

Influence of Lifestyle and Dietary Habits on the Prevalence of Food Allergies: A Scoping Review



Abstract
:1. Introduction
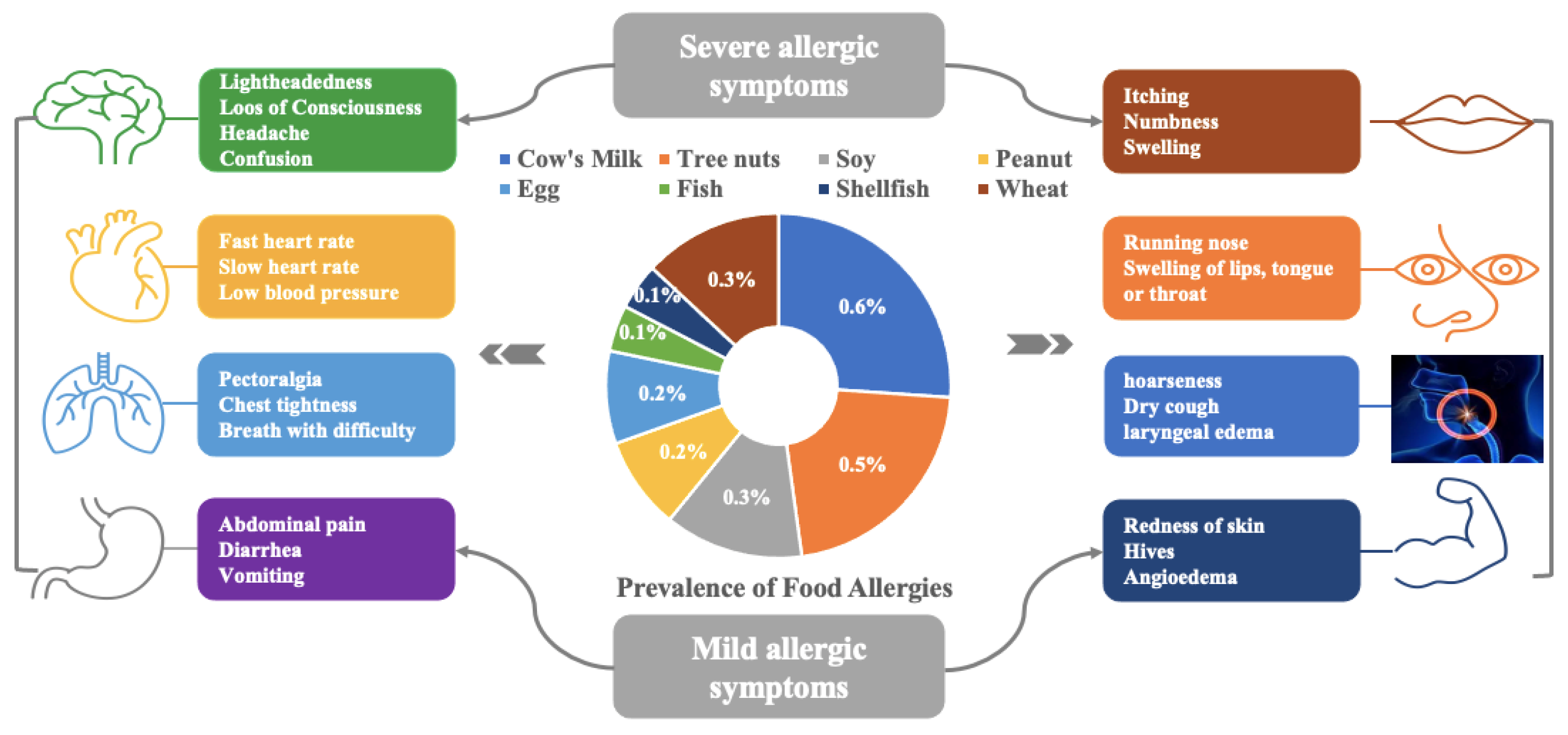
1.1. Clinical Manifestation/Symptoms of Food Allergy
1.2. Pathophysiology/Mechanism of Food Allergy(ies)
1.3. Exposure Route
1.4. Diagnosis of Food Allergies
1.5. Management and Prevention of Food Allergies
2. Materials and Methods
2.1. Study Design
2.2. Research Questions
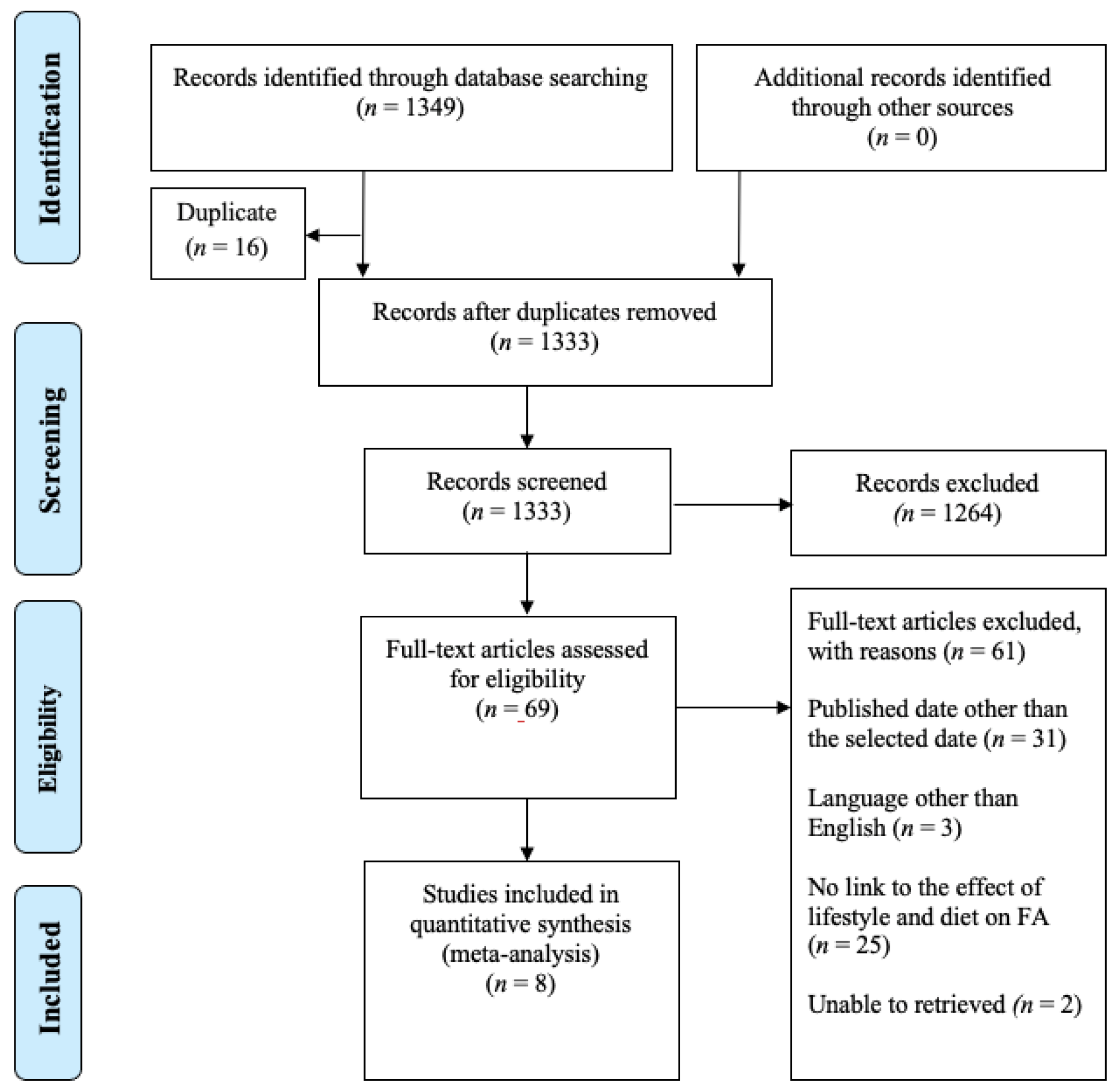
2.3. Source of Data/Studies Identification
2.4. Studies Selection
2.5. Data Charting
2.6. Results Collation, Summary, and Report
3. Results
3.1. Study Characteristics
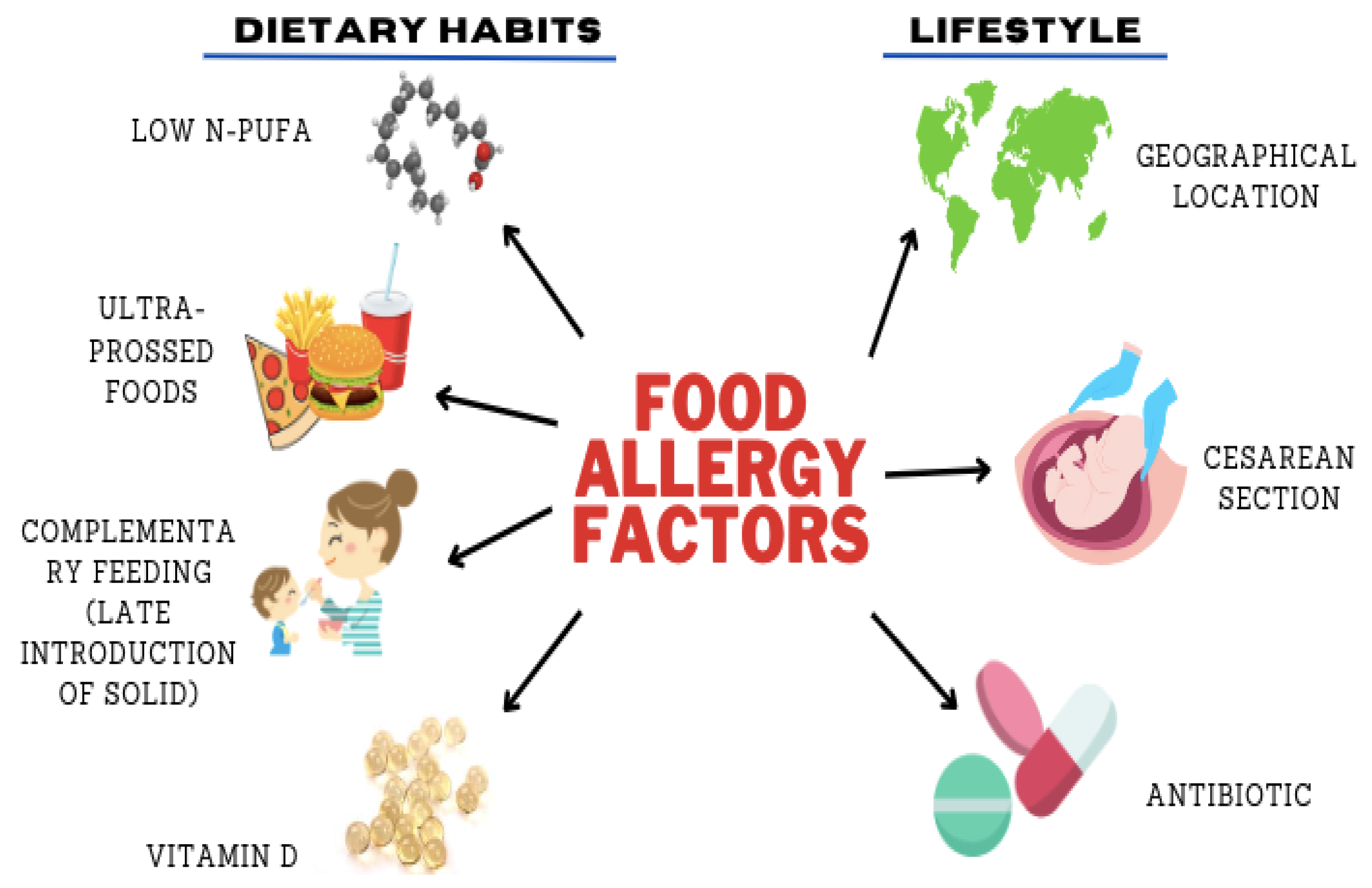
3.2. Effect of Dietary Habits on FA
3.2.1. Fatty Acid/Polyunsaturated Fatty Acid (PUFA)
3.2.2. Ultra-Processed Foods (UPFs)
3.2.3. Late Introduction/Exposure to Solids
3.2.4. Vitamin D Insufficiency
3.3. Effect of Lifestyle on FA
3.3.1. Geographical Locations/Racial Disparities
3.3.2. Caesarean Section
3.3.3. Antibiotic
3.4. Principal Findings
3.4.1. n-3 PUFA (Polyunsaturated Fatty Acid)
3.4.2. Ultra-Processed Foods (UPFs)
3.4.3. Late Introduction/Exposure to Solid Foods
3.4.4. Vitamin D
3.4.5. Geographic Locations and Racial Disparities
3.4.6. Caesarean Section (CS)
3.4.7. Antibiotics
4. Limitations and Strengths
5. Recommendation
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics and Dissemination
References
- Kanchan, K.; Clay, S.; Irizar, H.; Bunyavanich, S.; Mathias, R.A. Current insights into the genetics of food allergy. J. Allergy Clin. Immunol. 2021, 147, 15–28. [Google Scholar] [CrossRef]
- Rona, R.J.; Keil, T.; Summers, C.; Gislason, D.; Zuidmeer, L.; Sodergren, E.; Sigurdardottir, S.T. The prevalence of food allergy: A meta-analysis General approach. 2006, 120, 638–646. J. Allergy Clin. Immunol. 2006, 120, 638–646. [Google Scholar] [CrossRef]
- Jackson, C.M.; Mahmood, M.M.; Järvinen, K.M. Farming lifestyle and human milk: Modulation of the infant microbiome and protection against allergy. Acta Paediatr. 2021, 111, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Renz, H.; Allen, K.J.; Sicherer, S.H.; Sampson, H.A.; Lack, G.; Beyer, K.; Oettgen, H.C. Food allergy. Nat. Rev. Dis. Prim. 2018, 4, 17098. [Google Scholar] [CrossRef]
- Mendes, C.; Costa, J.; Vicente, A.A.; Oliveira, M.B.P.P.; Mafra, I. Cashew Nut Allergy: Clinical Relevance and Allergen Characterisation. Clin. Rev. Allergy Immunol. 2019, 57, 1–22. [Google Scholar] [CrossRef]
- Oriel, R.C.; Wang, J. Diagnosis and Management of Food Allergy. Pediatr. Clin. N. Am. 2019, 66, 941–954. [Google Scholar] [CrossRef]
- Laia-Dias, I.; Lozoya-Ibáñez, C.; Skypala, I.; Gama, J.M.R.; Nurmatov, U.; Lourenço, O.; Taborda-Barata, L. Prevalence and risk factors for food allergy in older people: Protocol for a systematic review. BMJ Open 2019, 9, e029633. [Google Scholar] [CrossRef]
- Hoi, A.Y.; Ross, L.; Day, J.; Buchanan, R.R.C. Immunotherapeutic strategies in antiphospholipid syndrome. Intern. Med. J. 2017, 47, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Cosme-Blanco, W.; Arroyo-Flores, E.; Ale, H. Food allergies. Pediatr. Rev. 2020, 41, 403–413. [Google Scholar] [CrossRef]
- Ribeiro, L.W.; Moss, K.M.; Mishra, G.D. Dietary patterns and allergy in children aged 5–12 years in Australia: Findings from the Mothers and Their Children’s Health study. Allergol. Int. 2020, 69, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Krifa, I.; Hallez, Q.; van Zyl, L.E.; Braham, A.; Sahli, J.; Ben Nasr, S.; Shankland, R. Effectiveness of an online positive psychology intervention among Tunisian healthcare students on mental health and study engagement during the COVID-19 pandemic. Appl. Psychol. Health Well-Being 2021, 14, 1228–1254. [Google Scholar] [CrossRef]
- Benedé, S.; Blázquez, A.B.; Chiang, D.; Tordesillas, L.; Berin, M.C. The rise of food allergy: Environmental factors and emerging treatments. EBioMedicine 2016, 7, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.P.; Sicherer, S. Food allergy: Epidemiology, pathogenesis, diagnosis, prevention, and treatment. Curr. Opin. Immunol. 2020, 66, 57–64. [Google Scholar] [CrossRef]
- Savage, J.; Johns, C.B. Food Allergy Epidemiology and Natural History Food allergy Epidemiology Natural history Peanut Milk Egg. Immunol. Allergy Clin. 2015, 35, 45–59. [Google Scholar] [CrossRef]
- Stemeseder, T.; Klinglmayr, E.; Moser, S.; Lang, R.; Himly, M.; Oostingh, G.J.; Zumbach, J.; Bathke, A.C.; Hawranek, T.; Gadermaier, G. Influence of Intrinsic and Lifestyle Factors on the Development of IgE Sensitization. Int. Arch. Allergy Immunol. 2017, 173, 99–104. [Google Scholar] [CrossRef]
- Wang, J.; Vanga, S.K.; Raghavan, V. Effect of pre-harvest and post-harvest conditions on the fruit allergenicity: A review. Crit. Rev. Food Sci. Nutr. 2019, 59, 1027–1043. [Google Scholar] [CrossRef]
- Anvari, S.; Miller, J.; Yeh, C.; Davis, C.M. IgE-Mediated Food Allergy. Clin. Rev. Allergy Immunol. 2019, 57, 244–260. [Google Scholar] [CrossRef]
- Sathe, S.K.; Liu, C.; Zaffran, V.D. Food Allergy. Annu. Rev. Food Sci. Technol. 2016, 7, 191–220. [Google Scholar] [CrossRef]
- Satitsuksanoa, P.; Jansen, K.; Głobińska, A.; van de Veen, W.; Akdis, M. Regulatory immune mechanisms in tolerance to food allergy. Front. Immunol. 2018, 9, 2939. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, L.A.; Finlay, B.B. Early life factors that affect allergy development. Nat. Rev. Immunol. 2017, 17, 518–528. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Sampson, H.A. Food allergy. J. Allergy Clin. Immunol. 2010, 125 (Suppl. S2), S116–S125. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Freeland, D.; Nadeau, K. Food allergy: Immune mechanisms, diagnosis and immunotherapy. Nat. Rev. Immunol. 2016, 16, 751–765. [Google Scholar] [CrossRef]
- Boyce, J.A. Guidelines for the diagnosis and management of food allergy in the United States: Report of the NIAID-sponsored expert panel. J. Allergy Clin. Immunol. 2010, 126, 301–402. [Google Scholar] [CrossRef]
- Gupta, R.S.; Warren, C.M.; Smith, B.M.; Jiang, J.; Blumenstock, J.A.; Davis, M.M.; Schleimer, R.P.; Nadeau, K.C. Prevalence and Severity of Food Allergies Among US Adults. JAMA Netw. Open 2019, 2, e185630. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Vanga, S.K.; McCusker, C.; Raghavan, V. A Comprehensive Review on Kiwifruit Allergy: Pathogenesis, Diagnosis, Management, and Potential Modification of Allergens Through Processing. Compr. Rev. Food Sci. Food Saf. 2019, 18, 500–513. [Google Scholar] [CrossRef] [PubMed]
- Messina, M.; Venter, C. Recent Surveys on Food Allergy Prevalence. Nutr. Today 2020, 55, 22–29. [Google Scholar] [CrossRef]
- Pacific, A. Asia Pacific allergy. Asia Pac. Allergy 2012, 2, 76–85. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C. Chapter 11: Scoping reviews. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Malley, O. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- McGowan, J.; Straus, S.; Moher, D.; Langlois, E.V.; O’Brien, K.K.; Horsley, T.; Aldcroft, A.; Zarin, W.; Garitty, C.M.; Hempel, S.; et al. Reporting scoping reviews—PRISMA ScR extension. J. Clin. Epidemiol. 2020, 123, 177–179. [Google Scholar] [CrossRef]
- Papathoma, E.; Triga, M.; Fouzas, S. Cesarean section delivery and development of food allergy and atopic dermatitis in early childhood. Pediatr. Allergy Immunol. 2016, 27, 419–424. [Google Scholar] [CrossRef]
- Rosendahl, J.; Fogelholm, M.; Pelkonen, A. A History of Cow’s Milk Allergy Is Associated with Lower Vitamin D Status in Schoolchildren. Horm. Res. Paediatr. 2017, 88, 244–250. [Google Scholar] [CrossRef]
- Van Zyl, I. Fatty Acid and Micronutrient Intake and Status in Association with Allergy among Pregnant Urban Women in South Africa. Ph.D. Thesis, North-West University, Potchefstroom, South Africa, 2018. [Google Scholar]
- Li, M.; Lu, Z.K.; Amrol, D.J.; Mann, J.R.; Hardin, J.W.; Yuan, J.; Cox, C.L.; Love, B.L. Antibiotic Exposure and the Risk of Food Allergy: Evidence in the US Medicaid Pediatric Population. J. Allergy Clin. Immunol. Pract. 2019, 7, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Hicke-Roberts, A.; Wennergren, G.; Hesselmar, B. Late introduction of solids into infants’ diets may increase the risk of food allergy development. BMC Pediatr. 2020, 20, 273. [Google Scholar] [CrossRef]
- Cho, S.I.; Lee, H.; Lee, D.H.; Kim, K.H. Association of frequent intake of fast foods, energy drinks, or convenience food with atopic dermatitis in adolescents. Eur. J. Nutr. 2020, 59, 3171–3182. [Google Scholar] [CrossRef]
- Kayale, L.B.; Ling, J.; Henderson, E.; Carter, N. The influence of cultural attitudes to nut exposure on reported nut allergy: A pilot cross sectional study. PLoS ONE 2020, 15, e0234846. [Google Scholar] [CrossRef]
- Annesi-Maesano, I.; Fleddermann, M.; Hornef, M.; von Mutius, E.; Pabst, O.; Schaubeck, M.; Fiocchi, A. Allergic diseases in infancy: I—Epidemiology and current interpretation. World Allergy Organ. J. 2021, 14, 100591. [Google Scholar] [CrossRef]
- Best, K.P.; Gold, M.; Kennedy, D.; Martin, J.; Makrides, M. Omega-3 long-chain PUFA intake during pregnancy and allergic disease outcomes in the offspring: A systematic review and meta-analysis of observational studies and randomized controlled trials. Am. J. Clin. Nutr. 2016, 103, 128–143. [Google Scholar] [CrossRef]
- Bärebring, L.; Nwaru, B.I.; Lamberg-Allardt, C.; Thorisdottir, B.; Ramel, A.; Söderlund, F.; Arnesen, E.K.; Dierkes, J.; Åkesson, A. Supplementation with long chain n-3 fatty acids during pregnancy, lactation, or infancy in relation to risk of asthma and atopic disease during childhood: A systematic review and meta-analysis of randomized controlled clinical trials. Food Nutr. Res. 2022, 66, 8842. [Google Scholar] [CrossRef]
- Wang, C.S.; Wang, J.; Zhang, X.; Zhang, L.; Zhang, H.P.; Wang, L.; Wood, L.G.; Wang, G. Is the consumption of fast foods associated with asthma or other allergic diseases? Respirology 2018, 23, 901–913. [Google Scholar] [CrossRef] [PubMed]
- Melo, B.; Rezende, L.; Machado, P.; Gouveia, N.; Levy, R. Associations of ultra-processed food and drink products with asthma and wheezing among Brazilian adolescents. Pediatr. Allergy Immunol. 2018, 29, 504–511. [Google Scholar] [CrossRef]
- Hoffam, R. Ultra-Processed Foods Are Harmful for Our Health—Here’s Why. The Conversation. 2022. Available online: https://interestingengineering.com/health/ultra-processed-food-harmful (accessed on 22 July 2023).
- Kakieu Djossi, S.; Khedr, A.; Neupane, B.; Proskuriakova, E.; Jada, K.; Mostafa, J.A. Food Allergy Prevention: Early Versus Late Introduction of Food Allergens in Children. Cureus 2022, 14, e21046. [Google Scholar] [CrossRef]
- Olenec, J.; Gern, J.E. Age at first introduction of cow milk products and other food products in relation to infant atopic manifestations in the first 2 years of life: The KOALA birth cohort study. Pediatrics 2009, 124. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Erkkola, M.; Ahonen, S.; Kaila, M.; Haapala, A.M.; Kronberg-Kippilä, C.; Salmelin, R.; Veijola, R.; Ilonen, J.; Simell, O.; et al. Age at the introduction of solid foods during the first year and allergic sensitization at age 5 years. Pediatrics 2010, 125, 50–59. [Google Scholar] [CrossRef]
- Dai, N.; Li, X.; Wang, S.; Wang, J.; Gao, Y.; Li, Z. Timing of food introduction to the infant diet and risk of food allergy: A systematic review and Meta-analysis. J. Chin. Med. Assoc. 2021, 59, 563–569. [Google Scholar] [CrossRef]
- Smith, P.K.; Masilamani, M.; Li, X.-M.; Sampson, H.A. The false alarm hypothesis: Food allergy is associated with high dietary advanced glycation end-products and proglycating dietary sugars that mimic alarmins. J. Allergy Clin. Immunol. 2017, 139, 429–437. [Google Scholar] [CrossRef]
- Vassallo, M.F.; Camargo, C.A. Potential mechanisms for the hypothesized link between sunshine, vitamin D, and food allergy in children. J. Allergy Clin. Immunol. 2010, 126, 217–222. [Google Scholar] [CrossRef]
- Lieberman, J.A.; Greenhawt, M.; Nowak-Wegrzyn, A. The environment and food allergy. Ann. Allergy Asthma Immunol. 2018, 120, 455–457. [Google Scholar] [CrossRef]
- Allen, K.J.; Koplin, J.J.; Ponsonby, A.L.; Gurrin, L.C.; Wake, M.; Vuillermin, P.; Martin, P.; Matheson, M.; Lowe, A.; Robinson, M.; et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J. Allergy Clin. Immunol. 2013, 131, 1109–1116.e6. [Google Scholar] [CrossRef]
- Willits, E.K.; Wang, Z.; Jin, J.; Patel, B.; Motosue, M.; Bhagia, A.; Almasri, J.; Erwin, P.J.; Kumar, S.; Joshi, A.Y. Vitamin D and food allergies in children: A systematic review and meta-analysis. Allergy Asthma Proc. 2017, 38, e21–e28. [Google Scholar] [CrossRef]
- Psaroulaki, E.; Katsaras, G.N.; Samartzi, P.; Chatziravdeli, V.; Psaroulaki, D.; Oikonomou, E.; Tsitsani, P. Association of food allergy in children with vitamin D insufficiency: A systematic review and meta-analysis. Eur. J. Pediatr. 2023, 182, 1533–1554. [Google Scholar] [CrossRef]
- Panjari, M.; Koplin, J.J.; Dharmage, S.C.; Peters, R.L.; Gurrin, L.C.; Sawyer, S.M.; Mcwilliam, V.; Eckert, J.K.; Vicendese, D.; Erbas, B.; et al. Nut allergy prevalence and differences between Asian-born children and Australian-born children of Asian descent: A state-wide survey of children at primary school entry in Victoria, Australia. Clin. Exp. Allergy 2016, 46, 602–609. [Google Scholar] [CrossRef]
- Feng, H.; Xiong, X.; Chen, Z.; Xu, Q.; Zhang, Z.; Luo, N.; Wu, Y. Prevalence and Influencing Factors of Food Allergy in Global Context: A Meta-Analysis. Int. Arch. Allergy Immunol. 2023, 184, 320–352. [Google Scholar] [CrossRef]
- Thomas, S.; Meadows, J.; McQueen, K.A.K. Access to Cesarean Section Will Reduce Maternal Mortality in Low-Income Countries: A Mathematical Model. World J. Surg. 2016, 40, 1537–1541. [Google Scholar] [CrossRef]
- Gu, L.; Zhang, W.; Yang, W.; Liu, H. Systematic review and meta-analysis of whether cesarean section contributes to the incidence of allergic diseases in children: A protocol for systematic review and meta-analysis. Medicine 2019, 98, 2–5. [Google Scholar] [CrossRef]
- Sbihi, H.; Boutin, R.C.T.; Cutler, C.; Suen, M.; Finlay, B.B.; Turvey, S.E. Thinking bigger: How early-life environmental exposures shape the gut microbiome and influence the development of asthma and allergic disease. Allergy Eur. J. Allergy Clin. Immunol. 2019, 74, 2103–2115. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Westergaard, T. Caesarean delivery and risk of atopy and allergic disesase: Meta-analyses. Clin. Exp. Allergy 2008, 38, 634–642. [Google Scholar] [CrossRef]
- Xiong, Z.; Zhou, L.; Chen, Y.; Wang, J.; Zhao, L.; Li, M.; Chen, I.; Krewski, D.; Wen, S.W.; Xie, R. Prevalence of eczema between cesarean-born and vaginal-born infants within 1 year of age: A systematic review and meta-analysis. Eur. J. Pediatr. 2022, 181, 2237–2247. [Google Scholar] [CrossRef]
- Yang, X.; Zhou, C.; Guo, C.; Wang, J.; Chen, I.; Wen, S.W.; Krewski, D.; Yue, L.; Xie, R.H. The prevalence of food allergy in cesarean-born children aged 0–3 years: A systematic review and meta-analysis of cohort studies. Front. Pediatr. 2023, 10, 1044954. [Google Scholar] [CrossRef]
- Loo, E.X.L.; Sim, J.Z.T.; Loy, S.L.; Goh, A.; Chan, Y.H.; Tan, K.H.; Yap, F.; Gluckman, P.D.; Godfrey, K.M.; Van Bever, H.; et al. Europe PMC Funders Group Associations between caesarean delivery and allergic outcomes: Results from the GUSTO study. Ann. Allergy Asthma Immunol. 2017, 118, 636–638. [Google Scholar] [CrossRef]
- Verbanas, P. C-Section Delivery Prevents Babies from Receiving Beneficial Germs in Their Mother’s Microbiome, Which, in Turn, Affects Immune System Development, Says Rutgers Researcher. Rutgers University. Available online: https://www.rutgers.edu/news/hidden-reason-children-born-c-section-are-more-likely-develop-asthma (accessed on 26 July 2023).
- Ahmadizar, F.; Vijverberg, S.J.H.; Arets, H.G.M.; de Boer, A.; Lang, J.E.; Garssen, J.; Kraneveld, A.; Maitland-van der Zee, A.H. Early-life antibiotic exposure increases the risk of developing allergic symptoms later in life: A meta-analysis. Allergy Eur. J. Allergy Clin. Immunol. 2018, 73, 971–986. [Google Scholar] [CrossRef]
- Netea, S.A.; Messina, N.L.; Curtis, N. Early-life antibiotic exposure and childhood food allergy: A systematic review. J. Allergy Clin. Immunol. 2019, 144, 1445–1448. [Google Scholar] [CrossRef]
- Zhong, Y.; Zhang, Y.; Wang, Y.; Huang, R. Maternal antibiotic exposure during pregnancy and the risk of allergic diseases in childhood: A meta-analysis. Pediatr. Allergy Immunol. 2021, 32, 445–456. [Google Scholar] [CrossRef]
- Perkin, M.R.; Logan, K.; Tseng, A.; Raji, B.; Ayis, S.; Peacock, J.; Brough, H.; Marrs, T.; Radulovic, S.; Craven, J.; et al. Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N. Engl. J. Med. 2016, 374, 1733–1743. [Google Scholar] [CrossRef]
- Cukrowska, B. Microbial and nutritional programming—The importance of the microbiome and early exposure to potential food allergens in the development of allergies. Nutrients 2018, 10, 1541. [Google Scholar] [CrossRef]
- D’Auria, E.; Peroni, D.G.; Sartorio, M.U.A.; Verduci, E.; Zuccotti, G.V.; Venter, C. The Role of Diet Diversity and Diet Indices on Allergy Outcomes. Front. Pediatr. 2020, 8, 545. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Number | Question/Inquiry | Knowledge of Onset |
|---|---|---|
| 1 | Was one of the most common allergenic meals consumed two hours or less before the response started? | Most food allergies are caused by a small number of foods, including cow’s milk, eggs, peanuts, tree nuts, shellfish, finned fish, wheat, and soy. |
| 2 | Has there been prior consumption of the suspected food? | If you have previously tolerated a dish, it is less probable that this time will be different. |
| 3 | Has there been a previous response? | Reactions to the same food repeatedly indicate that it is more likely the cause. |
| 4 | What age did the food allergy start? | The most common causes of allergy onset in kids are allergies to milk, eggs, wheat, or peanuts, while the most common causes of allergy onset in adults are allergies to nuts, shellfish, or pollen–food allergy syndrome. |
| 5 | How was the food prepared? | Although reactions to small amounts of food can also happen, larger amounts of food are more likely to do so. For example, a person who is sensitive to whole cow’s milk or raw eggs may be able to handle smaller amounts of heated versions in baked products (such cookies or muffins). |
| 6 | Were there any enhancing influences? | Menstruation, exercise, infection, usage of pharmaceuticals (such as nonsteroidal anti-inflammatory drugs), and alcohol intake can increase responsiveness or make a reaction more severe. |
| 7 | What signs and symptoms did the patient experience? | IgE-mediated reactions are characterized by symptoms in the skin, lungs, stomach, and heart. An older person would feel “doom”, whereas a small child might weep, stop playing, or become listless. |
| Concept | Keyword | MeSH |
|---|---|---|
| Concept 1 | Food hypersensitivity | “Food Hypersensitivity” [Mesh] OR “Food Hypersensitivity” OR “FA” OR Hypersensitivities OR “hypersensitivity” OR “allergic” OR “sensitivities” OR “Allergies” OR “Food Allergies” OR “food” OR “oral allergy syndrome” |
| Concept 2 | Prevalence | “Prevalence” [Mesh] OR “Prevalence*” OR “epidemiology” OR “increase” OR “rise” |
| Concept 3 | Lifestyle | “Life Style” [Mesh] “Lifestyle*” OR “behavior” OR “way of life” OR “condition” OR “situation” |
| Concept 4 | Dietary habits | “Feeding Behavior” [Mesh] OR “Feeding Behavior” OR “diet” OR “feeding” OR “eating behavior” OR “consumption habit” OR “Feeding-Related Behaviors” OR “feeding pattern” OR “food habit” |
| Factors | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Settings | Any country; studies where specified data (see below) were collected with timeline between 2016 and 2021 | Studies reporting on data collected before 2016 |
| Participants | Any age | Participant groups selected based on a pre-existing health condition (including obesity, eating disorders, malnutrition) |
| Outcomes | A measure of diet and lifestyle (quantitative synthesis) | No link to the effect of lifestyle and diet on FAStudies reporting tracking of cigarette smokingStudies reporting solely alcohol intakeStudies reporting eating disorders or weight reduction behaviorsStudies reporting obesity |
| Study Type | Open access (cross-sectional studies, longitudinal prospective quantitative studies, with data reported including on specified outcome, human subjects) | Review papers, books, animal subjects, qualitative studies |
| Publication type | Journal article | Conference abstract, study protocol, report, thesis, dissertation, book, professional journal |
| Publication Date | 2016–2020 | Published date other than the selected date |
| Language | English | Languages other than English |
| Reference/Dates | Country | Sample Size and Age | Design of Publication | Study Limitations | Main Outcome |
|---|---|---|---|---|---|
| Papathoma et al., (2016) [34] | Greece | n = 459, 34 weeks | Prospective birth cohort study/Pediatric Allergy and Immunology | Data from a single center and a limited urban/suburban area. Small study sample. Lack of socioeconomical data. The proposed intermediate role of gut microbiota remains an assumption. | Delivery by CS predisposes the development of FAs but not atopic dermatitis in early childhood. Caesarean section delivery seems to upregulate the immune response to food allergens, especially in children with allergic predispositions. |
| Rosendahl et al., (2017) [35] | Finland | n = 171, 10 years | Cross-sectional study/Hormone Research in Paediatrics | This was a cross-sectional study with small N. Lacked information on consumed portion sizes and the use of vitamin-D-fortified fat spreads. | Fortification of food products with vitamin D have been successful in improving vitamin D status in children. |
| Van Zyl, (2018) [36] | South Africa | n = 250, women/mothers | Longitudinal observational research/Journal Article | The study’s limitations include a small sample size, the utilization of dietary intake data for zinc and vitamin E instead of assessing their actual status, and the inherent shortcomings associated with employing a Quantitative Food Frequency Questionnaire (QFFQ) to estimate accurate dietary intake. | A potential up-regulation of both fatty acid desaturase and elongase enzyme activity with a notable emphasis on elongase was observed. This finding predominantly highlights the involvement of the n-6 fatty acid pathway, suggesting a potential shift towards a more pro-inflammatory state. |
| Li et al., (2019) [37] | US | 1,001294, 2–18 years | Cross-sectional study /Journal of Allergy and Clinical Immunology: In Practice | N/A | Recent research has established a robust association between the exposure to antibiotics and the development of food allergies. |
| Ribeiro et al., (2020) [10] | Australia | n = 5780, 5–12 years | Cross-sectional cohort study/Allergology International | Mothers reported the daily frequency of their children’s intake using a specialized tool known as the Children’s Dietary Questionnaire. | Asian children who were born in Australia exhibited a higher prevalence of nut allergy compared to Asian children who had immigrated to Australia. |
| Hicke-Robert et al., (2020) [38] | Sweden | n = 1838, 7–8 years | Cross-sectional studies/BMC Pediatrics | The response rate in this study was approximately 60%, which is a common level observed in con-temporary epidemiological studies. | Late introduction of solids into infants’ diets may increase the risk of food allergy development. |
| Cho et al., (2020) [39] | Korea | n = 53,373, 15.03 ± 1.75 years | Cross-sectional study/European Journal of Nutrition | The severity of food allergies (FAs) in individuals who had recently been diagnosed or previously diagnosed was assessed through a survey. However, the survey did not provide a means to evaluate the severity of FA. Additionally, evaluating long-term food intake proved challenging. Furthermore, it is important to consider that responses or expo-sures to food in different countries may vary due to racial or cultural differences. | Frequent intake of fast foods, energy drinks, and convenience food was related to recently diagnosed FA in adolescents. |
| Kayale et al., (2020) [40] | UK | n = 3300, 3–16 years | Cross-sectional study/PLoS ONE | The data collection for this study relied solely on a questionnaire, without any clinical data being collected. Consequently, the accuracy of the findings is dependent on the respondents’ ability to recall information accurately. It is well known that recall can be both biased and inaccurate, with a potential limitation of parents forgetting events from early childhood due to the wide age range of children (3–16 years) included in the study. Moreover, it is worth noting that the overall response rate was 34%. | Regular and early consumption of a moderate number of nuts during infancy, as well as maternal ingestion of nuts during pregnancy or while breastfeeding, is believed to support the development of tolerance. |
| Factors | Author(s) | Publication Year | Factors | Country | Odd Ratio | Lower CI | Upper CI |
|---|---|---|---|---|---|---|---|
| Lifestyle | Papathoma et al. [34] | 2016 | C-section | Greece | 3.15 | 1.14 | 8.7 |
| Rosendahl et al. [35] | 2017 | Vitamin D | Finland | 0.14 | 0.039 | 0.241 | |
| Hicker-Rober [38] | 2020 | Late introduction | Sweden | 1.8 | 1.15 | 3.02 | |
| Dietary habits | Li et al. [37] | 2019 | Antibiotic | US | 1.4 | 1.34 | 1.45 |
| Ribeiro et al. [10] | 2018 | Ultra-processed foods | Australia | 1.28 | 1.08 | 1.51 | |
| Van Zyl et al. [36] | 2018 | n-3 PUFA | South Africa | 1.21 | 1.13 | 1.37 | |
| Cho et al. [39] | 2020 | Ultra-processed foods | Korea | 1.405 | 1.15 | 1.717 | |
| Kayale et al. [40] | 2020 | Geographical Location | UK | 1.0706 | 0.1108 | 10.3493 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rennie, G.H.; Zhao, J.; Camus-Ela, M.; Shi, J.; Jiang, L.; Zhang, L.; Wang, J.; Raghavan, V. Influence of Lifestyle and Dietary Habits on the Prevalence of Food Allergies: A Scoping Review. Foods 2023, 12, 3290. https://doi.org/10.3390/foods12173290
Rennie GH, Zhao J, Camus-Ela M, Shi J, Jiang L, Zhang L, Wang J, Raghavan V. Influence of Lifestyle and Dietary Habits on the Prevalence of Food Allergies: A Scoping Review. Foods. 2023; 12(17):3290. https://doi.org/10.3390/foods12173290
Chicago/Turabian StyleRennie, Gardiner Henric, Jinlong Zhao, Mukeshimana Camus-Ela, Jialu Shi, Lan Jiang, Lili Zhang, Jin Wang, and Vijaya Raghavan. 2023. "Influence of Lifestyle and Dietary Habits on the Prevalence of Food Allergies: A Scoping Review" Foods 12, no. 17: 3290. https://doi.org/10.3390/foods12173290
APA StyleRennie, G. H., Zhao, J., Camus-Ela, M., Shi, J., Jiang, L., Zhang, L., Wang, J., & Raghavan, V. (2023). Influence of Lifestyle and Dietary Habits on the Prevalence of Food Allergies: A Scoping Review. Foods, 12(17), 3290. https://doi.org/10.3390/foods12173290