


Establishment of Surgical Difficulty Grading System and Application of MRI-Based Artificial Intelligence to Stratify Difficulty in Laparoscopic Rectal Surgery

 ,
, 
Abstract
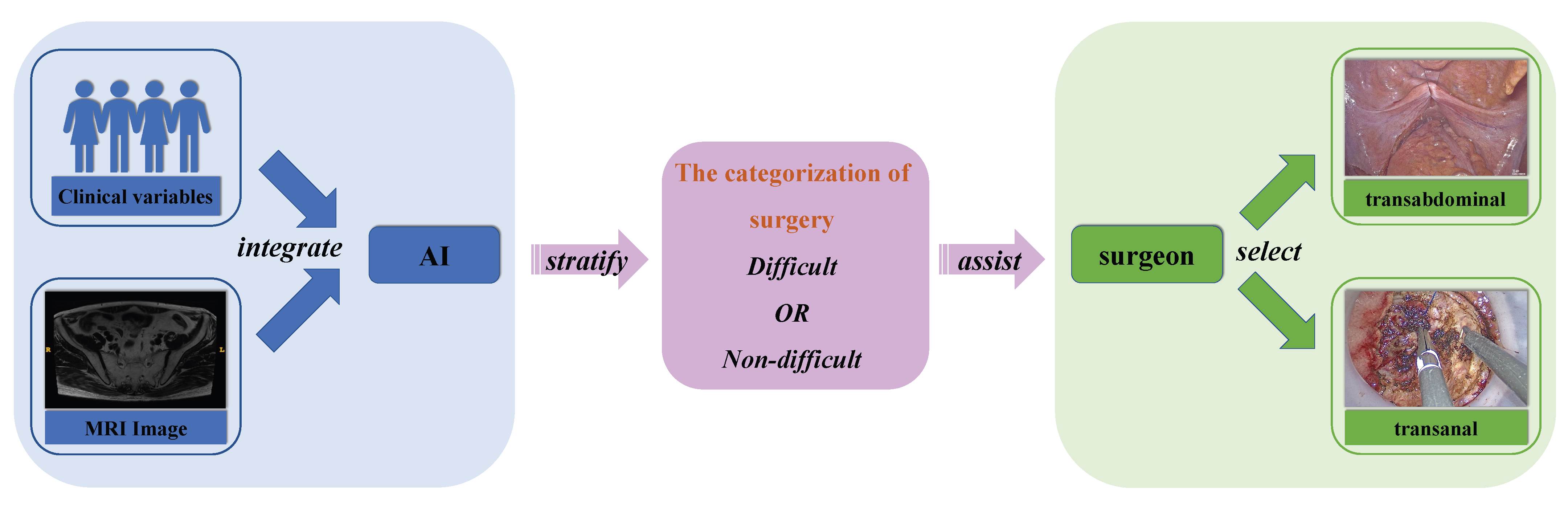
:1. Introduction
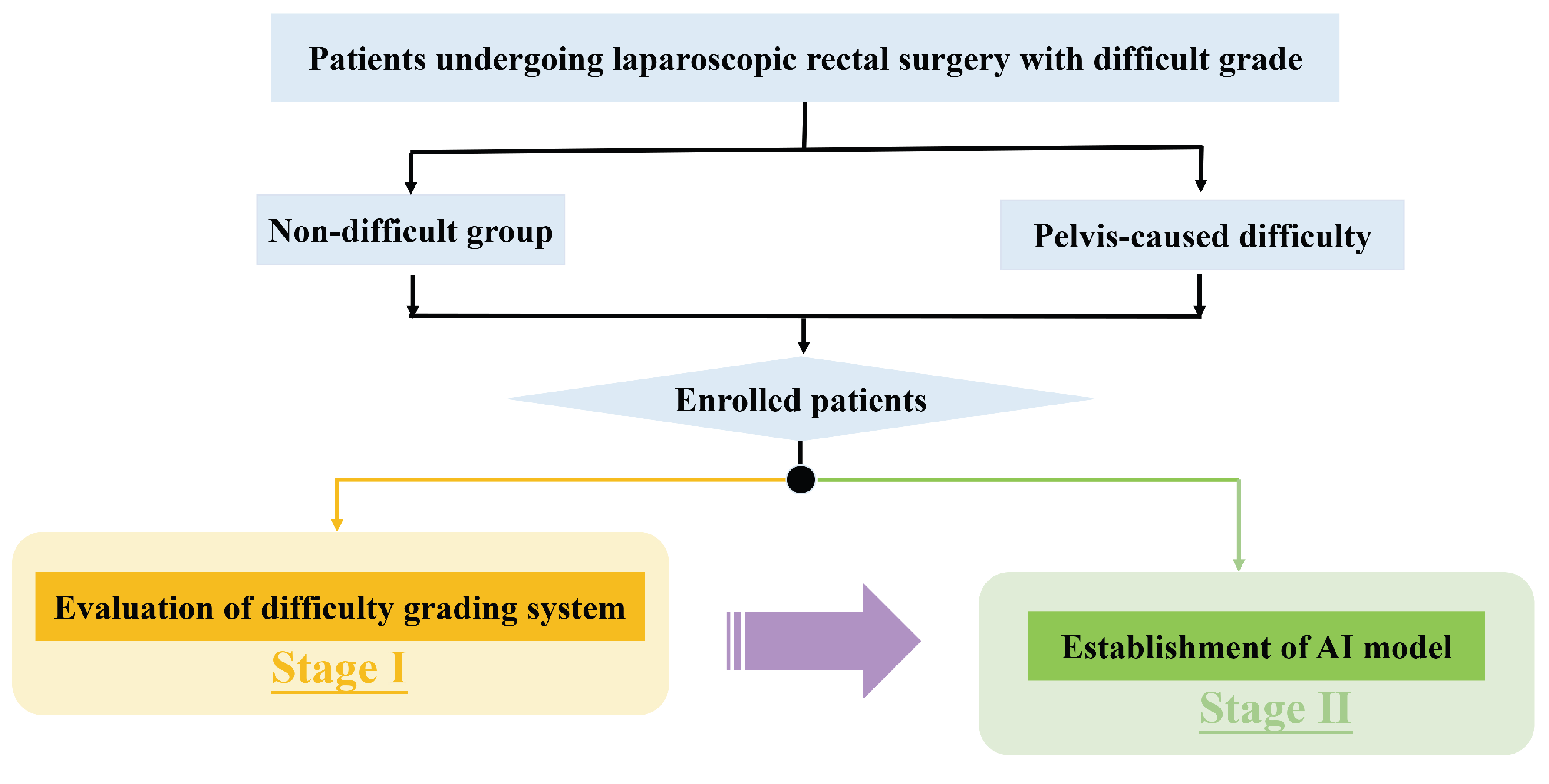
2. Materials and Methods
2.1. Patients
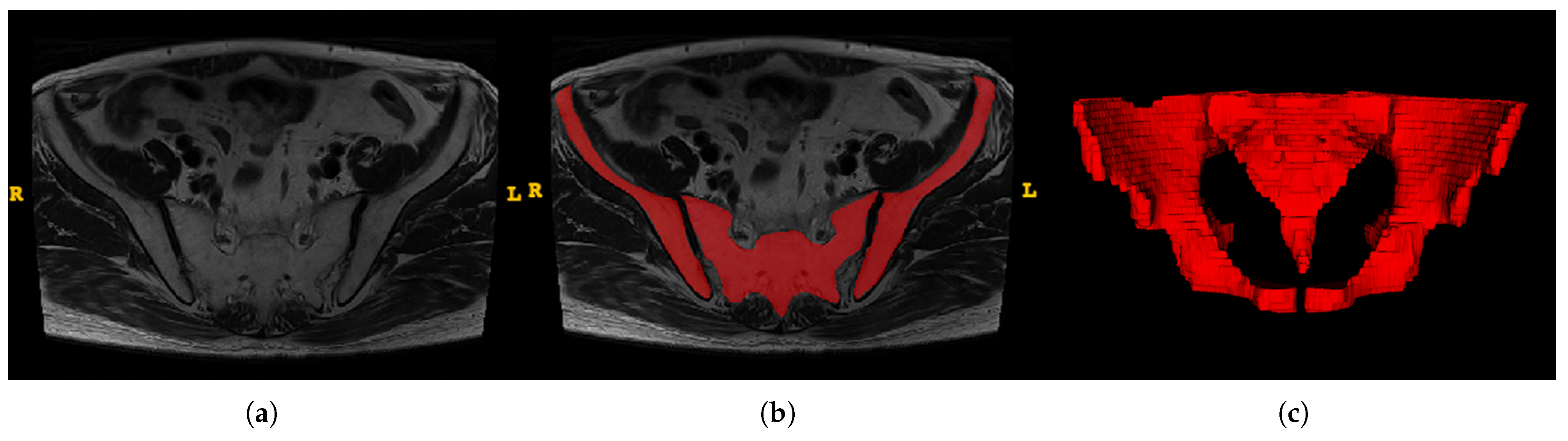
2.2. Image Preprocessing
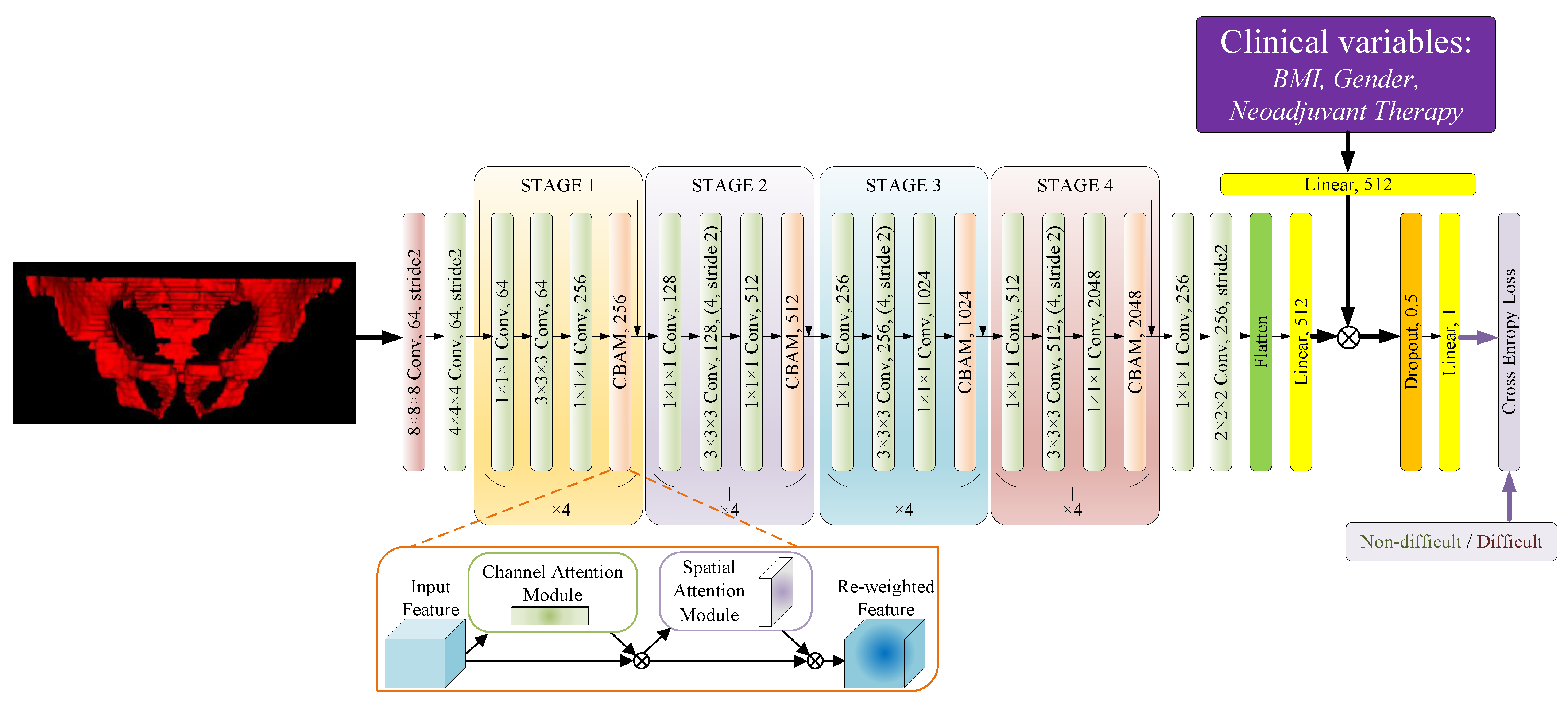
2.2.1. Network Architecture
2.2.2. Data Augmentation
2.2.3. Implementation and Metrics
2.3. Feature Extraction and Model Construction
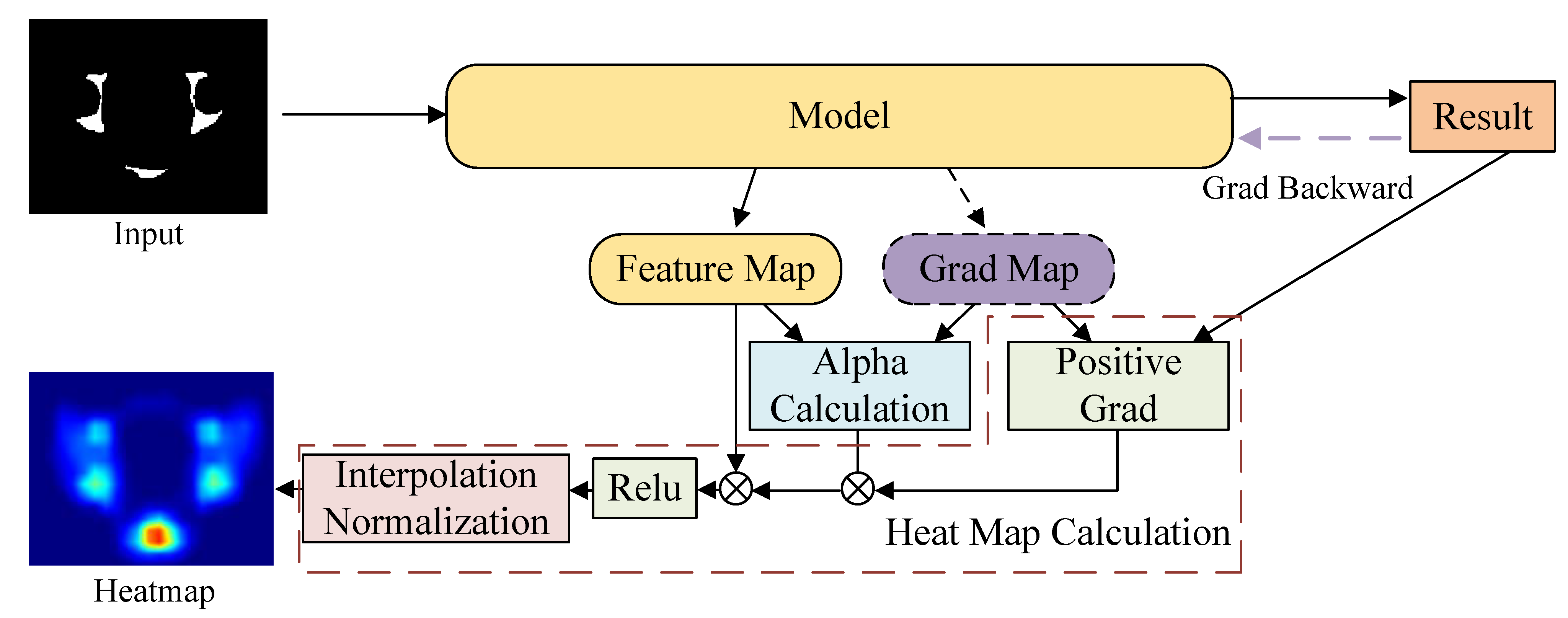
2.4. Visualization of the Attention Region
2.5. Statistics Analysis
3. Results
3.1. Grouped Patient Characteristics
3.2. Associations of Perioperative Outcomes with Surgical Difficulty (Stage I)
3.3. The Performance of Model (Stage II)
3.3.1. Cross Validation Study
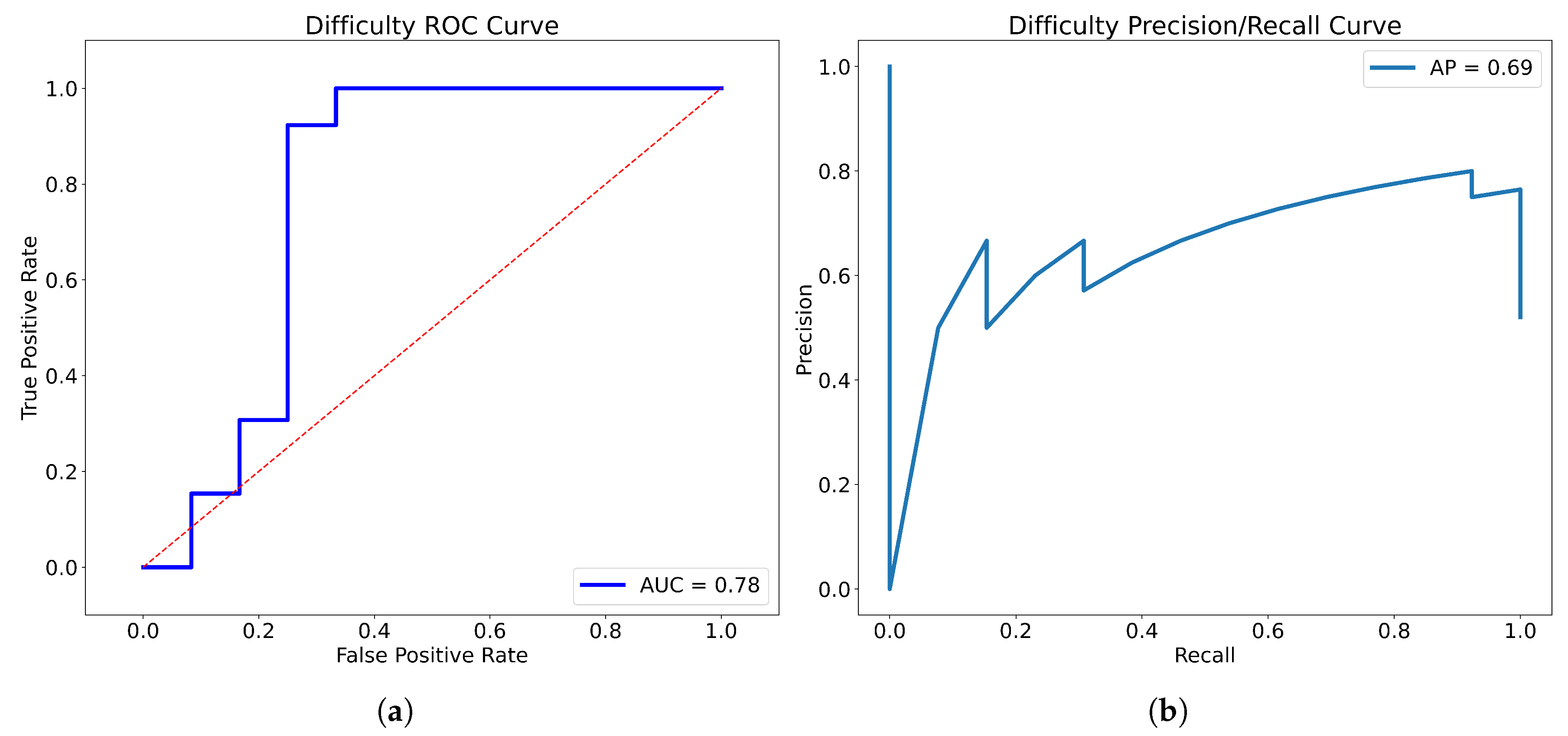
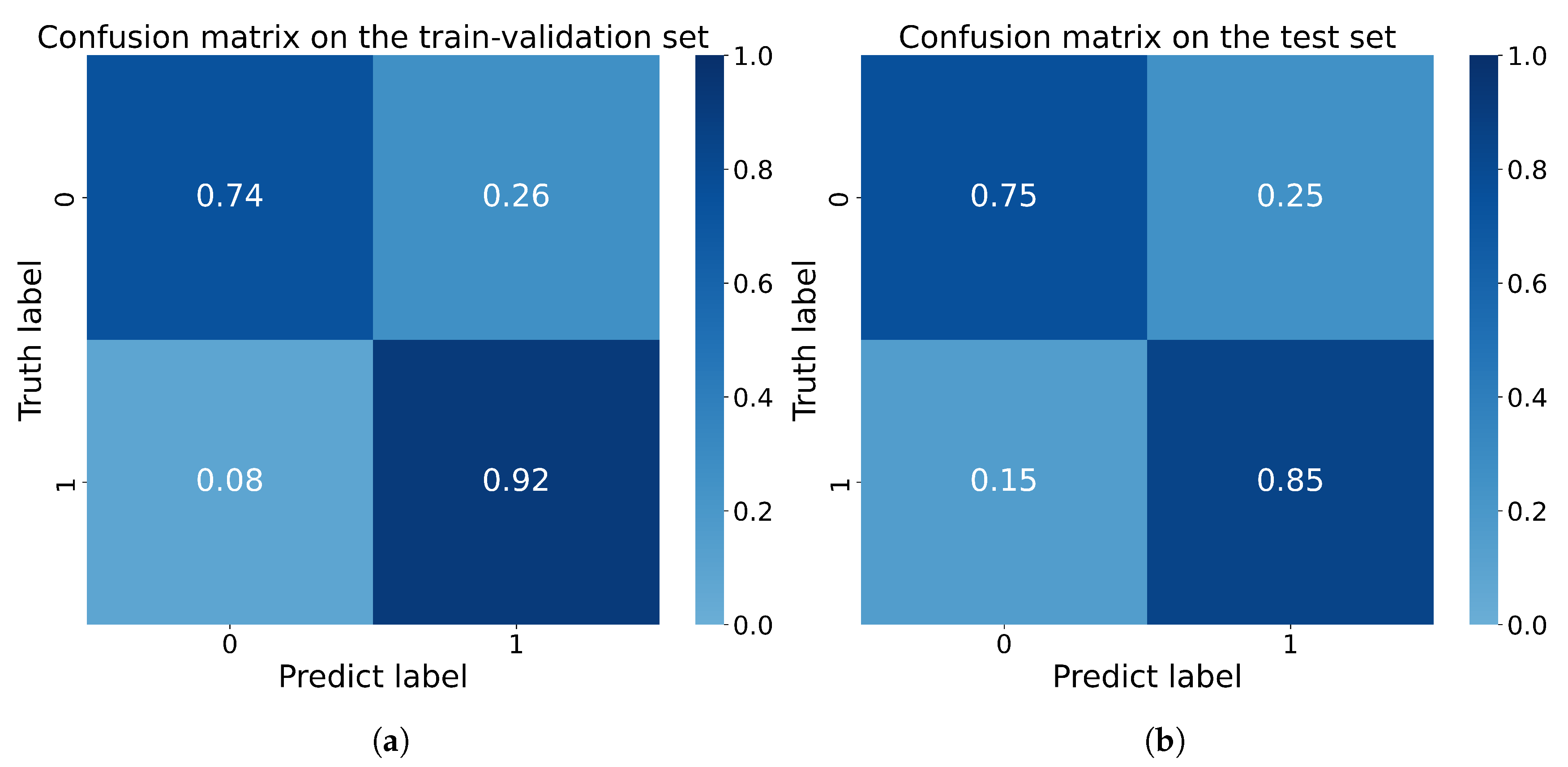
3.3.2. The Performance of the Merged Model
4. Discussion
5. Limitation
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Block Names | Output Size | Layers | |
|---|---|---|---|
| Conv1 | |||
| Conv2_x | |||
| Conv3_x | |||
| Conv4_x | |||
| Conv5_x | |||
| Classifier | (Batch size, 1) | , | Other Inputs Normalization (MinMax, Binary) |
| Flatten, Linear, →512 | Linear, 3→512, Sigmoid | ||
| Channel-wise Multiply | |||
| DropOut, 0.5, Linear, 512→1 | |||
References
- Igaki, T.; Kitaguchi, D.; Kojima, S.; Hasegawa, H.; Takeshita, N.; Mori, K.; Kinugasa, Y.; Ito, M. Artificial Intelligence-Based Total Mesorectal Excision Plane Navigation in Laparoscopic Colorectal Surgery. Dis. Colon. Rectum. 2022, 65, e329–e333. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.S.; Brown, K.G.M.; Waller, J.; Young, C.J.; Solomon, M.J. The role of MRI pelvimetry in predicting technical difficulty and outcomes of open and minimally invasive total mesorectal excision: A systematic review. Tech. Coloproctol. 2020, 24, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Wang, X.; Sun, Y.; Deng, Y.; Huang, Y.; Chi, P. A nomogram predicting the difficulty of laparoscopic surgery for rectal cancer. Surg. Today 2021, 51, 1835–1842. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, J.; Ye, C.; Lin, H.; Lu, X.; Huang, Y.; Chi, P. Pelvimetric and Nutritional Factors Predicting Surgical Difficulty in Laparoscopic Resection for Rectal Cancer Following Preoperative Chemoradiotherapy. World J. Surg. 2021, 45, 2261–2269. [Google Scholar] [CrossRef]
- Chen, J.; Sun, Y.; Chi, P.; Sun, B. MRI pelvimetry-based evaluation of surgical difficulty in laparoscopic total mesorectal excision after neoadjuvant chemoradiation for male rectal cancer. Surg. Today 2021, 51, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Han, Y.D.; Cho, M.S.; Hur, H.; Min, B.S.; Lee, K.Y.; Kim, N.K. Prediction of transabdominal total mesorectal excision difficulty according to the angle of pelvic floor muscle. Surg. Endosc. 2020, 34, 3043–3050. [Google Scholar] [CrossRef]
- Adamina, M.; Aigner, F.; Araujo, S.; Arezzo, A.; Ashamalla, S.; deBeche-Adams, T.; Bell, S.; Bemelman, W.; Brown, C.; Brunner, W. International expert consensus guidance on indications, implementation and quality measures for transanal total mesorectal excision. Color. Dis. 2020, 22, 749–755. [Google Scholar] [CrossRef]
- Baek, S.J.; Kim, C.H.; Cho, M.S.; Bae, S.U.; Hur, H.; Min, B.S.; Baik, S.H.; Lee, K.Y.; Kim, N.K. Robotic surgery for rectal cancer can overcome difficulties associated with pelvic anatomy. Surg. Endosc. 2015, 29, 1419–1424. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Li, X.T.; Shi, Y.J.; Lu, Q.Y.; Cao, W.; Zhang, H.M.; Wang, L.; Zhu, H.T.; Yu, T.; Guan, Z.; et al. Correlation Between the Distance to Mesorectal Fascia and Prognosis of cT3 Rectal Cancer: Results of a Multicenter Study From China. Dis. Colon. Rectum. 2022, 65, 322–332. [Google Scholar] [CrossRef]
- Collins, G.S.; Moons, K.G.M. Reporting of artificial intelligence prediction models. Lancet 2019, 393, 1577–1579. [Google Scholar] [CrossRef]
- Bedrikovetski, S.; Dudi-Venkata, N.N.; Kroon, H.M.; Seow, W.; Vather, R.; Carneiro, G.; Moore, J.W.; Sammour, T. Artificial intelligence for pre-operative lymph node staging in colorectal cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 1058. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Jiang, X.; Zhang, R.; Yu, T.; Liu, S.; Luo, Y. Radiomics signature as a new biomarker for preoperative prediction of neoadjuvant chemoradiotherapy response in locally advanced rectal cancer. Diagn. Interv. Radiol. 2021, 27, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Liu, Z.; Li, C.; Li, Z.; Lou, X.; Shao, L.; Wang, Y.; Huang, Y.; Chen, H.; Pang, X.; et al. Development and validation of a radiopathomics model to predict pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer: A multicentre observational study. Lancet Digit. Health 2022, 4, e8–e17. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.; Namazi, B.; Altieri, M.S.; Hashimoto, D.A.; Rivera, A.M.; Pucher, P.H.; Navarrete-Welton, A.; Sankaranarayanan, G.; Brunt, L.M.; Okrainec, A.; et al. Artificial Intelligence for Intraoperative Guidance: Using Semantic Segmentation to Identify Surgical Anatomy During Laparoscopic Cholecystectomy. Ann. Surg. 2022, 276, 363–369. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Cui, E.; Li, Z.; Ma, C.; Li, Q.; Lei, Y.; Lan, Y.; Yu, J.; Zhou, Z.; Li, R.; Long, W.; et al. Predicting the ISUP grade of clear cell renal cell carcinoma with multiparametric MR and multiphase CT radiomics. Eur. Radiol. 2020, 30, 2912–2921. [Google Scholar] [CrossRef] [PubMed]
- Yaniv, Z.; Lowekamp, B.C.; Johnson, H.J.; Beare, R. SimpleITK Image-Analysis Notebooks: A Collaborative Environment for Education and Reproducible Research. J. Digit. Imaging 2018, 31, 290–303. [Google Scholar] [CrossRef] [PubMed]
- Lowekamp, B.C.; Chen, D.T.; Ibanez, L.; Blezek, D. The Design of SimpleITK. Front. Neuroinform. 2013, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition, CVPR 2016, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Woo, S.; Park, J.; Lee, J.; Kweon, I.S. CBAM: Convolutional Block Attention Module. In Proceedings of the Computer Vision - ECCV 2018-15th European Conference, Munich, Germany, 8–14 September 2018; Springer: Berlin/Heidelberg, Germany, 2018; Volume 11211, pp. 3–19. [Google Scholar] [CrossRef]
- Cubuk, E.D.; Zoph, B.; Shlens, J.; Le, Q.V. Randaugment: Practical automated data augmentation with a reduced search space. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition, CVPR Workshops 2020, Seattle, WA, USA, 14–19 June 2020; pp. 3008–3017. [Google Scholar] [CrossRef]
- Zhou, B.; Khosla, A.; Lapedriza, À.; Oliva, A.; Torralba, A. Learning Deep Features for Discriminative Localization. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition, CVPR 2016, Las Vegas, NV, USA, 27–30 June 2016; pp. 2921–2929. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. In Proceedings of the IEEE International Conference on Computer Vision, ICCV 2017, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar] [CrossRef]
- Chattopadhay, A.; Sarkar, A.; Howlader, P.; Balasubramanian, V.N. Grad-CAM plus plus: Generalized Gradient-based Visual Explanations for Deep Convolutional Networks. In Proceedings of the 18th IEEE Winter Conference on Applications of Computer Vision (WACV), Lake Tahoe, NV, USA, 12–15 March 2018; IEEE: Piscataway, NJ, USA; pp. 839–847. [Google Scholar] [CrossRef]
- Thirion, J.P. Image matching as a diffusion process: An analogy with Maxwell’s demons. Med. Image Anal. 1998, 2, 243–260. [Google Scholar] [CrossRef]
- Pacal, I.; Karaboga, D.; Basturk, A.; Akay, B.; Nalbantoglu, U. A comprehensive review of deep learning in colon cancer. Comput. Biol. Med. 2020, 126, 104003. [Google Scholar] [CrossRef]
- Manwaring, M.L.; Ko, C.Y.; Fleshman, J.W.J., Jr.; Beck, D.E.; Schoetz, D.J., Jr.; Senagore, A.J.; Ricciardi, R.; Temple, L.K.; Morris, A.M.; Delaney, C.P. Identification of consensus-based quality end points for colorectal surgery. Dis. Colon. Rectum. 2012, 55, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Remue, C.; Abbes Orabi, N.; van Maanen, A.; Danse, E.; Dragean, A.; Debetancourt, D.; Humblet, Y.; Jouret-Mourin, A.; Maddalena, F.; et al. Lymph node ratio and surgical quality are strong prognostic factors of rectal cancer: Results from a single referral centre. Color. Dis. 2016, 18, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Cheng, J.; Bao, Y.; Gao, Z.; Jiang, K.; Wang, S.; Ye, Y.; Wang, Y.; Shen, Z. Magnetic resonance imaging pelvimetry predicts the technical difficulty of rectal surgery. Asian J. Surg. 2022, 45, 2626–2632. [Google Scholar] [CrossRef]
- Escal, L.; Nougaret, S.; Guiu, B.; Bertrand, M.M.; de Forges, H.; Tetreau, R.; Thezenas, S.; Rouanet, P. MRI-based score to predict surgical difficulty in patients with rectal cancer. Br. J. Surg. 2018, 105, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Killeen, T.; Banerjee, S.; Vijay, V.; Al-Dabbagh, Z.; Francis, D.; Warren, S. Magnetic resonance (MR) pelvimetry as a predictor of difficulty in laparoscopic operations for rectal cancer. Surg. Endosc. 2010, 24, 2974–2979. [Google Scholar] [CrossRef]
- Shimada, T.; Tsuruta, M.; Hasegawa, H.; Okabayashi, K.; Ishida, T.; Asada, Y.; Suzumura, H.; Kitagawa, Y. Pelvic inlet shape measured by three-dimensional pelvimetry is a predictor of the operative time in the anterior resection of rectal cancer. Surg. Today 2018, 48, 51–57. [Google Scholar] [CrossRef]
- Yamaoka, Y.; Yamaguchi, T.; Kinugasa, Y.; Shiomi, A.; Kagawa, H.; Yamakawa, Y.; Furutani, A.; Manabe, S.; Torii, K.; Koido, K.; et al. Mesorectal fat area as a useful predictor of the difficulty of robotic-assisted laparoscopic total mesorectal excision for rectal cancer. Surg. Endosc. 2019, 33, 557–566. [Google Scholar] [CrossRef]
- Iqbal, A.; Khan, A.; George, T.J.; Tan, S.; Qiu, P.; Yang, K.; Trevino, J.; Hughes, S. Objective Preoperative Parameters Predict Difficult Pelvic Dissections and Clinical Outcomes. J. Surg. Res. 2018, 232, 15–25. [Google Scholar] [CrossRef]
- Ferko, A.; Maly, O.; Orhalmi, J.; Dolejs, J. CT/MRI pelvimetry as a useful tool when selecting patients with rectal cancer for transanal total mesorectal excision. Surg. Endosc. 2016, 30, 1164–1171. [Google Scholar] [CrossRef]
- Jootun, N.; Sengupta, S.; Cunningham, C.; Charlton, P.; Betts, M.; Weaver, A.; Jacobs, C.; Hompes, R.; Muirhead, R. Neoadjuvant radiotherapy in rectal cancer - less is more? Color. Dis. 2020, 22, 261–268. [Google Scholar] [CrossRef]
- Glastonbury, C.M.; Parker, E.E.; Hoang, J.K. The postradiation neck: Evaluating response to treatment and recognizing complications. AJR Am. J. Roentgenol. 2010, 195, W164–W171. [Google Scholar] [CrossRef] [PubMed]
- Bandini, M.; Fossati, N.; Briganti, A. Nomograms in urologic oncology, advantages and disadvantages. Curr. Opin. Urol. 2019, 29, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Xu, J.; Zhang, Z.; Li, S.; Zhang, X.; Zhou, Y.; Zhang, X.; Lu, Y. Evaluation of Rectal Cancer Circumferential Resection Margin Using Faster Region-Based Convolutional Neural Network in High-Resolution Magnetic Resonance Images. Dis. Colon. Rectum. 2020, 63, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Yu, Q.; Gao, Y.; Zhou, Y.; Liu, G.; Dong, Q.; Ma, J.; Ding, L.; Yao, H.; Zhang, Z.; et al. Identification of Metastatic Lymph Nodes in MR Imaging with Faster Region-Based Convolutional Neural Networks. Cancer Res. 2018, 78, 5135–5143. [Google Scholar] [CrossRef]
- Yuan, Z.; Xu, T.; Cai, J.; Zhao, Y.; Cao, W.; Fichera, A.; Liu, X.; Yao, J.; Wang, H. Development and Validation of an Image-based Deep Learning Algorithm for Detection of Synchronous Peritoneal Carcinomatosis in Colorectal Cancer. Ann. Surg. 2022, 275, e645–e651. [Google Scholar] [CrossRef]









| Grade | Definition |
|---|---|
| I | Easy procedure, without difficulty |
| II | Difficult procedure, but no impact on specimen quality (complete TME) |
| III | Difficult procedure, with slight impact on specimen quality (near-complete TME) |
| IV | Very difficult procedure, with severe impact on specimen quality (incomplete TME) |
| Variable | Enrolled Patients(n = 108) | Difficult Group (n = 53) | Non-Difficult Group (n = 55) |
|---|---|---|---|
| Age, years, [median (IQR)] | 64 (56–70) | 66 (58–70) | 63 (53–69) |
| Male, n (%) | 73 (67.6) | 51 (96.2) | 22 (40.0) |
| BMI, kg/m , [mean (SD)] | 24.1 (3.4) | 25.0 (3.4) | 23.2 (3.1) |
| Neoadjuvant chemoradiotherapy, n (%) | 77 (71.3) | 45 (84.9) | 32 (58.2) |
| Previous abdominal surgery, n (%) | 13 (12.0) | 5 (9.4) | 8 (14.5) |
| Distance from tumor to anal verge, cm [mean (SD)] | 6.5 (2.0) | 6.3 (2.0) | 6.7 (2.0) |
| Tumor size, cm [median (IQR)] | 2.0 (1.3–3.1) | 2.0 (1.2–3.1) | 2.0 (1.3–3.1) |
| Surgery type | |||
| LAR, n (%) | 79 (73.1) | 35 (66.0) | 44 (85.5) |
| taTME, n (%) | 18 (16.7) | 12 (22.6) | 6 (10.9) |
| ISR, n (%) | 5 (4.6) | 1 (1.9) | 4 (7.3) |
| Others, n (%) | 6 (5.6) | 5 (9.4) | 1 (1.8) |
| Variable | Surgical Difficulty | p Value | |
|---|---|---|---|
| Difficult Group (n = 48) | Non-Difficult Group (n = 54) | ||
| Male, n (%) | 46 (95.8) | 21 (38.9) | <0.001 |
| BMI, kg/m , [mean (SD)] | 25.2 (3.3) | 23.2 (3.1) | 0.002 |
| Neoadjuvant chemoradiotherapy | 41 (85.4) | 32 (59.3) | 0.003 |
| Previous abdominal surgery | 4 (8.3) | 7 (13.0) | 0.452 |
| Distance from tumor to anal verge, cm [mean (SD)] | 6.5 (1.8) | 6.7 (2.0) | 0.437 |
| Tumor size, cm [median (IQR)] | 1.7 (1.2–3.0) | 2.0 (1.3–3.0) | 0.526 * |
| Duration of surgery, min [median (IQR)] | 145.0 (120.0–160.0) | 118.5 (100.0–141.3) | 0.001* |
| Blood loss, mL [median (IQR)] | 25 (20–50) | 20 (10–40) | 0.004 * |
| Diverting stoma, n (%) | 43 (89.6) | 37 (68.5) | 0.010 |
| Complete TME, n (%) | 31 (64.6) | 54 (100) | <0.001 |
| Lymph nodes harvested, n [median (IQR)] | 12 (8–17) | 13 (10–17) | 0.665 * |
| Postoperative complications, n (%) | 17 (35.4) | 19 (35.2) | 0.981 |
| Anastomotic leak, n (%) | 8 (16.7) | 2 (3.7) | 0.043 |
| Postoperative hospital stays, days [median (IQR)] | 7 (6–7) | 6 (6–8) | 0.478 * |
| Fold | Accuracy | Precision | Specificity | Recall | F1 Score |
|---|---|---|---|---|---|
| 1 | 0.850 | 0.889 | 0.900 | 0.800 | 0.842 |
| 2 | 0.750 | 0.692 | 0.600 | 0.900 | 0.782 |
| 3 | 0.850 | 0.818 | 0.800 | 0.900 | 0.857 |
| 4 | 0.850 | 0.818 | 0.800 | 0.900 | 0.857 |
| Average | 0.825 | 0.804 | 0.775 | 0.875 | 0.835 |
| Fold | Accuracy | Precision | Specificity | Recall | F1 Score |
|---|---|---|---|---|---|
| 1 | 0.840 | 0.800 | 0.750 | 0.923 | 0.857 |
| 2 | 0.880 | 0.813 | 0.750 | 1.000 | 0.897 |
| 3 | 0.800 | 0.786 | 0.750 | 0.846 | 0.815 |
| 4 | 0.800 | 0.786 | 0.750 | 0.846 | 0.815 |
| Average | 0.830 | 0.796 | 0.750 | 0.904 | 0.846 |
| Merged | 0.800 | 0.786 | 0.750 | 0.846 | 0.815 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Z.; Hou, W.; Liu, W.; Liu, J.; Li, K.; Wu, B.; Lin, G.; Xue, H.; Pan, J.; Xiao, Y. Establishment of Surgical Difficulty Grading System and Application of MRI-Based Artificial Intelligence to Stratify Difficulty in Laparoscopic Rectal Surgery. Bioengineering 2023, 10, 468. https://doi.org/10.3390/bioengineering10040468
Sun Z, Hou W, Liu W, Liu J, Li K, Wu B, Lin G, Xue H, Pan J, Xiao Y. Establishment of Surgical Difficulty Grading System and Application of MRI-Based Artificial Intelligence to Stratify Difficulty in Laparoscopic Rectal Surgery. Bioengineering. 2023; 10(4):468. https://doi.org/10.3390/bioengineering10040468
Chicago/Turabian StyleSun, Zhen, Wenyun Hou, Weimin Liu, Jingjuan Liu, Kexuan Li, Bin Wu, Guole Lin, Huadan Xue, Junjun Pan, and Yi Xiao. 2023. "Establishment of Surgical Difficulty Grading System and Application of MRI-Based Artificial Intelligence to Stratify Difficulty in Laparoscopic Rectal Surgery" Bioengineering 10, no. 4: 468. https://doi.org/10.3390/bioengineering10040468
APA StyleSun, Z., Hou, W., Liu, W., Liu, J., Li, K., Wu, B., Lin, G., Xue, H., Pan, J., & Xiao, Y. (2023). Establishment of Surgical Difficulty Grading System and Application of MRI-Based Artificial Intelligence to Stratify Difficulty in Laparoscopic Rectal Surgery. Bioengineering, 10(4), 468. https://doi.org/10.3390/bioengineering10040468