

Amyloidosis Cutis Dyschromica in a 16-Year-Old Filipino Girl: A Case Report

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
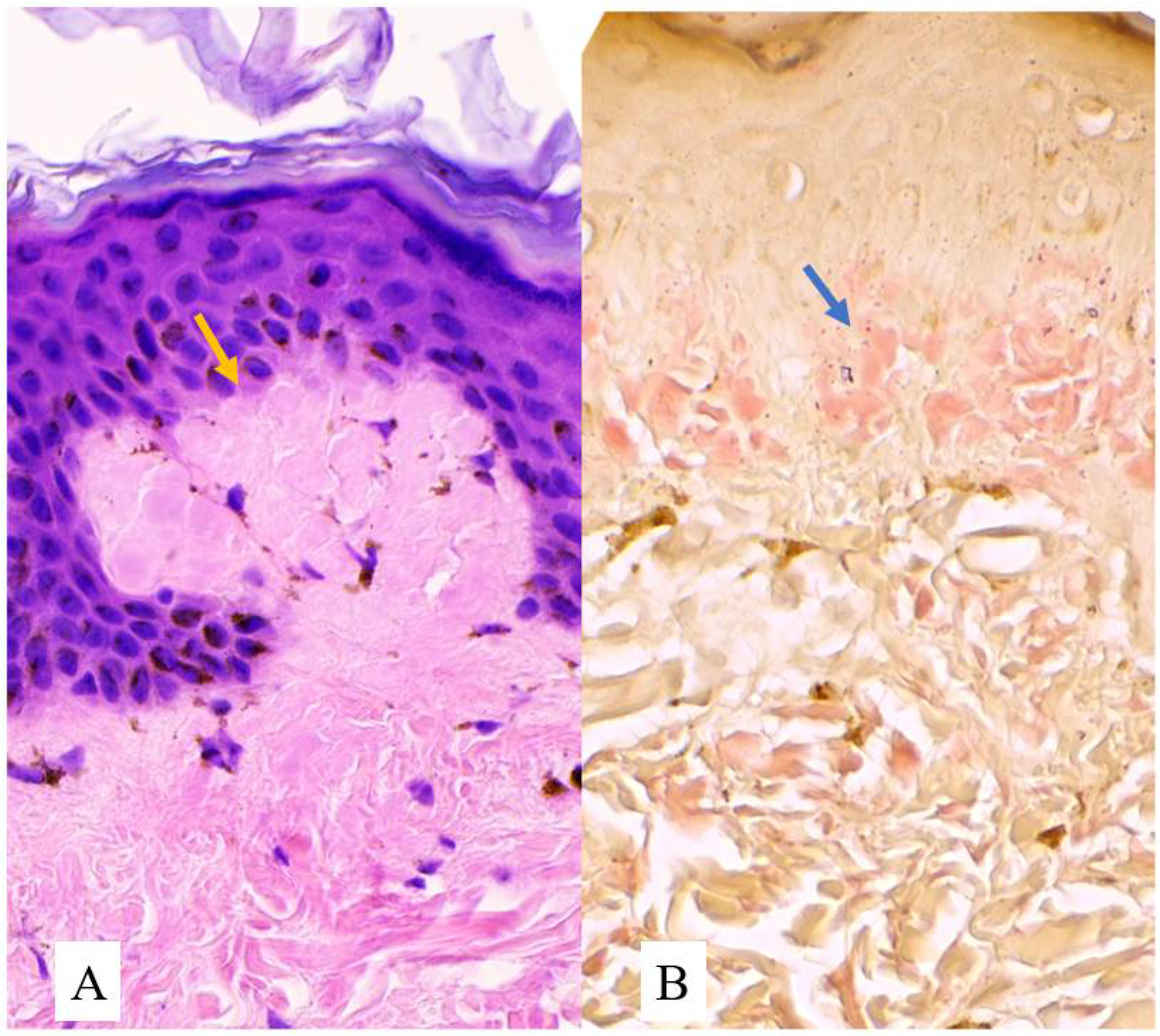
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morishima, T. A clinical variety of localized cutaneous amyloidosis characterized by dyschromia (amyloidosis cutis dyschromica). Jpn. J. Dermatol. B 1970, 3, 43–52. [Google Scholar]
- Moriwaki, S.; Nishigori, C.; Horiguchi, Y.; Imamura, S.; Toda, K.; Takebe, H. Amyloidosis cutis dyschromica: DNA repair reduction in the cellular response to UV light. Arch. Dermatol. 1992, 128, 966–970. [Google Scholar] [CrossRef] [PubMed]
- Sakhiya, J.; Sakhiya, D.; Patel, M.; Daruwala, F. Amyloidosis Cutis Dyschromica, A Rare Subtype of Primary Cutaneous Amyloidosis: Case Report and Literature Review. Indian Dermatol. Online J. 2021, 12, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Tiwary, A.K.; Mishra, D.K.; Lal, Y.A.; Chaudhary, S.S. Amyloidosis cutis dyschromica: A case report. J. Pak. Assoc. Dermatol. 2015, 25, 334–336. [Google Scholar]
- Mahon, C.; Oliver, F.; Purvis, D.; Agnew, K. Amyloidosis cutis dyschromica in two siblings and review of the epidemiology, clinical features and management in 48 cases. Australas. J. Dermatol. 2016, 57, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhong, Z.; Wang, X.; Zheng, L.; Wang, Y.; Wang, S.; Liu, S.; Li, H.; Guo, Z.; Gao, M. Case Report: Amyloidosis Cutis Dyschromica: Dermoscopy and Reflectance Confocal Microscopy and Gene Mutation Analysis of a Chinese Pedigree. Front. Med. 2021, 8, 774266. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, F.; Ebrahimzadeh, M.; Moghimi, M.; Noorbala, M.T. Familial amyloidosis cutis dyschromica: A case report. Acta Med. Iran. 2014, 52, 163–165. [Google Scholar] [PubMed]
- Kurian, S.S.; Rai, R.; Madhukar, S.T. Amyloidosis cutis dyschromica. Indian Dermatol. Online J. 2013, 4, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Onoufriadis, A.; Hsu, C.K.; Eide, C.R.; Nanda, A.; Orchard, G.E.; Tomita, K.; Sheriff, A.; Scott, W.; Tierney, C.; Lee, J.Y.; et al. Semidominant GPNMB Mutations in Amyloidosis Cutis Dyschromica. J. Investig. Dermatol. 2019, 139, 2550–2554.e9. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.F.; Lin, S.P.; Chiang, C.P.; Wu, Y.H.; H’ng, W.S.; Chang, C.P.; Chen, Y.T.; Wu, J.Y. Loss of GPNMB Causes Autosomal-Recessive Amyloidosis Cutis Dyschromica in Humans. Am. J. Hum. Genet. 2018, 102, 219–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, J.; Fang, H.; Yao, H. Amyloidosis cutis dyschromica. Orphanet J. Rare Dis. 2012, 7, 95. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bautista, F.E.R.; Marte-Jimenez, M.M.S.; Jamora, M.J.J. Amyloidosis Cutis Dyschromica in a 16-Year-Old Filipino Girl: A Case Report. Dermatopathology 2023, 10, 20-24. https://doi.org/10.3390/dermatopathology10010002
Bautista FER, Marte-Jimenez MMS, Jamora MJJ. Amyloidosis Cutis Dyschromica in a 16-Year-Old Filipino Girl: A Case Report. Dermatopathology. 2023; 10(1):20-24. https://doi.org/10.3390/dermatopathology10010002
Chicago/Turabian StyleBautista, Fendi EJ R., Marcia Marie S. Marte-Jimenez, and Maria Jasmin J. Jamora. 2023. "Amyloidosis Cutis Dyschromica in a 16-Year-Old Filipino Girl: A Case Report" Dermatopathology 10, no. 1: 20-24. https://doi.org/10.3390/dermatopathology10010002
APA StyleBautista, F. E. R., Marte-Jimenez, M. M. S., & Jamora, M. J. J. (2023). Amyloidosis Cutis Dyschromica in a 16-Year-Old Filipino Girl: A Case Report. Dermatopathology, 10(1), 20-24. https://doi.org/10.3390/dermatopathology10010002