Ultra-Low-Level Laser Therapy and Acupuncture Libralux: What Is so Special?


Abstract
:1. Introduction
2. Libralux Main Characteristics
- (a)
- A meridian resonance frequency (12 different values in the band 5–11 Hz);
- (b)
- An anti-addiction 1 Hz frequency.
- Laser wavelength (nm) 650 (red light)
- Peak emitted power (mW) 7
- Beam divergence (mrad) 35
- Spot size @ 20 mm (cm2) 0.2
- Spot size @200 mm (cm2) 20
- Modulated Emission:
- ◦
- Carrier Frequency 100 Hz Duty Cycle 1%
- ◦
- Meridian Modulation 5–11 Hz Duty Cycle 50%
- ◦
- Antiaddiction Modulation 1 Hz Duty Cycle 50%
- Mean Stimulation Power 0.0175 mW
- Mean Stimulation Energy (20 s) 0.35 mJ
3. The Evidence
4. The Libralux Application
5. The Physiological Mechanism
5.1. Musculoskeletal Pain
5.2. MP and Dysfunction
5.3. Libralux Effect
6. The Libralux and Its Effects
- (a)
- (b)
- The average density of ECM proteins [33] has a mean order of magnitude of 1013 chains per square centimetre; Libralux affords the same photon density (under the skin, an average power density of 20 nW over a 10 mm2 surface = 200 nW/cm2);
- (c)
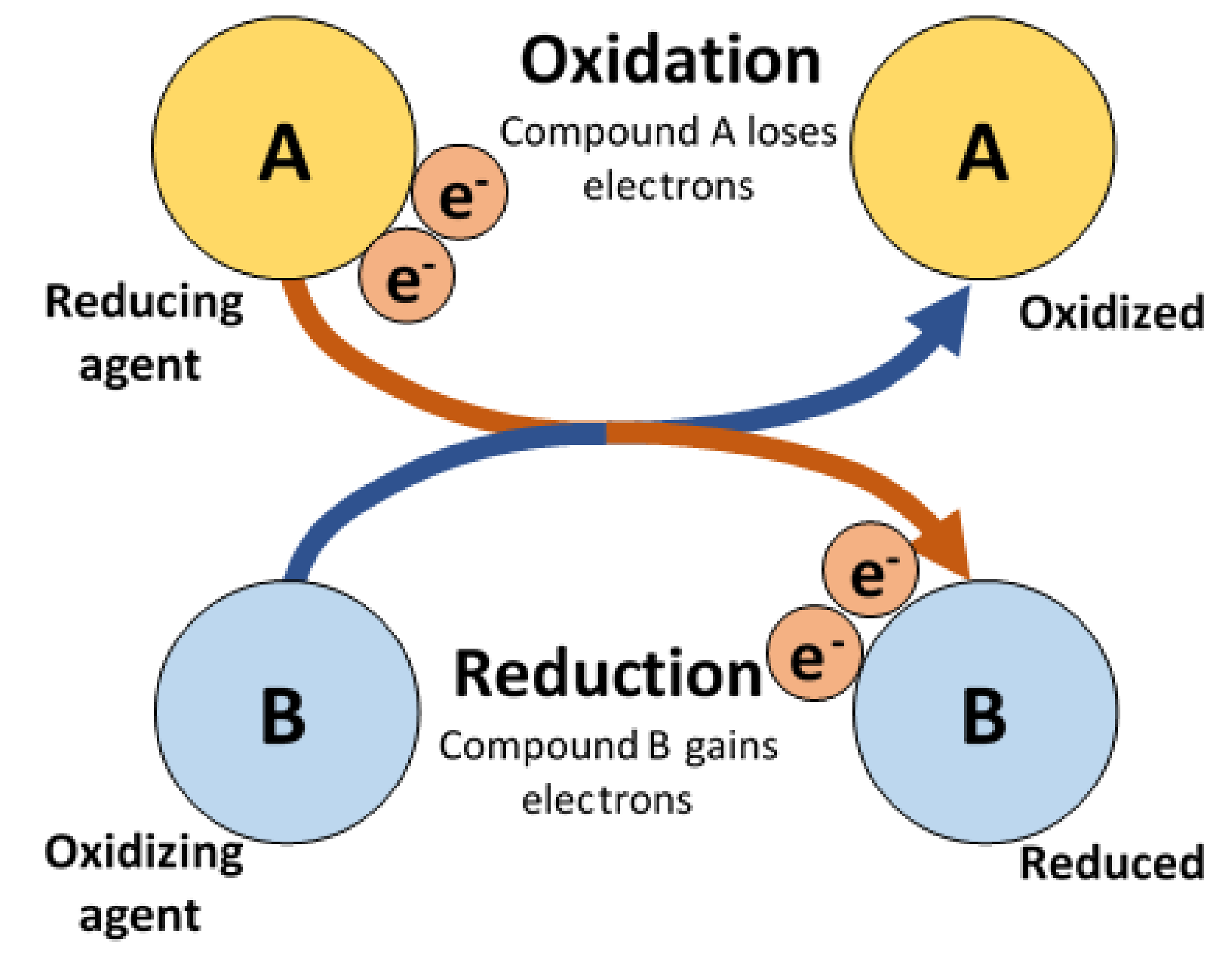
- At a body temperature of 37 °C, the oxidation emitted photons have a wavelength of 650 nm, identical to the Libralux emission;
- (d)
- While the oxidation process frees two photons, the following redox process requires just one photon; thus, the overflow of photons through the ECM can spread across the body along the ubiquitous ECM, which unlike surrounding tissues is transparent to visible light;
- (e)
- To start the process, one must stimulate the synchronization of photon flow from a distance as far away as possible from the affected area [34]; that is why the left leg is treated to obtain an effect on the right shoulder;
- (f)
- To access the ECM, Libralux exploits the acupuncture stimulation points (Aps) [35]—a funnel through the dermis and fascia filled with free nerve terminations (which is why APs are so sensitive to pressure) and a significantly higher percentage of small blood vessels [36]. The points have different properties in comparison to the surrounding tissues, including significantly lower electrical impedance [37] and a superior absorbance of visible light [38];
- (g)
- The acupuncture meridians are very likely to rely on ECM channels, in which the photonic flow can travel in a way that is very similar to the one experienced in classic acupuncture [39]. That is why we decided to select specific application protocols involving specific meridians. Links between acupuncture [40], its meridians [37], the extracellular soft tissue matrix and fascia, along with the mechanoreceptors [41], hydraulic transduction [42] and signalling pathways, appear to be quite tight, although robust evidence remains lacking.
7. Libralux and Acupuncture
8. Conclusions
9. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.Y.; Carroll, J.D.; Hamblin, M.R. The nuts and bolts of low-level laser (light) therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef]
- Tunér, J.; Hode, L. Laser Therapy. Clinical Practice and Scientific Background; Prima Books AB: Grängesberg, Sweden, 2002. [Google Scholar]
- Recommended treatment doses for Low Level Laser Therapy. Available online: https://waltza.co.za/documentation-links/recommendations/ (accessed on 14 February 2019).
- Baratto, L.; Calzà, L.; Capra, R.; Gallamini, M.; Giardino, L.; Giuliani, A.; Lorenzini, L.; Traverso, S. Ultra-low-level laser therapy. Lasers Med. Sci. 2011, 26, 103–112. [Google Scholar] [CrossRef]
- Kawakita, K.; Okada, K. Acupuncture therapy: Mechanism of action, efficacy, and safety: A potential intervention for psychogenic disorders? Biopsychosoc. Med. 2014, 8, 4. [Google Scholar] [CrossRef]
- Cohen, M.; Behrenbruch, C.; Cosic, I. Is there a link between acupuncture meridians, earth-ionosphere resonances and cerebral activity? In Proceedings of the 2nd International Conference on Bioelectromagnetism, Melbourne, Australia, 15–18 February 1998. [Google Scholar]
- Gallamini, M.; D’Angelo, G.; Belloni, G. Biolite: A Patented Ultra-Low-Level Laser-Therapy Device for Treating Musculoskeletal Pain and Associated Impairments. J. Acupunct. Meridian Stud. 2015, 8, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Baratto, L.; Capra, R.; Farinelli, M.; Monteforte, P.; Morasso, P.; Rovetta, G. Sonographic examination in patient with osteorathritis of the cervical spine reveals soft-tissues changes due to application with very low-power modulated laser. Int. J. Clin. Pharmacol. Res. 2000, 20, 13–16. [Google Scholar]
- Monteforte, P.; Baratto, L.; Molfetta, L.; Rovetta, G. Low-power Laser in osteoarthritis of the cervical spine. Int. J. Tissue React. 2003, 25, 131–136. [Google Scholar] [PubMed]
- Giuliani, A.; Fernadez, M.; Farinelli, M.; Baratto, L.; Capra, R.; Rovetta, G.; Monteforte, P.; Giardino, L.; Calzà, L. Very low level laser therapy attenuates edema and pain in experimental models. Int. J. Tissue React. 2004, 26, 29–37. [Google Scholar] [PubMed]
- Lorenzini, L.; Giuliani, A.; Giardino, L.; Calzà, L. Laser acupuncture for acute inflammatory, visceral and neuropathic pain relief: An experimental study in the laboratory rat. Res. Vet. Sci. 2009, 88, 159–165. [Google Scholar] [CrossRef]
- Giuliani, A.; Lorenzini, L.; Gallamini, M.; Massella, A.; Giardino, L.; Calzà, L. Low infra-red laser light irradiation on cultured neural cells: Effects on mitochondria and cell viability after oxidative stress. BMC Complement. Altern. Med. 2009, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Petruzzelli, S.; Congiu, A.; Gallamini, M.; Pompei, R. Ultra-low power laser stimulation impairs the adhesion of Staphylococcus aureus to primary human cells, and interferes with the expression of staphylococcal pathogenic factors. New Microbiol. 2014, 37, 193–199. [Google Scholar]
- Giuliani, A.; Lorenzini, L.; Alessandri, M.; Torricella, R.; Baldassarro, V.A.; Giardino Calzà, L. In vitro exposure to very low-level laser modifies expression level of extracellular matrix protein RNAs and mitochondria dynamics in mouse embryonic fibroblasts. BMC Complement. Altern. Med. 2015, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Xing, D. Molecular mechanisms of cell proliferation induced by low power laser irradiation. J. Biomed. Sci. 2009, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Baratto, L.; Simonini, M.; Morasso, P.; Re, C.; Spada, G. Nociception and control of stance: Measurement with force platform during Romberg test. Gait & Posture 2002, 16, S214–S215. [Google Scholar]
- Gallamini, M. Treating balance disorders by ultra-low-level laser stimulation of acupoints. J. Acupunct Meridian Stud. 2013, 6, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Scoppa, F.; Gallamini, M.; Belloni, G. Treating Balance Disorders with Ulllt Acupuncture Stimulation: A Further Pilot Study on Normal Subjects Confirms Clinical Applicability of Treatment. J. Nov. Physiother. 2015, 6, 285. [Google Scholar] [CrossRef]
- Staud, R. Peripheral pain mechanisms in chronic widespread pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Simons, D.G.; Mense, S. Understanding and measurement of muscle tone as related to clinical muscle pain. In Fascia Research: Basic Science and Implications for Conventional and Complementary Health Care; Findley, T., Schleip, R., Eds.; Elsevier Urban and Fischer: Munich, Germany, 2007; pp. 144–161. [Google Scholar]
- Pollack, G.H. Cells, Gels and the Engines of Life; Ebner and Sons Publishers: Seattle, WA, USA, 10 March 2001. [Google Scholar]
- Pollack, G.H. The role of aqueous interfaces in the cell. Adv. Colloids Interface Sci. 2003, 103, 173–196. [Google Scholar] [CrossRef]
- Findley, T. Fascia Research II: Second International Fascia Research Congress. Int. J. Ther. Massage Bodyw. 2009, 2, 4–9. [Google Scholar]
- Zügel, M.; Maganaris, C.N.; Wilke, J.; Jurkat-Rott, K.; Klingler, W.; Wearing, S.C.; Findley, T.; Barbe, M.F.; Steinacker, J.M.; Vleeming, A.; et al. Fascial tissue research in sports medicine: From molecules to tissue adaptation, injury and diagnostics: Consensus statement. Br. J. Sports Med. 2018, 52, 1497. [Google Scholar] [CrossRef]
- Hodges, P.W.; Tucker, K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain 2011, 152 (Suppl. 3), S90–S98. [Google Scholar] [CrossRef] [PubMed]
- Hodges, P.W. Pain and motor control: From the laboratory to rehabilitation. J. Electromyogr. Kinesiol. 2011, 21, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Tin, C.; Poon, C.S. Internal models in sensorimotor integration: Perspectives from adaptive control theory. J. Neural Eng. 2005, 2, S147–S163. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35 (Suppl. 2), ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Fried, L.P. Frailty and the older man. Med. Clin. N. Am. 1999, 83, 1173–1194. [Google Scholar] [CrossRef]
- Lubart, R.; Eichler, M.; Lavi, R.; Friedman, H.; Shainberg, A. Low-energy laser irradiation promotes cellular redox activity. Photomed. Laser Surg. 2005, 23, 3–9. [Google Scholar] [CrossRef]
- Karu, T.I. Mitochondrial Signaling in Mammalian Cells Activated by Red and Near-IR Radiation. Photochem. Photobiol. 2008, 84, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Wilden, L.; Karthein, R. Import of radiation phenomena of electrons and therapeutic low-level laser in regard to the mitochondrial energy transfer. J. Clin. Laser Med. Surg. 1998, 16, 159–165. [Google Scholar] [CrossRef]
- Iozzo, R.V.; Schaefer, L. Proteoglycan form and function: A comprehensive nomenclature of proteoglycans. Matrix Biol. 2015, 42, 11–55. [Google Scholar] [CrossRef]
- Giuliani, M.; Fernandez, L.; Giardino, L.; Calzà, M.; Farinelli, L.; Baratto, R. Capra Peripheral Stimulation for Pain Treatment. Pathos 2003, 10, 115–119. [Google Scholar]
- Bai, Y.; Wang, J.; Wu, J.; Dai, J.; Sha, O.; Yew, D.T.W.; Yuan, L.; Liang, Q. Review of Evidence Suggesting That the Fascia Network Could Be the Anatomical Basis for Acupoints and Meridians in the Human Body. Evid. Based Complement. Altern. Med. 2011, 2011, 260510. [Google Scholar] [CrossRef]
- Ifrim-Chen, F.; Mircea, I. further study on the anatomical, histological and biochemical bases underlying clinical acupuncture effectiveness. J. Chin. Med. 2004, 15, 69–78. [Google Scholar]
- Ahn, A.C.; Park, M.; Shaw, J.R.; McManus, C.A.; Kaptchuk, T.J.; Langevin, H.M. Electrical impedance of acupuncture meridians: The relevance of subcutaneous collagenous bands. PLoS ONE 2010, 5, e11907. [Google Scholar] [CrossRef] [PubMed]
- Lazoura, H.; Cohen, M.; Lazoura, E.; Cosic, I. Do Acupuncture Points Have Different Absorption Properties to Laser Light than Surrounding Skin? In Proceedings of the 2nd International Conference on Bioelectromagnetism, Melbourne, Australia, 15–18 February 1998. [Google Scholar]
- Zhang, W.; Wang, G.; Fuxe, K. Classic and Modern Meridian Studies: A Review of Low Hydraulic Resistance Channels along Meridians and Their Relevance for Therapeutic Effects in Traditional Chinese Medicine. Evid. Based Complement. Altern. Med. 2015, 2015, 410979. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.S.; Li, P.; Nilius, B.; Li, G. Ancient Chinese medicine and mechanistic evidence of acupuncture physiology. Pflugers Arch. 2011, 462, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Langevin, H.M.; Churchill, D.L.; Cipolla, M.J. Mechanical signaling through connective tissue: A mechanism for the therapeutic effect of acupuncture. FASEB J. 2001, 15, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Chin, P.; Fung, W. Probing the mystery of Chinese medicine meridian channels with special emphasis on the connective tissue interstitial fluid system, mechanotransduction, cells durotaxis and mast cell degranulation. Chin. Med. 2009, 4, 10. [Google Scholar]
- L’acuponcture Chinoise; Published in English as Chinese Acupuncture; Mercure de France: Paris, France, 1939–1941; Paul, Z. (Ed.) Paradigm Publications: Brookline, MA, USA, 1994; Volume 2. [Google Scholar]
- Hempen, C.H. dtv-Atlas Akupunktur; Deutscher Taschenbuch Verlag GmbH & Co., KG: Munchen, Germany, 1997. [Google Scholar]
- Jarmey, C.; Bouratinos, I. A Practical Guide to Acupoints, 2nd ed.; Lotus Publishing: Chichester, UK, 2018. [Google Scholar]
- Regional Office for the Western Pacific, WHO. Standard Acupuncture Nomenclature, 2nd ed.; World Health Organization—Regional Office of Western Pacific Manila Philippines: Metro Manila, Philippines, 1993. [Google Scholar]
- Vanzini, M.; Gallamini, M. Amblyopia: Can laser acupuncture be an option? J. Acupunct. Meridian Stud. 2016, 9, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Vanzini, M.; Gallamini, M. Laser Acupuncture in Open-Angle Glaucoma Treatment A Retrospective Study of Eye Blood Flow. J. Acupunct. Meridian Stud. 2018. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CODE | NAME | Anatomic Reference |
|---|---|---|
| LI4 | Hegu | In the middle of the second metacarpal bone on the radial side. |
| LI5 | Yangxi | On the radial side of the wrist in a depression between extensor pollicis longus and brevis tendons, found when the thumb is tilted upward. |
| LI11 | Quchi | With the elbow flexed, on the radial side of the upper arm at the border of the humerus |
| TE5 | Waiguan | 2 cun over the dorsal wrist flex crease, between the radius and the ulna. |
| SI2 | Qiangu | When a loose fist is made, at the ulnar end of the crease, distal to the fifth metacarpophalangeal joint at the junction of the red and white skin |
| SI8 | Xiaohai | Between the olecranon process of the ulna and the medial epicondyle of the humerus, found with the elbow flexed. |
| LR2 | Xingjian | On the dorsum of the foot between the first and second toes, proximal to the margin of the web at the junction of the red and white skin. |
| KI3 | Taixi | In the depression midway between the tip of the medial malleolus and the attachment of the Achilles tendon |
| BL60 | Kunlun | In a depression between the tip of the external malleolus and the Achilles tendon |
| ST36 | Zusanli | 3 cun below ST35, one finger width lateral from the anterior border of the tibia. |
| ST38 | Tiaokou | 8 cun below ST35, one finger width lateral from the anterior border of the tibia. |
| FM23 (**) | Xiyan | Lateral and medial knee depressions |
| BL40 | Weizhong | Midpoint of the transverse crease of the popliteal fossa, between the tendons of biceps femoris and semitendinosus. |
| BL66 | Tonggu | Anterior to the fifth metatarsophalangeal joint. |
| GB34 | Yanglingquan | In a depression anterior and inferior to the head of the fibula. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evangelista, L.; De Meo, B.; Bernabei, G.; Belloni, G.; D’Angelo, G.; Vanzini, M.; Calzà, L.; Gallamini, M. Ultra-Low-Level Laser Therapy and Acupuncture Libralux: What Is so Special? Medicines 2019, 6, 40. https://doi.org/10.3390/medicines6010040
Evangelista L, De Meo B, Bernabei G, Belloni G, D’Angelo G, Vanzini M, Calzà L, Gallamini M. Ultra-Low-Level Laser Therapy and Acupuncture Libralux: What Is so Special? Medicines. 2019; 6(1):40. https://doi.org/10.3390/medicines6010040
Chicago/Turabian StyleEvangelista, Luca, Bruno De Meo, Gianluca Bernabei, Gabriele Belloni, Giovanni D’Angelo, Marzio Vanzini, Laura Calzà, and Michele Gallamini. 2019. "Ultra-Low-Level Laser Therapy and Acupuncture Libralux: What Is so Special?" Medicines 6, no. 1: 40. https://doi.org/10.3390/medicines6010040
APA StyleEvangelista, L., De Meo, B., Bernabei, G., Belloni, G., D’Angelo, G., Vanzini, M., Calzà, L., & Gallamini, M. (2019). Ultra-Low-Level Laser Therapy and Acupuncture Libralux: What Is so Special? Medicines, 6(1), 40. https://doi.org/10.3390/medicines6010040