


Dietary Acrylamide Exposure and Cancer Risk: A Systematic Approach to Human Epidemiological Studies



Abstract
:1. Introduction
- Acrylamide formation mechanisms in foods: Uncertainties regarding acrylamide formation mechanisms in foods still continue [5]. It is reported that acrylamide is formed at high levels, especially in foods rich in carbohydrates, through thermal process above 120 °C [6]. Although it varies according to the type of food, the Maillard Reaction is accepted as the primary mechanism in the formation of acrylamide [7]. Apart from this mechanism, other mechanisms are also described including glycerol, fatty acids, aspartic acid carnosine, B-alanine, pyruvic acid, serine and cysteine compounds, also called acrolein pathway, and resulting in acrylamide formation [8,9,10].
- Acrylamide levels in foods: The level of acrylamide in foods varies depending on many factors such as the type and content of food, processing technique, and storage conditions [11]. In this context, much research, including traditional foods specific to societies, especially foods that are widely consumed around the world, has been carried out. In recent studies, acrylamide levels were found to be 779–1299 μg/kg in French fries [12], and 211–3515 μg/kg [13] in potato chips, which is quite high compared to the acrylamide levels in other foods. Acrylamide levels have been reported to be 31–454 μg/kg [14] in bread, 135–1139 μg/kg [13] in coffee, and 5.30–79.5 μg/kg in ready-to-drink (brewed) coffee [15]. It was determined to be <20–639 μg/kg [16], 15–109 μg/kg [17], and 12.3–1270 μg/kg [18] in breakfast cereal, infant formulas and baby biscuits, respectively. Acrylamide levels were reported to be <LOQ–143 µg/kg for some traditional Polish foods [19], and 11.7–527 μg/kg for some Turkish traditional foods [20].
- Acrylamide reduction in foods: The detection of acrylamide in foods led to studies on reducing acrylamide levels in foods, and many studies have been conducted on different foods. In studies within this scope, many factors, such as the type and amount of ingredient in product formulations, the pH and moisture level of the product, the degree and duration of the heat applied for the production or consumption of the food, oil type and storage conditions were changed to reduce the level of acrylamide in foods [7,12,21,22,23,24,25,26,27]. In addition, the acrylamide level in foods were tried to be reduced before thermal process by using many traditional and modern methods, such as immersing foods in various solutions and applying asparaginase enzyme, applying high pressure, heating in microwave ovens, using ultrasound and pulsed electric fields [7,27,28,29,30,31,32,33].
- Dietary acrylamide exposure: It is very important to assess the level of exposure to consumers to acrylamide-contaminated foods in terms of understanding the potential health risks of acrylamide and developing new strategies for the future [34]. The European Commission and Joint FAO/WHO Expert Committee to Food Additives (JECFA) reported that studies on exposure and risk assessments arising from acrylamide-contaminated foods are not sufficient and there is a need for systematic and comprehensive studies in this context [35,36]. In this context, many countries and researchers conduct risk analyses for dietary acrylamide exposure and evaluate acrylamide in terms of health. In studies of dietary acrylamide exposure, human exposure to acrylamide from different foods was determined to be 0.43 µg/kg bw/day in Poland [37], 0.22 µg/kg bw/day in Turkey [38], and 0.38 µg/kg bw/day in Portugal [39]. EFSA (2015) stated that infants and children are the group most exposed to acrylamide (average acrylamide intake 0.5–1.9 µg/kg bw/day), and infant formulas have a significant share in this exposure [11]. In the same report, it was stated that the mean acrylamide exposure in young, adult, elderly and older groups ranged between 0.4 and 0.9 µg/kg bw/day.
- The effect of acrylamide on health: Acrylamide, which is taken into the body through contact, digestion and respiration, is easily absorbed and dispersed in the body because it has a low molecular weight. The excretion of acrylamide and its compounds from the body is quite rapid. It was reported that acrylamide taken into the organism can bind to DNA, RNA and proteins in some tissues and cells by undergoing chemical reactions, and their desire and potential to form compounds with these substances is high [40,41,42,43]. Acrylamide was identified as a “possibly carcinogenic to humans” compound by the International Agency for Research on Cancer (IARC) in 1994 and classified in group 2A [44,45]. Acrylamide is predicted to be a human carcinogenic [46]. The European Commission has classified acrylamide in Category 1B as a carcinogen and mutagen, and in Category 2 as a reproductive toxicant [35]. The European Chemical Agency (2022) included acrylamide in the List of Substances of Very High Concern [47]. The widespread use of acrylamide as a synthetic chemical and the surprising discovery that it occurs naturally in foods raises a complex problem. Is the presence of acrylamide in foods risky for consumers’ health?
2. Materials and Methods
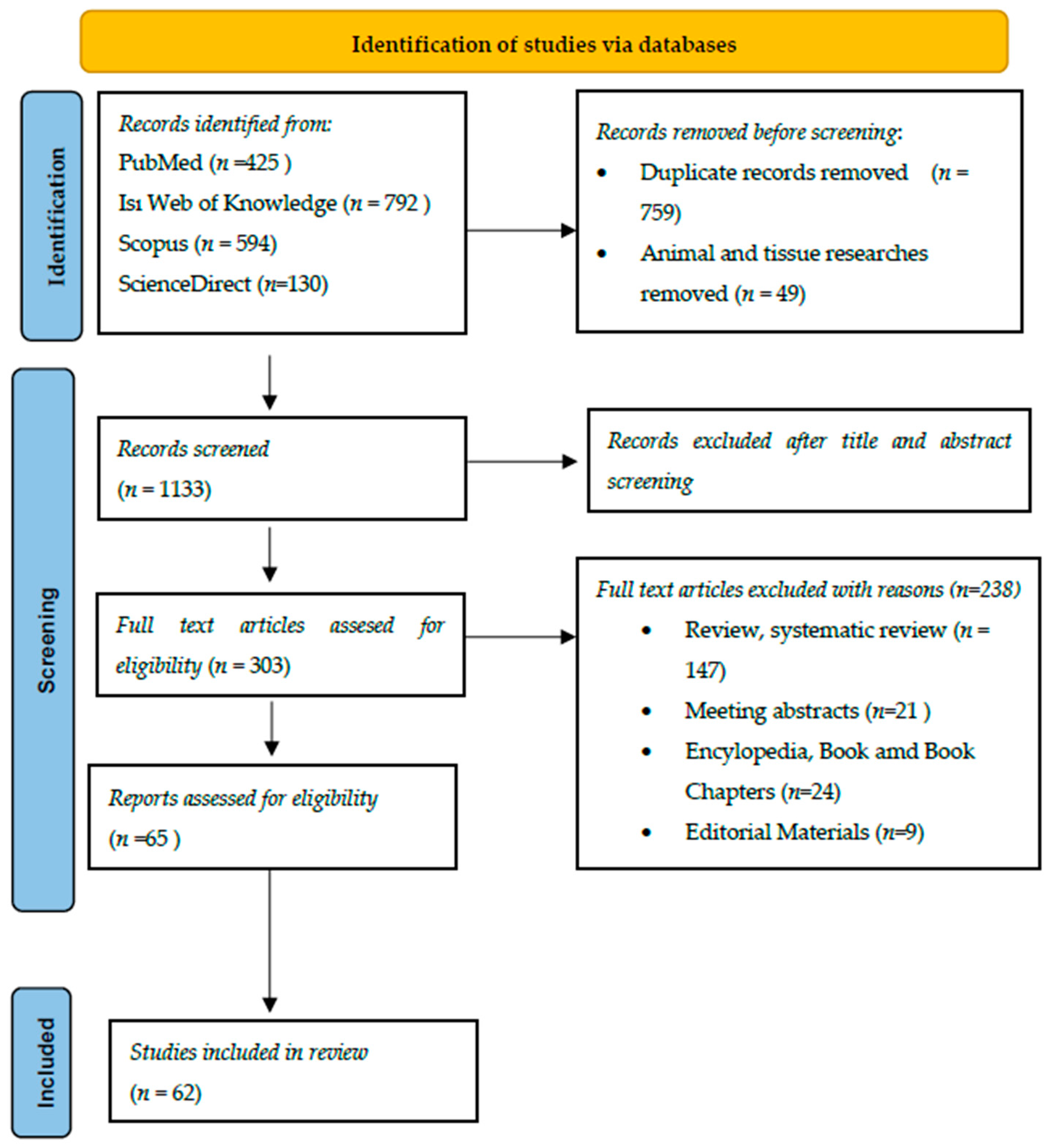
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
3.1. First Part
3.1.1. Prospective Cohort Studies
3.1.2. Case Cohort Studies
3.1.3. Case Control Studies
3.1.4. Meta-Analysis Studies
3.2. Second Part
4. Discussion
4.1. First Part
4.2. Second Part
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- International Programme on Chemical Safety (IPCS). Acrylamide. 2018. Available online: http://www.inchem.org/documents/pims/chemical/pim652.htm#PartTitle:1.%20%20NAME (accessed on 3 October 2022).
- Kumar, J.; Das, S.; Teoh, S.L. Dietary acrylamide and the risks of developing cancer: Facts to ponder. Front. Nutr. 2018, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institutes of Health (NIH). Acrylamid. 2018. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/acrylamide#section=Top (accessed on 6 November 2022).
- Tareke, E.; Rydberg, P.; Karlsson, P.; Eriksson, S.; Tornqvist, M. Analysis of acrylamide, a carcinogen formed in heated foodstuffs. J. Agricul. Food Chem. 2002, 51, 4998–5006. [Google Scholar] [CrossRef] [PubMed]
- Semla, M.; Goc, Z.; Martiniaková, M.; Omelka, R.; Formicki, G. Acrylamide: A common food toxin related to physiological functions and health. Phys. Res. 2017, 66, 205–217. [Google Scholar] [CrossRef]
- Stadler, R.H.; Blank, I.; Varga, N.; Robert, F.; Hau, J.; Guy, P.A.; Robert, M.C.; Riediker, S. Food chemistry: Acrylamide from Maillard reaction products. Nature 2022, 419, 449–450. [Google Scholar] [CrossRef] [PubMed]
- Maan, A.A.; Anjum, M.A.; Khan, M.K.I.; Nazir, A.; Saeed, F.; Afzaal, M.; Aadil, R.M. Acrylamide formation and different mitigation strategies during food processing–a review. Food Rev. Int. 2022, 38, 70–87. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, P.; Chen, F.; Yuan, Y.; Zhu, Y.; Yan, H.; Hu, X. Role of plant polyphenols in acrylamide formation and elimination. Food Chem. 2015, 186, 46–53. [Google Scholar] [CrossRef]
- Ou, J.; Zheng, J.; Huang, J.; Ho, C.T.; Ou, S. Interaction of acrylamide, acrolein, and 5-hydroxymethylfurfural with amino acids and DNA. J. Agricul. Food Chem. 2020, 68, 5039–5048. [Google Scholar] [CrossRef]
- Mollakhalili-Meybodi, N.; Khorshidian, N.; Nematollahi, A.; Arab, M. Acrylamide in bread: A review on formation, health risk assessment, and determination by analytical techniques. Environ. Sci. Pollut. Res. 2021, 28, 15627–15645. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Scientific Opinion on Acrylamide in Food. EFSA J. 2015, 13, 4104. [Google Scholar] [CrossRef] [Green Version]
- Basaran, B.; Turk, H. The influence of consecutive use of different oil types and frying oil in French fries on the acrylamide level. J. Food Comp. Anal. 2021, 104, 104177. [Google Scholar] [CrossRef]
- Deribew, H.A.; Woldegiorgis, A.Z. Acrylamide levels in coffee powder, potato chips and French fries in Addis Ababa city of Ethiopia. Food Cont. 2021, 123, 107727. [Google Scholar] [CrossRef]
- Esposito, F.; Velotto, S.; Rea, T.; Stasi, T.; Cirillo, T. Occurrence of acrylamide in Italian baked products and dietary exposure assessment. Molecules 2020, 25, 4156. [Google Scholar] [CrossRef]
- Basaran, B.; Aydın, F.; Kaban, G. The determination of acrylamide content in brewed coffee samples marketed in Turkey. Food Addit. Contam. Part A 2020, 37, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Mesías, M.; Sáez-Escudero, L.; Morales, F.J.; Delgado-Andrade, C. Reassessment of acrylamide content in breakfast cereals. Evolution of the Spanish market from 2006 to 2018. Food Cont. 2019, 105, 94–101. [Google Scholar] [CrossRef]
- Esposito, F.; Nolasco, A.; Caracciolo, F.; Velotto, S.; Montuori, P.; Romano, R.; Stasi, T.; Cirillo, T. Acrylamide in baby foods: A probabilistic exposure assessment. Foods 2021, 10, 2900. [Google Scholar] [CrossRef] [PubMed]
- Basaran, B.; Aydın, F. Determination of acrylamide levels in infant formulas and baby biscuits sold in Turkey. Lett. Appl. NanoBioSci. 2022, 11, 3155–3165. [Google Scholar] [CrossRef]
- Cieslik, I.; Cieslik, E.; Topolska, K.; Surma, M. Dietary acrylamide exposure from traditional food products in Lesser Poland and associated risk assessment. Ann. Agric. Environ. Med. 2020, 27, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Basaran, B.; Faiz, O. Determining the levels of acrylamide in some traditional foods unique to Turkey and risk assessment. Iran. J. Pharm. Res. 2022, 21, e123948. [Google Scholar] [CrossRef]
- Rydberg, P.; Eriksson, S.; Tareke, E.; Karlsson, P.; Ehrenberg, L.; Törnqvist, M. Investigations of factors that influence the acrylamide content of heated foodstuffs. J. Agric. Food Chem. 2003, 51, 7012–7018. [Google Scholar] [CrossRef]
- Amrein, T.M.; Bachmann, S.; Noti, A.; Biedermann, M.; Barbosa, M.F.; Biedermann-Brem, S.; Grob, K.; Keise, A.; Realini, P.; Escher, F.; et al. Potential of acrylamide formation, sugars, and free asparagine in potatoes: A comparison of cultivars and farming systems. J. Agric. Food Chem. 2003, 51, 5556–5560. [Google Scholar] [CrossRef]
- Boz, H.; Karaoğlu, M.M.; Kaban, G. The effects of cooking time and sugar on total phenols, hydroxymethylfurfural and acrylamide content of mulberry leather (pestil). Qual. Assur. Saf. Crop. Foods 2016, 8, 493–500. [Google Scholar] [CrossRef]
- Žilić, S.; Aktağ, I.G.; Dodig, D.; Filipović, M.; Gökmen, V. Acrylamide formation in biscuits made of different wholegrain flours depending on their free asparagine content and baking conditions. Food Res. Int. 2020, 132, 109109. [Google Scholar] [CrossRef]
- Schouten, M.A.; Tappi, S.; Romani, S. Acrylamide in coffee: Formation and possible mitigation strategies—A review. Crit. Rev. Food Sci. Nutr. 2020, 60, 3807–3821. [Google Scholar] [CrossRef]
- Rifai, L.; Saleh, F.A. A review on acrylamide in food: Occurrence, toxicity, and mitigation strategies. Int. J. Toxicol. 2020, 39, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Wang, Y.; Gupta, S.K.; Rosen, C.J. Potato tuber chemical properties in storage as affected by cultivar and nitrogen rate: Implications for acrylamide formation. Foods 2020, 9, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gökmen, V.; Şenyuva, H.Z. Effects of some cations on the formation of acrylamide and furfurals in glucose—Asparagine model system. Eur. Food Res. Technol. 2007, 225, 815–820. [Google Scholar] [CrossRef]
- Pedreschi, F.; Kaack, K.; Granby, K. The effect of asparaginase on acrylamide formation in French fries. Food Chem. 2008, 109, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Antunes-Rohling, A.; Ciudad-Hidalgo, S.; Mir-Bel, J.; Raso, J.; Cebrián, G.; Álvarez, I. Ultrasound as a pretreatment to reduce acrylamide formation in fried potatoes. Innov. Food Sci. Emerg. Technol. 2018, 49, 158–169. [Google Scholar] [CrossRef]
- Genovese, J.; Tappi, S.; Luo, W.; Tylewicz, U.; Marzocchi, S.; Marziali, S.; Romani, S.; Ragni, L.; Rocculi, P. Important factors to consider for acrylamide mitigation in potato crisps using pulsed electric fields. Innov. Food Sci. Emerg. Technol. 2019, 55, 18–26. [Google Scholar] [CrossRef]
- Michalak, J.; Czarnowska-Kujawska, M.; Klepacka, J.; Gujska, E. Effect of microwave heating on the acrylamide formation in foods. Molecules 2020, 25, 4140. [Google Scholar] [CrossRef]
- Nematollahi, A.; Meybodi, N.M.; Khaneghah, A.M. An overview of the combination of emerging technologies with conventional methods to reduce acrylamide in different food products: Perspectives and future challenges. Food Cont. 2021, 127, 108144. [Google Scholar] [CrossRef]
- Basaran, B.; Aydin, F. Estimating the acrylamide exposure of adult individuals from coffee: Turkey. Food Addit. Contam. Part A 2020, 37, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Commission Regulation (EU) 2017/2158 of 20 November 2017 Establishing Mitigation Measures and Benchmark Levels for the Reduction of the Presence of Acrylamide in Food. Available online: https://eur-lex.europa.eu/eli/reg/2017/2158/oj (accessed on 1 November 2022).
- Joint FAO/WHO Expert Committee on Food Additives (JECFA). Evaluation of Certain Food Contaminants. Seventy-Second Report of the Joint FAO/WHO Expert Committee on Food Additives (Rome, 16–25 February 2010). WHO Technical Reports Series 959, India. 2011. Available online: https://apps.who.int/iris/bitstream/handle/10665/44514/WHO?sequence=1 (accessed on 8 September 2022).
- Mojska, H.; Gielecin, I.; Szponar, L.; Oltarzewski, M. Estimation of the dietary acrylamide exposure of the Polish population. Food Chem. Toxicol. 2010, 48, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Basaran, B.; Anlar, P.; Oral, Z.F.Y.; Polat, Z.; Kaban, G. Risk assessment of acrylamide and 5-hydroxymethyl-2-furfural (5-HMF) exposure from bread consumption: Turkey. J. Food Comp. Anal. 2022, 107, 104409. [Google Scholar] [CrossRef]
- Costa, S.A.; Correia, D.; Carvalho, C.; Vilela, S.; Severo, M.; Lopes, C.; Torres, D. Risk characterization of dietary acrylamide exposure and associated factors in the Portuguese population. Food Addit. Contam. Part A 2022, 39, 888–900. [Google Scholar] [CrossRef]
- FAO/WHO (Food and Agricultural Organisation/World health Organisation). FAO/WHO Consultation on the Health Implications of Acrylamide in Food Geneva, 25–27 June 2002. Summary Report. Available online: http://www.who.int/foodsafety/publications/chem/acrylamide_june2002/en/ (accessed on 8 January 2020).
- Shipp, A.; Lawrence, G.; Gentry, R.; McDonald, T.; Bartow, H.; Bounds, J.; Macdonald, N.; Van Landingham, C. Acrylamide: Review of toxicity data and dose-response analyses for cancer and noncancer effects. Crit. Rev. Toxicol. 2008, 36, 481–608. [Google Scholar] [CrossRef]
- Atabati, H.; Abouhamzeh, B.; Abdollahifar, M.A.; Javadinia, S.S.; Bajestani, S.G.; Atamaleki, A.; Raoofi, A.; Fakhri, Y.; Oliveira, C.A.F.; Khaneghah, A.M. The association between high oral intake of acrylamide and risk of breast cancer: An updated systematic review and meta-analysis. Trends Food Sci. Technol. 2020, 100, 155–163. [Google Scholar] [CrossRef]
- Sengul, E.; Gelen, V.; Yildirim, S.; Tekin, S.; Dag, Y. The effects of selenium in acrylamide-induced nephrotoxicity in rats: Roles of oxidative stress, inflammation, apoptosis, and DNA damage. Biol. Trace Elem. Res. 2021, 199, 173–184. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). ACRYLAMIDE (Group 2A). 1994. Available online: https://inchem.org/documents/iarc/vol60/m60-11.html (accessed on 1 November 2022).
- Hogervorst, J.G.; Schouten, L.J. Dietary acrylamide and human cancer; even after 20 years of research an open question. Am. J. Clin. Nutr. 2022, 116, 846–847. [Google Scholar] [CrossRef]
- National Toxicology Program. Toxicology and carcinogenesis studies of acrylamide (CASRN 79-06-1) in F344/N rats and B6C3F1 mice (feed and drinking water studies). Natl. Toxicol. Program Tech. Rep. Ser. 2012, 575, 1–234. [Google Scholar]
- The European Chemical Agency. One Hazardous Chemical Added to the Candidate List. Available online: https://echa.europa.eu/-/one-hazardous-chemical-added-to-the-candidate-list (accessed on 6 November 2022).
- von Stedingk, H.; Vikström, A.C.; Rydberg, P.; Pedersen, M.; Nielsen, J.K.; Segerbäck, D.; Knudsen, L.E.; Törnqvist, M. Analysis of hemoglobin adducts from acrylamide, glycidamide, and ethylene oxide in paired mother/cord blood samples from Denmark. Chem. Res. Toxicol. 2011, 24, 1957–1965. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; Von Stedingk, H.; Botsivali, M.; Agramunt, S.; Alexander, J.; Brunborg, G.; Chatzi, L.; Fleming, S.; Fthenou, E.; Granum, B.; et al. Birth weight, head circumference, and prenatal exposure to acrylamide from maternal diet: The European prospective mother–child study (NewGeneris). Environ. Health Persp. 2012, 120, 1739–1745. [Google Scholar] [CrossRef]
- Duarte-Salles, T.; von Stedingk, H.; Granum, B.; Gutzkow, K.B.; Rydberg, P.; Tornqvist, M.; Mendez, M.A.; Brunborg, G.; Brantsæter, A.L.; Meltzer, H.M.; et al. Dietary acrylamide intake during pregnancy and fetal growth-results from the Norwegian mother and child cohort study (MoBa). Environ. Health Persp. 2013, 121, 374–379. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Environmental Health Criteria 49-Acrylamide; World Health Organization: Geneva, Switzerland, 1985. [Google Scholar]
- Myers, J.E.; Macun, I. Acrylamide Neuropathy in a South-African Factory—An Epidemiologic Investigation. Am. J. Ind. Med. 1991, 19, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Hagmar, L.; Törnqvist, M.; Nordander, C.; Rosén, I.; Bruze, M.; Kautiainen, A.; Magnusson, A.L.; Malmberg, B.; Aprea, P.; Granath, F.; et al. Health effects of occupational exposure to acrylamide using hemoglobin adducts as biomarkers of internal dose. Scand. J. Work Environ. Health 2001, 27, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Goffeng, L.O.; Alvestrand, M.; Ulvestad, B.; Sørensen, K.A.; Skaug, V.; Kjuus, H. Self-reported symptoms and neuropsychological function among tunnel workers previously exposed to acrylamide and N-methylolacrylamide. Scand. J. Work Environ. Health 2011, 37, 136–146. [Google Scholar] [CrossRef] [Green Version]
- Eisenbrand, G. Revisiting the evidence for genotoxicity of acrylamide (AA), key to risk assessment of dietary AA exposure. Arch. Toxicol. 2020, 94, 2939–2950. [Google Scholar] [CrossRef]
- Kucukler, S.; Caglayan, C.; Darendelioğlu, E.; Kandemir, F.M. Morin attenuates acrylamide-induced testicular toxicity in rats by regulating the NF-κB, Bax/Bcl-2 and PI3K/Akt/mTOR signaling pathways. Life Sci. 2020, 261, 118301. [Google Scholar] [CrossRef]
- Yedier, S.K.; Şekeroğlu, Z.A.; Şekeroğlu, V.; Aydın, B. Cytotoxic, genotoxic, and carcinogenic effects of acrylamide on human lung cells. Food Chem. Toxicol. 2022, 161, 112852. [Google Scholar] [CrossRef]
- Galindo, D.E.B.; Vidal-Casariego, A.; Calleja-Fernández, A.; Hernández-Moreno, A.; de la Maza, B.P.; Pedraza-Lorenzo, M.; Rodriguez-Garcia, M.A.; Avila-Turcios, D.M.; Alejo-Ramos, M.; Villar-Taibo, R.; et al. Appetite disorders in cancer patients: Impact on nutritional status and quality of life. Appetite 2017, 114, 23–27. [Google Scholar] [CrossRef]
- Ritchie, H.; Rose, M. Our World in Data. Causes of Death. 2019. Available online: https://ourworldindata.org/causes-of-death (accessed on 15 January 2020).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; PRISMA Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucci, L.A.; Sandin, S.; Bälter, K.; Adami, H.O.; Magnusson, C.; Weiderpass, E. Acrylamide intake and breast cancer risk in Swedish women. JAMA 2005, 293, 1322–1327. [Google Scholar] [CrossRef]
- Pelucchi, C.; Galeone, C.; Levi, F.; Negri, E.; Franceschi, S.; Talamini, R.; Bosetti, C.; Giacosa, A.; La Vecchia, C. Dietary acrylamide and human cancer. Int. J. Cancer 2006, 118, 467–471. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. A prospective study of dietary acrylamide intake and the risk of endometrial, ovarian, and breast cancer. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2304–2313. [Google Scholar] [CrossRef] [Green Version]
- Olesen, T.P.; Olsen, A.; Frandsen, H.; Frederiksen, K.; Overvad, K.; Tjønneland, A. Acrylamide exposure and incidence of breast cancer among postmenopausal women in the Danish Diet, Cancer and Health Study. Int. J. Cancer 2008, 122, 2094–2100. [Google Scholar] [CrossRef]
- Larsson, S.C.; Åkesson, A.; Wolk, A. Long-term dietary acrylamide intake and breast cancer risk in a prospective cohort of Swedish women. Am. J. Epidemiol. 2009, 169, 376–381. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.M.; Mucci, L.A.; Cho, E.; Hunter, D.J.; Chen, W.Y.; Willett, W.C. Dietary acrylamide intake and risk of premenopausal breast cancer. Am. J. Epidemiol. 2009, 169, 954–961. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, G.S.; Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake and estrogen and progesterone receptor-defined postmenopausal breast cancer risk. Breast Cancer Res. Treat. 2010, 122, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.M.; Mucci, L.A.; Rosner, B.A.; Willett, W.C. A prospective study of dietary acrylamide intake and the risk of breast, endometrial, and ovarian cancers. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2503–2515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burley, V.J.; Greenwood, D.C.; Hepworth, S.J.; Fraser, L.K.; De Kok, T.M.; Van Breda, S.G.; Kyrtopoulos, S.; Botsivali, M.; Kleinjans, J.; A McKinney, P.; et al. Dietary acrylamide intake and risk of breast cancer in the UK women’s cohort. Br. J. Cancer. 2010, 103, 1749. [Google Scholar] [CrossRef]
- Pelucchi, C.; La Vecchia, C.; Bosetti, C.; Boyle, P.; Boffetta, P. Exposure to acrylamide and human cancer—A review and meta-analysis of epidemiologic studies. Ann. Oncol. 2011, 22, 1487–1499. [Google Scholar] [CrossRef]
- Pelucchi, C.; Bosetti, C.; Galeone, C.; La Vecchia, C. Dietary acrylamide and cancer risk: An updated meta-analysis. Int. J. Cancer 2015, 136, 2912–2922. [Google Scholar] [CrossRef]
- Kotemori, A.; Ishihara, J.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S.; JPHC Study Group. Dietary acrylamide intake and risk of breast cancer: The Japan Public Health Center-based Prospective Study. Cancer Sci. 2018, 109, 843–853. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; van den Brandt, P.A.; Godschalk, R.W.; van Schooten, F.J.; Schouten, L.J. Interaction between dietary acrylamide intake and genetic variants for estrogen receptor-positive breast cancer risk. Eur. J. Nutr. 2019, 58, 1033–1045. [Google Scholar] [CrossRef] [Green Version]
- Adani, G.; Filippini, T.; Wise, L.A.; Halldorsson, T.I.; Blaha, L.; Vinceti, M. Dietary intake of acrylamide and risk of breast, endometrial, and ovarian cancers: A systematic review and dose—Response meta-analysis. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1095–1106. [Google Scholar] [CrossRef] [Green Version]
- Benisi-Kohansal, S.; Salari-Moghaddam, A.; Rohani, Z.S.; Esmaillzadeh, A. Dietary acrylamide intake and risk of women’s cancers: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2021, 126, 1355–1363. [Google Scholar] [CrossRef]
- Larsson, S.C.; Håkansson, N.; Åkesson, A.; Wolk, A. Long-term dietary acrylamide intake and risk of endometrial cancer in a prospective cohort of Swedish women. Int. J. Cancer 2009, 124, 1196–1199. [Google Scholar] [CrossRef]
- Obón-Santacana, M.; Kaaks, R.; Slimani, N.; Lujan-Barroso, L.; Freisling, H.; Ferrari, P.; Dossus, L.; Chabbert-Buffet, N.; Baglietto, L.; Fortner, R.; et al. Dietary intake of acrylamide and endometrial cancer risk in the European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Cancer 2014, 111, 987. [Google Scholar] [CrossRef]
- Je, Y. Dietary acrylamide intake and risk of endometrial cancer in prospective cohort studies. Arch. Gynecol. Obstet. 2015, 291, 1395–1401. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Van Den Brandt, P.A.; Godschalk, R.W.; van Schooten, F.J.; Schouten, L.J. The influence of single nucleotide polymorphisms on the association between dietary acrylamide intake and endometrial cancer risk. Sci. Rep. 2016, 6, 34902. [Google Scholar] [CrossRef]
- Obón-Santacana, M.; Freisling, H.; Peeters, P.H.; Lujan-Barroso, L.; Ferrari, P.; Boutron-Ruault, M.-C.; Mesrine, S.; Baglietto, L.; Turzanski-Fortner, R.; Katzke, V.A.; et al. Acrylamide and glycidamide hemoglobin adduct levels and endometrial cancer risk: A nested case-control study in nonsmoking postmenopausal women from the EPIC cohort. Int. J. Cancer 2016, 138, 1129–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelucchi, C.; Galeone, C.; Negri, E.; Bosetti, C.; Serraino, D.; Montella, M.; Talamini, R.; La Vecchia, C. Dietary acrylamide and the risk of endometrial cancer: An Italian case-control. Nutr. Cancer 2016, 68, 187–192. [Google Scholar] [CrossRef]
- Kotemori, A.; Ishihara, J.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S.; JPHC Study Group. Dietary acrylamide intake and the risk of endometrial or ovarian cancers in Japanese women. Cancer Sci. 2018, 109, 3316. [Google Scholar] [CrossRef]
- Huang, H.; Wang, X. Acrylamide intake and endometrial cancer risk: A meta-analysis. Int. J. Clin. Exp. Med. 2019, 12, 11018–11026. [Google Scholar]
- Larsson, S.C.; Åkesson, A.; Wolk, A. Long-term dietary acrylamide intake and risk of epithelial ovarian cancer in a prospective cohort of Swedish women. Cancer Epidemiol. Prevent. Biomark. 2009, 18, 994–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, J.; Terry, K.L.; Poole, E.M.; Wilson, K.M.; Rosner, B.A.; Willett, W.C.; Vesper, H.W.; Tworoger, S.S. Acrylamide hemoglobin adduct levels and ovarian cancer risk: A nested case–control study acrylamide hemoglobin adducts and risk of ovarian cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obón-Santacana, M.; Peeters, P.H.; Freisling, H.; Dossus, L.; Clavel-Chapelon, F.; Baglietto, L.; Schock, H.; Fortner, R.T.; Boeing, H.; Tjønneland, A.; et al. Dietary Intake of Acrylamide and Epithelial Ovarian Cancer Risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) CohortAcrylamide Intake and Epithelial Ovarian Cancer Risk in EPIC. Cancer Epidemiol. Biomark. Prev. 2015, 24, 291–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogervorst, J.G.; van den Brandt, P.A.; Godschalk, R.W.; van Schooten, F.J.; Schouten, L.J. Interactions between dietary acrylamide intake and genes for ovarian cancer risk. Eur. J. Epidemiol. 2017, 32, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Khodavandi, A.; Alizadeh, F.; Razis, A.F.A. Association between dietary intake and risk of ovarian cancer: A systematic review and meta-analysis. Eur. J. Nutr. 2021, 60, 1707–1736. [Google Scholar] [CrossRef]
- Mucci, L.A.; Adami, H.O.; Wolk, A. Prospective study of dietary acrylamide and risk of colorectal cancer among women. Int. J. Cancer 2006, 118, 169–173. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake is not associated with gastrointestinal cancer risk. J. Nutr. 2008, 138, 2229–2236. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Lagergren, J.; Lu, Y. Dietary acrylamide intake and risk of esophageal cancer in a population-based case-control study in Sweden. Int. J. Cancer 2011, 128, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Lujan-Barroso, L.; González, C.A.; Slimani, N.; Obón-Santacana, M.; Ferrari, P.; Freisling, H.; Overvad, K.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Racine, A.; et al. Dietary intake of acrylamide and esophageal cancer risk in the European Prospective Investigation into Cancer and Nutrition cohort. Cancer Causes Cont. 2014, 25, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Sobue, T.; Kitamura, T.; Kitamura, Y.; Ishihara, J.; Kotemori, A.; Zha, L.; Ikeda, S.; Sawada, N.; Iwasaki, M.; et al. Dietary Acrylamide Intake and Risk of Esophageal, Gastric, and Colorectal Cancer: The Japan Public Health Center–Based Prospective Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1461–1468. [Google Scholar] [CrossRef]
- Filippini, T.; Halldorsson, T.I.; Capitão, C.; Martins, R.; Giannakou, K.; Hogervorst, J.; Vinceti, M.; Åkesson, A.; Leander, K.; Katsonouri, A.; et al. Dietary acrylamide exposure and risk of site-specific cancer: A systematic review and dose-response meta-analysis of epidemiological studies. Front. Nutrit. 2022, 9, 875607. [Google Scholar] [CrossRef] [PubMed]
- Hirvonen, T.; Kontto, J.; Jestoi, M.; Valsta, L.; Peltonen, K.; Pietinen, P.; Virtanen, S.M.; Sinkko, H.; Kronberg-Kippila, C.; Virtamo, J. Dietary acrylamide intake and the risk of cancer among Finnish male smokers. Cancer Causes Cont. 2010, 21, 2223–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucci, L.A.; Dickman, P.W.; Steineck, G.; Adami, H.O.; Augustsson, K. Dietary acrylamide and cancer of the large bowel, kidney, and bladder: Absence of an association in a population-based study in Sweden. Br. J. Cancer 2003, 88, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, S.C.; Åkesson, A.; Bergkvist, L.; Wolk, A. Dietary acrylamide intake and risk of colorectal cancer in a prospective cohort of men. Europ. J. Cancer 2009, 45, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Galeone, C.; Talamini, R.; Negri, E.; Polesel, J.; Serraino, D.; La Vecchia, C. Dietary acrylamide and pancreatic cancer risk in an Italian case–control study. Ann. Oncol. 2011, 22, 1910–1915. [Google Scholar] [CrossRef]
- Obón-Santacana, M.; Slimani, N.; Lujan-Barroso, L.; Travier, N.; Hallmans, G.; Freisling, H.; Ferrari, P.; Boutron-Ruault, M.; Racine, A.; Clavel, F.; et al. Dietary intake of acrylamide and pancreatic cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Ann. Oncol. 2013, 24, 2645–2651. [Google Scholar] [CrossRef]
- Pelucchi, C.; Rosato, V.; Bracci, P.M.; Li, D.; Neale, R.E.; Lucenteforte, E.; Serraino, D.; Anderson, K.; Fontham, E.; Holly, E.; et al. Dietary acrylamide and the risk of pancreatic cancer in the International Pancreatic Cancer Case–Control Consortium (PanC4). Ann. Oncol. 2017, 28, 408–414. [Google Scholar] [CrossRef]
- Kito, K.; Ishihara, J.; Kotemori, A.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Dietary acrylamide intake and the risk of pancreatic cancer: The Japan public health center-based prospective study. Nutrients 2020, 12, 3584. [Google Scholar] [CrossRef]
- Zha, L.; Sobue, T.; Kitamura, T.; Kitamura, Y.; Ishihara, J.; Kotemori, A.; Liu, R.; Ikeda, S.; Sawada, N.; Iwasaki, M.; et al. Dietary acrylamide intake and the risk of liver cancer: The Japan public health center-based prospective study. Nutrients 2020, 12, 2503. [Google Scholar] [CrossRef]
- Liu, Z.M.; Tse, L.A.; Ho, S.C.; Wu, S.; Chen, B.; Chan, D.; Wong, S.Y.S. Dietary acrylamide exposure was associated with increased cancer mortality in Chinese elderly men and women: A 11-year prospective study of Mr. and Ms. OS Hong Kong. J. Cancer Res. Clin. Oncol. 2017, 143, 2317–2326. [Google Scholar] [CrossRef]
- Larsson, S.C.; Åkesson, A.; Wolk, A. Dietary acrylamide intake and prostate cancer risk in a prospective cohort of Swedish men. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1939–1941. [Google Scholar] [CrossRef] [Green Version]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake and the risk of renal cell, bladder, and prostate cancer. Am. J. Clin. Nutr. 2008, 87, 1428–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, K.M.; Bälter, K.; Adami, H.O.; Grönberg, H.; Vikström, A.C.; Paulsson, B.; Törnqvist, M.; Mucci, L.A. Acrylamide exposure measured by food frequency questionnaire and hemoglobin adduct levels and prostate cancer risk in the Cancer of the Prostate in Sweden Study. Int. J. Cancer 2009, 124, 2384–2390. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.M.; Giovannucci, E.; Stampfer, M.J.; Mucci, L.A. Dietary acrylamide and risk of prostate cancer. Int. J. Cancer 2012, 131, 479–487. [Google Scholar] [CrossRef]
- Perloy, A.; Schouten, L.J.; van den Brandt, P.A.; Godschalk, R.; van Schooten, F.J.; Hogervorst, J.G. The role of genetic variants in the association between dietary acrylamide and advanced prostate cancer in the Netherlands cohort study on diet and cancer. Nutr. Cancer. 2018, 70, 620–631. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, S.; Sobue, T.; Kitamura, T.; Ishihara, J.; Kotemori, A.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Tsugane, S.; et al. Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study. Nutrients 2021, 13, 780. [Google Scholar] [CrossRef]
- Mucci, L.A.; Lindblad, P.; Steineck, G.; Adami, H.O. Dietary acrylamide and risk of renal cell cancer. Int. J. Cancer 2004, 109, 774–776. [Google Scholar] [CrossRef]
- Pelucchi, C.; Galeone, C.; Maso, L.D.; Talamini, R.; Montella, M.; Ramazzotti, V.; Negri, E.; Franceschi, S.; Vecchia, C.L. Dietary acrylamide and renal cell cancer. Int. J. Cancer 2007, 120, 1376–1377. [Google Scholar] [CrossRef]
- Graff, R.E.; Cho, E.; Preston, M.A.; Sanchez, A.; Mucci, L.A.; Wilson, K.M. Dietary acrylamide intake and risk of renal cell carcinoma in two large prospective cohorts. Cancer Epidemiol. Biomark. Prev. 2018, 27, 979–982. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.L.; Hodge, R.A.; Um, C.Y.; Gapstur, S.M. Dietary acrylamide is not associated with renal cell cancer risk in the CPS-II nutrition cohort. Cancer Epidemiol. Biomark. Prev. 2019, 28, 616–619. [Google Scholar] [CrossRef]
- Jiang, F.; Teng, M.; Zhu, Y.X.; Li, Y.J. No association between dietary acrylamide and renal cell carcinoma: An updated meta-analysis. J. Sci. Food Agric. 2020, 100, 3071–3077. [Google Scholar] [CrossRef] [PubMed]
- Schouten, L.J.; Hogervorst, J.G.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake and the risk of head-neck and thyroid cancers: Results from the Netherlands Cohort Study. Am. J. Epidemiol. 2009, 170, 873–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Lung cancer risk in relation to dietary acrylamide intake. J. Natl. Cancer Inst. 2009, 101, 651–662. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Zha, L.; Sobue, T.; Kitamura, T.; Ishihara, J.; Kotemori, A.; Ikeda, S.; Sawada, N.; Iwasaki, M.; Tsugane, S. Dietary acrylamide intake and risk of lung cancer: The Japan public health center based prospective study. Nutrients 2020, 12, 2417. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake and brain cancer risk. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1663–1666. [Google Scholar] [CrossRef] [Green Version]
- Bongers, M.L.; Hogervorst, J.G.; Schouten, L.J.; Goldbohm, R.A.; Schouten, H.C.; van den Brandt, P.A. Dietary acrylamide intake and the risk of lymphatic malignancies: The Netherlands Cohort Study on diet and cancer. PLoS ONE 2012, 7, e38016. [Google Scholar] [CrossRef] [Green Version]
- Zha, L.; Liu, R.; Sobue, T.; Kitamura, T.; Ishihara, J.; Kotemori, A.; Ikeda, S.; Sawada, N.; Iwasaki, M.; Tsugane, S.; et al. Dietary acrylamide ıntake and the risk of hematological malignancies: The Japan Public Health Center-based prospective study. Nutrients 2021, 13, 590. [Google Scholar] [CrossRef]
- Lipunova, N.; Schouten, L.J.; van den Brandt, P.A.; Hogervorst, J.G. A prospective cohort study on dietary acrylamide intake and the risk for cutaneous malignant melanoma. Eur. J. Cancer Prev. 2017, 26, 528–531. [Google Scholar] [CrossRef]
- The Japan Public Health Center (JPHC). Japan Public Health Center-Based Prospective Study. 2010. Available online: https://epi.ncc.go.jp/en/jphc/index.html (accessed on 6 September 2021).
- Riboldi, B.P.; Vinhas, Á.M.; Moreira, J.D. Risks of dietary acrylamide exposure: A systematic review. Food Chem. 2014, 157, 310–322. [Google Scholar] [CrossRef]
- Virk-Baker, M.K.; Nagy, T.R.; Barnes, S.; Groopman, J. Dietary acrylamide and human cancer: A systematic review of literature. Nutr. Cancer 2014, 66, 774–790. [Google Scholar] [CrossRef]


{kind=link}
| Type of Cancer—Reference | Cases | Mean Dietary Acrylamide Intake | Risk |
|---|---|---|---|
| Breast Cancer | |||
| Mucci et al. (2005) [62] | 667 | 25.9 µg/day (0.37 µg/kg bw/day) | na |
| Pelucchi et al. (2006) [63] | 2900 | 24.32 µg/day (0.38 µg/kg bw/day) | na |
| Hogervorst et al. (2007) [64] | 1350 | 21.0 ± 11.9 µg/day (0.32 ± 0.19 µg/kg bw/day | na |
| Olesen et al. (2008) [65] | 374 | Hb-AA: 47 (pmol/g globin) Hb-GA: 26 (pmol/g globin) | No relationship was found between Hb-AA (p: 0.83) and Hb-GA (p: 0.65) levels and breast cancer. However, a positive correlation was found between ER+ positive breast cancer and Hb-AA in non-smokers. |
| Larsson et al. (2009) [66] | 2952 | 24.6 ± 7.6 µg/day (0.38 ± 0.17 µg/kg bw/day | na |
| Wilson et al. (2009) [67] | 1179 | 20.2 µg/day (0.32 µg/kg bw/day | na |
| Pedersen et al. (2010) [68] | 1690 | 18.3 µg/day (0.27 µg/kg bw/day) | No relationship was found between breast cancer and dietary acrylamide exposure. However, in ER+, PR+ and ER+/PR+ breast cancer cases, a partial increase was detected with acrylamide exposure, which was not statistically significant. |
| Wilson et al. (2010) [69] | 6301 | 9–26 µg/day (0.13–0.42 µg/kg bw/day) | na |
| Burley et al. (2010) [70] | 1084 | 15 µg/day (0.23 µg/kg bw/day) | No relationship was found between breast cancer and dietary acrylamide exposure. However, a positive relationship was found between premenopausal breast cancer and acrylamide exposure. |
| Pelucchi et al. (2011) [71] | 9048 | - | na |
| Pelucchi et al. (2015) [72] | 16,773 | - | na |
| Kotemori et al. (2018) [73] | 792 | 7.0 ± 3.7 µg/day (0.14 ± 0.13 µg/kg bw/day) | na |
| Hogervorst et al. (2019) [74] | 844 | 20.6 ± 11.3 µg/day | No positive correlation was found between ER+ breast cancer and dietary acrylamide exposure. On the contrary, an inverse relationship was found between acrylamide and ER+ breast cancer. However, a significant association was found between several SNPs genes (rs1056827 in CYP1B1, rs2959008 and rs7173655 in CYP11A1, the GSTT1gene deletion and rs1052133 in hOGG1) and acrylamide exposure. It was stated that acrylamide may cause breast cancer with its effect on sex hormones. |
| Adani et al. (2020) [75] | - | - | No association was found between exposure and risk for breast cancer, particularly in never-smokers and postmenopausal women, or an inverse relationship was found. In a limited subgroup analysis of premenopausal women, acrylamide intake starting at 20 μg/day was associated with a linear increase in breast cancer risk. |
| Atabati et al. (2020) [42] | - | - | High intakes of acrylamide could marginal significantly reduce the risk of breast cancer. |
| Benisi-Kohansal et al. (2021) [76] | - | - | na |
| Uterine Cancer | |||
| Hogervorst et al. (2007) [64] | 327 | 21.0 ± 11.9 µg/day (0.32 ± 0.19 µg/kg bw/day) | No relationship was found between uterine cancer and dietary acrylamide exposure. However, increased acrylamide exposure in non-smokers women increased the risk of uterine cancer. |
| Larsson et al. (2009) [77] | 687 | 24.6 ± 7.6 µg/day (0.38 ± 0.17 µg/kg bw/day) | na |
| Wilson et al. (2010) [69] | 484 | 9–26 µg/day (0.13–0.42 µg/kg bw/day) | The risk of uterine cancer increased with increasing dietary acrylamide exposure. |
| Pelucchi et al. (2011) [71] | 908 | - | na |
| Obón-Santacana et al. (2014) [78] | 1.382 | 23.7 ± 13.0 µg/day (0.4 ± 0.2 µg/kg bw/day) | No association was found between dietary acrylamide exposure and uterine cancer. However, increased exposure to acrylamide was associated with an increased risk of EC type I in both smokers and non-smokers. |
| Je (2015) [79] | 2.099 | - | No relationship was found between uterine cancer and dietary acrylamide exposure. However, among non-smokers, the risk of uterine cancer increased with high acrylamide exposure. |
| Pelucchi et al. (2015) [72] | 2774 | - | na |
| Hogervorst et al. (2016) [80] | 393 | 21.3 ± 12.7 µg/day | No positive correlation was found between uterine cancer and dietary acrylamide exposure. However, a statistically significant relationship was found between exposure to acrylamide with a few nominal SNPs genes (CYP2E1: rs915906; rs2480258) and the deletions (GSTM1-GSTT1). This was explained as acrylamide exposure may contribute to the risk of developing uterine cancer. |
| Obón-Santacana et al. (2016) [81] | 383 | Hb-AA: 39.9 (pmol/g Hb) Hb-GA: 34.1 (pmol/g Hb) | na |
| Pelucchi et al. (2016) [82] | 454 | 33.7 μg/day | na |
| Kotemori et al. (2018) [83] | 161 | 7.1 ± 3.7 μg/day (0.14 ± 0.13 µg/kg bw/day) | na |
| Huang and Wang (2019) [84] | 3228 | The current meta-analysis did not support a significant association between acrylamide intake and endometrial cancer risk. However, women with high acrylamide exposure who never smoked had a higher risk of endometrial cancer. | |
| Adani et al. (2020) [75] | - | - | While intermediate acrylamide exposure caused the highest risk of endometrial cancer, the relationship between exposure and cancer was linear and positive in never-smokers. High acrylamide exposure was associated with a linearly increased risk of endometrial cancer, particularly in never-smokers. |
| Benisi-Kohansal et al. (2021) [76] | - | - | na |
| Ovarian Cancer | |||
| Pelucchi et al. (2006) [63] | 1031 | 23.33 µg/day (0.37 µg/kg bw/day) | na |
| Hogervorst et al. (2007) [64] | 300 | 21.0 ± 11.9 µg/day (0.32 ± 0.19 µg/kg bw/day) | A statistically significant association was found between dietary acrylamide exposure and ovarian cancer (especially in non-smokers). |
| Larsson et al. (2009) [85] | 368 | 24.6 ± 7.6 µg/day (0.38 ± 0.17 µg/kg bw/day) | na |
| Wilson et al. (2010) [69] | 416 | 9–26 µg/day (0.13–0.42 µg/kg bw/day) | No statistical relationship was found between dietary acrylamide exposure and ovarian cancer. However, it was stated that the risk of possible ovarian cancer may increase due to the risk of multiple tumors. |
| Pelucchi et al. (2011) [71] | 908 | - | na |
| Xie et al. (2013) [86] | 263 | Hb-AA: 112.6 pmol/g | na |
| Pelucchi et al. (2015) [72] | 2010 | - | na |
| Obón-Santacana et al. (2015) [87] | 1191 | 21.3 µg/day (0.3 µg/kg bw/day) | na |
| Hogervorst et al. (2017) [88] | 252 | 21.9 ± 13.1 µg/day | No statistically significant relationship was found between genetic variants and acrylamide exposure. However, a significant correlation was found between the nominal SNPs gene (HSD3B1/B2: rs4659175; rs10923823) and its proxies rs7546652, rs1047303 and rs6428830 and acrylamide exposure. It was stated that acrylamide may cause ovarian cancer due to its effect on sex hormones. |
| Kotemori et al. (2018) [83] | 122 | 7.0 ± 3.7 μg/day (0.14 ± 0.13 µg/kg bw/day) | na |
| Adani et al. (2020) [75] | - | - | The risk of ovarian cancer slightly increased in individuals with dietary acrylamide exposure, particularly in never-smokers. High acrylamide intake caused a linear increase in the risk of ovarian and endometrial cancer, especially in never-smokers. |
| Benisi-Kohansal et al. (2021) [76] | - | - | na |
| Khodavandi, Alizadeh, and Razis (2021) [89] | - | - | na |
| Type of Cancer—Reference | Cases | Mean Dietary Acrylamide Intake | Risk |
|---|---|---|---|
| Esophageal Cancer | |||
| Pelucchi et al. (2006) [63] | 395 | 27.47 µg/day (0.36 µg/kg bw/day) | na |
| Hogervorst et al. (2008) [91] | 216 | 21.8 ± 12.1 µg/day (0.30 ± 0.18 µg/kg bw/day) | na |
| Lin, Lagergren, and Lu (2011) [92] | EC: 618 E-AC: 189 GEJ-AC:222 E-SCC: 167 | E-AC: 37.6 ± 14.6 µg/day GEJ-AC: 37.5 ± 14.1 µg/day E-SCC: 38.5 ± 14.6 µg/day | All combined esophageal tumors increased with increasing acrylamide exposure. A statistically significant relationship was found especially in overweight and obese patients. A statistically significant relationship was found between E-SCC and dietary acrylamide exposure. This is much stronger in non-smokers with E-SCC. |
| Pelucchi et al. (2011) [71] | 611 | - | na |
| Luján-Barroso et al. (2014) [93] | EC: 341 E-AC: 142 E-SCC:176 Other: 23 | 26.22 ± 14.79 µg/day | Dietary acrylamide exposure increased the risk of E-AC cancer and tumors. However, since this increase was not linear, a statistically significant relationship could not be determined. |
| Pelucchi et al. (2015) [72] | 1546 | - | na |
| Liu et al. (2019) [94] | 391 | 6.80 µg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Gastric Cancer | |||
| Hogervorst et al. (2008) [91] | 563 | 21.8 ± 12.1 µg/day (0.30 ± 0.18 µg/kg bw/day) | na |
| Hirvonen et al. (2010) [96] | 224 | 36.8 μg/day | na |
| Pelucchi et al. (2016) [82] | 787 | - | na |
| Liu et al. (2019) [94] | 2218 | 6.8 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Colorectal Cancer | |||
| Mucci et al. (2003) [97] | Total:591 E: 346 K: 245 | 28.6 µg/day | An inverse relationship was found between dietary acrylamide exposure and colon cancer. |
| Mucci, Adami, and Wolk (2006) [90] | Total: 741 Kolon: 504 Rektum: 237 | 24.6 µg/day (0.38 µg/kg bw/day) | na |
| Pelucchi et al. (2006) [63] | Total: 2280 Kolon:1394 Rektum:886 | 27.69 µg/day (0.40 µg/kg bw/day) | na |
| Hogervorst et al. (2008) [91] | 2190 | 21.8 ± 12.1 µg/day (0.30 ± 0.18 µg/kg bw/day) | na |
| Larsson et al. (2009) [98] | Kolon: 410 Rektum: 266 | 36.1 ± 9.6 μg/day | na |
| Hirvonen et al. (2010) [96] | 316 | 21.9–55.7 μg/day | na |
| Pelucchi et al. (2011) [71] | Kolorektum: 5887 Kolon: 3813 Rektum: 1899 | - | na |
| Hogervorst et al. (2007) [64] | M: 341 W: 282 | E: 23 μg/day (0.29 µg/kg bw/day) K: 20 μg/day (0.29 µg/kg bw/day) | No statistically significant relationship was found between dietary acrylamide exposure and total colorectal cancer. There was also an inverse relationship between acrylamide exposure and tumors with the APC mutation among women. |
| Pelucchi et al. (2015) [72] | 6794 | - | na |
| Liu et al. (2019) [94] | 2470 | 6.8 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Pancreatic Cancer | |||
| Hogervorst et al. (2008) [91] | 349 | 21.8 ± 12.1 µg/day (0.30 ± 0.18 µg/kg bw/day) | na |
| Hirvonen et al. (2010) [96] | 192 | 21.9–55.7 μg/day | na |
| Pelucchi et al. (2011) [99] | 326 | 33.51 ± 17.42 µg/day | na |
| Obón-Santacana et al. (2013) [100] | 865 | 26.22 µg/day 0.38 µg/kg bw/day | na |
| Pelucchi et al. (2015) [72] | 1732 | - | na |
| Pelucchi et al. (2017) [101] | 1975 | - | na |
| Kito et al. (2020) [102] | 576 | 6.90 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Liver Cancer | |||
| Zha et al. (2020) [103] | 744 | 6.90 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Digestive System Cancers | |||
| Liu et al. (2017) [104] | 131 | 14.6 ± 8.2 μg/day | The relationship between dietary acrylamide exposure and digestive system cancers was found to be statistically significant. |
| Type of Cancer—Reference | Cases | Mean Dietary Acrylamide Intake | Risk |
|---|---|---|---|
| Prostate Cancer | |||
| Pelucchi et al. (2006) [63] | 1294 | 25.59 µg/day (0.33 µg/kg bw/day) | na |
| Hogervorst et al. (2008) [106] | 2246 | 22.4 µg/day (0.29 µg/kg bw/day) | na |
| Wilson et al. (2009) [107] | 1489 | 43.8 ± 13.7 µg/day (0.54 ± 0.18 µg/kg bw/day) Hb-AA: 54.7 pmol/g globin | na |
| Larsson et al. (2009) [105] | 2696 | 36.1 ± 9.6 μg/day | na |
| Hirvonen et al. (2010) [96] | 799 | 21.9–55.7 μg/day | na |
| Pelucchi et al. (2011) [71] | 7735 | - | na |
| Wilson et al. (2012) [108] | 5025 | 10.5–40.1 μg/day | na |
| Pelucchi et al. (2015) [72] | 13,559 | - | na |
| Perloy et al. (2018) [109] | 948 | 22.9 μg/day | na |
| Ikeda et al. (2021) [110] | 1195 | 6.40 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Bladder Cancer | |||
| Mucci et al. (2003) [97] | 233 | 29.4 ± 0.9 μg/day | na |
| Hogervorst et al. (2008) [106] | 1210 | 9.5–40.8 μg/day | na |
| Hirvonen et al. (2010) [96] | 365 | 21.9–55.7 μg/day | na |
| Pelucchi et al. (2011) [71] | 1473 | - | na |
| Pelucchi et al. (2015) [72] | 1838 | - | na |
| Ikeda et al. (2021) [110] | 392 | 6.40 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Renal Cancer | |||
| Mucci et al. (2003) [97] | 133 | 28.4 ± 1.2 μg/day | na |
| Mucci et al. (2004) [111] | 379 | 27.6 ± 0.7 μg/day | na |
| Pelucchi et al. (2007) [112] | 767 | 37 μg/day (0.475 µg/kg bw/day) | na |
| Hogervorst et al. (2008) [106] | 339 | 9.5–40.8 μg/day | A positive correlation was found between dietary acrylamide exposure and renal cancer. |
| Hirvonen et al. (2010) [96] | 184 | 21.9–55.7 μg/day | na |
| Pelucchi et al. (2011) [71] | 1618 | - | na |
| Pelucchi et al. (2015) [72] | 1802 | - | na |
| Graff et al. (2018) [113] | 629 | Female: 15.8 μg/day Male: 21.7 μg/day | na |
| McCullough et al. (2019) [114] | 412 | 22.6 μg/day | na |
| Jiang et al. (2020) [115] | 2843 | - | na |
| Ikeda et al. (2021) [110] | 208 | 6.40 μg/day (0.12 µg/kg bw/day) | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Type of Cancer—Reference | Cases | Mean Dietary Acrylamide Intake | Risk |
|---|---|---|---|
| Oral cavity/pharyngeal cancer | |||
| Pelucchi et al. (2006) [63] | 749 | 29.24 μg/day (0.40 µg/kg bw/day) | na |
| Schouten et al. (2009) | OCC: 101 (M: 61-W:40) OHC: 83 (M: 41-W:22) | OCC-M: 18.8 μg/day (0.25 µg/kg bw/day) OCC-W: 18.8 μg/day (0.28 µg/kg bw/day) OHC-M: 18.3 μg/day (0.23 µg/kg bw/day) OHC-W: 20.7 μg/day (0.32 µg/kg bw/day) | No statistically significant relationship was found between dietary acrylamide exposure and OCC cancer. However, it was stated that acrylamide exposure may increase the risk of OCC cancer in non-smokers. OHC: na |
| Pelucchi et al. (2015) [72] | 933 | - | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Throat Cancer | |||
| Pelucchi et al. (2006) [63] | 527 | 27.10 μg/day (0.36 µg/kg bw/day) | na |
| Schouten et al. (2009) [116] | LC: 180 (M: 170-W:10) | LC-M: 23.3 μg/day (0.31 µg/kg bw/day) LC-W: 21.0 μg/day (0.35 µg/kg bw/day) | na |
| Pelucchi et al. (2015) [72] | 707 | - | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Lung Cancer | |||
| Hogervorst et al. (2009) [117] | M: 1.600 W: 295 | - | M: na W: A very strong inverse relationship was found between dietary acrylamide exposure and adenocarcinoma. |
| Hirvonen et al. (2010) [96] | 1.703 | 21.9–55.7 μg/day | A positive correlation was found between dietary acrylamide exposure and lung cancer. |
| Pelucchi et al. (2015) [72] | 3.598 | - | na |
| Liu et al. (2020) [118] | M: 1187 W: 485 | Female: 6.8 μg/day Male: 7.0 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Respiratory System Cancers | |||
| Liu et al. (2017) [104] | 104 | 14.6 ± 8.2 μg/day | The increase in the number of respiratory system cancer cases with dietary acrylamide exposure was found to be statistically significant. |
| Type of Cancer—Reference | Cases | Mean Dietary Acrylamide Intake | Risk |
|---|---|---|---|
| Brain Cancer | |||
| Hogervorst et al. (2009) [119] | 216 | 22.1 μg/day (0.30 µg/kg bw/day) | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Thyroid Cancer | |||
| Schouten et al. (2009) [116] | M: 19 W: 47 | M: 22.1 μg/day (0.28 µg/kg bw/day) W: 21.6 μg/day (0.33 µg/kg bw/day) | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| Lymphatic Malignancies | |||
| Hirvonen et al. (2010) [96] | L: 175 | 21.9–55.7 μg/day | na |
| Bongers et al. (2012) [120] | Total LM: 1233 CLL:200 DLCL:259 MM:323 FL:89 WMI:89 MCL-M:56 T-cell-M:54 | CLL: 20.0–21.0 μg/day DLCL: 21.0–23.0 μg/day MM: 21.0–25.0 μg/day FL: 23.0–26.0 μg/day WMI: 23.0–26.0 μg/day MCL-M: 20.0–22.0 μg/day T-cell-M: 22.0–27.0 μg/day | A statistically significant relationship was only found between dietary acrylamide exposure and MM-M. |
| Pelucchi et al. (2015) [72] | 1208 | - | na |
| Zha et al. (2021) [121] | ML: 326 MM: 126 L: 224 | 6.90 μg/day | na |
| Filippini et al. (2022) [95] | - | 23 μg/day | na |
| All Types of Cancer | |||
| Liu et al. (2017) [104] | 131 | 14.6 ± 8.2 μg/day | The relationship between dietary acrylamide exposure and all cancer types was found to be statistically significant. |
| Skin Cancer | |||
| Lipunova et al. (2017) [122] | CMM-M:241 SSM-M:90 NM-M:40 CMM-W:236 SSM-W:102 NM-W:30 | 23.9 μg/day 24.1 μg/day 27.5 μg/day 21.2 μg/day 20.5 μg/day 21.5 μg/day | Modeling with an increase of 10 μg/day acrylamide increased the risk of CMM-M among men. But this increase was not linear. A weaker correlation was found among non-smokers in terms of CMM-M. The increased risk of NM-M among men was statistically significant. Among non-smokers, this relationship was much stronger. No significant relationship was found between SSM-M and acrylamide exposure among men. According to the same modeling, no statistically significant data could be obtained between acrylamide exposure and melanoma risk in women. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Başaran, B.; Çuvalcı, B.; Kaban, G. Dietary Acrylamide Exposure and Cancer Risk: A Systematic Approach to Human Epidemiological Studies. Foods 2023, 12, 346. https://doi.org/10.3390/foods12020346
Başaran B, Çuvalcı B, Kaban G. Dietary Acrylamide Exposure and Cancer Risk: A Systematic Approach to Human Epidemiological Studies. Foods. 2023; 12(2):346. https://doi.org/10.3390/foods12020346
Chicago/Turabian StyleBaşaran, Burhan, Burcu Çuvalcı, and Güzin Kaban. 2023. "Dietary Acrylamide Exposure and Cancer Risk: A Systematic Approach to Human Epidemiological Studies" Foods 12, no. 2: 346. https://doi.org/10.3390/foods12020346
APA StyleBaşaran, B., Çuvalcı, B., & Kaban, G. (2023). Dietary Acrylamide Exposure and Cancer Risk: A Systematic Approach to Human Epidemiological Studies. Foods, 12(2), 346. https://doi.org/10.3390/foods12020346