bavarian ambulatory COVID-19 monitor |
| 5C | psychological antecedents of vaccination readiness |
| CFS | clinical frailty scale |
| CI | confidence interval |
| OR | odds ratio |
| DP | depersonalization |
| DRKS | German Register of Clinical Studies |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders 5th edition |
| EE | emotional exhaustion |
| GAD-7 | Generalized Anxiety Disorder Scale-7 |
| GP | general practitioner |
| HCWs | healthcare workers |
| HLS-EU-Q16 | Health Literacy Questionnaire |
| IQR | interquartile range |
| MBI-HSS | Maslach Burnout Inventory—Human Services Survey |
| OECD | Organization for Economic Cooperation and Development |
| PA | personal accomplishment |
| PCR | polymerase-chain reaction |
| PHQ-9 | Patient Health Questionnaire-9 |
| Q | quartile |
References
- Mercier, G.; Arquizan, C.; Roubille, F. Understanding the effects of COVID-19 on health care and systems. Lancet Public Health 2020, 5, e524. [Google Scholar] [CrossRef] [PubMed]
- Pitkälä, K.H. COVID-19 has hit nursing homes hard. Eur. Geriatr. Med. 2020, 11, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Shikha, D.; Kushwaha, P.; Gokdemir, O.; Marzo, R.R.; Bhattacharya, S. Editorial: Health literacy and disease prevention. Front. Public Health 2023, 11, 1128257. [Google Scholar] [CrossRef] [PubMed]
- van der Gaag, M.; Heijmans, M.; Ballester, M.; Orrego, C.; Niño de Guzmán, E.; Ninov, L.; Rademakers, J. Preferences Regarding Self-Management Intervention Outcomes of Dutch Chronically Ill Patients with Limited Health Literacy. Front. Public Health 2022, 10, 842462. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.B.; Wong, K.L.Y.; To-Miles, F.; Dunn, S.; Gregorio, M.; Wong, L.; Tam, S.; Huynh, P.; Hung, L. Exploring experiences of loneliness among Canadian long-term care residents during the COVID-19 pandemic: A qualitative study. Int. J. Older People Nurs. 2023, 18, e12509. [Google Scholar] [CrossRef]
- El-Ghitany, E.M.; Ashour, A.; Omran, E.A.; Farghaly, A.G.; Hassaan, M.A.; Azzam, N. COVID-19 vaccine acceptance rates and predictors among the Egyptian general population and Healthcare workers, the intersectionality of age and other factors. Sci. Rep. 2022, 12, 19832. [Google Scholar] [CrossRef]
- Liu, Y.; Meng, H.; Tu, N.; Liu, D. The Relationship between Health Literacy, Social Support, Depression, and Frailty among Community-Dwelling Older Patients with Hypertension and Diabetes in China. Front. Public Health 2020, 8, 280. [Google Scholar] [CrossRef] [PubMed]
- Ding, K.-R.; Wang, S.-B.; Xu, W.-Q.; Lin, L.-H.; Liao, D.-D.; Chen, H.-B.; Tan, W.-Y.; Huang, J.-H.; Hou, C.-L.; Jia, F.-J. Low mental health literacy and its association with depression, anxiety and poor sleep quality in Chinese elderly. Asia-Pac. Psychiatry 2022, 14, e12520. [Google Scholar] [CrossRef]
- Gorenko, J.A.; Moran, C.; Flynn, M.; Dobson, K.; Konnert, C. Social Isolation and Psychological Distress among Older Adults Related to COVID-19: A Narrative Review of Remotely-Delivered Interventions and Recommendations. J. Appl. Gerontol. 2021, 40, 3–13. [Google Scholar] [CrossRef]
- Filindassi, V.; Pedrini, C.; Sabadini, C.; Duradoni, M.; Guazzini, A. Impact of COVID-19 First Wave on Psychological and Psychosocial Dimensions: A Systematic Review. COVID 2022, 2, 273–340. [Google Scholar] [CrossRef]
- Guazzini, A.; Pesce, A.; Marotta, L.; Duradoni, M. Through the Second Wave: Analysis of the Psychological and Perceptive Changes in the Italian Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1635. [Google Scholar] [CrossRef]
- Pereira-Lima, K.; Loureiro, S.R.; Silveira, I.L.M.; Crippa, J.A.; Hallak, J.E.C.; Zuardi, A.W.; Osório, F.L. Workplace Protections and Burnout among Brazilian Frontline Health Care Professionals during the COVID-19 Pandemic. Front. Psychol. 2022, 13, 880049. [Google Scholar] [CrossRef]
- Takahashi, T.; Ekoyama, S.; Tachikawa, H.; Midorikawa, H.; Shiratori, Y.; Ota, M.; Takahashi, S.; Arai, T. Mental Health of Caregivers Working in Nursing Homes during the COVID-19 Pandemic. Dement. Geriatr. Cogn. Disord. 2022, 51, 233–240. [Google Scholar] [CrossRef]
- Perlis, R.H.; Ognyanova, K.; Santillana, M.; Lin, J.; Druckman, J.; Lazer, D.; Green, J.; Simonson, M.; Baum, M.A.; Della Volpe, J. Association of Major Depressive Symptoms with Endorsement of COVID-19 Vaccine Misinformation among US Adults. JAMA Netw. Open 2022, 5, e2145697. [Google Scholar] [CrossRef]
- Warren, N.; Kisely, S.; Siskind, D. Maximizing the Uptake of a COVID-19 Vaccine in People with Severe Mental Illness: A Public Health Priority. JAMA Psychiatry 2021, 78, 589–590. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2019, 13, e0208601. [Google Scholar] [CrossRef]
- Dumyati, G.; Jump, R.L.P.; Gaur, S. Mandating COVID-19 Vaccine for Nursing Home Staff: An Ethical Obligation. J. Am. Med. Dir. Assoc. 2021, 22, 1967–1968. [Google Scholar] [CrossRef]
- Koch, J.; Piechotta, V.; Berner, R.; Bogdan, C.; Burchard, G.; Heininger, U.; Hummers, E.; von Kries, R.; Ledig, T.; Littmann, M. Wissenschaftliche Begründung der STIKO zur Implementierung der COVID-19-Impfung in die allgemeinen Empfehlungen der STIKO 2023. 2023. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2023/21/Art_02.html (accessed on 1 February 2024).
- Robert Koch-Institut. Monitoring von COVID-19 und der Impfsituation in Langzeitpflegeeinrichtungen-Stand der Erhebung September 2021 bis Februar 2022; Berlin, 2022. Available online: https://www.rki.de/DE/Content/Infekt/Impfen/ImpfungenAZ/COVID-19/Monitoring_Covid-19_Impfen_Langzeitpflege.html#:~:text=Das%20Robert%20Koch%2DInstitut%20(%20RKI,freiwilligen%20Teilnahme%20der%20Pflegeeinrichtungen%20durchgef%C3%BChrt (accessed on 1 February 2024).
- Hering, C.; Gangnus, A.; Kohl, R.; Steinhagen-Thiessen, E.; Kuhlmey, A.; Gellert, P. COVID-19-Impfstatus von Pflegenden und assoziierte Faktoren in der stationären Langzeitpflege. ZGerontol Geriatr 2023. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Gensichen, J.; Zöllinger, I.; Gágyor, I.; Hausen, A.; Hölscher, M.; Janke, C.; Kühlein, T.; Nassehi, A.; Teupser, D.; Arend, F.; et al. Impact of the COVID-19 pandemic on people in need of care or support: Protocol for a SARSCoV-2 registry. BMJ Open 2023, 13, e071134. [Google Scholar] [CrossRef] [PubMed]
- Sanftenberg, L.; Dreischulte, T.; Härdtlein, A.; Kosub, H.; Gágyor, I.; Kurotschka, P.K.; Kühlein, T.; Burggraf, L.; Eck, S.; Roos, M.; et al. Process evaluation in practice based research networks: A study protocol for a mixed-methods implementation study. BMJ Open 2023, 13, e065947. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Cmaj 2005, 173, 489–495. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md State Med. J. 1965, 14, 61–65. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Callahan, C.M.; Unverzagt, F.W.; Hui, S.L.; Perkins, A.J.; Hendrie, H.C. Six-item screener to identify cognitive impairment among potential subjects for clinical research. Med. Care 2002, 40, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.M.; Cho, Y.S.; Park, S.; Lee, B.H.; Sohn, B.K.; Choi, C.H.; Choi, J.S.; Jeong, H.Y.; Cho, S.J.; Lee, J.H.; et al. Montreal cognitive assessment reflects cognitive reserve. BMC Geriatr 2018, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Goggins, W.; Sham, A.; Ho, S.C. Social Determinants of Frailty. Gerontology 2005, 51, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Berglund, H.; Hasson, H.; Wilhelmson, K.; Dunér, A.; Dahlin-Ivanoff, S. The Impact of Socioeconomic Conditions, Social Networks, and Health on Frail Older People’s Life Satisfaction: A Cross-Sectional Study. Health Psychol. Res. 2016, 4, 5578. [Google Scholar] [CrossRef]
- Bustamante, A.V.; Vilar-Compte, M.; Ochoa Lagunas, A. Social support and chronic disease management among older adults of Mexican heritage: A U.S.-Mexico perspective. Soc. Sci. Med. 2018, 216, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Harun, S.; Çetin, F.; Basım, N. The Effect of Burnout on Organizational Citizenship Behaviour: The Mediating Role of Job Satisfaction. Int. J. Contemp. Econ. Adm. Sci. 2011, 1, 40–64. [Google Scholar]
- Zekja, I.; Kamberi, F.; Bruijn, R.; Kokuri, T.; Asimakopoulou, E. COVID-19 Mental Health Impact and Readiness to Be Vaccinated among Medical Academic Staff in Non-EU and EU Countries. OBM Neurobiol. 2023, 7, 166. [Google Scholar] [CrossRef]
- Maksymenko, S.; Kokun, O.; Topolov, I.; Nemesh, O.; Flaherty, M. The influnece of occupational stress on employees’ mental health. Wiad Lek 2021, 74, 2818–2822. [Google Scholar] [CrossRef] [PubMed]
- Lamptey, E. Should Breakthrough SARS-CoV-2 Infection Affect Our Confidence in the COVID-19 Vaccines? Infect. Chemother. 2021, 53, 676–685. [Google Scholar] [CrossRef] [PubMed]
- von Lengerke, T.; Helmer, S.; Tomsic, I.; Pischke, C.R.; Wegwarth, O.; Kendel, F.; Härter, M. Education Level and Attitudes to Vaccination in the General Population: An Analysis of Representative Surveys Conducted by the German Federal Centre for Health Education, 2012 to 2018. Dtsch. Arztebl. Int. 2021, 118, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Tsai, H.H.; Huang, H.L.; Wang, Y.W.; Huang, C.H.; Liu, C.Y. Depression in nursing home residents and its correlation with meaning of family involvement and depression of family. Int. Psychogeriatr. 2023, 35, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Ong, H.S.; Fernandez, P.A.; Lim, H.K. Family engagement as part of managing patients with mental illness in primary care. Singap. Med. J. 2021, 62, 213. [Google Scholar] [CrossRef]
- Banbury, A.; Nancarrow, S.; Dart, J.; Gray, L.; Dodson, S.; Osborne, R.; Parkinson, L. Adding value to remote monitoring: Co-design of a health literacy intervention for older people with chronic disease delivered by telehealth—The telehealth literacy project. Patient Educ. Couns. 2020, 103, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef] [PubMed]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, J.W.; Layne, D.M.; Catchpole, K.; Evans, H.; Nemeth, L.S. A Qualitative Protocol to Examine Resilience Culture in Healthcare Teams during COVID-19. Healthcare 2021, 9, 1168. [Google Scholar] [CrossRef] [PubMed]
- Katz, P.R. An international perspective on long term care: Focus on nursing homes. J. Am. Med. Dir. Assoc. 2011, 12, 487–492.e1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Data | People in Need of Care (n = 285) | |
|---|---|---|
| Age (year), Median (Q1–Q3) | 84.0 (75.0–89.0) | |
| Missing Data | 2 (0.7%) | |
| Female sex, n (%) | 195 (68.4%) | |
| Missing Data | 0 (0.0%) | |
| Marital Status, n (%) | ||
| Not Married/Widowed | 222 (77.9%) | |
| Married | 63 (22.1%) | |
| Missing Data | 0 (0.0%) | |
| Ethnic Origin, n (%) | ||
| Caucasian | 283 (99.3%) | |
| Others | 1 (0.4%) | |
| Missing Data | 1 (0.4%) | |
| Education, n (%) | ||
| Non-academic degree | 225 (78.9%) | |
| Academic degree | 53 (18.6%) | |
| Missing Data | 7 (2.5%) | |
| Type of Care, n (%) | ||
| Inpatient | 198 (69.5%) | |
| Outpatient | 66 (23.2%) | |
| Missing Data | 21 (7.4%) | |
| Barthel Index Score, Median (Q1–Q3) | 75.0 (50.0–90.0) | |
| Missing Data | 2 (0.7%) | |
| Legal Representative, n (%) | ||
| Yes | 114 (40.0%) | |
| No | 161 (56.5%) | |
| Missing Data | 10 (3.5%) | |
| Scale | n (%) | Median (Q1–Q3) |
| Score PHQ-9 (4-Scale) | 282 (98.9%) | 4.0 (2.0–7.0) |
| PHQ-9, depression symptoms | ||
| No depression symptoms | 154 (54.0%) | |
| Mild depression symptoms | 86 (30.2%) | |
| Moderate depression symptoms | 30 (10.5%) | |
| Moderate to severe depression symptoms | 9 (3.2%) | |
| Severe depression symptoms | 3 (1.1%) | |
| Missing | 3 (1.1%) | |
| Clinical depression—PHQ-9 score ≥ 10 | 42 (14.7%) | |
| Score GAD-7 (4-Scale) | 277 (97.2%) | 1.0 (0.0–4.0) |
| GAD-7, general anxiety disorder | ||
| No anxiety disorder | 216 (75.8%) | |
| Mild anxiety disorder | 37 (13.0%) | |
| Moderate anxiety disorder | 18 (6.3%) | |
| Severe anxiety disorder | 6 (2.1%) | |
| Missing | 8 (2.8%) | |
| Clinical anxiety—GAD-7 score ≥ 10 | 24 (8.4%) | |
| Score HLS-EU-Q16 (2-Scale) | 285 (100.0%) | 14.0 (10.0–16.0) |
| HLS-EU-Q16, health literacy | ||
| Inadequate | 55 (19.3%) | |
| Problematic | 53 (18.6%) | |
| Sufficient | 177 (62.1%) | |
| People in Need of Care | Health Literacy HLS-EU_Q16 | ||
|---|---|---|---|
| Univariate (Odds Ratio (95%CI); p-Value) | Multivariate (Odds Ratio (95%CI); p-Value) | ||
| Martial Status | 2.0 (1.1–3.8); 0.023 * | 1.8 (0.9–3.5); 0.101 | |
| Academic Degree | 2.2 (1.1–4.3); 0.024 * | 3.1 (1.5–6.6); 0.003 ** | |
| Barthel Index Score | 0–30 | 0.4 (0.2–1.0); 0.051 | 0.5 (0.2–1.3); 0.151 |
| 35–80 | 0.4 (0.2–0.9); 0.020 * | 0.4 (0.2–1.0); 0.042 * | |
| 85–95 | 0.6 (0.3–1.4); 0.233 | 0.9 (0.4–2.1); 0.736 | |
| Legal Representative | 0.4 (0.2–0.9); <0.001 *** | 0.4 (0.2–0.6); <0.001 *** | |
| PHQ9 Clinical Cut-off ≥ 10 | 0.4 (0.2–0.7); <0.001 *** | 0.3 (0.2–0.6); 0.001 *** | |
| Sociodemographic Data | Healthcare Workers (HCWs) (n = 220) | |
|---|---|---|
| Age (year), Median (Q1–Q3) | 47.0 (34.0–56.0) | |
| Missing Data | 5 (2.3%) | |
| Female sex, n (%) | 174 (79.1%) | |
| Missing Data | 0 (0.0%) | |
| Marital Status, n (%) | ||
| Not Married/Widowed | 130 (59.1%) | |
| Married | 90 (40.9%) | |
| Missing Data | 0 (0.0%) | |
| Ethnic Origin, n (%) | ||
| Caucasian | 191 (86.8%) | |
| Others | 19 (8.6%) | |
| Missing Data | 10 (4.5%) | |
| Education, n (%) | ||
| Non-academic degree | 139 (63.2%) | |
| Academic degree | 79 (35.9%) | |
| Missing Data | 2 (0.9%) | |
| Type of Care, n (%) | ||
| Inpatient | 215 (97.7%) | |
| Outpatient | 5 (2.3%) | |
| Missing Data | 0 (0.0%) | |
| Function in the Facility, n (%) | ||
| Nursing Staff | 31 (14.1%) | |
| Elderly Care Staff | 143 (65.0%) | |
| Missing Data | 46 (20.9%) | |
| Employment Relationship, n (%) | ||
| Full-time employed | 169 (76.8%) | |
| Part-time employed | 49 (22.3%) | |
| Missing Data | 2 (0.9%) | |
| Care for COVID-19-infected patients, n (%) | 162 (73.6%) | |
| Missing Data | 12 (5.5%) | |
| Scale | n (%) | Median (Q1–Q3) |
| Score PHQ-9 (4-Scale) | 217 (98.6%) | 6.0 (3.0–10.0) |
| PHQ-9, depression Syndromes, No. (%) | ||
| No depression Syndromes | 84 (38.2%) | |
| Mild depression Syndromes | 71 (32.3%) | |
| Moderate depression Syndromes | 44 (20.0%) | |
| Moderate to severe depression Syndromes | 13 (5.9%) | |
| Severe depression Syndromes | 5 (2.3%) | |
| Missing | 3 (1.4%) | |
| Clinical depression—score ≥ 10 | 62 (28.2%) | |
| MBI total score (7-Scale) | ||
| Emotional Exhaustion (EE) | 204 (92.7%) | 15.5 (9.0–26.0) |
| Low | 106 (48.2%) | |
| Average | 51 (23.2%) | |
| High | 47 (21.4%) | |
| Missing | 16 (7.3%) | |
| Depersonalization (DP) | 217 (98.6%) | 5.0 (1.5–9.0) |
| Low | 131 (59.5%) | |
| Average | 48 (21.8%) | |
| High | 38 (17.3%) | |
| Missing | 3 (1.4%) | |
| Personal Accomplishment (PA) | 214 (97.3%) | 30.0 (23.0–36.0) |
| Low | 34 (15.5%) | |
| Average | 59 (26.8%) | |
| High | 121 (55.0%) | |
| Missing | 6 (2.7%) | |
| Vaccination readiness 5C (7-Scale) | ||
| Confidence | 219 (99.5%) | 4.0 (2.0–5.0) |
| Complacency | 219 (99.5%) | 1.0 (0.0–3.0) |
| Constraints | 218 (99.1%) | 0.0 (0.0–2.0) |
| Calculation | 219 (99.5%) | 4.0 (2.0–5.0) |
| Collective Responsibility | 197 (89.5%) | 0.0 (0.0–2.0) |
| Healthcare Workers (HCWs) | Univariate (Odds Ratio (95%CI); p-Value) | Multivariate (Odds Ratio (95%CI); p-Value) |
|---|---|---|
| Confidence | ||
| Current care for COVID-19-infected patients | 0.4 (0.2–0.9); 0.023 * | 0.3 (0.1–0.8); 0.016 * |
| PHQ9 Score | 0.9 (0.9–1.0); 0.006 ** | 0.9 (0.9–1.0); 0.066 |
| MBI—Depersonalization | 0.4 (0.2–0.8); 0.009 ** | 0.6 (0.3–1.2); 0.168 |
| MBI—Personal Accomplishment | 0.4 (0.2–1.0); 0.043 * | 0.6 (0.2–1.4); 0.203 |
| Complacency | ||
| MBI—Depersonalization | 2.9 (1.4–6.0); 0.005 ** | 2.9 (1.4–6.0); 0.005 ** |
| Constraints | ||
| Current care for COVID-19-infected patients | 2.6 (1.0–6.6); 0.046 * | 2.5 (0.9–7.4); 0.092 |
| PHQ9 Score | 1.1 (1.0–1.2); 0.008 ** | 1.1 (1.0–1.2); 0.023 * |
| MBI—Emotional Exhaustion | 2.4 (1.1–5.4); 0.028 * | 0.7 (0.2–2.0); 0.526 |
| MBI—Depersonalization | 3.9 (1.8–8.6); 0.001 *** | 3.7 (1.4–10.0); 0.010 ** |
| Calculation | ||
| Academic | 2.0 (1.1–3.4); 0.016 * | 1.9 (1.0–3.3); 0.034 * |
| MBI—Depersonalization | 0.5 (0.9–0.9); 0.033 * | 0.5 (0.3–1.1); 0.071 |
| MBI—Personal Accomplishment | 0.4 (0.2–1.0); 0.046 * | 0.5 (0.2–1.2); 0.114 |
| Collective Responsibility | ||
| MBI—Depersonalization | 4.5 (1.9–10.8); 0.001 *** | 4.5 (1.9–10.8); 0.001 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanftenberg, L.; Gschwendner, M.; Grass, A.; Rottenkolber, M.; Zöllinger, I.; Sebastiao, M.; Kühlein, T.; Hindenburg, D.; Gágyor, I.; Wildgruber, D.; et al. Associations of Mental Health Issues with Health Literacy and Vaccination Readiness against COVID-19 in Long-Term Care Facilities—A Cross-Sectional Analysis. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 432-446. https://doi.org/10.3390/ejihpe14030029
Sanftenberg L, Gschwendner M, Grass A, Rottenkolber M, Zöllinger I, Sebastiao M, Kühlein T, Hindenburg D, Gágyor I, Wildgruber D, et al. Associations of Mental Health Issues with Health Literacy and Vaccination Readiness against COVID-19 in Long-Term Care Facilities—A Cross-Sectional Analysis. European Journal of Investigation in Health, Psychology and Education. 2024; 14(3):432-446. https://doi.org/10.3390/ejihpe14030029
Chicago/Turabian StyleSanftenberg, Linda, Maresa Gschwendner, Andreas Grass, Marietta Rottenkolber, Isabel Zöllinger, Maria Sebastiao, Thomas Kühlein, Dagmar Hindenburg, Ildikó Gágyor, Domenika Wildgruber, and et al. 2024. "Associations of Mental Health Issues with Health Literacy and Vaccination Readiness against COVID-19 in Long-Term Care Facilities—A Cross-Sectional Analysis" European Journal of Investigation in Health, Psychology and Education 14, no. 3: 432-446. https://doi.org/10.3390/ejihpe14030029
APA StyleSanftenberg, L., Gschwendner, M., Grass, A., Rottenkolber, M., Zöllinger, I., Sebastiao, M., Kühlein, T., Hindenburg, D., Gágyor, I., Wildgruber, D., Hausen, A., Janke, C., Hoelscher, M., Teupser, D., Dreischulte, T., Gensichen, J., & on behalf of the BACOM Study Group. (2024). Associations of Mental Health Issues with Health Literacy and Vaccination Readiness against COVID-19 in Long-Term Care Facilities—A Cross-Sectional Analysis. European Journal of Investigation in Health, Psychology and Education, 14(3), 432-446. https://doi.org/10.3390/ejihpe14030029