


Epileptic Tissue Localization through Skewness-Based Functional Connectivity in the High-Frequency Band of Intracranial EEG

Abstract
:1. Introduction
2. Methods
2.1. iEEG Dataset
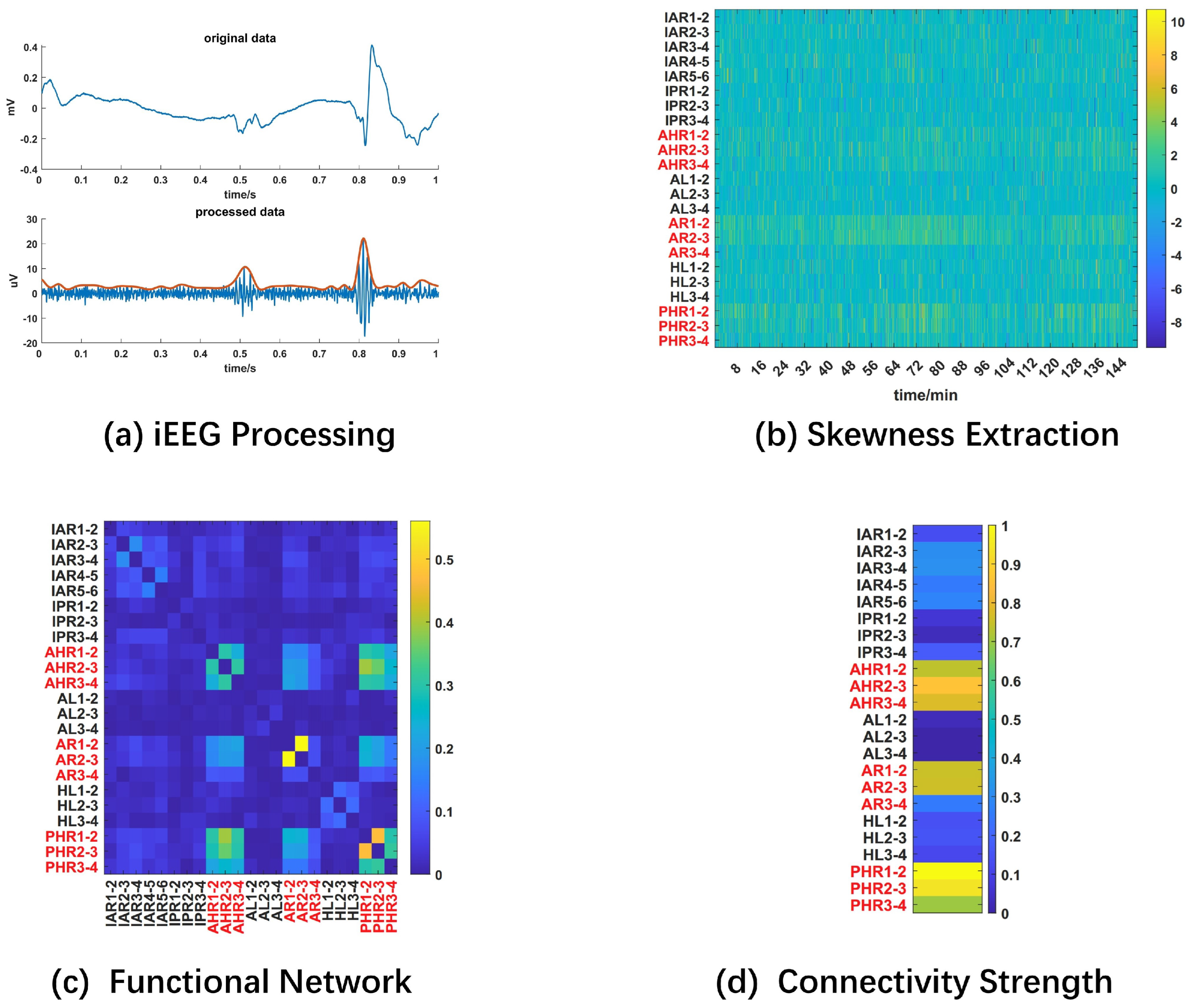
2.2. iEEG Signal Processing
- Bad channel removal: bad channels marked in the datasets are excluded;
- Rereference: iEEG signals are transformed into a bipolar montage for each electrode to suppress interference caused by severe common-mode noise and outliers during recording;
- Filtering: each iEEG segment is band-passed in the range of 80–500 Hz (dataset 1) or high-passed above 80 Hz (dataset 2) with a finite-impulse-response (FIR) forward–backward filter with stopband attenuation at 60 dB in the Fieldtrip toolbox [24]; furthermore, 60 Hz power line noise and its harmonics are filtered out with two-order Butterworth notch filters with a cutoff frequency of 5 Hz;
- Envelope extraction: the peak upper envelope of iEEG signals is extracted using spline interpolation over local maxima. The upper envelope is used to remove the influence of oscillating components;
- Segmentation: the continuous envelope is further segmented into 1-second epochs without overlap to enhance the temporal resolution.
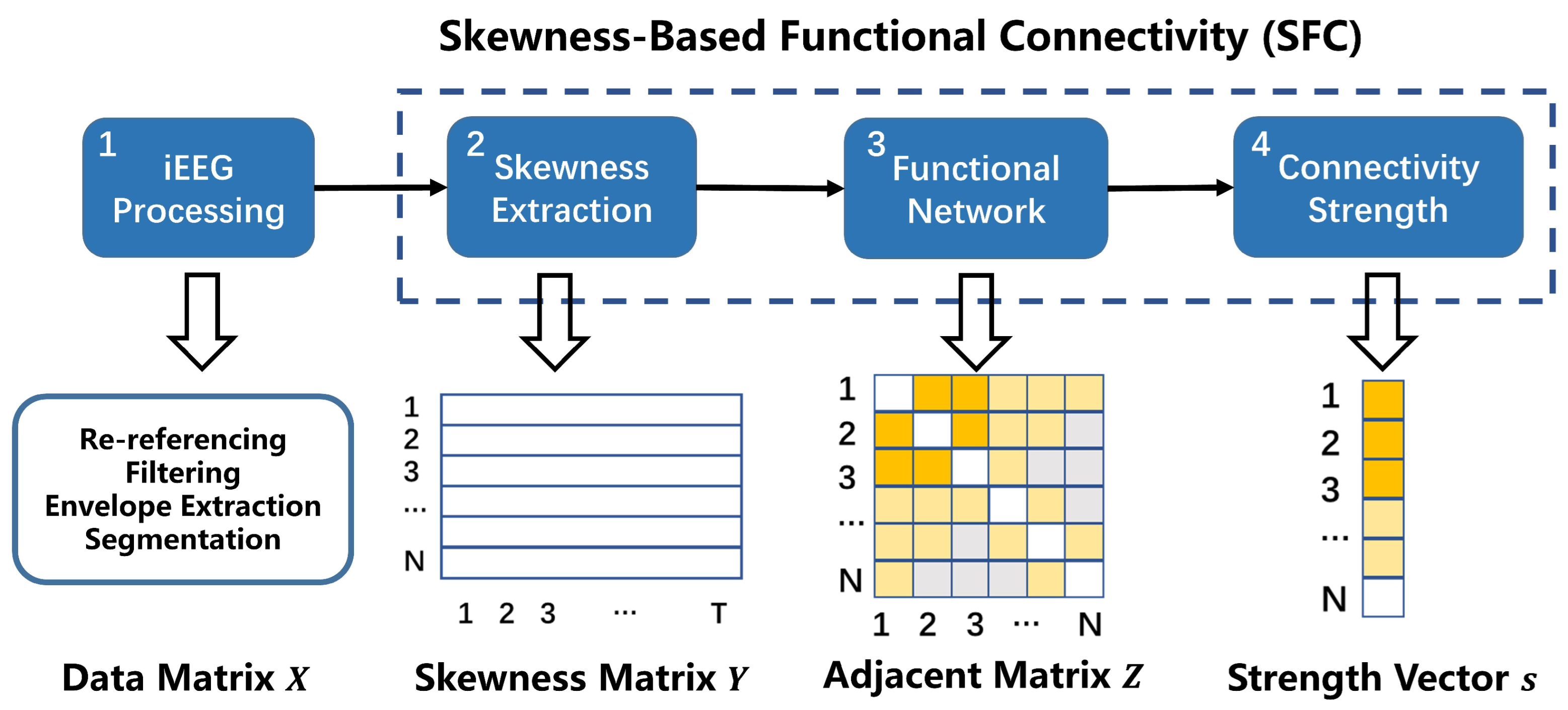
2.3. Skewness-Based Functional Connectivity Analysis
2.4. Epileptic Tissue Localization
2.5. Comparison with the Low-Frequency Band and Direct Extension to the High-Frequency Band
2.6. Statistical Analysis
3. Results
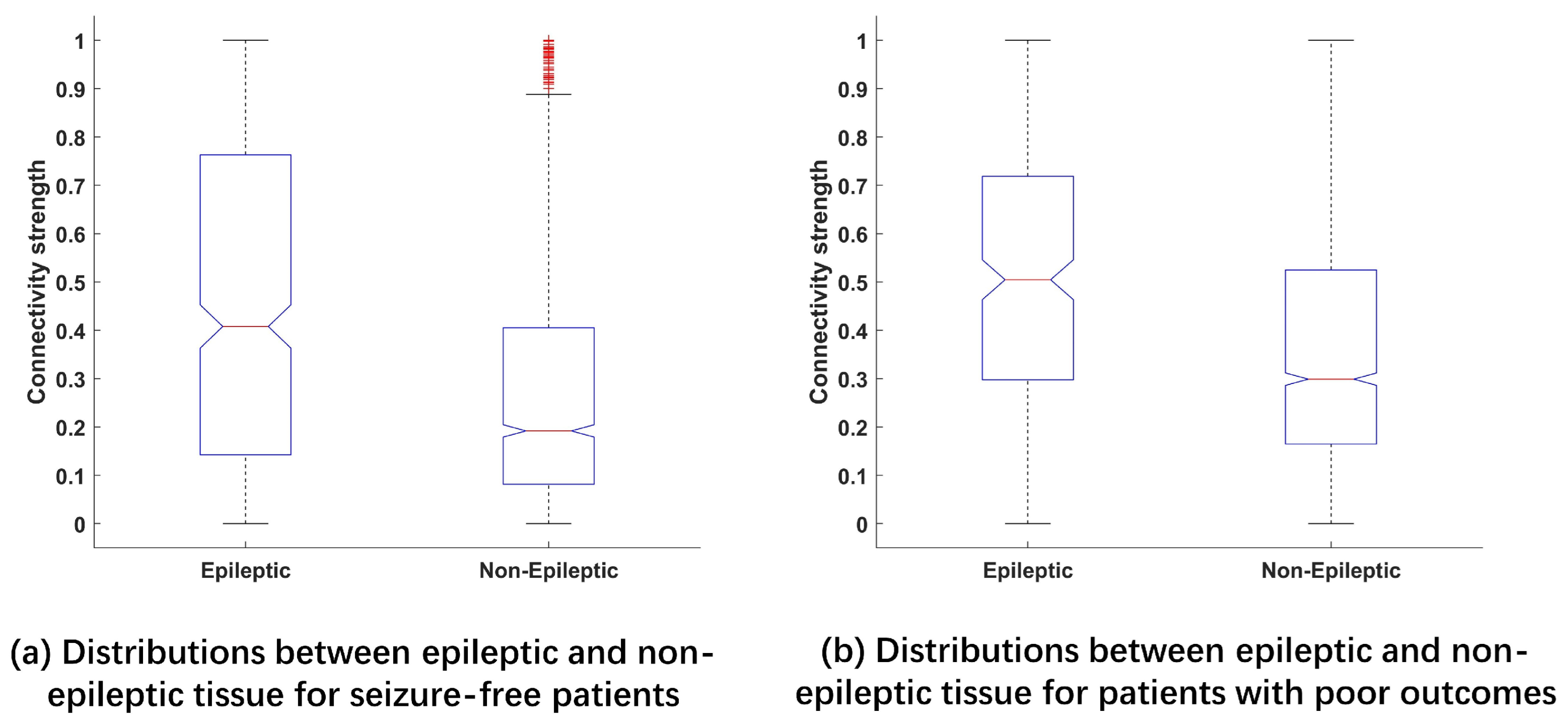
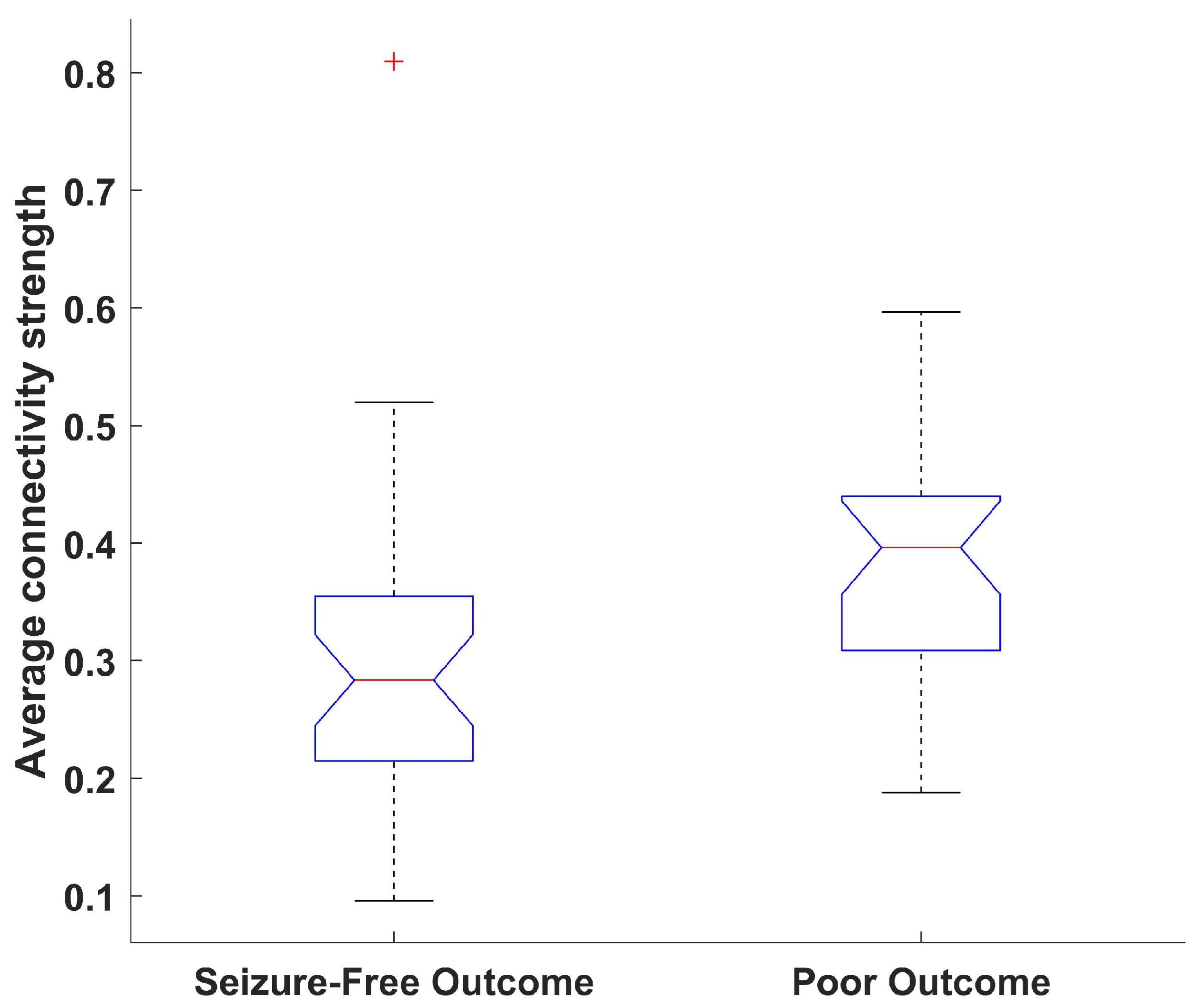
3.1. Connectivity Strengths between Epileptic and Normal Tissue
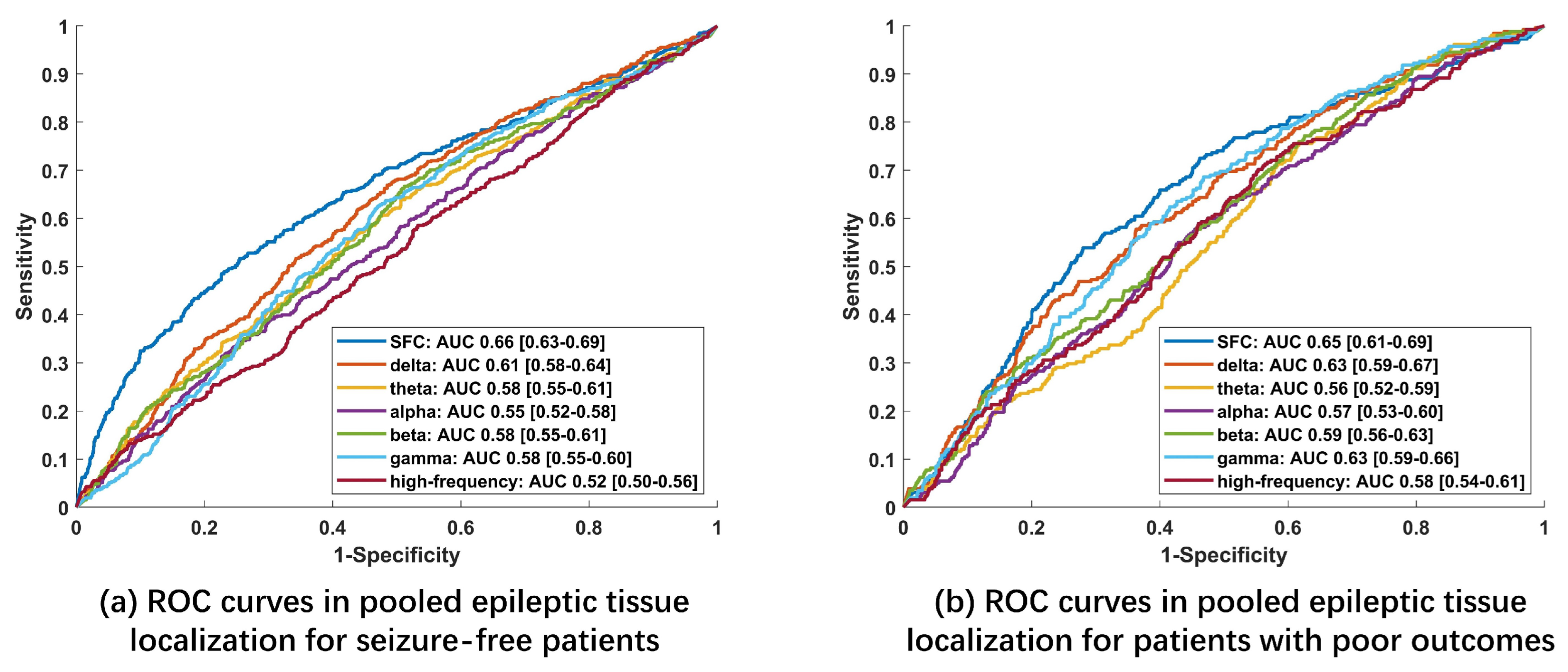
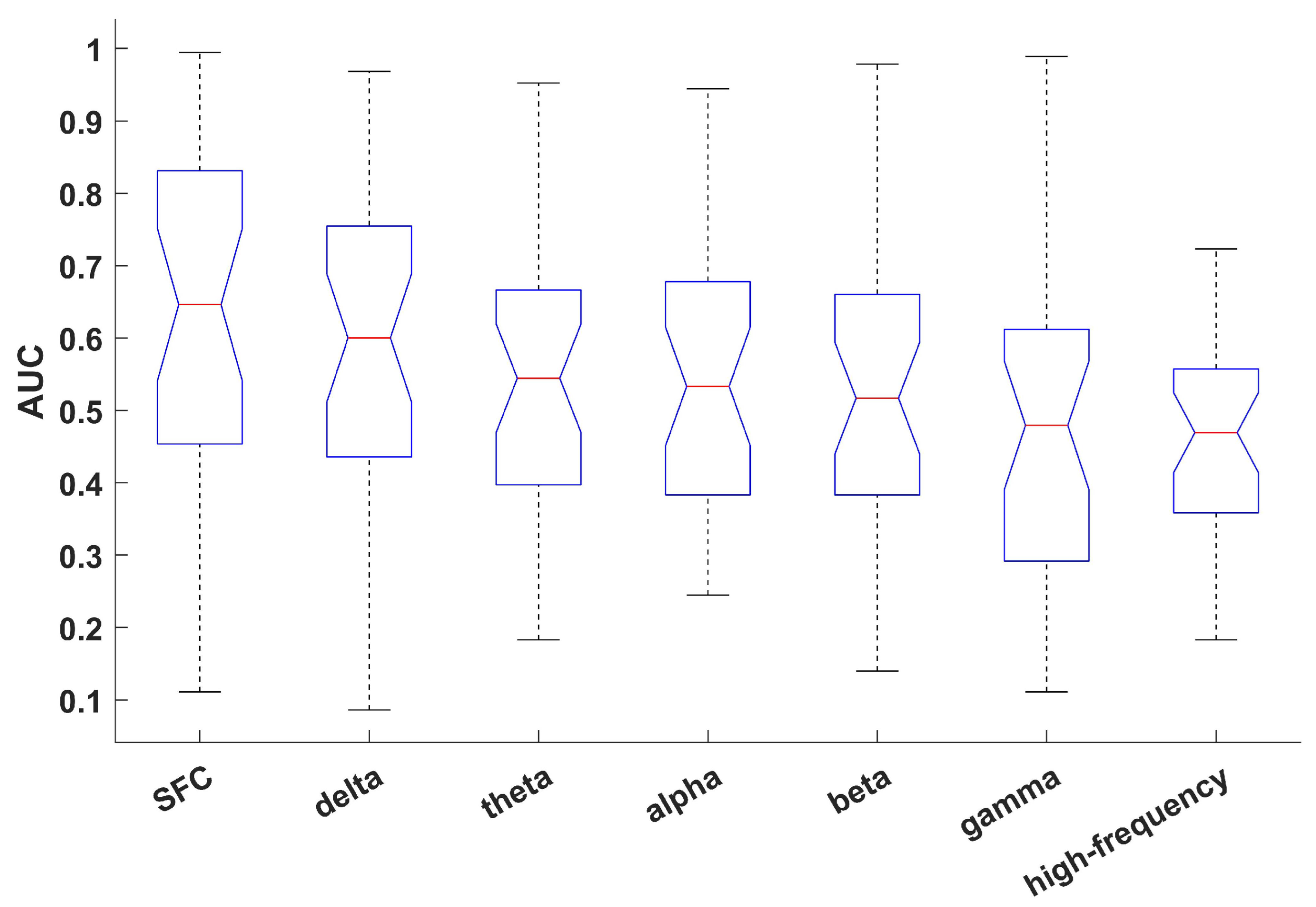
3.2. Pooled Epileptic Tissue Localization
3.3. Individual Epileptic Tissue Localization for Seizure-Free Patients
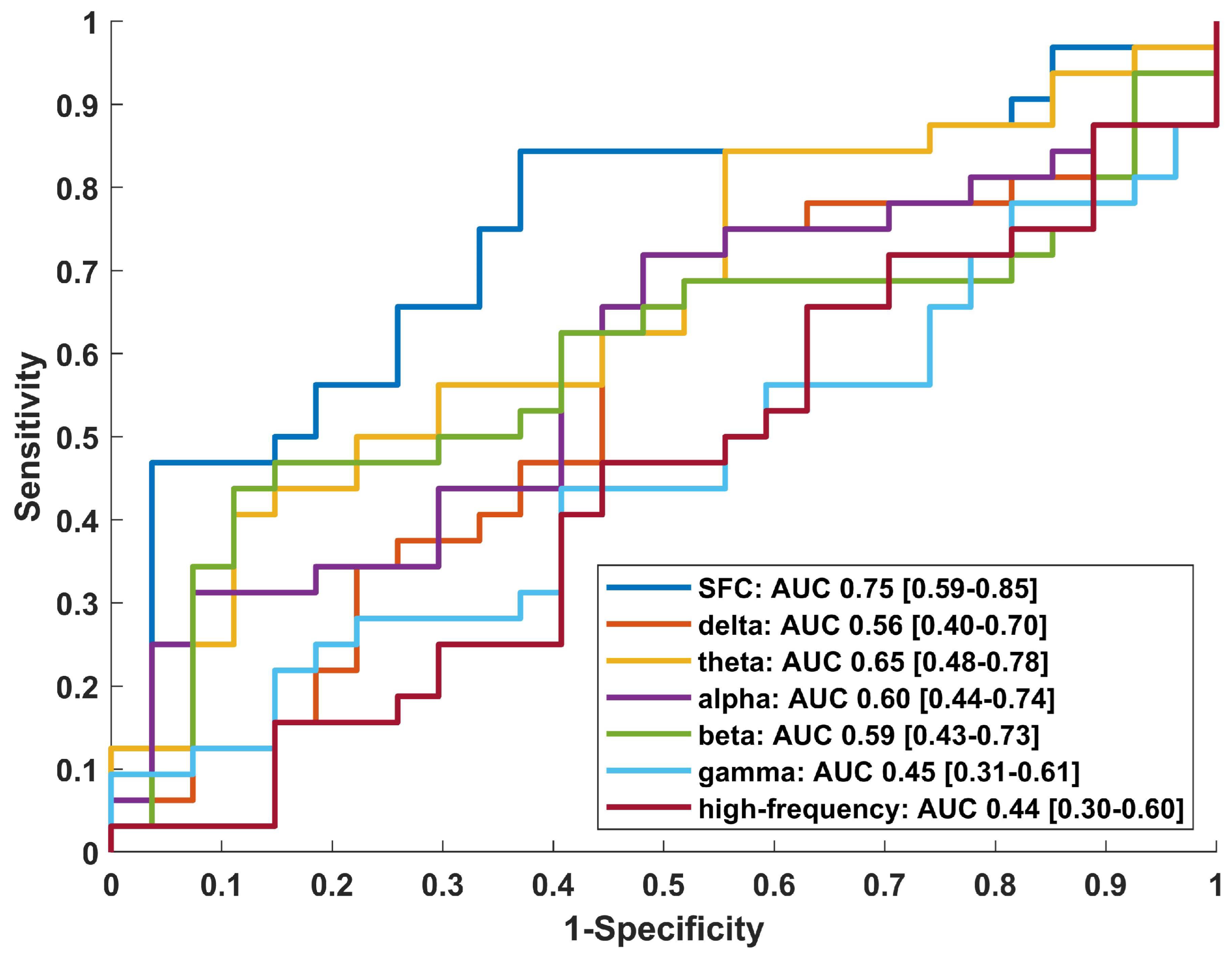
3.4. Surgical Outcome Evaluation
4. Discussion
4.1. Epileptic Tissue Localization Based on Connectivity in Different Frequency Bands
4.2. Comparison with Network Analysis Based on HFOs
4.3. Limitation and Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| iEEG | Intracranial electroencephalography |
| HFOs | High-frequency oscillations |
| HFA | High-frequency activity |
| SFC | Skewness-based functional connectivity |
| SOZ | Seizure onset zone |
| RZ | Resected zone |
| AUC | Area under the curve |
| CI | Confidence interval |
| FRs | Fast ripples |
| TLE | Temporal lobe epilepsy |
| ETLE | Extratemporal lobe epilepsy |
| ILAE | International League Against Epilepsy |
| ECoG | Electrocorticography |
| SEEG | Stereoelectroencephalography |
| ROC | Receiver operating characteristic |
| FPR | False-positive rate |
| IQR | Interquartile range |
References
- Thijs, R.D.; Surges, R.; O’Brien, T.J.; Sander, J.W. Epilepsy in adults. Lancet 2019, 393, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Kini, L.G.; Bernabei, J.M.; Mikhail, F.; Hadar, P.; Shah, P.; Khambhati, A.N.; Oechsel, K.; Archer, R.; Boccanfuso, J.; Conrad, E.; et al. Virtual resection predicts surgical outcome for drug-resistant epilepsy. Brain 2019, 142, 3892–3905. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.M.; Lee, A.T.; Kudo, K.; Ranasinghe, K.G.; Morise, H.; Findlay, A.M.; Kirsch, H.E.; Chang, E.F.; Nagarajan, S.S.; Rao, V.R. Network connectivity predicts effectiveness of responsive neurostimulation in focal epilepsy. Brain Commun. 2022, 4, fcac104t. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.A.; Pastore, T.; Orosz, I.; Rubinstein, D.; Gorniak, R.; Waldman, Z.; Fried, I.; Wu, C.; Sharan, A.; Slezak, D.; et al. Graph Theoretical Measures of Fast Ripples Support the Epileptic Network Hypothesis. Brain Commun. 2022, 4, fcac101. [Google Scholar] [CrossRef]
- Sindhu, K.R.; Staba, R.; Lopour, B.A. Trends in the use of automated algorithms for the detection of high-frequency oscillations associated with human epilepsy. Epilepsia 2020, 61, 1553–1569. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.; Wu, J.Y.; Perucca, P.; Zelmann, R.; Mader, M.; Dubeau, F.; Mathern, G.W.; Schulze-Bonhage, A.; Gotman, J. Removing high-frequency oscillations: A prospective multicenter study on seizure outcome. Neurology 2018, 91, e1040–e1052. [Google Scholar] [CrossRef]
- Minthe, A.; Janzarik, W.G.; Lachner-Piza, D.; Reinacher, P.; Schulze-Bonhage, A.; Dümpelmann, M.; Jacobs, J. Stable high frequency background EEG activity distinguishes epileptic from healthy brain regions. Brain Commun. 2020, 2, fcaa107. [Google Scholar] [CrossRef] [PubMed]
- Stovall, T.; Hunt, B.; Glynn, S.; Stacey, W.C.; Gliske, S.V. Interictal high frequency background activity as a biomarker of epileptogenic tissue. Brain Commun. 2021, 3, fcab188. [Google Scholar] [CrossRef] [PubMed]
- Mooij, A.H.; Frauscher, B.; Gotman, J.; Huiskamp, G.J. A skew-based method for identifying intracranial EEG channels with epileptic activity without detecting spikes, ripples, or fast ripples. Clin. Neurophysiol. 2020, 131, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Lagarde, S.; Roehri, N.; Lambert, I.; Trebuchon, A.; McGonigal, A.; Carron, R.; Scavarda, D.; Milh, M.; Pizzo, F.; Colombet, B.; et al. Interictal stereotactic-EEG functional connectivity in refractory focal epilepsies. Brain 2018, 141, 2966–2980. [Google Scholar] [CrossRef] [Green Version]
- Jiruska, P.; Alvarado-Rojas, C.; Schevon, C.A.; Staba, R.; Stacey, W.; Wendling, F.; Avoli, M. Update on the mechanisms and roles of high-frequency oscillations in seizures and epileptic disorders. Epilepsia 2017, 58, 1330–1339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guragain, H.; Cimbalnik, J.; Stead, M.; Groppe, D.M.; Berry, B.M.; Kremen, V.; Kenney-Jung, D.; Britton, J.; Worrell, G.A.; Brinkmann, B.H. Spatial variation in high-frequency oscillation rates and amplitudes in intracranial EEG. Neurology 2018, 90, e639–e646. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, S.B.; Porter, B.E.; Marsh, E.D. Interictal network synchrony and local heterogeneity predict epilepsy surgery outcome among pediatric patients. Epilepsia 2017, 58, 402–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zweiphenning, W.J.E.M.; Keijzer, H.M.; Diessen, E.; van’t Klooster, M.A.; Klink, N.E.C.; Leijten, F.S.S.; Rijen, P.C.; Putten, M.J.A.M.; Braun, K.P.J.; Zijlmans, M. Increased gamma and decreased fast ripple connections of epileptic tissue: A high-frequency directed network approach. Epilepsia 2019, 60, 1908–1920. [Google Scholar] [CrossRef] [Green Version]
- Zijlmans, M.; Worrell, G.A.; Dümpelmann, M.; Stieglitz, T.; Barborica, A.; Heers, M.; Ikeda, A.; Usui, N.; Quyen, M.L.V. How to record high-frequency oscillations in epilepsy: A practical guideline. Epilepsia 2017, 58, 1305–1315. [Google Scholar] [CrossRef] [Green Version]
- Gliske, S.V.; Irwin, Z.T.; Chestek, C.; Hegeman, G.L.; Brinkmann, B.; Sagher, O.; Garton, H.J.L.; Worrell, G.A.; Stacey, W.C. Variability in the location of high frequency oscillations during prolonged intracranial EEG recordings. Nat. Commun. 2018, 9, 2155. [Google Scholar] [CrossRef]
- Otárula, K.A.G.; von Ellenrieder, N.; Cuello-Oderiz, C.; Dubeau, F.; Gotman, J. High-Frequency Oscillation Networks and Surgical Outcome in Adult Focal Epilepsy. Ann. Neurol. 2019, 85, 485–494. [Google Scholar] [CrossRef]
- Tamilia, E.; Park, E.H.; Percivati, S.; Bolton, J.; Taffoni, F.; Peters, J.M.; Grant, P.E.; Pearl, P.L.; Madsen, J.R.; Papadelis, C. Surgical resection of ripple onset predicts outcome in pediatric epilepsy. Ann. Neurol. 2018, 84, 331–346. [Google Scholar] [CrossRef]
- Xiang, J.; Maue, E.; Fan, Y.; Qi, L.; Mangano, F.T.; Greiner, H.; Tenney, J. Kurtosis and skewness of high-frequency brain signals are altered in paediatric epilepsy. Brain Commun. 2020, 2, fcaa036. [Google Scholar] [CrossRef]
- Gliske, S.V.; Qin, Z.; Lau, K.; Alvarado-Rojas, C.; Salami, P.; Zelmann, R.; Stacey, W.C. Distinguishing false and true positive detections of high frequency oscillations. J. Neural Eng. 2020, 17, 056005. [Google Scholar] [CrossRef]
- Fedele, T.; Burnos, S.; Boran, E.; Krayenbühl, N.; Hilfiker, P.; Grunwald, T.; Sarnthein, J. Resection of high frequency oscillations predicts seizure outcome in the individual patient. Sci. Rep. 2017, 7, 13836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnarsdottir, K.; Li, A.; Smith, R.; Kang, J.; Korzeniewska, A.; Crone, N.; Rouse, A.; Cheng, J.; Kinsman, M.; Landazuri, P.; et al. Epilepsy-iEEG-Interictal-Multicenter-Dataset; Version 1.0.2; iEEG: Philadelphia, PA, USA, 2022. [Google Scholar] [CrossRef]
- Wieser, H.G.; Blume, W.T.; Fish, D.; Goldensohn, E.; Hufnagel, A.; King, D.; Sperling, M.R.; Lüders, H.; Pedley, T.A. Proposal for a New Classification of Outcome with Respect to Epileptic Seizures Following Epilepsy Surgery. Epilepsia 2008, 42, 282–286. [Google Scholar] [CrossRef]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.M. FieldTrip: Open Source Software for Advanced Analysis of MEG, EEG, and Invasive Electrophysiological Data. Comput. Intell. Neurosci. 2011, 2011, 156869. [Google Scholar] [CrossRef] [PubMed]
- Engel, J., Jr. Outcome with respect to epileptic seizures. In Surgical Treatment of the Epilepsies; Raven Press: New York, NY, USA, 1993; pp. 609–621. [Google Scholar]
- Zweiphenning, W.; van’t Klooster, M.; van Diessen, E.; van Klink, N.; Huiskamp, G.; Gebbink, T.; Leijten, F.; Gosselaar, P.; Otte, W.; Stam, C.; et al. High frequency oscillations and high frequency functional network characteristics in the intraoperative electrocorticogram in epilepsy. Neuroimage Clin. 2016, 12, 928–939. [Google Scholar] [CrossRef] [Green Version]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. NeuroImage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. 2007, 82, 591–605. [Google Scholar] [CrossRef]
- Shah, P.; Bernabei, J.M.; Kini, L.G.; Ashourvan, A.; Boccanfuso, J.; Archer, R.; Oechsel, K.; Das, S.R.; Stein, J.M.; Lucas, T.H.; et al. High interictal connectivity within the resection zone is associated with favorable post-surgical outcomes in focal epilepsy patients. Neuroimage Clin. 2019, 23, 101908. [Google Scholar] [CrossRef]
- Lundstrom, B.N.; Brinkmann, B.H.; Worrell, G.A. Low frequency novel interictal EEG biomarker for localizing seizures and predicting outcomes. Brain Commun. 2021, 3, fcab231. [Google Scholar] [CrossRef]
- Boly, M.; Jones, B.; Findlay, G.; Plumley, E.; Mensen, A.; Hermann, B.; Tononi, G.; Maganti, R. Altered sleep homeostasis correlates with cognitive impairment in patients with focal epilepsy. Brain 2017, 140, 1026–1040. [Google Scholar] [CrossRef] [Green Version]
- Ren, L.; Kucewicz, M.T.; Cimbalnik, J.; Matsumoto, J.Y.; Brinkmann, B.H.; Hu, W.; Marsh, W.R.; Meyer, F.B.; Stead, S.M.; Worrell, G.A. Gamma oscillations precede interictal epileptiform spikes in the seizure onset zone. Neurology 2015, 84, 602–608. [Google Scholar] [CrossRef] [Green Version]
- Burnos, S.; Frauscher, B.; Zelmann, R.; Haegelen, C.; Sarnthein, J.; Gotman, J. The morphology of high frequency oscillations (HFO) does not improve delineating the epileptogenic zone. Clin. Neurophysiol. 2016, 127, 2140–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Gender | Age | iEEG Type | Sample Rate | Engel Class | ILAE Class | Treatment | Location of Epileptic Tissue |
|---|---|---|---|---|---|---|---|---|
| P-1 | M | 25 | depth, strip | 2000 | N/A | 1 | resection | TLE |
| P-2 | M | 33 | depth | 2000 | N/A | 1 | resection | TLE |
| P-3 | F | 20 | depth | 2000 | N/A | 1 | resection | TLE |
| P-4 | F | 20 | depth | 2000 | N/A | 1 | resection | TLE |
| P-5 | M | 40 | depth | 2000 | N/A | 1 | resection | TLE |
| P-6 | M | 48 | depth | 2000 | N/A | 1 | resection | TLE |
| P-7 | M | 25 | depth | 2000 | N/A | 3 | resection | TLE |
| P-8 | F | 21 | depth | 2000 | N/A | 3 | resection | TLE |
| P-9 | M | 52 | depth | 2000 | N/A | 5 | resection | TLE |
| P-10 | M | 37 | strip, grid | 2000 | N/A | 1 | resection | ETLE |
| P-11 | M | 36 | depth, grid | 2000 | N/A | 1 | resection | ETLE |
| P-12 | M | 49 | depth, grid | 2000 | N/A | 1 | resection | ETLE |
| P-13 | M | 17 | depth, grid | 2000 | N/A | 1 | resection | ETLE |
| P-14 | F | 46 | depth, grid, strip | 2000 | N/A | 1 | resection | ETLE |
| P-15 | F | 31 | strip, grid | 2000 | N/A | 1 | resection | ETLE |
| P-16 | F | 17 | depth, grid | 2000 | N/A | 1 | resection | ETLE |
| P-17 | M | 30 | strip, grid | 2000 | N/A | 5 | resection | ETLE |
| P-18 | M | 40 | depth, strip | 2000 | N/A | 5 | resection | ETLE |
| P-19 | M | 38 | grid | 2000 | N/A | 6 | resection | ETLE |
| P-20 | M | 17 | grid | 2000 | N/A | 5 | resection | ETLE |
| Patient ID | Gender | Age | iEEG Type | Sample Rate | Engel Class | ILAE Class | Treatment | Location of Epileptic Tissue |
|---|---|---|---|---|---|---|---|---|
| NIH1 | F | 57 | SEEG | 1000 | 1 | 1 | resection | anterior temporal lobe |
| NIH2 | M | 31 | SEEG | 1000 | 1 | 1 | resection | right post hippocampus, temporal pole/anterior insula |
| NIH3 | F | 36 | SEEG | 1000 | 1 | 1 | resection | left temporal pole/mesial temporal |
| NIH4 | M | 39 | SEEG | 1000 | 1 | 1 | resection | right parietal |
| NIH5 | M | 41 | SEEG | 1000 | 1 | 1 | resection | right frontal |
| NIH6 | F | 20 | SEEG | 1000 | 3 | 3 | resection | left mesial temporal/amygdala |
| NIH7 | M | 46 | SEEG | 1000 | 3 | 4 | resection | bitemporal or orbitofrontal |
| NIH8 | M | 37 | SEEG | 1000 | 2 | 4 | resection | post hippocampus |
| NIH9 | F | 16 | SEEG | 1000 | 3 | 4 | resection | left frontal, parietal operculum, insula |
| NIH10 | M | 25 | SEEG | 1000 | 2 | 3 | resection | left insula |
| NIH11 | M | 27 | SEEG | 1000 | 2 | 3 | resection | left perirolandic |
| PY18N002 | M | 62 | SEEG | 1000 | 2 | 2 | resection | N/A |
| PY18N007 | F | 32 | SEEG | 1000 | 4 | 5 | MRgLiTT | N/A |
| PY18N013 | F | 24 | SEEG | 1000 | 1 | 1 | resection | N/A |
| PY18N015 | F | N/A | SEEG | 1000 | 1 | 1 | resection | N/A |
| PY19N012 | M | 48 | SEEG | 1000 | 2 | 3 | ablation | N/A |
| PY19N015 | F | 23 | SEEG | 1000 | 3 | 4 | RNS | N/A |
| PY19N023 | M | 32 | SEEG | 1000 | 1 | 1 | resection | N/A |
| PY19N026 | F | 35 | SEEG | 1000 | 1 | 1 | ablation | N/A |
| jh103 | N/A | N/A | ECoG | 1000 | 4 | 6 | resection | right anterior temporal lobe |
| jh105 | N/A | N/A | ECoG | 1000 | 1 | 1 | resection | right temporal lobe |
| pt1 | F | 30 | ECoG | 1000 | 1 | 2 | resection | right anterior temporal Lobe |
| pt2 | F | 28 | ECoG | 1000 | 1 | 1 | resection | left anterior temporal lobe |
| pt3 | M | 45 | ECoG | 1000 | 1 | 1 | resection | right frontal lobe |
| rns002 | F | 36 | SEEG | 2000 | 3 | N/A | RNS | N/A |
| rns003 | M | 21 | SEEG | 2000 | 3 | N/A | RNS | N/A |
| rns004 | M | 52 | SEEG | 500 | 4 | N/A | RNS | N/A |
| rns005 | M | 23 | SEEG | 2000 | 3 | N/A | RNS | N/A |
| rns006 | M | 49 | SEEG | 500 | 1 | N/A | RNS | N/A |
| rns009 | M | 48 | SEEG | 1024 | 3 | N/A | RNS | N/A |
| rns011 | F | 24 | SEEG | 2000 | 4 | N/A | RNS | N/A |
| rns013 | M | 25 | SEEG | 2000 | 2 | N/A | RNS | N/A |
| rns014 | M | 36 | SEEG | 2000 | 4 | N/A | RNS | N/A |
| rns015 | M | 27 | SEEG | 2000 | 2 | N/A | RNS | N/A |
| umf001 | F | 37 | ECoG | 1000 | 1 | 1 | resection | right anterior temporal lobe |
| umf002 | F | 39 | ECoG | 1000 | 2 | 1 | resection | right anterior temporal lobe |
| umf003 | M | 43 | ECoG | 1000 | 3 | 4 | resection | left temporal lobe |
| umf004 | F | 23 | SEEG | 1000 | 1 | 1 | resection | left anterior medial temporal lobe |
| umf005 | F | 32 | ECoG | 1000 | 1 | 1 | resection | right anterior temporal lobe |
| SFC | Delta | Theta | Alpha | Beta | Gamma | High-Frequency | |
|---|---|---|---|---|---|---|---|
| AUC 95% CI | 0.63 [0.56–0.71] | 0.59 [0.50–0.67] | 0.56 [0.48–0.63] | 0.54 [0.47–0.62] | 0.52 [0.44–0.60] | 0.47 [0.39–0.55] | 0.46 [0.41–0.51] |
| Cohen’s d | - | 0.17 | 0.27 | 0.31 | 0.42 | 0.65 | 0.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, M.; Zhang, L.; Gong, Y.; Li, L.; Liu, X. Epileptic Tissue Localization through Skewness-Based Functional Connectivity in the High-Frequency Band of Intracranial EEG. Bioengineering 2023, 10, 461. https://doi.org/10.3390/bioengineering10040461
Shen M, Zhang L, Gong Y, Li L, Liu X. Epileptic Tissue Localization through Skewness-Based Functional Connectivity in the High-Frequency Band of Intracranial EEG. Bioengineering. 2023; 10(4):461. https://doi.org/10.3390/bioengineering10040461
Chicago/Turabian StyleShen, Mu, Lin Zhang, Yi Gong, Lei Li, and Xianzeng Liu. 2023. "Epileptic Tissue Localization through Skewness-Based Functional Connectivity in the High-Frequency Band of Intracranial EEG" Bioengineering 10, no. 4: 461. https://doi.org/10.3390/bioengineering10040461
APA StyleShen, M., Zhang, L., Gong, Y., Li, L., & Liu, X. (2023). Epileptic Tissue Localization through Skewness-Based Functional Connectivity in the High-Frequency Band of Intracranial EEG. Bioengineering, 10(4), 461. https://doi.org/10.3390/bioengineering10040461