
Effectiveness of Yoga Lifestyle on Lipid Metabolism in a Vulnerable Population—A Community Based Multicenter Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
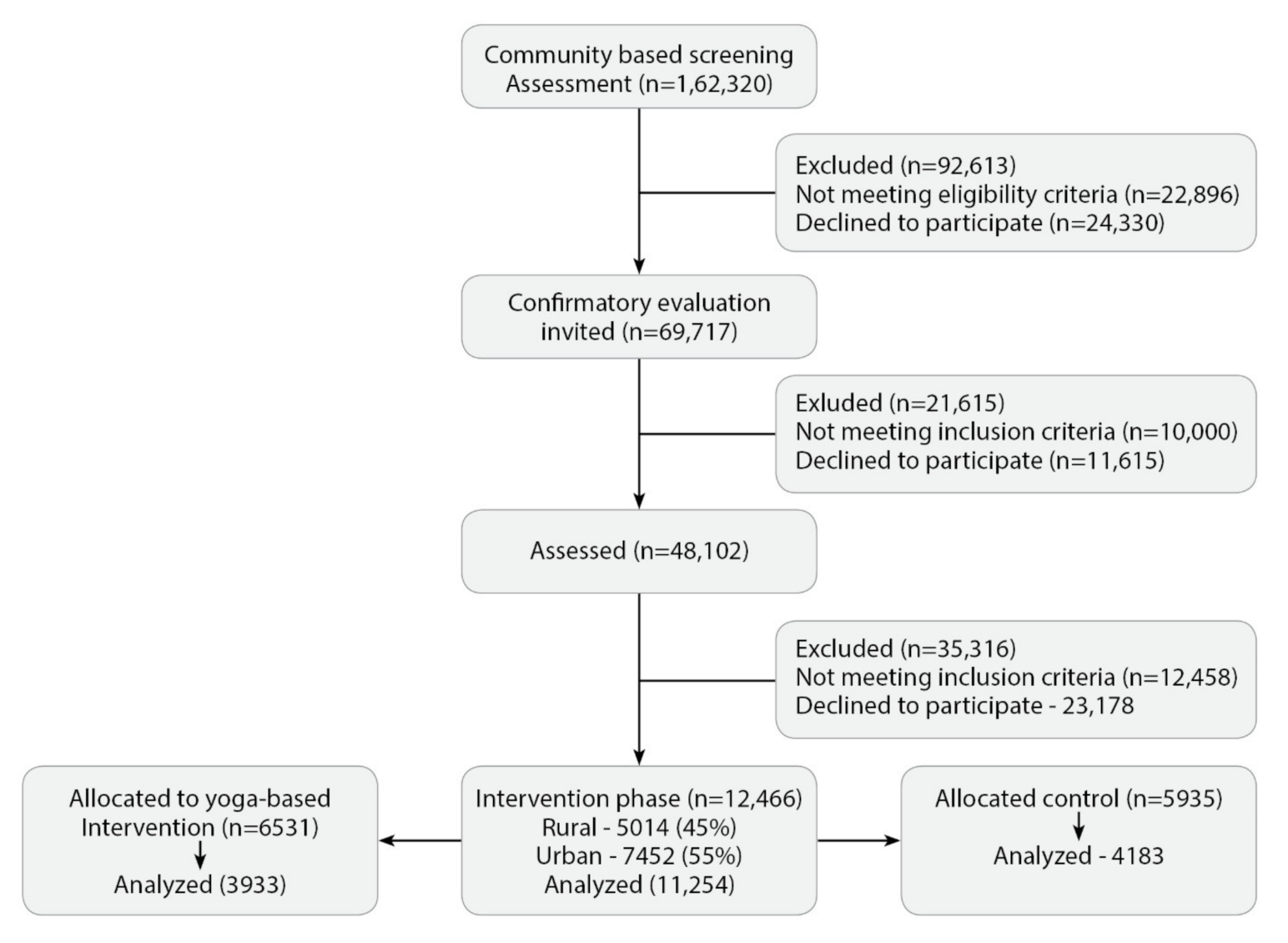
2.2. Screening and Recruitment
2.3. Randomization and Allocation Concealment
2.4. Selection Criteria for Phase 2 (RCT)
2.5. Blinding and Masking
2.6. Assessments
2.7. Quality Assurance and Training
2.8. Intervention
Diabetes Yoga Protocol
2.9. Statistical Analysis
3. Results
4. Discussion
4.1. Yoga as an Effective Tool
4.2. Strengths
4.3. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Ethical Compliance
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DYP | Diabetes yoga lifestyle protocol |
| NMB | Niyantrita Madhumeha Bharata Abhiyaan |
| NABL | National Accreditation Board for Testing and Calibration Laboratories |
| A1c | Glycated hemoglobin |
| TC | Total cholesterol |
| TG | Triglyceride |
| LDL | Low-density lipoprotein |
| HDL | High-density lipoprotein |
| VLDL | Very-low-density lipoprotein |
| T2DM | Type-2 diabetes mellitus |
| CHD | Coronary heart disease |
| ADA | American Diabetes Association |
| ANS | Autonomic nervous system |
| SAM | Sympatho-adrenal medullary |
| HPA | Hypothalamic pituitary adrenal |
| NO | Nitric oxide |
| IDRS | Indian diabetes risk score |
| IYA | Indian Yoga Association |
| CEB | Census enumeration blocks |
| SRF | Senior research fellows |
| ASHA | Accredited social health activists |
| IEC | Institutional ethics committee |
References
- Mithal, A.; Majhi, D.; Shunmugavelu, M.; Talwarkar, P.G.; Vasnawala, H.; Raza, A.S. Prevalence of dyslipidemia in adult Indian diabetic patients: A cross sectional study (SOLID). Indian J. Endocrinol. Metab. 2014, 18, 642–647. [Google Scholar] [CrossRef]
- Rosenson, R.S.; Brewer, H.B.; Ansell, B.; Barter, P.; Chapman, M.J.; Heinecke, J.W.; Kontush, A.; Tall, A.R.; Webb, N.R. Translation of high-density lipoprotein function into clinical practice: Current prospects and future challenges. Circulation 2013, 128, 1256–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, A.T.; Zhao, B.; Jose, P.O.; Azar, K.M.; Fortmann, S.P.; Palaniappan, L.P. Racial/Ethnic Differences in Dyslipidemia Patterns. Circulation 2014, 129, 570–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pu, J.; Romanelli, R.; Zhao, B.; Azar, K.M.; Hastings, K.G.; Nimbal, V.; Fortmann, S.P.; Palaniappan, L.P. Dyslipidemia in Special Ethnic Populations. Cardiol. Clin. 2015, 33, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Chandra, K.S.; Bansal, M.; Nair, T.; Iyengar, S.; Gupta, R.; Manchanda, S.C.; Mohanan, P.; Rao, V.D.; Manjunath, C.; Sawhney, J.; et al. Consensus statement on management of dyslipidemia in Indian subjects. Indian Heart J. 2014, 66, S1–S51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmer, J.A. Diabetic dyslipidemia and atherosclerosis: Evidence from clinical trials. Curr. Diabetes Rep. 2008, 8, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Management of dyslipidemia in adults with diabetes. Diabetes care 2003, 26, s83–s86. [Google Scholar]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic Syndrome as a Precursor of Cardiovascular Disease and Type 2 Diabetes Mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef]
- Joshi, S.R.; Anjana, R.M.; Deepa, M.; Pradeepa, R.; Bhansali, A.; Dhandania, V.K.; Joshi, P.P.; Unnikrishnan, R.; Nirmal, E.; Subashini, R.; et al. Prevalence of Dyslipidemia in Urban and Rural India: The ICMR–INDIAB Study. PLoS ONE 2014, 9, e96808. [Google Scholar] [CrossRef] [Green Version]
- Fox, C.S.; Coady, S.; Sorlie, P.D.; D’Agostino, R.B.; Pencina, M.J.; Vasan, R.S.; Meigs, J.B.; Levy, D.; Savage, P.J. Increasing Cardiovascular Disease Burden Due to Diabetes Mellitus. Circulation 2007, 115, 1544–1550. [Google Scholar] [CrossRef]
- Silverio, A.; Cavallo, P.; De Rosa, R.; Galasso, G. Big Health Data and Cardiovascular Diseases: A Challenge for Research, an Opportunity for Clinical Care. Front. Med. 2019, 6, 36. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.; Mondal, S.; Kundu, B. Yoga as a therapeutic intervention for the management of type 2 diabetes mellitus. Int. J. Yoga 2018, 11, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Tundwala, V.; Gupta, R.P.; Kumar, S.; Singh, V.B.; Sandeep, B.R.; Dayal, P.; Prakash, P. A study on effect of yoga and various asanas on obesity, hypertension and dyslipidemia. Int. J. Basic Appl. Med. Sci. 2012, 2, 93–98. [Google Scholar]
- Chandrasekaran, A.M.; Kinra, S.; Ajay, V.S.; Chattopadhyay, K.; Singh, K.; Singh, K.; Praveen, P.A.; Soni, D.; Devarajan, R.; Kondal, D.; et al. Effectiveness and cost-effectiveness of a Yoga-based Cardiac Rehabilitation (Yoga-CaRe) program following acute myocardial infarction: Study rationale and design of a multi-center randomized controlled trial. Int. J. Cardiol. 2019, 280, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Sudha, S.; Chopra, M.; Khan, F.; Sharma, K. Physical Exercise and Yoga: As an alternative approach towards COVID-19 management. Curr. Tradit. Med. 2021, 7, 1. [Google Scholar] [CrossRef]
- Yeung, A.C.; Chang, D.H.T.; Bensoussan, A.; Kiat, H. Yoga and cardiac rehabilitation: A brief review of evidence. J. Yoga Phys. Ther. 2015, 5, 1000207. [Google Scholar] [CrossRef]
- Bali, P.; Kaur, N.; Tiwari, A.; Bammidi, S.; Podder, V.; Devi, C.; Kumar, S.; Sivapuram, M.S.; Ghani, A.; Modgil, S.; et al. Effectiveness of Yoga as the Public Health Intervention Module in the Management of Diabetes and Diabetes Associated Dementia in South East Asia: A Narrative Review. Neuroepidemiology 2020, 54, 287–303. [Google Scholar] [CrossRef]
- Pal, D.K.; Bhalla, A.; Bammidi, S.; Telles, S.; Kohli, A.; Kumar, S.; Devi, P.; Kaur, N.; Sharma, K.; Kumar, R.; et al. Can Yoga-Based Diabetes Management Studies Facilitate Integrative Medicine in India Current Status and Future Directions. Integr. Med. Int. 2017, 4, 125–141. [Google Scholar] [CrossRef]
- Arati, M.; Arpita, P.; Arati, M. Effect of yoga (asana and pranayama) on serum lipid profile in normal healthy volunteers. Int. J. Contemp. Med. Res. 2015, 2, 1277–1281. [Google Scholar]
- Behar, S.; Graff, E.; Reicher-Reiss, H.; Boyko, V.; Benderly, M.; Shotan, A.; Brunner, D. Low total cholesterol is associated with high total mortality in patients with coronary heart disease. Eur. Heart J. 1997, 18, 52–59. [Google Scholar] [CrossRef]
- Elmehdawi, R.R. Hypolipidemia: A word of caution. Libyan J. Med. 2008, 3, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Shantakumari, N.; Sequeira, S.; El Deeb, R. Effects of a yoga intervention on lipid profiles of diabetes patients with dyslipidemia. Indian Heart J. 2013, 65, 127–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damodaran, A.; Malathi, A.; Patil, N.; Shah, N.; Marathe, S. Therapeutic potential of yoga practices in modifying cardiovascular risk profile in middle aged men and women. J. Assoc. Physicians India 2002, 50, 633–640. [Google Scholar]
- Innes, K.E.; Selfe, T.K. Yoga for Adults with Type 2 Diabetes: A Systematic Review of Controlled Trials. J. Diabetes Res. 2016, 2016, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Raveendran, A.V.; Deshpandae, A.; Joshi, S.R. Therapeutic Role of Yoga in Type 2 Diabetes. Endocrinol. Metab. 2018, 33, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Gotto Jr, A.M. Cholesterol management in theory and practice. Circulation 1997, 96, 4424–4430. [Google Scholar] [CrossRef]
- Mahesh, N.K.; Kumar, A.; Bhat, K.G.; Verma, N. Role of yoga therapy on lipid profile in patients of hypertension and prehypertension. Int. J. Adv. Med. 2018, 5, 321. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, R.; Banu, A.; Irman, S.; Jaiswal, R.K. Importance of yoga in diabetes and dyslipidemia. Int. J. Res. Med. Sci. 2016, 4, 3504–3508. [Google Scholar] [CrossRef] [Green Version]
- Nagendra, H.R.; Nagarathna, R.; Rajesh, S.K.; Amit, S.; Telles, S.; Hankey, A. Niyantrita Madhumeha Bharata 2017, methodology for a nationwide diabetes prevalence estimate: Part 1. Int. J. Yoga 2019, 12, 179–192. [Google Scholar] [CrossRef]
- Weber, M.B.; Ranjani, H.; Staimez, L.R.; Anjana, R.M.; Ali, M.; Narayan, K.V.; Mohan, V. The Stepwise Approach to Diabetes Prevention: Results From the D-CLIP Randomized Controlled Trial. Diabetes Care 2016, 39, 1760–1767. [Google Scholar] [CrossRef] [Green Version]
- Nagarathna, R.; Rajesh, S.K.; Amit, S.; Patil, S.; Anand, A.; Nagendra, H.R. Methodology of Niyantrita Madhumeha Bharata Abhiyaan- 2017, a nationwide multicentric trial on the effect of a validated culturally acceptable lifestyle intervention for primary prevention of diabetes: Part 2. Int. J. Yoga 2019, 12, 193–205. [Google Scholar] [CrossRef]
- Sattar, N.; Rawshani, A.; Franzén, S.; Rawshani, A.; Svensson, A.M.; Rosengren, A.; McGuire, D.K.; Eliasson, B.; Gudbjörnsdottir, S. Age at diagnosis of type 2 diabetes mellitus and associations with cardiovascular and mortality risks: Findings from the Swedish National Diabetes Registry. Circulation 2019, 139, 2228–2237. [Google Scholar] [CrossRef]
- Kaur, N.; Malik, N.; Mathur, D.; Pal, S.; Malik, R.; Rana, S. Mindfulness and yoga halt the conversion of pre-diabetic rural women into diabetics-a pilot study. Integr. Med. Case Rep. 2020, 1, 8–18. [Google Scholar] [CrossRef]
- Singh, S.; Kyizom, T.; Singh, K.P.; Tandon, O.P.; Madhu, S.V. Influence of pranayamas and yoga-asanas on serum insulin, blood glucose and lipid profile in type 2 diabetes. Indian J. Clin. Biochem. 2008, 23, 365–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bijlani, R.L.; Vempati, R.P.; Yadav, R.K.; Ray, R.B.; Gupta, V.; Sharma, R.; Mehta, N.; Mahapatra, S.C. A Brief but Comprehensive Lifestyle Education Program Based on Yoga Reduces Risk Factors for Cardiovascular Disease and Diabetes Mellitus. J. Altern. Complement. Med. 2005, 11, 267–274. [Google Scholar] [CrossRef]
- Satyapriya, M.; Nagarathna, R.; Padmalatha, V.; Nagendra, H. Effect of integrated yoga on anxiety, depression & well being in normal pregnancy. Complement. Ther. Clin. Pr. 2013, 19, 230–236. [Google Scholar] [CrossRef]
- Satyapriya, M.; Nagendra, H.R.; Nagarathna, R.; Padmalatha, V. Effect of integrated yoga on stress and heart rate variability in pregnant women. Int. J. Gynecol. Obstet. 2008, 104, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Madanmohan, A.B.B.; Sanjay, Z.; Dayanidy, G.; Basavaraddi, I.V. Effect of yoga therapy on reaction time, biochemical parameters and wellness score of peri and post-menopausal diabetic patients. Int. J. Yoga 2012, 5, 5–10. [Google Scholar] [CrossRef]
- Udupa, K.; Sathyaprabha, T.N.; Telles, S.; Singh, N. Influence of Yoga on the Autonomic Nervous System. In Research-Based Perspectives on the Psychophysiology of Yoga; IGI Global: Hershey, PA, USA, 2018; pp. 67–85. [Google Scholar]
- Sathyaprabha, T.; Kisan, R.; Adoor, M.; Nalini, A.; Kutty, B.M.; Murthy, B.C.; Sujan, M.; Rao, R.; Raju, T. Effect of Yoga on migraine: A comprehensive study using clinical profile and cardiac autonomic functions. Int. J. Yoga 2014, 7, 126–132. [Google Scholar] [CrossRef]
- Rao, R.M.; Vadiraja, H.; Nagaratna, R.; Gopinath, K.S.; Patil, S.; Diwakar, R.B.; Shahsidhara, H.; Ajaikumar, B.; Nagendra, H. Effect of yoga on sleep quality and neuroendocrine immune response in metastatic breast cancer patients. Indian J. Palliat. Care 2017, 23, 253–260. [Google Scholar] [CrossRef]
- Goldstein, J.L.; Brown, M.S. History of Discovery: The LDL receptor. Arterioscler. Thromb. Vasc. Biol. 2009, 29, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Rosenson, R.S.; Brewer, H.B.; Davidson, W.S.; Fayad, Z.A.; Fuster, V.; Goldstein, J.; Hellerstein, M.; Jiang, X.C.; Phillips, M.C.; Rader, D.J.; et al. Cholesterol efflux and atheroprotection: Advancing the concept of reverse cholesterol transport. Circulation 2012, 125, 1905–1919. [Google Scholar] [CrossRef] [Green Version]
- Pal, R.; Gupta, N. Yogic practices on oxidative stress and of antioxidant level: A systematic review of randomized controlled trials. J. Complement. Integr. Med. 2017, 16. [Google Scholar] [CrossRef] [PubMed]
- Manna, I. Effects of yoga training on body composition and oxidant-antioxidant status among healthy male. Int. J. Yoga 2018, 11, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Shete, S.U.; Verma, A.; Kulkarni, D.D.; Bhogal, R.S. Effect of yoga training on inflammatory cytokines and C-reactive protein in employees of small-scale industries. J. Educ. Health Promot. 2017, 6, 76. [Google Scholar] [CrossRef] [PubMed]
- Javalkar, S.R. The economic burden of health expenditure on diabetes mellitus among urban poor: A cross sectional study. Int. J. Community Med. Public Health 2019, 6, 1162–1166. [Google Scholar] [CrossRef] [Green Version]
- Podder, V.; Srivastava, V.; Kumar, S.; Nagarathna, R.; Sivapuram, M.S.; Kaur, N.; Sharma, K.; Singh, A.K.; Malik, N.; Anand, A.; et al. Prevalence and Awareness of Stroke and Other Comorbidities Associated with Diabetes in Northwest India. J. Neurosci. Rural. Pr. 2020, 11, 467–473. [Google Scholar] [CrossRef]
- Kumar, S.; Anand, A.; Nagarathna, R.; Kaur, N.; Sivapuram, M.S.; Pannu, V.; Pal, D.K.; Malik, N.; Singh, A.K.; Nagendra, H.R. Prevalence of prediabetes, and diabetes in Chandigarh and Panchkula region based on glycated haemoglobin and Indian diabetes risk score. Endocrinol. Diabetes Metab. 2021, 4, 162. [Google Scholar] [CrossRef]
- Goyal, A.K.; Bhadada, S.; Malik, N.; Anand, A.; Kumar, R.; Bammidi, S.; Tyagi, R.; Modgil, S.; Sharma, K.; Bali, P.; et al. Guinness world record attempt as a method to pivot the role of Yoga in Diabetes management. Ann. Neurosci. 2019, 26, 21–24. [Google Scholar] [CrossRef] [Green Version]
- Anand, A.; Banik, A.; Thakur, K.; Masters, C.L. The Animal Models of Dementia and Alzheimer’s Disease for Pre-Clinical Testing and Clinical Translation. Curr. Alzheimer Res. 2012, 9, 1010–1029. [Google Scholar] [CrossRef]
- Sharma, N.K.; Gupta, A.; Prabhakar, S.; Singh, R.; Sharma, S.K.; Chen, W.; Anand, A. Association between CFH Y402H Polymorphism and Age Related Macular Degeneration in North Indian Cohort. PLoS ONE 2013, 8, e70193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagarathna, R.; Tyagi, R.; Kaur, G.; Vendan, V.; Acharya, I.N.; Anand, A.; Singh, A.; Nagendra, H.R. Efficacy of a Validated Yoga Protocol on Dyslipidemia in Diabetes Patients: NMB-2017 India Trial. Medicines 2019, 6, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ved, R.R.; Gupta, G.; Singh, S. India’s health and wellness centres: Realizing universal health coverage through comprehensive primary health care. WHO South-East Asia J. Public Health 2019, 8, 18–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Demographic Details | Yoga | Control | p Value | ||
|---|---|---|---|---|---|
| Age (years) | Mean ± SD | 48.7 ± 10.64 | 48.41 ± 10.22 | 0.03 | |
| Gender | Male N (%) | 1682 (42.8%) | 1710 (40.9%) | <0.001 | |
| Female N (%) | 2251 (57.2%) | 2473 (59.1%) | |||
| Area | Urban N (%) | 2693 (69.5%) | 2203 (52.7%) | <0.001 | |
| Rural N (%) | 1240 (31.5%) | 1980 (47.3%) | |||
| Occupation | Profession | 594 | 778 | 0.05 | |
| Semi-Profession | 106 | 130 | |||
| Clerical, Shop owner | 1415 | 1405 | |||
| Skilled worker | 1321 | 1345 | |||
| Semi-skilled worker | 90 | 95 | |||
| Unskilled worker | 153 | 170 | |||
| Diabetes status | Self-declared Known DM | <5 yrs | 502 | 616 | <0.001 |
| 5–10 yrs | 163 | 220 | |||
| >10 yrs | 160 | 209 | |||
| Newly diagnosed DM | 1105 | 2145 | |||
| Pre-diabetes | 806 | 678 | |||
| No DM, only high risk on IDRS | 1197 | 315 | |||
| Group | TC_Pre (mg/dL) | TC_Post (mg/dL) | TG_Pre (mg/dL) | TG_Post (mg/dL) | LDL_Pre (mg/dL) | LDL_Post (mg/dL) | HDL_Pre (mg/dL) | HDL_Post (mg/dL) |
|---|---|---|---|---|---|---|---|---|
| Yoga | 181.80 ± 39.75 | 176.64 ± 38.59 *† | 150.42 ± 70.52 | 153.51 ± 72.88 *† | 103.54 ± 34.09 | 98.65 ± 33.67 *† | 49.30 ± 11.48 | 48.61 ± 11.55 *† |
| Control | 183.44 ± 40.33 | 193.27 ± 47.27 * | 155.86 ± 79.40 | 191.12 ± 107.44 * | 103.99 ± 33.00 | 108.01 ± 40.4 * | 48.92 ± 11.53 | 44.62 ± 12.15 * |
| Groups | Lipid Categories | Diabetes A1c (≥6.5) | Prediabetes (A1c 5.3–6.4) with Diabetes High Risk (IDRS ≥ 60) | Normoglycemia (A1c <5.3) with Diabetes High Risk (IDRS ≥60) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre, mg/dL | Post, mg/dL | Diff (%) | Pre, mg/dL | Post, mg/dL | Diff (%) | Pre, mg/dL | Post, mg/dL | Diff (%) | ||
| Yoga | TC (<150) | 131.35 ± 15.76 | 167.62 ± 37.67 | −36.27 *† (27.6%) | 130.25 ± 16.20 | 160.94 ± 37.02 | −30.69 * (23.5%) | 131.80 ± 15.30 | 163.83 ± 39.55 | −32.03 * (24.3%) |
| TC (150–200) | 175.32 ± 14.18 | 176.61 ± 38.97 | −1.29 (0.73%) | 174.25 ± 13.93 | 174.92 ± 36.88 | −0.67† (0.38%) | 175.61 ± 13.72 | 174.50 ± 35.34 | 1.11 (0.63%) | |
| TC (>200) | 228.71 ± 24.20 | 185.83 ± 37.61 | 42.87 *† (18.7%) | 230.24 ± 25.64 | 187.10 ± 39.79 | 43.14 *† (18.7%) | 232.64 ± 27.93 | 187.55 ± 39.07 | 45.09 *(19.3%) | |
| TG (<150) | 104.97 ± 26.33 | 147.60 ± 71.72 | −42.62 *† (40.6%) | 105.63 ± 25.70 | 143.61 ± 67.49 | −37.98 *† (35.9%) | 104.96 ± 25.49 | 148.03 ± 70.88 | −43.07 * (41.0%) | |
| TG (150–200) | 173.51 ± 14.58 | 155.25 ± 71.17 | 18.26 *† (10.5%) | 171.58 ± 14.19 | 155.81 ± 61.34 | 15.77 *† (9.19%) | 173.06 ± 14.55 | 169.29 ± 81.49 | 3.77 (2.17%) | |
| TG (>200) | 266.78 ± 56.77 | 164.65 ± 74.78 | 102.18 *† (38.3%) | 267.97 ± 60.35 | 173.76 ± 81.09 | 94.21 *† (35.1%) | 262.82 ± 55.22 | 168.69 ± 80.60 | 94.13 * (35.8%) | |
| LDL (<100) | 76.68 ± 15.96 | 95.04 ± 34.41 | −18.36 *† (23.9%) | 76.55 ± 16.76 | 92.66 ± 33.15 | −16.11 * (21.0%) | 76.56 ± 17.02 | 92.19 ± 31.17 | −15.37 * (20.0%) | |
| LDL (100–130) | 113.79 ± 8.53 | 101.32 ± 31.96 | 12.47 *† (10.9%) | 113.06 ± 8.18 | 98.34 ± 31.88 | 14.72 *† (13.0%) | 113.91 ± 8.27 | 100.67 ± 31.93 | 13.23 * (11.6%) | |
| LDL (>130) | 152.75 ± 20.71 | 107.06 ± 35.31 | 45.68 *† (29.9%) | 154.14 ± 21.15 | 108.14 ± 35.04 | 46.0 *† (29.8%) | 155.41 ± 24.62 | 108.25 ± 35.03 | 47.15 * (30.3%) | |
| HDL (<45) | 38.69 ± 5.26 | 47.01 ± 11.43 | −8.31 *† (21.4%) | 38.48 ± 5.17 | 45.98 ± 11.34 | −7.5 (19.4%) | 38.70 ± 5.24 | 46.34 ± 11.32 | −7.64 * (19.7%) | |
| HDL (45–60) | 52.12 ± 4.14 | 49.39 ± 11.54 | 2.72 *† (5.2%) | 52.25 ± 4.28 | 50.12 ± 11.40 | 2.13 *† (4.0%) | 52.07 ± 4.21 | 49.22 ± 11.06 | 2.85 * (5.4%) | |
| HDL (>60) | 67.86 ± 6.74 | 51.36 ± 11.51 | 16.49 *† (24.3%) | 67.66 ± 6.94 | 51.25 ± 11.56 | 16.41 *† (24.2%) | 69.07 ± 9.11 | 50.84 ± 12.40 | 18.23 * (26.3%) | |
| Control | TC (<150) | 130.65 ± 15.57 | 170.51 ± 40.59 | −39.86 * (30.5%) | 130.40 ± 14.89 | 167.51 ± 37.52 | −37.10 * (28.4%) | 128.57 ± 14.05 | 180.68 ± 52.30 | −52.11 * (40.5%) |
| TC (150–200) | 175.53 ± 14.17 | 182.58 ± 41.71 | −7.05 * (4%) | 175.82 ± 13.77 | 182.46 ± 40.62 | −6.63 * (3.8%) | 173.26 ± 14.12 | 181.01 ± 42.40 | −7.74 * (4.46%) | |
| TC (>200) | 228.75 ± 27.34 | 224.04 ± 44.16 | 4.70 * (2.0%) | 227.27 ± 24.48 | 221.15 ± 40.59 | 6.11 * (2.7%) | 229.43 ± 25.02 | 225.69 ± 40.98 | 3.74 * (1.63%) | |
| TG (<150) | 104.76 ± 25.95 | 162.69 ± 102.67 | −57.93 * (55.2%) | 106.41 ± 26.33 | 174.32 ± 111.57 | −67.90 * (63.8%) | 106.68 ± 27.13 | 164.42 ± 100.67 | −57.73 * (54.1%) | |
| TG (150–200) | 173.09 ± 14.65 | 158.38 ± 80.19 | 14.71 * (3.18%) | 173.60 ± 15.59 | 167.25 ± 86.19 | 6.34 * (3.6%) | 177.69 ± 16.44 | 165.00 ± 88.74 | 12.69 (7.1%) | |
| TG (>200) | 278.24 ± 64.15 | 287.10 ± 75.54 | −8.85 * (3.1%) | 274.04 ± 64.22 | 284.63 ± 74.75 | −10.59 * (3.8%) | 278.12 ± 67.55 | 288.13 ± 75.20 | −10.01 * (4.5%) | |
| LDL (<100) | 76.79 ± 16.08 | 95.78 ± 33.91 | −18.98 * (24.7%) | 76.71 ± 16.03 | 100.65 ± 36.26 | −23.94 * (31.2%) | 75.95 ± 16.96 | 98.89 ± 34.74 | −22.94 * (30.2%) | |
| LDL (100–129) | 114.44 ± 8.47 | 99.44 ± 34.25 | 14.99 * (13.0%) | 113.98 ± 8.61 | 100.90 ± 38.79 | 13.08 * (11.4%) | 114.78 ± 8.68 | 94.11 ± 34.02 | 20.67 * (18.0%) | |
| LDL (>130) | 151.63 ± 18.93 | 146.32 ± 37.31 | 5.31 * (3.5%) | 149.74 ± 16.28 | 143.78 ± 18;25 | 5.96 * (3.98%) | 151.70 ± 18.68 | 145.87 ± 39.92 | 5.82 (3.8%) | |
| HDL (<45) | 38.86 ± 5.00 | 38.21 ± 7.53 | 0.44 (1.1%) | 38.13 ± 4.98 | 37.03 ± 7.13 | 1.10 * (2.8%) | 37.90 ± 4.64 | 38.25 ± 6.61 | −0.34 (0.89%) | |
| HDL (45–60) | 51.96 ± 4.13 | 48.68 ± 12.81 | 3.28 * (6.3%) | 51.62 ± 4.28 | 48.85 ± 13.44 | 2.76 * (5.2%) | 51.67 ± 3.89 | 49.11 ± 13.18 | 2.55 * (4.9%) | |
| HDL (>60) | 67.90 ± 6.08 | 51.45 ± 11.88 | 16.44 * (24.2%) | 68.24 ± 6.21 | 49.75 ± 11.85 | 18.48 * (27.0%) | 67.28 ± 5.00 | 50.92 ± 11.66 | 16.35 * (24.3%) | |
| Groups | TC (mg/dL) | TG (mg/dL) | LDL (mg/dL) | HDL (mg/dL) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Y/C | Pre | Post | Df | Pre | Post | Df | pre | Post | Df | pre | Post | df | ||
| Gender | Male | Y | 181.96 ± 39.77 | 177.44 ± 38.43 | 4.52 | 150.02 ± 69.88 | 154.33 ± 73.82 | −4.31 | 103.5 ± 34.72 | 98.73 ± 33.36 | 4.78 | 49.3 ± 11.53 | 48.90 ± 11.83 | 0.48 |
| C | 181.24 ± 39.63 | 192.73 ± 47.73 | −11.49 | 153.74 ± 77.62 | 189.80 ± 108.57 | −36.06 | 104.88 ± 32.90 | 109.07 ± 41.25 | −4.19 | 49.30 ± 11.55 | 44.77 ± 12.26 | 4.52 | ||
| Female | Y | 181.68 ± 39.74 | 176.03 ± 38.70* | 5.64 | 150.73 ± 71.01 | 152.89 ± 72.17 | −2.16 | 103.56 ± 33.61 | 98.59 ± 33.90* | 4.96 | 49.24 ± 11.44 | 48.39 ± 11.34 | 0.84 | |
| C | 184.96 ± 40.75 | 193.65 ± 46.95 | −8.68 | 157.34 ± 80.60 | 192.04 ± 106.65 | −34.69 | 103.37 ± 33.05 | 107.28 ± 39.88 | −3.90 | 48.66 ± 11.51 | 44.51 ± 12.08 | 4.15 | ||
| Location | Urban | Y | 181.30 ± 39.74 | 176.66 ± 38.74 | 4.63 | 150.16 ± 7070.62 | 153.87 ± 73.05 | −3.70 | 103.07 ± 34.11 | 98.54 ± 33.84 * | 4.53 | 49.41 ± 11.39 | 48.66 ± 11.64 | 0.75 |
| C | 183.30 ± 40.00 | 193.99 ± 47.13 * | −10.69 | 154.43 ± 79.19 | 188.01 ± 105.64 | −33.58 | 104.35 ± 33.18 | 107.7 ± 40.14 * | −3.41 | 49.00 ± 11.67 | 44.94 ± 12.40 * | 4.06 | ||
| Rural | Y | 182.89 ± 39.77 | 176.58 ± 38.39 * | 6.31 | 150.99 ± 70.33 | 152.72 ± 72.51 | −1.72 | 104.55 ± 34.04 | 98.88 ± 33.31 * | 5.66 | 49.07 ± 11.67 | 48.51 ± 11.37 | 0.56 | |
| C | 183.59 ± 40.70 | 192.48 ± 47.42 | −8.8 | 157.45 ± 79.63 * | 194.56 ± 109.32 | −37.11 | 103.5 ± 32.79 * | 108.2 ± 40.80 * | −4.69 | 48.83 ± 11.37 | 44.26 ± 11.87 * | 4.57 | ||
| Age groups | <40 | Y | 180.80 ± 38.78 | 177.0 ± 38.38 * | 3.78 | 149.63 ± 73.17 | 150.10 ± 70.10 | −0.46 | 102.28 ± 33.28 | 99.62 ± 33.40 | 2.65 | 49.33 ± 11.16 | 48.83 ± 11.21 | 0.50 |
| <40 | C | 182.42 ± 40.51 | 195.43 ± 46.12 | −11.00 | 155.05 ± 78.79 | 191.03 ± 109.61 | −35.98 | 104.28 ± 32.65 | 107.91 ± 40.93 | −3.63 | 49.30 ± 11.52 | 44.88 ± 12.46 | 4.42 | |
| >40 | Y | 182.18 ± 39.93 | 176.49 ± 38.85 * | 5.68 | 150.71 ± 69.49 | 154.90 ± 73.79 * | −4.18 | 103.92 ± 34.33 | 98.28 ± 33.92 * | 5.64 | 49.34 ± 11.54 | 48.55 ± 11.54 * | 0.79 | |
| >40 | C | 183.10 ± 40.27 | 192.53 ± 47.65 * | −9.43 | 156.14 ± 79.63 | 191.15 ± 106.70 * | −35.00 | 103.89 ± 33.12 | 108.0 ± 40.29 * | −4.15 | 48.79 ± 11.53 | 44.53 ± 12.05 * | 4.26 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagarathna, R.; Kumar, S.; Anand, A.; Acharya, I.N.; Singh, A.K.; Patil, S.S.; Latha, R.H.; Datey, P.; Nagendra, H.R. Effectiveness of Yoga Lifestyle on Lipid Metabolism in a Vulnerable Population—A Community Based Multicenter Randomized Controlled Trial. Medicines 2021, 8, 37. https://doi.org/10.3390/medicines8070037
Nagarathna R, Kumar S, Anand A, Acharya IN, Singh AK, Patil SS, Latha RH, Datey P, Nagendra HR. Effectiveness of Yoga Lifestyle on Lipid Metabolism in a Vulnerable Population—A Community Based Multicenter Randomized Controlled Trial. Medicines. 2021; 8(7):37. https://doi.org/10.3390/medicines8070037
Chicago/Turabian StyleNagarathna, Raghuram, Saurabh Kumar, Akshay Anand, Ishwara N. Acharya, Amit Kumar Singh, Suchitra S. Patil, Ramesh H Latha, Purnima Datey, and Hongasandra Ramarao Nagendra. 2021. "Effectiveness of Yoga Lifestyle on Lipid Metabolism in a Vulnerable Population—A Community Based Multicenter Randomized Controlled Trial" Medicines 8, no. 7: 37. https://doi.org/10.3390/medicines8070037
APA StyleNagarathna, R., Kumar, S., Anand, A., Acharya, I. N., Singh, A. K., Patil, S. S., Latha, R. H., Datey, P., & Nagendra, H. R. (2021). Effectiveness of Yoga Lifestyle on Lipid Metabolism in a Vulnerable Population—A Community Based Multicenter Randomized Controlled Trial. Medicines, 8(7), 37. https://doi.org/10.3390/medicines8070037