Biophotonic Effects of Low-Level Laser Therapy at Different Wavelengths for Potential Wound Healing


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Fibroblast Cells
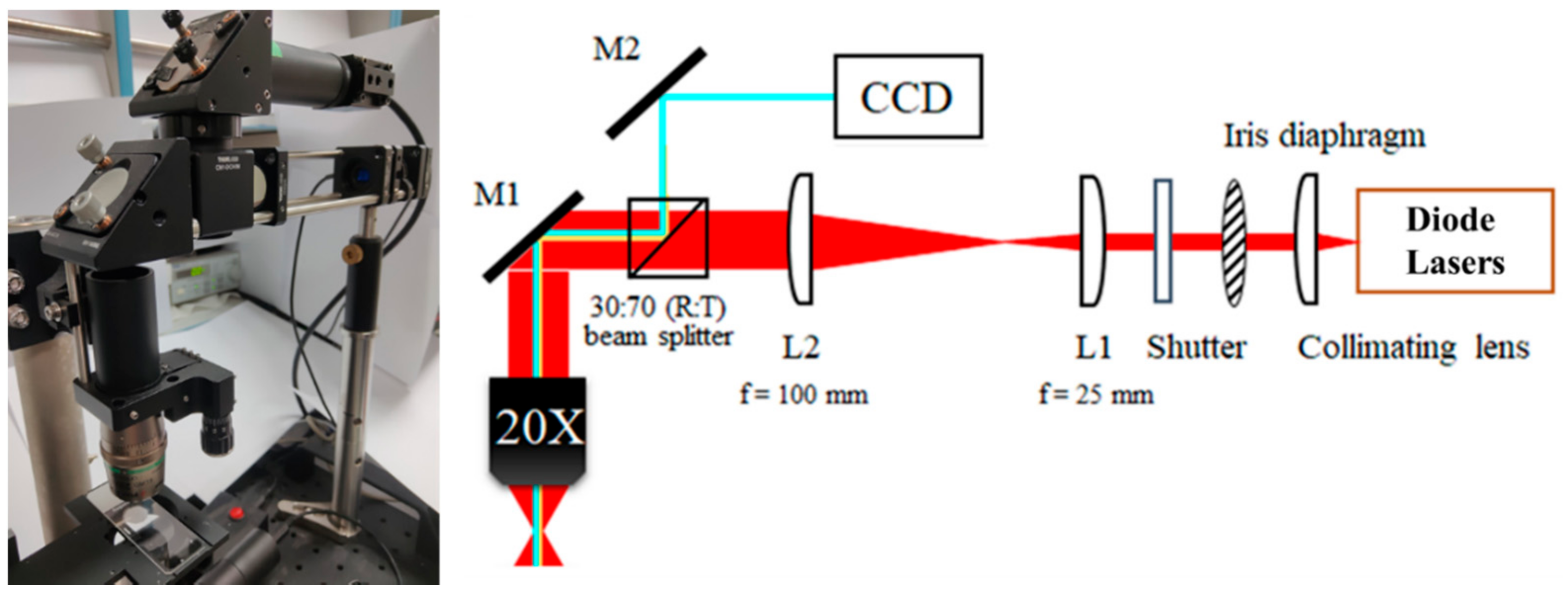
2.2. Low-Level Laser Illumination
2.3. Assessment of Cell Viability
2.4. Real-Time Polymerase Chain Reaction and Enzyme-Linked Immunosorbent Assay
2.5. Clinical Study: Histological and Immunohistochemical Analysis
2.6. Clinical Study: Basic Fibroblast Growth Factor and Vascular Endothelial Growth Factor Levels
2.7. Statistical Analysis
3. Results
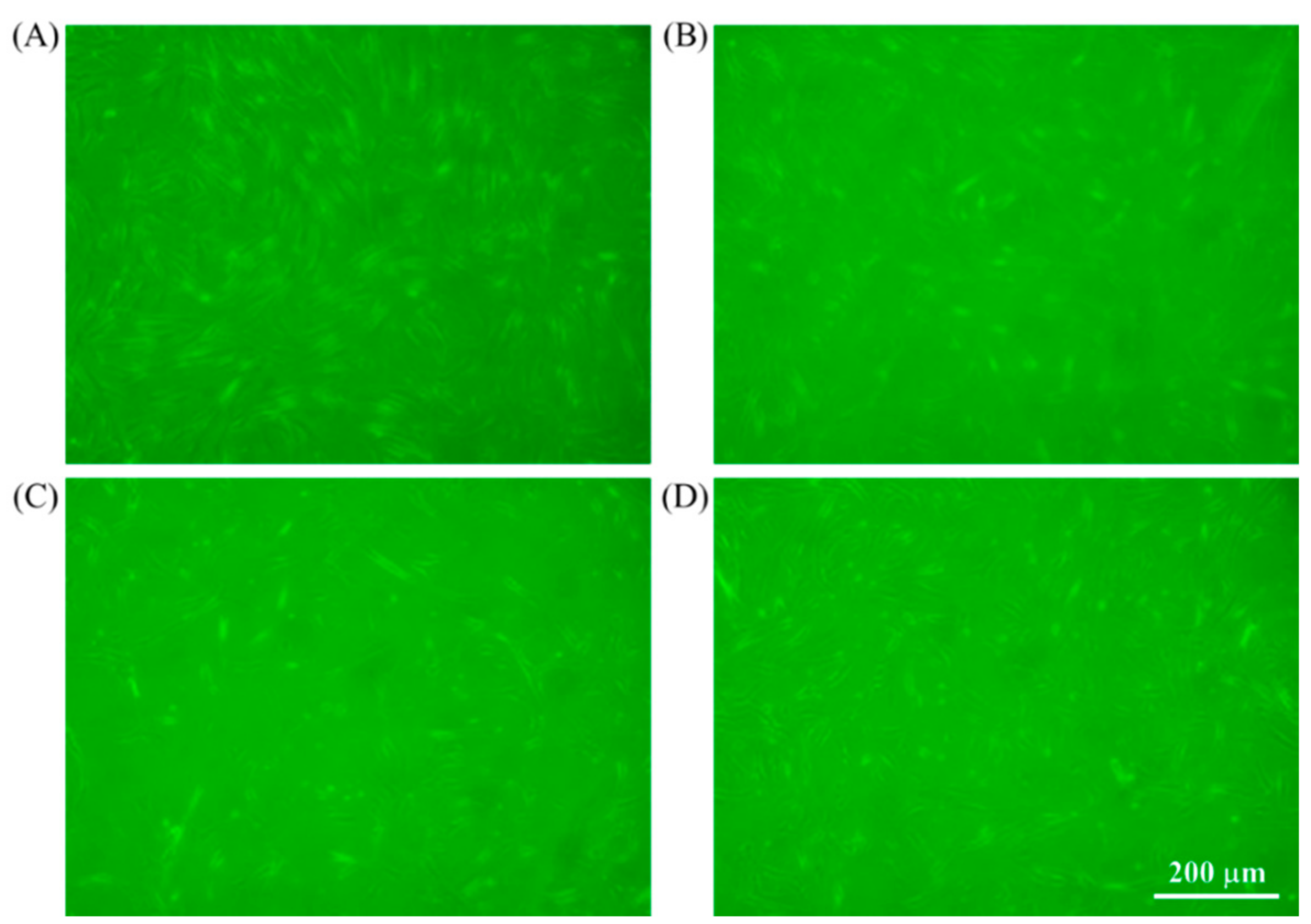
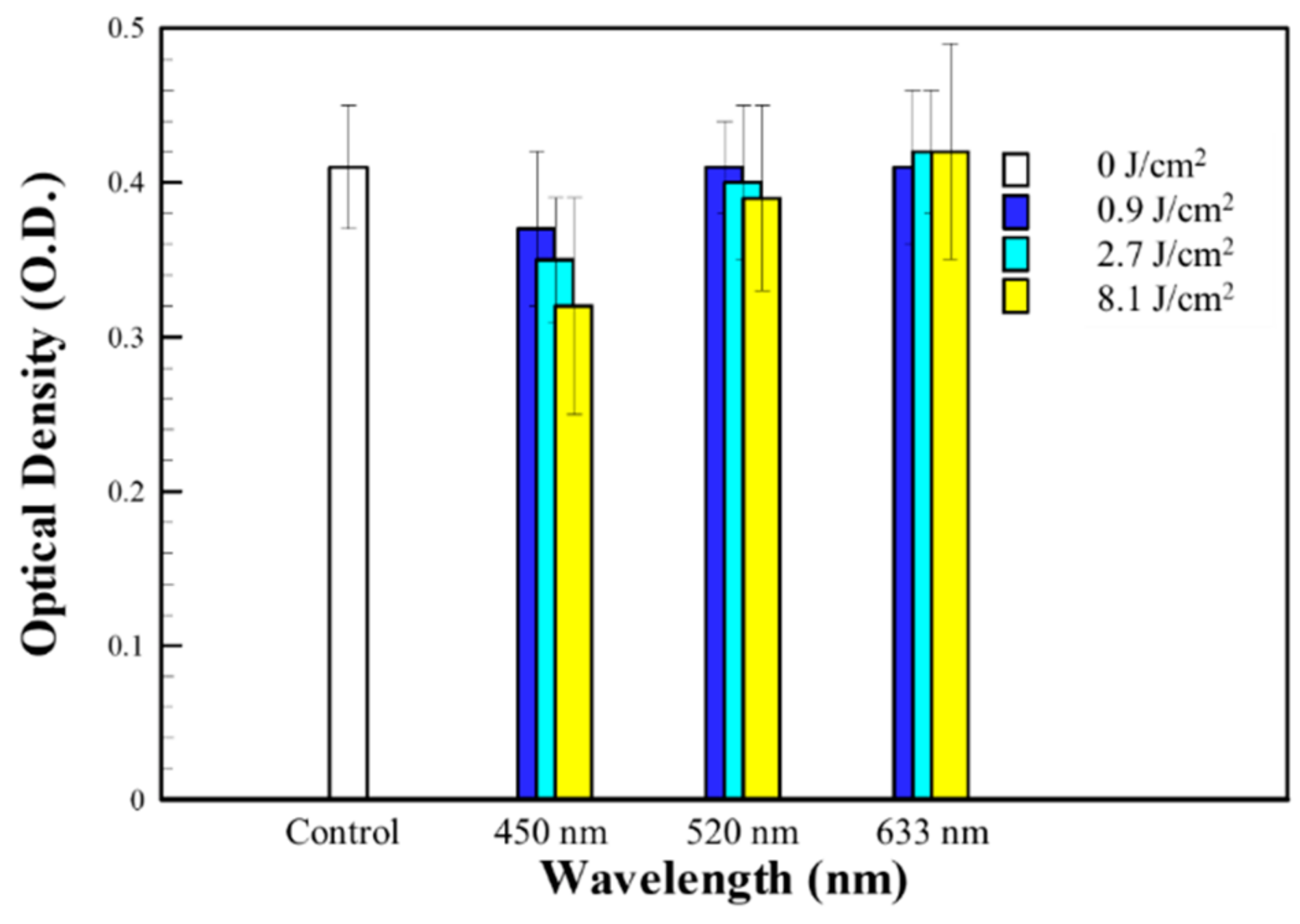
3.1. In Vitro Study: Human Fibroblast Cells
3.2. In Vitro Study: Real-Time Polymerase Chain Reaction and Enzyme-Linked Immunosorbent Assay
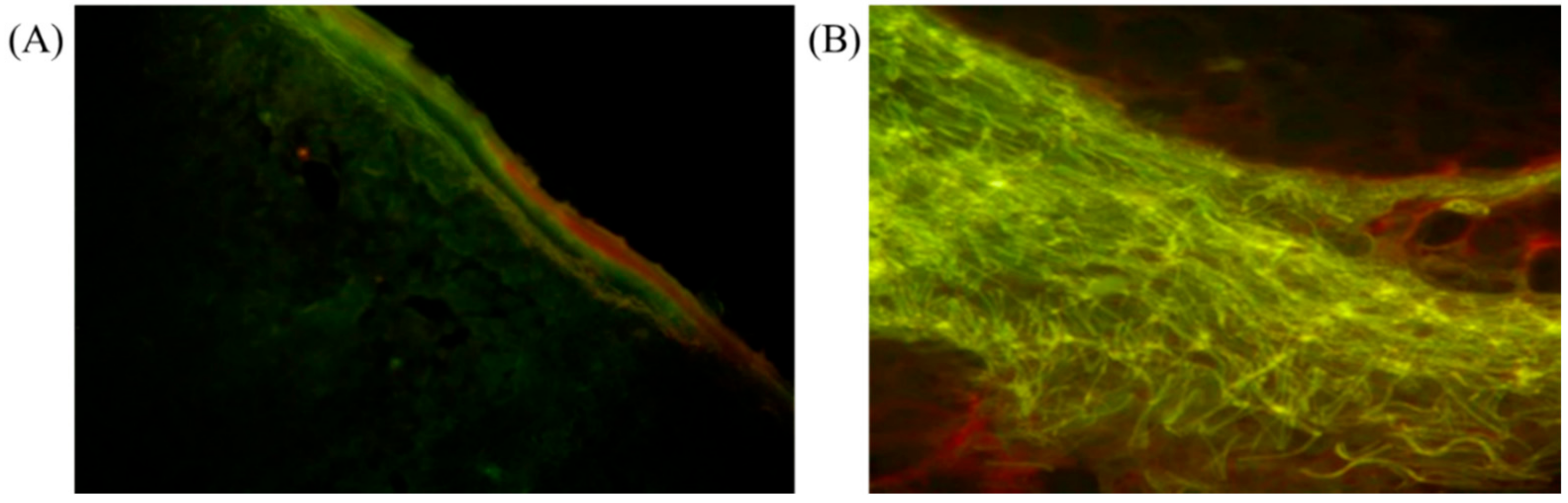
3.3. Clinical Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.Y.; Carroll, J.D.; Hamblin, M.R. The Nuts and Bolts of Low-level Laser (Light) Therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [PubMed]
- Whelan, H.T.; Smits Jr, R.L.; Buchman, E.V.; Whelan, N.T.; Turner, S.G.; Margolis, D.A.; Cevenini, V.; Stinson, H.; Ignatius, R.; Martin, T. Effect of NASA light-emitting diode irradiation on wound healing. J. Clin. Laser Med. Surg. 2001, 19, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Whelan, H.T.; Wong-Riley, M.T.; Eells, J.T.; VerHoeve, J.N.; Das, R.; Jett, M. DARPA soldier self-care: Rapid healing of laser eye injuries with light emitting diode technology. In Proceedings of the RTO HFM Symposium on “Combat Casualty Care in Ground Based Tactical Situations: Trauma Technology and Emergency Medical Procedures”, St. Pete Beach, FL, USA, 16–18 August 2004. [Google Scholar]
- Whelan, H.T.; Buchmann, E.V.; Dhokalia, A.; Kane, M.P.; Whelan, N.T.; Wong-Riley, M.T.T.; Eells, J.T.; Gould, L.J.; Hammamieh, R.; Das, R.; et al. Effect of NASA light-emitting diode irradiation on molecular changes for wound healing in diabetic mice. J. Clin. Laser Med. Surg. 2003, 21, 67–74. [Google Scholar] [CrossRef]
- Desmet, K.D.; Paz, D.A.; Corry, J.J.; Eells, J.T.; Wong-Riley, M.T.; Henry, M.M.; Buchmann, E.V.; Connelly, M.P.; Dovi, J.V.; Liang, H.L.; et al. Clinical and experimental applications of NIR-LED photobiomodulation. Photomed. Laser Ther. 2006, 24, 121–128. [Google Scholar] [CrossRef]
- Mester, A.F.; Mester, A. Wound healing. Laser Ther. 1989, 1, 7–15. [Google Scholar] [CrossRef]
- Trelles, M.A.; Allones, I. Red light-emitting diode (LED) therapy accelerates wound healing post-blepharoplasty and periocular laser ablative resurfacing. J. Cosmet. Laser Ther. 2006, 8, 39–42. [Google Scholar] [CrossRef]
- Dall Agnol, M.A.; Nicolau, R.A.; de Lima, C.J.; Munin, E. Comparative analysis of coherent light action (laser) versus non-coherent light (light-emitting diode) for tissue repair in diabetic rats. Lasers Med. Sci. 2009, 24, 909–916. [Google Scholar] [CrossRef]
- Corazza, A.V.; Jorge, J.; Kurachi, C.; Bagnato, V.S. Photobiomodulation on the angiogenesis of skin wounds in rats using different light sources. Photomed. Laser Surg. 2007, 25, 102–106. [Google Scholar] [CrossRef]
- Erdle, B.J.; Brouxhon, S.; Kaplan, M.; Vanbuskirk, J.; Pentland, A.P. Effects of continuous-wave (670-nm) red light on wound healing. Dermatol. Surg. 2008, 34, 320–325. [Google Scholar]
- Chen, Q.; Yang, J.; Yin, H.; Li, Y.; Qiu, H.; Gu, Y.; Yang, H.; Xiaoxi, D.; Xiafei, S.; Che, B.; et al. Optimization of photo-biomodulation therapy for wound healing of diabetic foot ulcers in vitro and in vivo. Biomed. Opt. Express 2022, 13, 2450–2466. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, J.T.; McLoda, T.A.; Seegmiller, J.G.; Baxter, G.D. Low-level laser therapy facilites superficial wound healing in humans: A triple-blind, sham-controlled study. J. Athl. Train. 2004, 39, 223–229. [Google Scholar] [PubMed]
- Huang, C.-F.; Colley, M.M.S.; Lu, L.-S.; Chang, C.-Y.; Peng, P.-W.; Yang, T.-S. Performance characterization of continuous-wave laser-induced forward transfer of liquid bioink. Appl. Phys. Express 2019, 12, 116504. [Google Scholar] [CrossRef]
- Pan, L.-C.; Hang, N.-L.; Colley, M.M.; Chang, J.; Hsiao, Y.-C.; Lu, L.-S.; Li, B.-S.; Chang, C.-J.; Yang, T.-S. Single Cell Effects of Photobiomodulation on Mitochondrial Membrane Potential and Reactive Oxygen Species Production in Human Adipose Mesenchymal Stem Cells. Cells 2022, 11, 972. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.I.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef]
- Roberts, W.G.; Berns, M.W. In vitro photosensitation I. Cellular uptake and subcellular location of mono-L-aspartyl chlorin e6, chloro-aluminium sulfonated phthalocyanine, and photofrin®. Lasers Surg. Med. 1989, 9, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Li, J.; Gao, J.; Ogawa, R.; Ou, C.; Yang, B.; Fu, B. Improvement of the Survival of Human Autologous Fat Transplantation by Using VEGF-Transfected Adipose-Derived Stem Cells. Plast. Reconstr. Surg. 2009, 124, 1437–1446. [Google Scholar] [CrossRef]
- Kim, W.-S.; Park, B.-S.; Park, S.-H.; Kim, H.-K.; Sung, J.-H. Antiwrinkle effect of adipose-derived stem cell: Activation of dermal fibroblast by secretory factors. J. Dermatol. Sci. 2009, 53, 96–102. [Google Scholar] [CrossRef]
- Kim, W.-S.; Park, B.-S.; Sung, J.-H. Protective role of adipose-derived stem cells and their soluble factors in photoaging. Arch. Dermatol. Res. 2009, 301, 329–336. [Google Scholar] [CrossRef]
- Jeong, J.H.; Fan, Y.; You, G.Y.; Choi, T.H.; Kim, S. Improvement of photoaged skin wrinkles with cultured human fibroblasts and adipose-derived stem cells: A comparative study. J. Plast. Reconstr. Aesthetic Surg. 2015, 68, 372–381. [Google Scholar] [CrossRef]
- Poulalhon, N.; Farge, D.; Roos, N.; Tacheau, C.; Neuzillet, C.; Michel, L.; Mauviel, A.; Verrecchia, F. Modulation of collagen and MMP-1 gene expression in fibroblasts by the immuno-suppressive drug rapamycin. A direct role as an antifibrotic agent? J. Biol. Chem. 2006, 281, 33045–33052. [Google Scholar] [CrossRef] [PubMed]
- Kajanne, R.; Miettinen, P.; Mehlem, A.; Leivonen, S.-K.; Birrer, M.; Foschi, M.; Kähäri, V.-M.; Leppä, S. EGF-R regulates MMP function in fibroblasts through MAPK and AP-1 pathways. J. Cell. Physiol. 2007, 212, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Westermarck, J.; Holmström, T.; Ahonen, M.; Eriksson, J.E.; Kahari, V.M. Enhancement of fibroblast collagenase-1 (MMP-1) gene expression by tumor promoter okadaic acid is mediated by stress-activated protein kinases Jun N-terminal kinase and p38. Matrix Biol. 1998, 17, 547–557. [Google Scholar] [CrossRef]
- Khoramizadeh, M.R.; Falak, R.; Pezeshki, M.; Ghahary, A.; Saadat, F.; Varshokar, K.; Safavifar, F.; Mansouri, P. Dermal wound fibroblasts and matrix metalloproteinases (MMPs): Their possible role in allergic contact dermatitis. Iran. J. Allergy Asthma Immunol. 2004, 3, 7–11. [Google Scholar]
- Hattori, N.; Mochizuki, S.; Kishi, K.; Nakajima, T.; Takaishi, H.; D’Armiento, J.; Okada, Y. MMP-13 Plays a Role in Keratinocyte Migration, Angiogenesis, and Contraction in Mouse Skin Wound Healing. Am. J. Pathol. 2009, 175, 533–546. [Google Scholar] [CrossRef]
- Howard, E.W.; Crider, B.J.; Updike, D.L.; Bullen, E.C.; Parks, E.E.; Haaksma, C.J.; Sherry, D.M.; Tomasek, J.J. MMP-2 expression by fibroblasts is suppressed by the myofibroblast phenotype. Exp. Cell Res. 2012, 318, 1542–1553. [Google Scholar] [CrossRef]
- Lindner, D.; Zietsch, C.; Becher, P.M.; Schulze, K.; Schultheiss, H.-P.; Tschöpe, C.; Westermann, D. Differential Expression of Matrix Metalloproteases in Human Fibroblasts with Different Origins. Biochem. Res. Int. 2012, 2012, 875742. [Google Scholar] [CrossRef]
- Kim, J.-H.; Jung, M.; Kim, H.-S.; Kim, Y.-M.; Choi, E.-H. Adipose-derived stem cells as a new therapeutic modality for ageing skin. Exp. Dermatol. 2011, 20, 383–387. [Google Scholar] [CrossRef]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef]
- Banks, R.; Forbes, M.A.; Kinsey, S.E.; Stanley, A.; Ingham, E.; Walters, C.; Selby, P.J. Release of the angiogenic cytokine vascular endothelial growth factor (VEGF) from platelets: Significance for VEGF measurements and cancer biology. Br. J. Cancer 1998, 77, 956–964. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MMP-1 | MMP-2 | MMP-9 | |
|---|---|---|---|
| Wavelength (nm) | Mean ± SD (%) | ||
| Control | 0.68 ± 0.13 | 0.67 ± 0.14 | 0.69 ± 0.02 |
| 633 | 0.13 ± 0.06 | 0.13 ± 0.07 | 0.15 ± 0.05 |
| 520 | 0.37 ± 0.11 | 0.30 ± 0.15 | 0.39 ± 0.09 |
| 450 | 0.41 ± 0.12 | 0.36 ± 0.11 | 0.45 ± 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.-S.; Nguyen, L.-T.-H.; Hsiao, Y.-C.; Pan, L.-C.; Chang, C.-J. Biophotonic Effects of Low-Level Laser Therapy at Different Wavelengths for Potential Wound Healing. Photonics 2022, 9, 591. https://doi.org/10.3390/photonics9080591
Yang T-S, Nguyen L-T-H, Hsiao Y-C, Pan L-C, Chang C-J. Biophotonic Effects of Low-Level Laser Therapy at Different Wavelengths for Potential Wound Healing. Photonics. 2022; 9(8):591. https://doi.org/10.3390/photonics9080591
Chicago/Turabian StyleYang, Tzu-Sen, Le-Thanh-Hang Nguyen, Yu-Cheng Hsiao, Li-Chern Pan, and Cheng-Jen Chang. 2022. "Biophotonic Effects of Low-Level Laser Therapy at Different Wavelengths for Potential Wound Healing" Photonics 9, no. 8: 591. https://doi.org/10.3390/photonics9080591
APA StyleYang, T. -S., Nguyen, L. -T. -H., Hsiao, Y. -C., Pan, L. -C., & Chang, C. -J. (2022). Biophotonic Effects of Low-Level Laser Therapy at Different Wavelengths for Potential Wound Healing. Photonics, 9(8), 591. https://doi.org/10.3390/photonics9080591