1. Introduction
Growing evidence suggests that the use of blue light-emitting digital devices can interfere with human tissue at the level of biological ocular structures [
1,
2]. We all have some knowledge of UV ray exposure risks. This radiation (UVA and UVB) easily passes through the atmosphere and can cause damage to the skin and eyes. However, UV radiation is absorbed by the frontal structures of the eye (cornea and lens) and does not reach the retina. This is a key difference between UV light and blue light risks—blue light passes through the sensitive tissues of the human eye [
3].
Publications on blue light emitted by digital devices state that the risk of blue light from these digital devices and similar devices with prolonged exposure is below safe viewing limits; therefore, blue light should not cause structural changes to ocular tissues [
4]. Blue light can have both a negative and positive impact on human eyes. According to UNE EN/IEC 62471, the standard classification for photobiological safety, blue radiation is contained between the ranges of 380–495 nm [
5]. This range of wavelengths is relevant for adequate vision performance and the balance of some physiological processes. Human vision evolved with sunlight, the largest natural source of blue radiation with the shortest wavelength and highest frequency within the visible spectrum [
6].
Digital devices that use LED technology, as well as other artificial light sources, expose their users to artificial digital blue radiation on a daily basis. This can be potentially harmful to the human eye due to the proximity of the ultraviolet spectrum, particularly to the retina, due to its higher energy wavelengths and high potential to alter ocular tissues [
7]. However, chronic exposure over a lifetime can have a cumulative, long-term degenerative impact, which should continue to be discussed [
8]. New data and new devices should be updated.
Brightness, color, pattern, and time of exposure to light can interfere with and alter cellular functions. Most current devices are frequently used at night for many hours, which can negatively affect users’ sleep and eyes [
9,
10,
11,
12].
Not all wavelengths corresponding to different colors have the same effect on human eyes. There is evidence showing the probability of a greater impact of light with a wavelength up to 495 nm, where many older devices have been shown to have peaks, specifically at these wavelengths [
2].
Digital devices have replaced paper and other non-digital formats and have also changed traditional low-intensity and reflected lighting. However, these new ways of viewing have very different light ranges, naturally having biological effects on users. This problem is significant when we observe that, across Europe, 51% of all devices are desktops, followed by smartphones with 46%, and the use of mobile data in Europe has increased by 569% since 2016 [
13].
Digital devices with Internet access still have several possibilities of use, such as access to browsers, online games, social networks, or digital books, with evidence in the performance of several of these tasks at the same time.
Until the end of the 20th century, most light measurement studies quantified light stimuli in Lux, the photopic illuminance unit. The most frequent resource was the luxmeter, due to its easy access and because it is a very popular device for measuring lighting and photography. However, this measurement method was not sufficient to provide complete data [
14]. This experimental work arises from the need to measure, register, and update data referring to the daily use of digital devices, quantifying their illuminance and irradiance values.
2. Objectives
Considering background references [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12], this new experimental work proposes the light measurement, or more precisely, obtaining the spectral profile of three contemporary devices that are widely used daily. In particular, it was decided to include three categories of devices: a tablet, a smartphone, and a laptop computer. Comparative tests were carried out between the three devices’ categories using text and a game display.
The visible blue light hazard was defined by the CIE/IEC (62778:2014). Known as human photopic photoreceptor responses, namely, S cones (λ = 420 nm), M cones (λ = 530 nm), and L cones (λ = 560 nm), the danger of exposure to blue light occurs at 420 nm, which corresponds to the maximum absorption of A2E. The isomer A2E (
N-retinylidene-
N-retinylethanolamine) is one of the bis-retinoid constituents of retinal pigment epithelium lipofuscin. For all lipofuscin chromophores, there is maximum absorption in the visible range of the spectrum (A2E: λ
max = 338 nm), and the isomer A2E is the unique constituent of retinal pigment epithelial cells [
15]. The exposure would cause changes in the retinal pigment epithelium and the death of photoreceptor cells [
16].
With the objective of obtaining data to analyze the risk factors, the spectral profile of each category in the automatic adjustment was analyzed. Later, we analyzed the same sources with blue light-blocking lenses from Carl Zeiss, Shamir, Hoya, and Novacel. Knowing the response peak for each of the five photopigments in the human eye [
17], the purpose of this experimental work was to provide reliable reference data for each device, compare them with each other, and extrapolate these data for eventual complementary studies.
As mentioned before, we set out to measure the irradiance and spectral profiles of three of the most popular and contemporary devices to compare their emissions. Some of the frequent uses of these devices are reading or playing games. We measured and compared the light output of the same screens with the game and with the text.
Since the devices have screen lighting conditions, we tried to test the real effect of these adjustments on the spectral profile using two strategies:
- 1
Acquisition of emission from light-emitting screens in automatic mode (without manually interfering with the brightness or intensity settings of the devices).
- 2
Using the same methodology, lenses from the brands Carl Zeiss, Shamir, Hoya, and Novacel were placed on the device-optic fiber interface, all currently available with blue blocking.
The irradiance of screens with different configurations at a wavelength of 450 nm was also measured. Devices with a 0% brightness were equivalent to being turned off, so screens with a brightness of 100%, 75%, 50%, and 25% were measured on a white background. In this way, we expect to obtain the differences between the various configurations and the maximum value for the blue light peaks, as well as the subsequent measurements.
3. Materials and Methods
Three categories of the most popular brand of devices in 2022 (iPad Pro
®, iPhone 12 mini
®, Macbook Pro
®, Apple Inc., Cupertino, CA, USA) were chosen, according to the International Data Corporation (IDC) [
18,
19]. The data for each device was obtained from the manufacturer’s technical specifications, and the light measurements were acquired at a distance from the source as close as possible, starting from zero. The characteristics of the devices can be consulted in
Table 1.
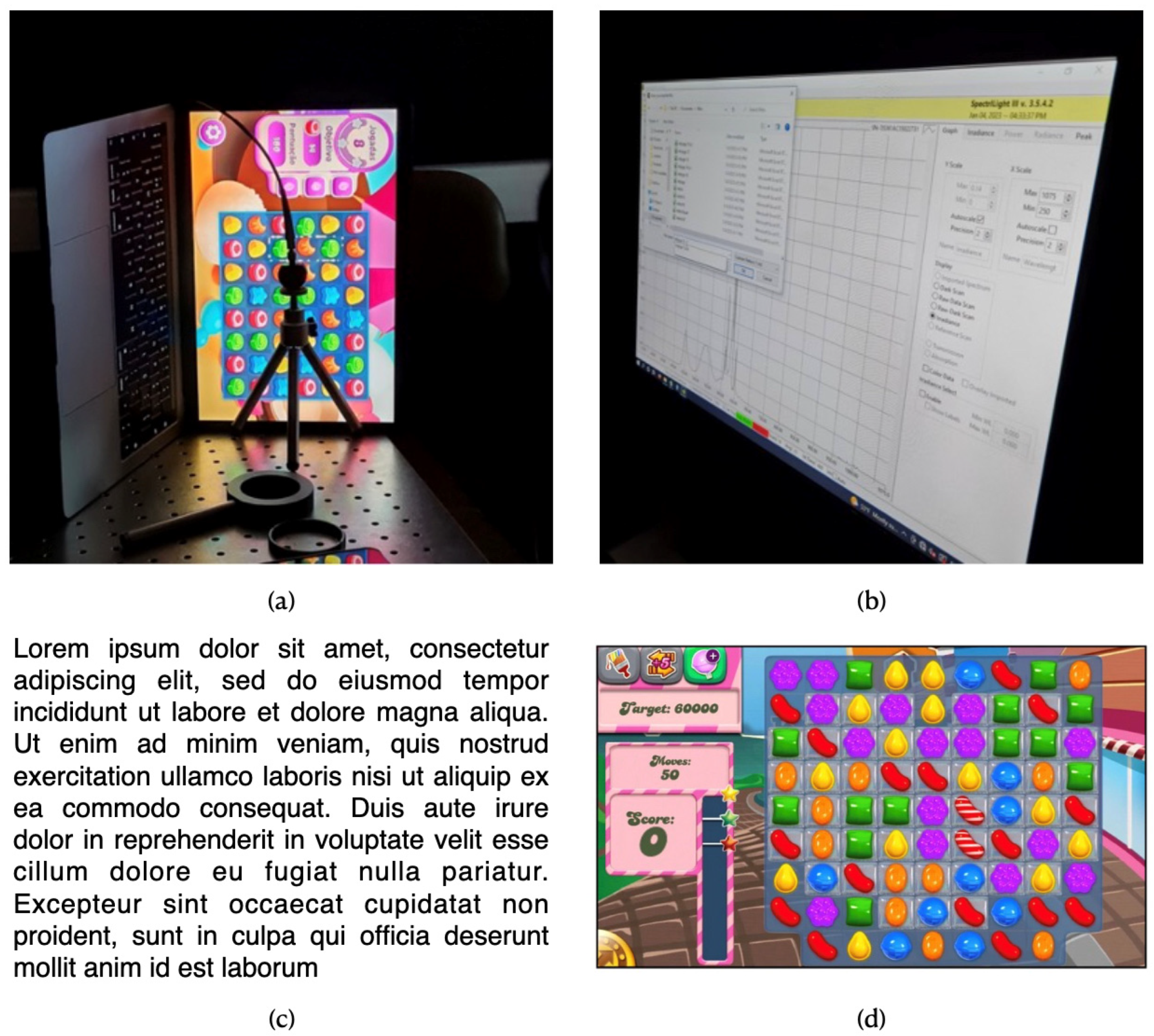
Any of the selected devices can be used at night in an unlit, completely darkened room. For this reason, the first measurements were carried out in a room without lighting, and the brightness levels were not adjusted, leaving all devices with the configuration in automatic mode. For each device, the illuminance and irradiance were measured with the respective exact spectral power distribution (SPD) with the calibrated spectroradiometer (SpectraLight III, ILT 950, International Light Technologies, Inc., Peabody, MA, USA). The setup and measurement output are shown in
Figure 1.
Regarding the first strategy mentioned in
Section 2, the measurements used similar images on all devices, both for the text and for the popular game (
Figure 1), while the illuminance and irradiance measurements were recorded with the spectroradiometer.
In the second strategy, we tested blue-blocking lenses, all with the same refractive index (n = 1.5), with a neutral refractive power (p = 00.00 D), and with the following commercial names: Blue Guard® (Carl Zeiss, Aalen, Germany), Blue Zero® (Shamir, Vilar, Portugal), Blue Control® (Hoya, Amsterdam, The Netherlands), and Blue Clear® (Novacel, La Moiserie, France). Each lens was placed between the tested device and the spectroradiometer, and the first strategy measurements were repeated using the same protocol, but at this time with blue light-blocking lenses between the different sources and the spectroradiometer.
The evaluated lenses’ manufacturers advertise the blocking of potentially harmful light, blue-violet light, up to around 40%. They have little disagreement with each other on what percentage of blue light should be transmitted. By absorbing the percentage of blue from 400 nm to 455 nm, lenses maintain high transparency above 455 nm, and manufacturers refer to this important factor related to the circadian rhythm [
20,
21,
22,
23]. Despite this information, there is no consensus regarding ophthalmic lenses with blue light blocking. An article published by the Cochrane Database of Systematic Reviews analyzed data from several previous trials that studied how blue light-filtering lenses affect visual fatigue, sleep quality, and eye health. The authors revealed that the results were inconclusive and that the lenses may not alleviate symptoms of eye strain during the use of digital devices, further stating that, based on the clinical trials reviewed, there is little or no effect on visual performance, macular health, or sleep in adult populations [
24].
4. Results
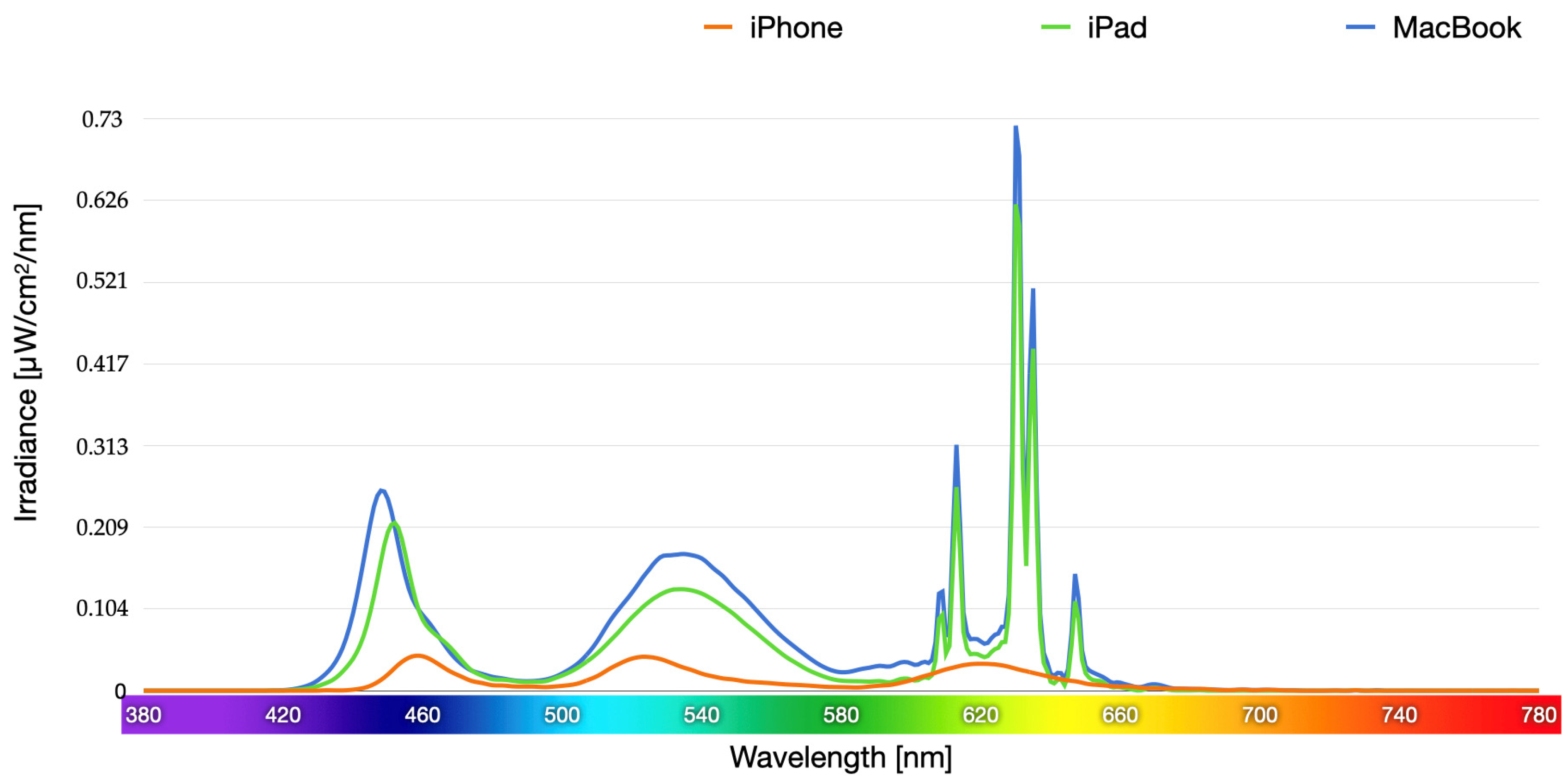
Figure 2 and
Figure 3 show the emission spectrum of the three devices’ categories, comparing them to each other, in μW/cm
2/nm (spectral irradiance). All devices showed very similar enhanced short-wavelength blue peaks when displaying the same text (445–455 nm). The spectral profile of the Candy Crush
® game was also very similar; text emissions, however, showed greater intensity.
The first strategic measurements were repeated using the same protocol, but this time with blue light-blocking lenses between the different sources and the spectrodiometer. All tested blue-blocking lenses reduced short-wavelength light emissions for the smartphone category (
Figure 4), the tablet category (
Figure 5), and the computer category (
Figure 6). After the graphical presentation of the spectral irradiance (μW/cm
2/nm), we converted to irradiance in mW/cm
2, facilitating analysis, comparison, and extrapolation with the luminaires or solar radiation irradiance.
Blue blocking lenses selectively reduce light at short wavelengths of transmission but do not interfere with medium and long wavelengths of transmission, and this selective blocking can reduce the contrast of some objects.
The generation to which the tested lenses belong was designed to limit exposure to potentially harmful blue light, and it proved to be effective in doing so. However, its use may have some undesirable effects, such as changes in color perception [
25] and reduced contrast [
26]. A recent study demonstrated that commercially available blue light-blocking lenses effectively attenuate exposure to blue light but can reduce image contrast, which can also significantly alter the perceived speed of objects. These data regarding selective light blocking may have consequences for visual function and the perception of objects [
27].
Decreasing the phone’s brightness decreases the phone’s lighting, making it difficult to view images, which makes most users use their devices in automatic mode. However, the intensity where the blue light peak (450 nm) occurs was compared instead of the entire range of blue light emitted by the devices.
Decreasing brightness was also effective in reducing the intensity of blue light. Decreasing brightness from 100% to 50% resulted in a decrease of 83.7%, 70.3%, and 74.6% for the iPhone 12 mini, iPad Pro, and Macbook Pro, respectively (
Figure 7).
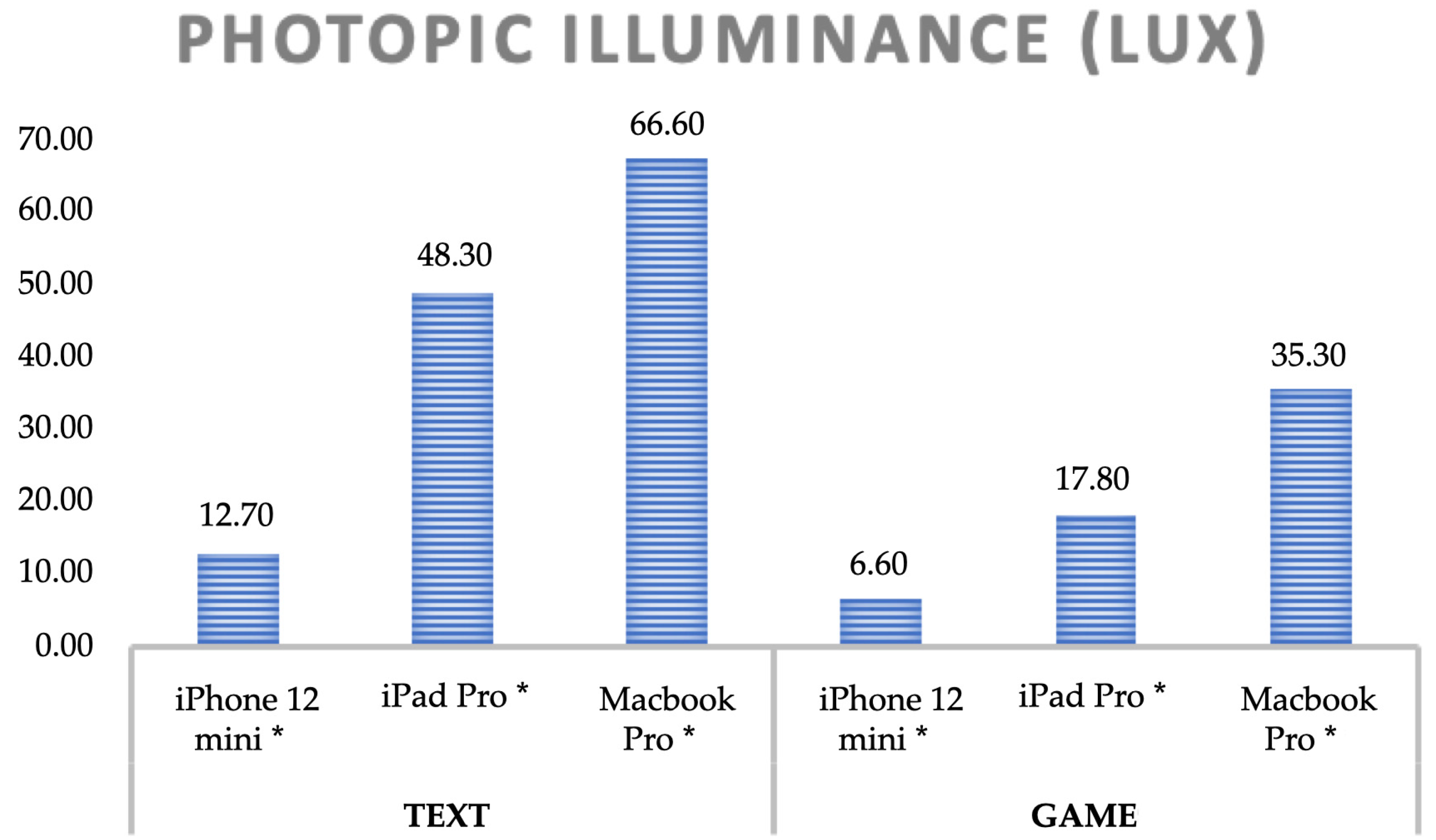
Finally, the irradiance for each of the five photopigments of the human eye is presented according to the values of the International Commission on Illumination (CIE) for the two measurements: the text and the game (
Figure 8). The spectral distribution for each human retinal photoreceptor, its irradiance and illuminance, and the spectral peaks in the several emitting devices can be easily quantified and compared for the two proposed display conditions (
Figure 8 and
Figure 9).
Melanopsin, the structural photopigment of ipRGC cells, is more closely related to non-image photoreceptor opsins than to rod and cone opsins [
27]. Melanopsin phototransduction depends on irradiance, a fundamental light response of ipRGCs, even at low light levels, requiring only 1 lux or less to suppress melatonin in humans [
28].
The efficiency of melanopsin is comparable to that of rod and cone opsins. However, melanopsin photoreception is much less sensitive than that of rods or cones [
29]. This stimulus combination causes circadian and neurophysiological responses into non-image-forming responses to light [
30,
31].
Physiological responses to light signals are defined by the melanopsin-driven phototransduction mechanism of ipRGC and rods and cones. Each of these light-detection mechanisms has a distinct spectral sensitivity. Rhodopsin is the rod photopigment with peak sensitivity (λ
max) at 495 nm in all mammalian species. Cones have distinct spectra. The cyanolable S-cone opsin has sensitive peaks to wavelengths up to 420 nm; the M cones contain chlorolabe, with a peak sensitivity of 530 nm; and the L cones contain a red-sensitive opsin (erythrolable), with a maximum peak of 560 nm [
32]. However, this radiation does not reach the retina without passing through the refractive media of the human eyes. The cornea, aqueous humor, and vitreous are the ocular refractive media, permeable to wavelengths between 300 nm and 400 nm, but the lens absorbs the most energetic visible light and therefore blocks and protects the retina from potential damage caused by exposure to blue light. The lens blocks most UV radiation between 300 nm and 420 nm, reducing the risk of retinal damage from digital devices [
8]. The aging of the lens will result in a lower incidence of blue light on the retina due to it turning yellow. This factor will result in a reduction in the activation of retinal ganglion cells sensitive to blue light, which mediate non-visual responses to light, such as the pupillary light reflex or the suppression of melatonin, and a consequent change in the circadian cycle.
In the ocular tissues, three main types of damage caused by light are generally known:
Photomechanical: caused by high radiation in short periods of exposure due to the impossibility of dissipating the heat generated;
Photothermal: produced by the light energy transfer to the retina when irradiation is high enough to increase the temperature above the ambient level of the retina. Radiation triggers locally limited heating of tissues, which can result in protein denaturation, loss of cellular integrity, and inflammatory responses;
Photochemical: produced when light energy induces a photooxidative and toxic response in retinal cells.
One of the main differences between photochemical damage and other damage is their light-inducing sources [
33]. Thermal and photomechanical damage only occurs due to coherent light sources, for example, lasers. Photochemical damage is produced by exposure to solar radiation and, in the long term, can be produced by radiation from digital devices. From this perspective, the blue light emissions of the measured devices did not show high values that could be of concern for eye diseases, but the impact of blue light on ocular structures is not an isolated phenomenon and a multidisciplinary approach can contribute to improving research into the safety of artificial blue light and digital devices [
34].
The blue light range is between 380 nm and 495 nm and can be essentially divided into two ranges: blue-violet light (380–455 nm) and turquoise light (455–495 nm). Turquoise blue light helps maintain and regulate memory, cognition, humor, and hormonal balance and synchronize our biological rhythms (the circadian cycle), but blue-violet light can pose a potential risk to the eyes of digital device users [
35]. Thus, the spectral profiles of blue light were measured in the different categories of digital devices with the presentation of the text and the game (
Figure 10).
To provide data on the negative impact and risks to eye and visual health and the environment, based on the International Commission on Non-Ionizing Radiation Protection (IC-NIRP), it can be stated that data collected from all devices present low risks when using LED devices as they fall into groups RG0 (no risk) and RG1 (low risk), as we can see in
Table 2 [
36].
However, consecutive and cumulative exposure to digital devices can lead to potential long-term sequelae, raising the question: could exposure even with low irradiance, but during daily periods throughout life, be harmful to ocular health?
5. Analysis
In this study, we evaluated the screens’ irradiance for three digital device categories in different configurations and the ability of ophthalmic lenses to block blue light. Although decreasing glare intensity provides a percentage reduction in blue light intensity, its effect on eye health is still unknown. It is clear that the categories of devices studied are the only sources of blue light that we look at directly. As we spend more and more time exposed to these digital devices, it is important to try to understand how blue light can impact our health and well-being.
We can see the spectral emission data obtained from the three categories of devices in
Figure 8. It shows that they all have peaks in the blue wavelength, which are very similar for the text and for the game display (445–455 nm). However, the spectral profile in the text display revealed greater intensity than in the game display. The tested ophthalmic lenses slightly reduced blue-wavelength light emissions. In the text, the emission peaks in the blue range, at 450 nm, went from 0.00003 mW/cm
2/nm on the iPhone
®, from 0.00022 mW/cm
2/nm on the iPad Pro
®, and from 0.00021 mW/cm
2/nm on the Macbook Pro
® to an average value of all tested lenses of 0.00002 mW/cm
2/nm, 0.00019 mW/cm
2/nm, and 0.00020 mW/cm
2/nm, respectively. On the game display, the emission peaks in the blue range, at 450 nm, went from 0.00002 mW/cm
2/nm on the iPhone
®, from 0.00023 mW/cm
2/nm on the iPad Pro
®, and from 0.00024 mW/cm
2/nm on the Macbook Pro
®, to an average of all tested lenses of 0.000015 mW/cm
2/nm, 0.00015 mW/cm
2/nm, and 0.00013 mW/cm
2/nm, respectively (
Figure 2 to
Figure 6). Studies carried out with RPE cells that were exposed to blue light for 8 h a day at intensities of 0.6 to 0.1 mW/cm
2 (the intensity range where some of the digital devices studied are located) showed that exposure to blue light produced effects on the cell layers of the RPE. One of these effects was a decrease in the number of cells, demonstrating a possible relationship between the use of personal digital devices and damage to the retina [
37].
The spectral irradiance showed that the emissions from the three categories of digital devices are much lower than those received by the sun in the atmosphere, as we can see in
Table 3. It is important to consider that the irradiances presented in this study correspond to the emissions from the screens of electronic devices at 450 nm. Spectral irradiances were integrated from 380 nm to 500 nm to determine the total emissions of devices in each device category.
Considering the entire spectrum of visible light, the images combine the three primary colors, reducing the amount of blue light in isolation but increasing emissions at longer wavelengths that also contribute to eye risks.
The differences observed between the devices are related to their particular characteristics as well as the use of blue light-blocking lenses that reduce the emission of blue light. These irradiances are about three orders of magnitude lower than those estimated from the solar spectrum in both clear and cloudy conditions. Our results agree with other previous studies in which the emissions of different electronic devices were measured and evaluated for their potential blue light hazards. [
39]
Devices with manually adjusted brightness of 100%, 75%, 50%, and 25% on a white background obtained emission peaks in the blue range, at 450 nm, of 0.0004 mW/cm2/nm (at 100% brightness), 0.00018 mW/cm2/nm (at 75% brightness), 0.00006 mW/cm2/nm (at 50% brightness), and 0.00003 mW/cm2/nm (at 25% brightness) on iPhone®, 0.00195 mW/cm2/nm (at 100% brightness), 0.00135 mW/cm2/nm (at 75% brightness), 0.00059 mW/cm2/nm (at 50% brightness) and 0.00017 mW/cm2/nm (at 25% brightness) on iPad Pro® and 0.0017 mW/cm2/nm (at 100% brightness), 0.00094 mW/cm2/nm (at 75% brightness), 0.00043 mW/cm2/nm (at 50% brightness) and 0.00013 mW/cm2/nm (at 25% brightness) on the Macbook Pro®. This way, we obtained the maximum emission value, at 450 nm, and other reference values since the minimum is equivalent to digital equipment being turned off.
Background evidence is divided regarding the effectiveness of blue light-blocking lenses. While some say that ophthalmic lenses can be a resource and have been shown to effectively attenuate blue light exposure, impacting circadian rhythm and photoreceptor function [
40], others state they find no evidence to support the use of blue light-blocking lenses to improve visual performance, sleep quality, alleviate eye strain, or maintain macular health [
32]. However, we can state that lenses have been shown to effectively attenuate the spectral emission of blue light, although this selective blocking of light may have consequences for visual function and color perception. Therefore, blue light-blocking lenses may have advantages despite altering the image’s appearance during use. They also decrease digital devices’ lighting, causing changes to the image displayed on the screen but reducing the intensity of blue light. Tested lenses are not expected to cause significant changes in daytime conditions but may slightly affect performance in conditions where the overall luminance is considerably lower. As blue-blocking ophthalmic lenses incorporate filters that block, in addition to blue light, harmful ultraviolet radiation protection, we can affirm that long-term use can have an impact on protecting against possible damage to the functional ocular tissues, particularly UV radiation from sunlight. However, there are no scientific evidence that lenses are useful to protect human eyes exposed to blue light from smartphones, tablets, or computer monitors, especially at night, despite the reduction in emissions under analysis [
25]. The blue light-blocking filter feature demonstrates, at wavelengths above 460 nm, that there is no effect on the behavior of the RPE cells. In contrast, blue light, at wavelengths between 400 nm and 460 nm, was responsible for the changes observed in exposed RPE cells [
41].
It is necessary to consider the blue light saturation in ocular structures and extrapolate from research results. To date, modeling studies have provided information on the possible long-term effects of repeated exposure to artificial blue light, but further experimental research will be needed to add knowledge in this area.
In our opinion, it would be of the utmost importance for research to establish a standard approach for measuring and recording the characteristics of light sources. The potential long-term effects of artificial blue light exposure will be better understood with a quantification of light exposure and consequent indexes of ocular health, circadian function, and other metrics of interest.
The prolonged exposure to blue light implications and the quick pace of technological developments can affect many physiological processes, with numerous implications beyond the safety of digital devices. Therefore, good practices are recommended for using digital devices rich in blue light, such as moderate use or interruption of use at night.
As the contribution of light peaking at 555 nm becomes clearer, it is also important to understand how changing the spectral composition of light can affect its therapeutic effects. New insights into artificial blue light may support safer and more effective light therapy and prevention practices. The effort to understand and study the safety of artificial blue light, its potential risks, and its benefits must be encouraged.
Decreasing the intensity of blue light will provide the benefits of better sleep and protection against potential eye diseases, but more research is needed to investigate this potential health risk [
32].
6. Discussion
Three current devices were tested in the tablet, smartphone, and laptop categories. The effects of reading stimuli and, above all, games on registered digital devices show significant differences between the spectral profile of the text and the game tested, both in terms of irradiance and illuminance values.
The evaluated blue light-blocking lenses effectively reduced the emission of enriched light with a wavelength of around 450 nm. The reduction of the spectrum emitted in the Blue Light Hazard (BLH) ranges is in accordance with what was announced by the manufacturers of the tested ophthalmic lenses. The BLH highlights the risks of blue radiation for each wavelength between 390 nm and 500 nm. Based on in vitro and in vivo studies, it calculates the risk of damage from wavelengths along the blue radiation spectrum. However, according to the CIE International Commission on Illumination, BLH is not based on common artificial light sources such as LEDs or digital devices and is not particularly relevant for lenses that block blue radiation or for determining eye hazards from radiation, whether digital or artificial blue.
Digital devices’ producers presented new models of digital devices with a frequency that far exceeded the time taken to carry out experimental work and publish new research. This fact compromises the current studies that evaluate the hardware at the time of publication. Despite these limitations, the tendency of new devices to enhance the definition of screens, increasing brightness and contrast in daytime use. These daytime characteristics are the same as nighttime use, which can interfere with sleep quality and with some ocular structures. The human retina is adapted for both photopic and color vision due to the fovea. This area of the retina has a high density of photoreceptors, the cones.
These photoreceptor cells of three types, S, M, and L cones, respond to short, medium, and long wavelengths with a unique photopigment with absorption peaks at 420, 530, and 560 nm, respectively [
42,
43]. In 1971, a pioneering study using electrophysiological recordings found similarities in activity in gangion cells in humans and in the retinas of other animal species. The spectral sensitivity in humans of ipRGC cells, non-visual photopics, presents a sensitivity peak at 480 nm [
44]. Although the blue light emission of the devices measured in this study did not present high values that raise concerns for eye diseases, these levels can influence circadian rhythms and sleep quality [
34]. Non-visual effects are not the subject of this study, but the data suggest deeper analyses of the blue light impact on the human circadian system and the possible consequences for human health. At noon, sunlight has a high intensity, a high color temperature, and a high blue light content. During the night, these factors decrease strongly. Humanity has adapted to these variations of the solar day and synchronized the circadian rhythm with these three factors: intensity, color temperature, and blue content.
Exposure to inappropriately high light intensities in the late afternoon or evening can disrupt the regular waking rhythm and lead to insomnia and even serious illnesses [
45,
46]. It is therefore highly advisable to limit exposure to high-intensity light during those periods of the day so as not to be counterproductive to the natural circadian rhythm. In addition, the spectral sensitivity of ganglion cells is fundamental to controlling the circadian rhythm.
This specific role of blue light must be taken into account when using these digital devices, as well as when planning and using artificial lighting. The European Scientific Committee on Health, Environmental, and Emerging Risks states that there is no evidence of risk under normal conditions of use; however, further research into cumulative exposure to digital devices and their long-term effects will be necessary. Daily exposure to blue light throughout life can be harmful. Despite the available information regarding the use of digital devices and its associated risks, it is very difficult to indicate to users the best choices for their health. However, it is evident that recent technological advances in devices have emphasized features that improve their brightness, blue light output, visibility, and contrast in daylight conditions. These features that improve usability during the day can have harmful effects when used at night, interfering with the quality of sleep and potentially affecting different ocular structures. The emission of blue light by digital devices and their safety in use is still just a hypothesis, and, therefore, this topic generates controversy and no consensus in the scientific community.
Despite the lack of consensus in the literature, reducing direct exposure to blue light, whether by reducing the number of hours per day or by reducing the irradiation at night, might be an advantage. Tested and commercially available lenses have shown the ability to reduce blue radiation up to 450 nm, attenuating the emission of blue light, which is responsible for interfering with the functional activity of photoreceptors and ocular surface symptoms [
25]. The retina’s exposure to blue radiation regulates the melatonin hormone, with greater sensitivity in the 480 nm range. The tested lenses showed the ability to transmit this beneficial blue light to trigger physiological processes that control our biological clock and maintain our well-being in general.
Using digital devices at night in the three categories tested continues to raise concerns due to their effects on human physiology [
47]. The use of filters in ophthalmic lenses (not consensual), hardware or software, offers some of the solutions to control the light spectrums emitted by these devices [
48,
49]. Blue light-blocking glasses may not attenuate occasional symptoms such as blurred vision, tiredness, and dry eyes, as well as headaches [
24], despite the lenses preventing large amounts of visible blue light from reaching the eye, as shown in
Figure 4,
Figure 5 and
Figure 6.
There is also a great lack of agreement regarding ophthalmic blue light absorption filters. A recent 2023 Cochrane review [
24] suggests, based on the best available evidence, that no clinically significant difference was found between blue light-blocking lenses compared to non-blue light-blocking lenses. They add that they were unable to determine whether blue light filter lenses affect a patient’s contrast sensitivity, color discrimination, uncomfortable glare, macular health, melatonin levels, or overall visual satisfaction compared to no blue light filter. However, all other conclusions in this Cochrane summary are based on low to very low evidence [
24]. Taking another approach, a 2020 investigation found that neutral density filters with blue-blocking technology demonstrated effectiveness in reducing symptoms such as dry eye, fatigue, headaches, and blurred vision. These are common symptoms of computer vision syndrome [
50,
51].
In order to carry out future research and experimental work in this area of study, it is also essential to have consistency in the units to prevent the comparison of experimental conditions. It is agreed that to measure blue light, illuminance has the units of lux, luminance cd/m2, or irradiance W/m2, to characterize light sources. Frequently, the details of the light sources are not known in the publications, and the respective units cannot be converted.
A faster and more sustainable solution may lie in technological advances and concerns about the irradiance and illuminance of new devices. A better image does not necessarily mean a brighter one.
7. Conclusions
In today’s world, artificial light is an unavoidable reality. However, among the various sources of artificial light emitting blue light, digital devices stand out as those with which we interact in terms of the number of hours. Whether for professional obligations or leisure activities, the increasing exposure to these devices leads to a pertinent exploration of the ramifications of blue light on our overall well-being and visual health.
In conclusion, it is recognized that low-luminance artificial blue light emitted by digital devices does not have an immediate and acute impact on our eyes. However, qualitative and quantitative research (still insufficient) needs to be conducted to determine the extent to which prolonged exposure to blue light from these devices may affect our eyes in the long term. The data from this comparative study helps us understand the potential implications for our eye health and overall quality of life. The results of this research establish a set of methodologies that could serve as a model for future studies in this field. Furthermore, when evaluating the spectral emission of the tested devices, based on knowledge from previous research, it can be concluded that under normal circumstances and without prolonged exposure, blue light levels should not have a significant impact on eye health. It is also essential to highlight that this study, as it is a preliminary analysis to test methodologies, is not free from limitations:
Only one Apple device per category was tested, leaving devices with the Android operating system, Windows, Symbian OS, Bada, and MeeGo, among others, to be tested.
The contribution of environmental factors was not considered, knowing that the spectral emission of these devices is not the only factor in their interaction with ocular structures.
Some users of these devices (Macbook, iPad, and iPhone) can manually adjust the light intensity or invert the colors. Thus, the results are only applicable to users using auto/default lighting settings.
The exposure time to these sources is another important factor, not considered, in the cellular photoexcitation of human eyes.
Technological development and the consequent emergence of new devices are faster than the analysis time, data interpretation, and eventual publication of new research. It obviously results in technological outdatedness at the time of publication.
The saturation time of ocular structures for each device and the intensity are not known, but it is an important area for future research.
Only automatic configuration for each device with text and a game was tested.
The importance of continuous integration of new data from future and ongoing studies is crucial to incorporating updated information and evaluating the safety implications of emerging technological advances. This becomes especially relevant due to the persistent daily presence of these devices in our lives, demanding a vigilant approach regarding the potential risks that may arise with prolonged use. The research methodology was also replicated by incorporating various blue-blocking lenses in front of the digital devices. This replication confirmed that all lenses effectively reduced the emission of short-wavelength light. In the specific spectral emissions of the tested devices, the irradiance for blue light risk ranged from 0.99 × 10
−3 to 5.26 × 10
−3 mW/cm
2. The differences observed between devices are related to the particular characteristics of each device category. These spectral irradiances are lower (in the order of hundreds of times) than solar radiation (
Figure 3), which in practice means that the measurements carried out indicated that the blue irradiance received by the human eye during approximately one minute outdoors is greater than the blue light received by the tested smartphone for 24 h.
Emphasizing the importance of future analyses, it is crucial that spectral measurements encompass a broader array of diverse artificial sources. This approach aims to avoid unrealistic values and conclusions.
As research endeavors to formulate new strategies for comprehending the genuine impacts of artificial blue light, it becomes imperative to consider not only the potential health consequences but also explore innovative forms of technological performance that contribute to the overall users’ well-being.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}