
Evaluation of Melanocyte Loss in Mycosis Fungoides Using SOX10 Immunohistochemistry



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bagherani, N.; Smoller, B.R. An overview of cutaneous T cell lymphomas. F1000Res 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Hristov, A.C.; Tejasvi, T.; Wilcox, R.A. Mycosis fungoides and Sezary syndrome: 2019 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2019, 94, 1027–1041. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, A.E.; Patel, K.; Goyal, K.; O’Leary, D.; Rubin, N.; Pearson, D.; Bohjanen, K.; Goyal, A. Mycosis fungoides: Developments in incidence, treatment and survival. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Smoller, B.R. Mycosis fungoides: What do/do not we know? J. Cutan. Pathol. 2008, 35 (Suppl. 2), 35–39. [Google Scholar] [CrossRef] [PubMed]
- Agar, N.S.; Wedgeworth, E.; Crichton, S.; Mitchell, T.J.; Cox, M.; Ferreira, S.; Robson, A.; Calonje, E.; Stefanato, C.M.; Wain, E.M.; et al. Survival outcomes and prognostic factors in mycosis fungoides/Sezary syndrome: Validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J. Clin. Oncol. 2010, 28, 4730–4739. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Lacarrubba, F.; Verzi, A.E.; Micali, G.; Caltabiano, R. Confocal microscopy features of patch-stage mycosis fungoides and their correlation with horizontal histopathological sections. A case series. J. Cutan. Pathol. 2019, 46, 163–165. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, S.A.; Cicek, D.; Demir, B. Dermoscopy in differential diagnosis of inflammatory dermatoses and mycosis fungoides. Int. J. Dermatol. 2020, 59, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Hodak, E.; Amitay-Laish, I. Mycosis fungoides: A great imitator. Clin. Dermatol. 2019, 37, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Castano, E.; Glick, S.; Wolgast, L.; Naeem, R.; Sunkara, J.; Elston, D.; Jacobson, M. Hypopigmented mycosis fungoides in childhood and adolescence: A long-term retrospective study. J. Cutan. Pathol. 2013, 40, 924–934. [Google Scholar] [CrossRef] [PubMed]
- Rodney, I.J.; Kindred, C.; Angra, K.; Qutub, O.N.; Villanueva, A.R.; Halder, R.M. Hypopigmented mycosis fungoides: A retrospective clinicohistopathologic study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Liu, Z.; Liu, J.; Liu, Y.; Zhang, W.; Zhang, Y. Mycosis Fungoides and Variants of Mycosis Fungoides: A Retrospective Study of 93 Patients in a Chinese Population at a Single Center. Ann. Dermatol. 2020, 32, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Mollaaghababa, R.; Pavan, W.J. The importance of having your SOX on: Role of SOX10 in the development of neural crest-derived melanocytes and glia. Oncogene 2003, 22, 3024–3034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shakhova, O.; Zingg, D.; Schaefer, S.M.; Hari, L.; Civenni, G.; Blunschi, J.; Claudinot, S.; Okoniewski, M.; Beermann, F.; Mihic-Probst, D.; et al. Sox10 promotes the formation and maintenance of giant congenital naevi and melanoma. Nat. Cell Biol. 2012, 14, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Furlan, F.C.; de Paula Pereira, B.A.; da Silva, L.F.; Sanches, J.A. Loss of melanocytes in hypopigmented mycosis fungoides: A study of 18 patients. J. Cutan. Pathol. 2014, 41, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Pimpinelli, N.; Olsen, E.A.; Santucci, M.; Vonderheid, E.; Haeffner, A.C.; Stevens, S.; Burg, G.; Cerroni, L.; Dreno, B.; Glusac, E.; et al. Defining early mycosis fungoides. J. Am. Acad. Dermatol. 2005, 53, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Amorim, G.M.; Niemeyer-Corbellini, J.P.; Quintella, D.C.; Cuzzi, T.; Ramos, E.S.M. Hypopigmented mycosis fungoides: A 20-case retrospective series. Int. J. Dermatol. 2018, 57, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Martinez Villarreal, A.; Gantchev, J.; Lagace, F.; Barolet, A.; Sasseville, D.; Odum, N.; Charli-Joseph, Y.V.; Hernandez Salazar, A.; Litvinov, I.V. Hypopigmented Mycosis Fungoides: Loss of Pigmentation Reflects Antitumor Immune Response in Young Patients. Cancers 2020, 12, 2007. [Google Scholar] [CrossRef] [PubMed]
- Chuang, G.S.; Wasserman, D.I.; Byers, H.R.; Demierre, M.F. Hypopigmented T-cell dyscrasia evolving to hypopigmented mycosis fungoides during etanercept therapy. J. Am. Acad. Dermatol. 2008, 59, S121–S122. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Escala, M.E.; Posligua, A.L.; Wickless, H.; Rutherford, A.; Sable, K.A.; Rubio-Gonzalez, B.; Zhou, X.A.; Kaplan, J.B.; Pro, B.; Choi, J.; et al. Progression of undiagnosed cutaneous lymphoma after anti-tumor necrosis factor-alpha therapy. J. Am. Acad. Dermatol. 2018, 78, 1068–1076. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Results | Hypopigmented | Conventional | All |
|---|---|---|---|
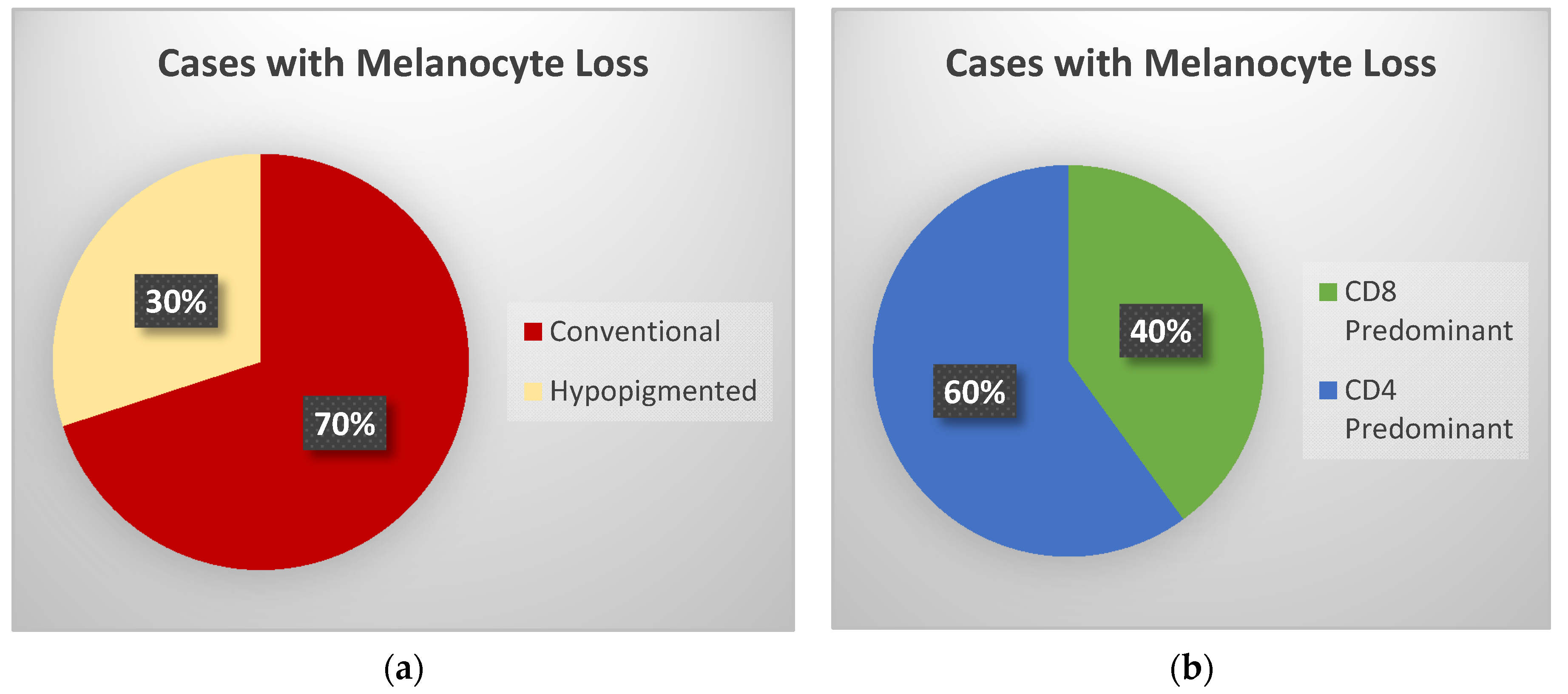
| Melanocyte loss | 3 (43%) | 7 (54%) | 10 (50%) |
| CD4 predominant | 4 (57%) | 9 (69%) | 13 (65%) |
| Ethnicity non-Caucasian | 6 (86%) | 2 (15%) | 8 (40%) |
| Gender (female) | 5 (71%) | 4 (31%) | 9 (45%) |
| Age (Average) | 43 | 54 | 50 |
| Range | 30–62 | 15–86 | 15–86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barron, C.R.; Smoller, B.R. Evaluation of Melanocyte Loss in Mycosis Fungoides Using SOX10 Immunohistochemistry. Dermatopathology 2021, 8, 277-284. https://doi.org/10.3390/dermatopathology8030034
Barron CR, Smoller BR. Evaluation of Melanocyte Loss in Mycosis Fungoides Using SOX10 Immunohistochemistry. Dermatopathology. 2021; 8(3):277-284. https://doi.org/10.3390/dermatopathology8030034
Chicago/Turabian StyleBarron, Cynthia Reyes, and Bruce R. Smoller. 2021. "Evaluation of Melanocyte Loss in Mycosis Fungoides Using SOX10 Immunohistochemistry" Dermatopathology 8, no. 3: 277-284. https://doi.org/10.3390/dermatopathology8030034
APA StyleBarron, C. R., & Smoller, B. R. (2021). Evaluation of Melanocyte Loss in Mycosis Fungoides Using SOX10 Immunohistochemistry. Dermatopathology, 8(3), 277-284. https://doi.org/10.3390/dermatopathology8030034