
Comparative Study Regarding the Adherence to the Mediterranean Diet and the Eating Habits of Two Groups—The Romanian Children and Adolescents Living in Nord-West of Romania and Their Romanian Counterparts Living in Italy

 , ,
, ,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Weight and Height Assessment
2.2. KIDMED Test
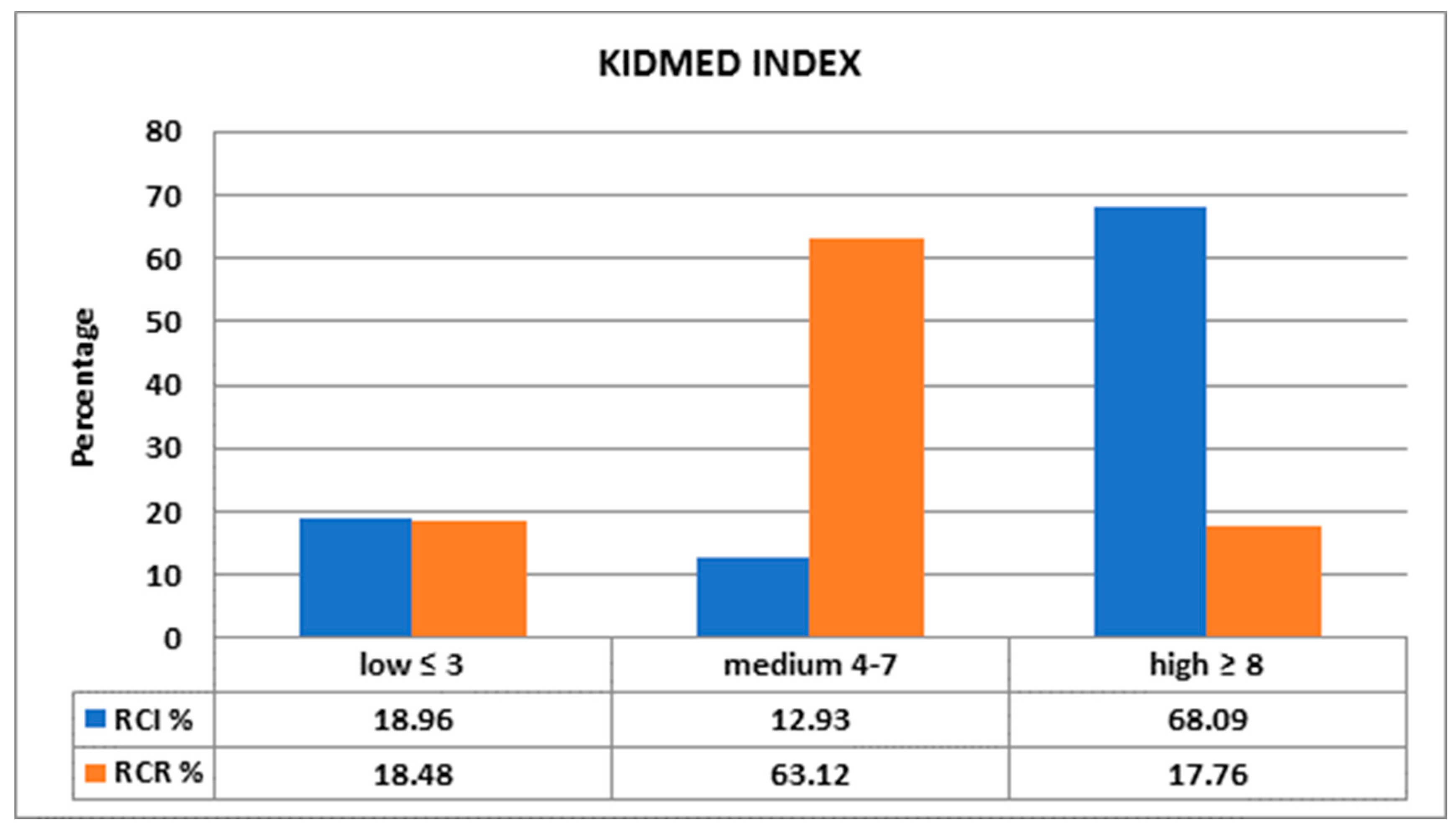
- (1)
- >8: optimal Mediterranean diet;
- (2)
- 4–7: improvement needed to adjust intake to Mediterranean patterns;
- (3)
- ≤3: extremely low diet quality [20].
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNESCO. The Mediterranean Diet. Inscribed in 2010 on the Representative List of the Intangible Cultural Heritage of Humanity. Available online: https://ich.unesco.org/en/RL/mediterranean-diet-00884# (accessed on 12 July 2021).
- Mediterranean Diet Pyramid: A Lifestyle for Today. Available online: https://dietamediterranea.com/piramidedm/piramide_INGLES.pdf (accessed on 12 December 2020).
- Mancini, J.G.; Filion, K.B.; Atallah, R.; Eisenberg, M.J. Systematic Review of the Mediterranean Diet for Long-Term Weight Loss. Am. J. Med. 2016, 129, 407–415.e4. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open 2015, 5, e008222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafatos, A.; Verhagen, H.; Moschandreas, J.; Apostolaki, I.; VanWesterop, J.J. Mediterranean diet of Crete: Foods and nutrient content. J. Am. Diet. Assoc. 2000, 100, 1487e93. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61 (Suppl. 6), S1402e6. [Google Scholar] [CrossRef]
- Bulló, M.; Lamuela-Reventós, R.; Salas-Salvadó, J. Mediterranean diet and oxidation: Nuts and olive oil as important sources off at and antioxidants. Curr. Top. Med. Chem. 2011, 11, 1797–1810. [Google Scholar] [CrossRef]
- Nadtochiy, S.; Redman, E. Mediterranean diet and cardioprotection: The role of nitrite, polyunsaturated fatty acids, and polyphenols. Nutrition 2011, 27, 733–744. [Google Scholar] [CrossRef] [Green Version]
- Waters, E.; de Silva-Sanigorski, A.; Hall, B.J.; Brown, T.; Campbell, K.J.; Gao, Y. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12, CD001871. [Google Scholar] [CrossRef]
- Belahsen, R. Nutrition transition and food sustainability. Proc. Nutr. Soc. 2014, 73, 385–388. [Google Scholar] [CrossRef] [Green Version]
- Khanna, P.; Chattu, V.K.; Aeri, B.T. Nutritional Aspects of Depression in Adolescents—A Systematic Review. Int. J. Prev. Med. 2019, 10, 42. [Google Scholar]
- Chau, M.M.; Burgermaster, M.; Mamykina, L. The use of social media in nutrition interventions for adolescents and young adults-A systematic review. Int. J. Med. Inform. 2018, 120, 77–91. [Google Scholar] [CrossRef]
- Dondi, A.; Piccinno, V.; Morigi, F.; Sureshkumar, S.; Gori, D.; Lanari, M. Food Insecurity and Major Diet-Related Morbidities in Migrating Children: A Systematic Review. Nutrients 2020, 12, 379. [Google Scholar] [CrossRef] [Green Version]
- Desbouys, L.; Méjean, C.; de Henauw, S.; Castetbon, K. Socio-economic and cultural disparities in diet among adolescents and young adults: A systematic review. Public Health Nutr. 2020, 23, 843–860. [Google Scholar] [CrossRef] [Green Version]
- Food as a Key Medium for Social Inclusion and Intercultural Dialogue: A Taste of Lessons Learned from European Initiatives. Available online: https://www.agronauten.net/wp-content/uploads/2018/03/FR_report_final-version_ENG.pdf (accessed on 12 December 2020).
- National Report Romanian Immigrants in Italy. Available online: http://www.participation-citoyenne.eu/sites/default/files/report-italy.pdf (accessed on 12 December 2020).
- Caritas, Dossier Statistico Immigrazione Caritas-Migrantes «Oltre la crisi insieme» 2011, 21 Rapporto, Ed. Idos Roma. 2011. Available online: https://www.caritas.it/materiali/Pubblicazioni/libri_2011/dossier_immigrazione2011/pittau.pdf (accessed on 12 December 2020).
- Osei-Kwasi, H.A.; Nicolaou, M.; Powell, K.; Terragni, L.; Maes, L.; Stronks, K.; Lien, N.; Holdsworth, M.; DEDIPAC Consortium. Systematic mapping review of the factors influencing dietary behaviour in ethnic minority groups living in Europe: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Ribas, L.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur. J. Clin. Nutr. 2003, 57, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef]
- Merra, G.; Noce, A.; Marrone, G.; Cintoni, M.; Tarsitano, M.G.; Capacci, A.; de Lorenzo, A. Influence of Mediterranean Diet on Human Gut Microbiota. Nutrients 2021, 13, 7. [Google Scholar] [CrossRef]
- Santulli, G.; Pascale, V.; Finelli, R.; Visco, V.; Giannotti, R.; Massari, A.; Morisco, C.; Ciccarelli, M.; Illario, M.; Iaccarino, G.; et al. We are What We Eat: Impact of Food from Short Supply Chain on Metabolic Syndrome. J. Clin. Med. 2019, 8, 2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echeverría, G.; McGee, E.E.; Urquiaga, I.; Jiménez, P.; D’Acuña, S.; Villarroel, L.; Velasco, N.; Leighton, F.; Rigotti, A. Inverse Associations between a Locally Validated Mediterranean Diet Index, Overweight/Obesity, and Metabolic Syndrome in Chilean Adults. Nutrients 2017, 9, 862. [Google Scholar] [CrossRef] [Green Version]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Foundation Expert Group:Mediterranean diet pyramid today. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Archero, F.; Ricotti, R.; Solito, A.; Carrera, D.; Civello, F.; Di Bella, R.; Bellone, S.; Prodam, F. Adherence to the Mediterranean Diet among School Children and Adolescents Living in Northern Italy and Unhealthy Food Behaviors Associated to Overweight. Nutrients 2018, 10, 1322. [Google Scholar] [CrossRef] [Green Version]
- Mistretta, A.; Marventano, S. Mediterranean diet adherence and body composition among Southern Italian adolescents. Obes. Res. Clin. Pract. 2017, 11, 215–226. [Google Scholar] [CrossRef]
- Grosso, G.; Marventano, S. Factors associated with adherence to the Mediterranean diet among adolescents living in Sicily, Southern Italy. Nutrients 2013, 5, 4908–4923. [Google Scholar] [CrossRef] [Green Version]
- Santomauro, F.; Lorini, C. Adherence to Mediterranean diet in a sample of Tuscan adolescents. Nutrition 2014, 30, 1379–1383. [Google Scholar] [CrossRef]
- Foreigners Resident on 1 January—Citizenship. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPSTRCIT1# (accessed on 12 December 2020).
- FAO. Mediterranean Food Consumption Patterns—Diet, Environment, Society, Economy and Health; FAO: Italy, Rome, 2015; Available online: http://www.fao.org/documents/card/fr/c/9104aa92-4561-4375-abb2-2651260fdaca/ (accessed on 12 December 2020).
- García Cabrera, S.; Herrera Fernández, N.; Rodríguez Hernández, C.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. Kidmed test; prevalence of low adherence to the mediterranean diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Kontogianni, M.D.; Vidra, N.; Farmaki, A.E.; Koinaki, S.; Belogianni, K.; Sofrona, S.; Magkanari, F.; Yannakoulia, M. Adherence rates to the Mediterranean diet are low in a representative sample of Greek children and adolescents. J. Nutr. 2008, 138, 1951–1956. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Navarro, J.; Conde, P.; Díez, J.; Gutiérrez-Sastre, M.; González-Salgado, I.; Sandín, M.; Gittelsohn, J.; Franco, M. Urban environment and dietary behaviours as perceived by residents living in socioeconomically diverse neighbourhoods: A qualitative study in a Mediterranean context. Appetite 2021, 157, 104983. [Google Scholar] [CrossRef]
- Schröder, H.; Mendez, M.A.; Ribas-Barba, L.; Covas, M.; Serra-Majem, L. Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int. J. Pediatric Obes. 2010, 5, 516–519. [Google Scholar] [CrossRef]
- Notario-Barandiaran, L.; Valera-Gran, D.; Gonzalez-Palacios, S. High adherence to a mediterranean diet at age 4 reduces overweight, obesity and abdominal obesity incidence in children at the age of 8. Int. J. Obes. 2020, 44, 1906–1917. [Google Scholar] [CrossRef]
- Mendez, M.A.; Popkin, B.M.; Jakszyn, P. Adherence to a Mediterranean diet is associated with reduced 3-year incidence of obesity. J. Nutr. 2006, 136, 2934–2938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckland, G.; Bach, A.; Serra-Majem, L. Obesity, and the Mediterranean diet: A systematic review of observational and intervention studies. Obes. Rev. 2008, 9, 582–593. [Google Scholar] [CrossRef]
- Tognon, G.; Hebestreit, A.; Lanfer, A.; Moreno, L.A.; Pala, V.; Siani, A.; Tornaritis, M.; de Henauw, S.; Veidebaum, T.; Molnà, D.; et al. Mediterranean diet, overweight and body composition in children from eight European countries: Cross-sectional and prospective results from the IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 205e213. [Google Scholar] [CrossRef]
- Alkerwi, A.; Sauvageot, N.; Pagny, S.; Beissel, J.; Delagardelle, C.; Lair, M.L. Acculturation, immigration status and cardiovascular risk factors among Portuguese immigrants to Luxembourg: Findings from ORISCAV-LUX study. BMC Public Health 2012, 12, 864. [Google Scholar] [CrossRef] [Green Version]
- Espinosa, P.; Clemente, M.; Uña, O. Motivational Values, Parental Influences and the Experience of Discrimination among Romanian and Moroccan Young Immigrants in Spain. Span. J. Psychol. 2016, 19, E76. [Google Scholar] [CrossRef] [PubMed]
- Masih, T.; Dimmock, J.A.; Epel, E.S.; Guelfi, K.J. Stress-induced eating and the relaxation response as a potential antidote: A review and hypothesis. Appetite 2017, 118, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Petre, I.L. Study on the evolution of olive price in Romania. In Agrarian Economy and Rural Development—Realities and Perspectives for Romania, Proceedings of the 9th Edition of the International Symposium, November 2018, Bucharest, Romania; The Research Institute for Agricultural Economy and Rural Development (ICEADR): Bucharest, Romania, 2018; pp. 169–174. [Google Scholar]
- Romani, A.; Ieri, F.; Urciuoli, S.; Noce, A.; Marrone, G.; Nediani, C.; Bernini, R. Health Effects of Phenolic Compounds Found in Extra-Virgin Olive Oil, By-Products, and Leaf of Olea europaea L. Nutrients 2019, 11, 1776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grosso, G.; Galvano, F. Mediterranean diet adherence in children and adolescents in southern European countries. NFS J. 2017, 3, 16–19. [Google Scholar] [CrossRef] [Green Version]
- Idelson, P.I.; Scalfi, L. Adherence to the Mediterranean Diet in children and adolescents: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 283–299. [Google Scholar] [CrossRef] [PubMed]
- Gualdi-Russo, E.; Zaccagni, L.; Manzon, V.S.; Masotti, S.; Rinaldo, N.; Khyatti, M. Obesity and physical activity in children of immigrants. Eur. J. Public Health 2014, 24 (Suppl. 1), 40–46. [Google Scholar] [CrossRef] [Green Version]
- Jiménez Boraita, R.; Arriscado Alsina, D.; Dalmau Torres, J.M.; Gargallo Ibort, E. Calidad de vida relacionada con la salud y hábitos de vida: Diferencias entre adolescentes migrantes y autóctonos. Rev. Esp. Salud. Publica. 2020, 94, e202004023. [Google Scholar] [CrossRef]
- Bawaked, R.A.; Gomez, S.F.; Homs, C.; Casas Esteve, R.; Cardenas, G.; Fìto, M.; Schröder, H. Association of eating behaviours, lifestyle, and maternal education with adherence to the Mediterranean diet in Spanish children. Appetite 2018, 130, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, G.; Moreira, P.; Ròsario, R.; Araùjo, A.; Teixeira, V.H.; Lopes, O.; Moreira, A.; Padrao, P. Adherence to the Medieterranea diet in children: Is it associated with economic cost? Porto Biomed. J. 2017, 2, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KIDMED TEST | |
|---|---|
| Insert a value of 0 if the parent does not reply. For FRUIT and VEGETABLES consider only the question A or B. | |
| (A) Does the child eat one piece of fresh FRUIT every day, or drink a fresh fruit juice? | +1 |
| (B) Does the child eat at least two pieces of fresh FRUIT every day? | +1 |
| (A) Does the child eat once a day raw or cooked VEGETABLES? | +1 |
| (B) Does the child eat more than once a day raw or cooked VEGETABLES? | +1 |
| Does the child eat FISH (fresh or frozen) often (at least twice or three times a week)? | +1 |
| Do you go with him/her to fast-food restaurants more than once a week (and the child eats hamburgers, French fries and drinks sweetened beverages)? | −1 |
| Does he/she eat LEGUMES more than once a week? | +1 |
| Does he/she eat PASTA AND RICE more or less every day? (five or more times a week) | +1 |
| Does he/she eat BREAD OR CEREALS (without added sugar) for breakfast? | +1 |
| Does he/she eat NUTS OR DRY FRUIT regularly? (at least twice or three times a week) | +1 |
| Do you use OLIVE OIL at home? | +1 |
| Does the child SKIP BREAKFAST in the morning? | −1 |
| Does he/she eat milk derivatives, MILK, YOGHURT, or similar products, for breakfast? | +1 |
| Does he/she eat BAKERY PRODUCTS OR INDUSTRIAL SNACKS for breakfast? | −1 |
| Does he/she eat TWO YOGHURTS AND/OR CHEESE (maximum 40 g) during the day? | +1 |
| Does he/she eat SWEETS AND CANDIES often during the day? | −1 |
| KIDMED INDEX Low ≤ 3, Medium 4–7, High ≥ 8 | TOTAL … |
| Features | Participants (n = 530) | |
|---|---|---|
| RCR (n = 414) | RCI (n = 116) | |
| Sex: female | 217 | 57 |
| Sex: male | 197 | 59 |
| Body Weight (kg) | 36.5 ± 15.36 | 26.629 ± 14.178 |
| Body Height (m) | 1.4 ± 0.21 | 1.198 ± 0.242 |
| Body—Mass Index (BMI) (kg/m2) | 18.17 ± 4.07 | 17.244 ± 3.371 |
| Aged 1–5 | 18.59% | 41.37% |
| Aged 6–9 | 32.12% | 35.34% |
| Aged 10–12 | 28.26% | 16.37% |
| Aged 13–16 | 21.01% | 6.89% |
| Type of Diet | KIDMED Score % RCI | KIDMED Score % RCR | p |
|---|---|---|---|
| Consumption of a fruit or a fruit juice every day | 56.89 | 61.59 | 0.81 |
| Consumption of a second fruit every day | 35.34 | 29.47 | 0.015 * |
| Consumption of raw or cooked vegetables 1 time a day | 56.89 | 58.70 | 0.72 |
| Consumption of raw or cooked vegetables >1 time a day | 37.93 | 23.67 | 0.0001 * |
| Consumption of fish regularly (at least 2–3 times a week) | 61.21 | 31.88 | 0.0001 * |
| Eating >1 time per week at a fast food (hamburger) restaurant | 44.82 | 15.94 | 0.0001 * |
| Consumption of beans >1 time per week | 68.10 | 50.24 | 0.073 |
| Consumption of pasta or rice almost every day (≥5 times a week) | 95.68 | 33.33 | 0.0001 * |
| Consumption of cereals or grains (bread, etc.) for breakfast | 87.93 | 83.09 | 0.71 |
| Consumption of nuts regularly (at least 2–3 times per week) | 31.03 | 57.97 | 0.0001 * |
| Consumption of olive oil at home | 94.82 | 81.88 | 0.001 * |
| Skipping breakfast | 25.86 | 22.95 | 0.59 |
| Consumption of a dairy product for breakfast (yoghurts, milk, etc.) | 87.93 | 90.82 | 0.80 |
| Consumption of commercially baked goods or pastries for breakfast | 75.00 | 39.13 | 0.0001 * |
| Consumption of yoghurts and/or cheese (40 g) daily | 37.06 | 49.52 | 0.023 * |
| Consumption of sweets or candy several times every day | 56.89 | 35.02 | 0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pira, C.; Trapani, G.; Fadda, M.; Finocchiaro, C.; Bertino, E.; Coscia, A.; Ciocan, C.; Cuciureanu, M.; Hegheş, S.-C.; Vranceanu, M.; et al. Comparative Study Regarding the Adherence to the Mediterranean Diet and the Eating Habits of Two Groups—The Romanian Children and Adolescents Living in Nord-West of Romania and Their Romanian Counterparts Living in Italy. Foods 2021, 10, 2045. https://doi.org/10.3390/foods10092045
Pira C, Trapani G, Fadda M, Finocchiaro C, Bertino E, Coscia A, Ciocan C, Cuciureanu M, Hegheş S-C, Vranceanu M, et al. Comparative Study Regarding the Adherence to the Mediterranean Diet and the Eating Habits of Two Groups—The Romanian Children and Adolescents Living in Nord-West of Romania and Their Romanian Counterparts Living in Italy. Foods. 2021; 10(9):2045. https://doi.org/10.3390/foods10092045
Chicago/Turabian StylePira, Costanza, Gianfranco Trapani, Maurizio Fadda, Concetta Finocchiaro, Enrico Bertino, Alessandra Coscia, Catalina Ciocan, Magdalena Cuciureanu, Simona-Codruţa Hegheş, Maria Vranceanu, and et al. 2021. "Comparative Study Regarding the Adherence to the Mediterranean Diet and the Eating Habits of Two Groups—The Romanian Children and Adolescents Living in Nord-West of Romania and Their Romanian Counterparts Living in Italy" Foods 10, no. 9: 2045. https://doi.org/10.3390/foods10092045
APA StylePira, C., Trapani, G., Fadda, M., Finocchiaro, C., Bertino, E., Coscia, A., Ciocan, C., Cuciureanu, M., Hegheş, S. -C., Vranceanu, M., Miere, D., & Filip, L. (2021). Comparative Study Regarding the Adherence to the Mediterranean Diet and the Eating Habits of Two Groups—The Romanian Children and Adolescents Living in Nord-West of Romania and Their Romanian Counterparts Living in Italy. Foods, 10(9), 2045. https://doi.org/10.3390/foods10092045