


Blood Glucose Level Time Series Forecasting: Nested Deep Ensemble Learning Lag Fusion


Abstract
:1. Introduction
2. Literature Survey
3. Material
4. Methods
4.1. Data Curation
4.1.1. Missingness Treatment
4.1.2. Sparsity Handling
4.1.3. Data Alignment
4.1.4. Data Transformation
4.1.5. Stationarity Inspection
4.1.6. Problem Reframing
4.2. Modelling
4.2.1. Preliminary
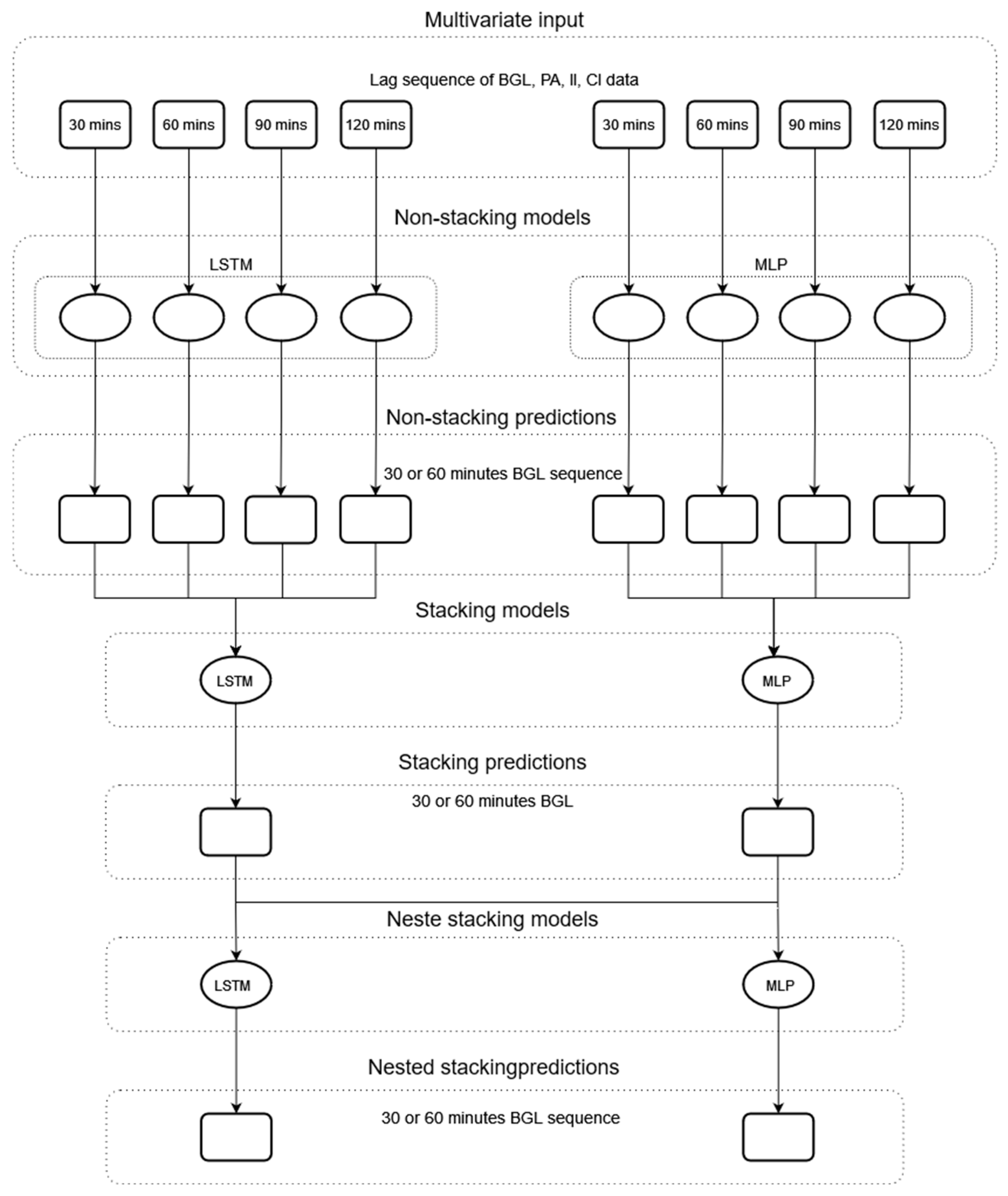
4.2.2. Model Development
4.3. Model Assessment
4.3.1. Regression Evaluation
4.3.2. Clinical Evaluation
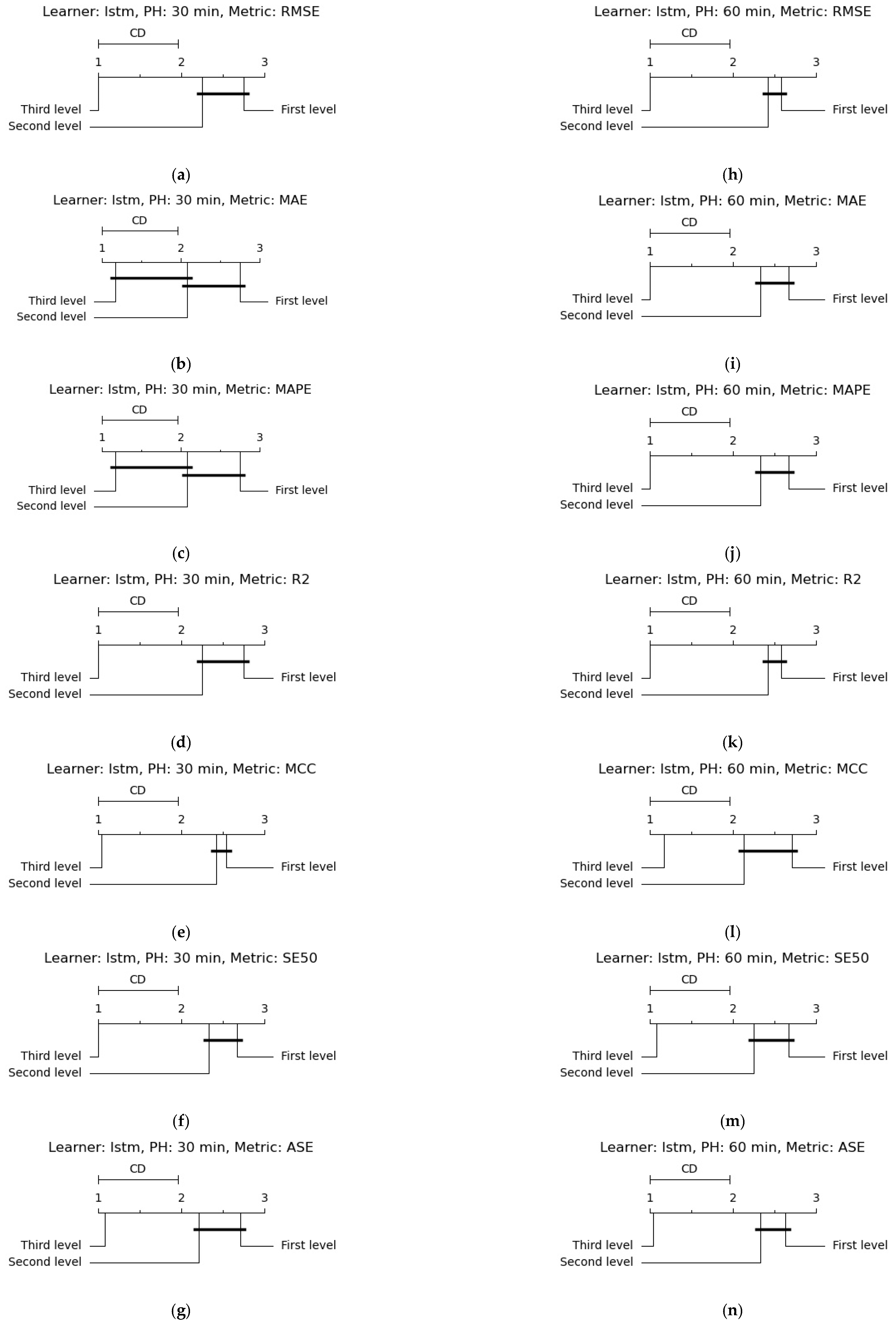
4.3.3. Statistical Analysis
5. Results and Discussion
6. Summary and Conclusions
7. Software and Code
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| PID | PH | LL | Evaluation metric | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | |||
| 559 | 30 | 30 | 19.96 ± 0.09 | 13.78 ± 0.11 | 8.83 ± 0.11 | 90.45 ± 0.08 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 |
| 60 | 19.65 ± 0.06 | 13.56 ± 0.03 | 8.78 ± 0.03 | 90.75 ± 0.05 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 | ||
| 90 | 19.85 ± 0.01 | 13.73 ± 0.02 | 8.81 ± 0.04 | 90.56 ± 0.01 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 | ||
| 120 | 19.88 ± 0.07 | 13.83 ± 0.05 | 8.81 ± 0.04 | 90.53 ± 0.07 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 30 | 33.73 ± 0.04 | 24.46 ± 0.04 | 16.49 ± 0.05 | 72.59 ± 0.06 | 0.58 ± 0.00 | 0.77 ± 0.00 | 0.33 ± 0.00 | |
| 60 | 32.04 ± 0.05 | 23.12 ± 0.09 | 15.43 ± 0.11 | 75.26 ± 0.08 | 0.62 ± 0.01 | 0.79 ± 0.00 | 0.31 ± 0.00 | ||
| 90 | 31.67 ± 0.05 | 22.84 ± 0.06 | 15.23 ± 0.04 | 75.82 ± 0.08 | 0.64 ± 0.00 | 0.79 ± 0.00 | 0.31 ± 0.00 | ||
| 120 | 31.36 ± 0.06 | 22.78 ± 0.06 | 15.18 ± 0.07 | 76.30 ± 0.08 | 0.63 ± 0.00 | 0.79 ± 0.00 | 0.31 ± 0.00 | ||
| 563 | 30 | 30 | 18.71 ± 0.05 | 13.46 ± 0.06 | 8.47 ± 0.04 | 82.97 ± 0.09 | 0.74 ± 0.00 | 0.91 ± 0.00 | 0.19 ± 0.00 |
| 60 | 18.89 ± 0.03 | 13.33 ± 0.03 | 8.30 ± 0.02 | 82.65 ± 0.05 | 0.74 ± 0.00 | 0.91 ± 0.00 | 0.19 ± 0.00 | ||
| 90 | 19.09 ± 0.03 | 13.42 ± 0.03 | 8.34 ± 0.02 | 82.27 ± 0.06 | 0.74 ± 0.01 | 0.91 ± 0.00 | 0.19 ± 0.00 | ||
| 120 | 19.29 ± 0.01 | 13.61 ± 0.00 | 8.45 ± 0.00 | 81.91 ± 0.02 | 0.73 ± 0.01 | 0.91 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 30 | 30.44 ± 0.08 | 22.46 ± 0.08 | 14.40 ± 0.06 | 55.00 ± 0.23 | 0.49 ± 0.00 | 0.78 ± 0.00 | 0.33 ± 0.00 | |
| 60 | 30.43 ± 0.05 | 21.75 ± 0.02 | 13.57 ± 0.02 | 55.02 ± 0.14 | 0.56 ± 0.01 | 0.80 ± 0.00 | 0.30 ± 0.00 | ||
| 90 | 30.65 ± 0.01 | 21.69 ± 0.04 | 13.46 ± 0.04 | 54.36 ± 0.04 | 0.57 ± 0.01 | 0.81 ± 0.00 | 0.30 ± 0.00 | ||
| 120 | 30.68 ± 0.15 | 21.72 ± 0.09 | 13.47 ± 0.05 | 54.28 ± 0.44 | 0.57 ± 0.00 | 0.81 ± 0.00 | 0.30 ± 0.00 | ||
| 570 | 30 | 30 | 18.24 ± 0.19 | 13.27 ± 0.15 | 6.74 ± 0.08 | 92.71 ± 0.15 | 0.84 ± 0.00 | 0.95 ± 0.00 | 0.13 ± 0.00 |
| 60 | 17.44 ± 0.03 | 12.47 ± 0.03 | 6.38 ± 0.03 | 93.34 ± 0.03 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | ||
| 90 | 17.58 ± 0.03 | 12.54 ± 0.03 | 6.45 ± 0.01 | 93.24 ± 0.03 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | ||
| 120 | 17.71 ± 0.13 | 12.53 ± 0.11 | 6.41 ± 0.06 | 93.13 ± 0.10 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | ||
| 60 | 30 | 30.36 ± 0.08 | 23.08 ± 0.07 | 11.89 ± 0.03 | 79.85 ± 0.10 | 0.74 ± 0.00 | 0.89 ± 0.00 | 0.22 ± 0.00 | |
| 60 | 28.89 ± 0.03 | 21.33 ± 0.04 | 10.92 ± 0.01 | 81.76 ± 0.04 | 0.78 ± 0.00 | 0.91 ± 0.00 | 0.20 ± 0.00 | ||
| 90 | 28.95 ± 0.10 | 21.07 ± 0.09 | 10.82 ± 0.02 | 81.68 ± 0.13 | 0.79 ± 0.00 | 0.91 ± 0.00 | 0.20 ± 0.00 | ||
| 120 | 29.00 ± 0.14 | 20.97 ± 0.13 | 10.73 ± 0.04 | 81.62 ± 0.18 | 0.79 ± 0.00 | 0.91 ± 0.00 | 0.20 ± 0.00 | ||
| 575 | 30 | 30 | 24.12 ± 0.06 | 16.05 ± 0.10 | 11.43 ± 0.09 | 84.48 ± 0.07 | 0.73 ± 0.00 | 0.86 ± 0.00 | 0.24 ± 0.00 |
| 60 | 24.49 ± 0.04 | 15.93 ± 0.02 | 11.39 ± 0.02 | 84.00 ± 0.06 | 0.73 ± 0.00 | 0.85 ± 0.00 | 0.25 ± 0.00 | ||
| 90 | 24.38 ± 0.09 | 15.97 ± 0.13 | 11.56 ± 0.11 | 84.13 ± 0.12 | 0.74 ± 0.00 | 0.85 ± 0.00 | 0.25 ± 0.00 | ||
| 120 | 24.35 ± 0.09 | 16.07 ± 0.12 | 11.72 ± 0.16 | 84.17 ± 0.12 | 0.75 ± 0.00 | 0.85 ± 0.01 | 0.25 ± 0.00 | ||
| 60 | 30 | 36.22 ± 0.10 | 26.77 ± 0.12 | 19.49 ± 0.10 | 65.08 ± 0.19 | 0.51 ± 0.00 | 0.69 ± 0.00 | 0.40 ± 0.00 | |
| 60 | 36.27 ± 0.20 | 26.24 ± 0.25 | 18.96 ± 0.17 | 64.96 ± 0.39 | 0.54 ± 0.01 | 0.70 ± 0.00 | 0.39 ± 0.00 | ||
| 90 | 35.90 ± 0.23 | 25.73 ± 0.11 | 18.79 ± 0.09 | 65.68 ± 0.44 | 0.55 ± 0.00 | 0.70 ± 0.00 | 0.39 ± 0.00 | ||
| 120 | 35.63 ± 0.17 | 25.66 ± 0.20 | 18.91 ± 0.17 | 66.19 ± 0.32 | 0.57 ± 0.01 | 0.71 ± 0.00 | 0.38 ± 0.00 | ||
| 588 | 30 | 30 | 18.80 ± 0.09 | 13.99 ± 0.09 | 8.63 ± 0.07 | 84.49 ± 0.15 | 0.75 ± 0.00 | 0.92 ± 0.00 | 0.19 ± 0.00 |
| 60 | 18.27 ± 0.42 | 13.61 ± 0.20 | 8.36 ± 0.06 | 85.35 ± 0.68 | 0.75 ± 0.02 | 0.93 ± 0.00 | 0.18 ± 0.00 | ||
| 90 | 18.07 ± 0.35 | 13.50 ± 0.15 | 8.29 ± 0.01 | 85.66 ± 0.56 | 0.76 ± 0.01 | 0.93 ± 0.00 | 0.18 ± 0.00 | ||
| 120 | 18.44 ± 0.67 | 13.64 ± 0.37 | 8.26 ± 0.13 | 85.06 ± 1.09 | 0.75 ± 0.02 | 0.93 ± 0.01 | 0.18 ± 0.00 | ||
| 60 | 30 | 30.36 ± 0.11 | 22.68 ± 0.13 | 14.16 ± 0.12 | 59.60 ± 0.28 | 0.58 ± 0.00 | 0.77 ± 0.00 | 0.31 ± 0.00 | |
| 60 | 30.72 ± 0.26 | 22.76 ± 0.25 | 13.62 ± 0.16 | 58.65 ± 0.69 | 0.56 ± 0.01 | 0.79 ± 0.00 | 0.30 ± 0.00 | ||
| 90 | 30.58 ± 0.05 | 22.47 ± 0.10 | 13.41 ± 0.08 | 59.01 ± 0.13 | 0.56 ± 0.00 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 120 | 30.48 ± 0.25 | 22.39 ± 0.26 | 13.33 ± 0.19 | 59.29 ± 0.67 | 0.57 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 591 | 30 | 30 | 22.89 ± 0.02 | 16.68 ± 0.02 | 12.98 ± 0.02 | 80.47 ± 0.04 | 0.62 ± 0.00 | 0.79 ± 0.00 | 0.29 ± 0.00 |
| 60 | 22.98 ± 0.11 | 16.61 ± 0.05 | 12.99 ± 0.03 | 80.32 ± 0.18 | 0.65 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 90 | 23.01 ± 0.06 | 16.71 ± 0.01 | 13.12 ± 0.02 | 80.26 ± 0.09 | 0.64 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 120 | 22.97 ± 0.07 | 16.78 ± 0.05 | 13.21 ± 0.11 | 80.32 ± 0.12 | 0.64 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 60 | 30 | 35.00 ± 0.05 | 27.27 ± 0.06 | 22.01 ± 0.07 | 54.35 ± 0.14 | 0.36 ± 0.00 | 0.64 ± 0.00 | 0.45 ± 0.00 | |
| 60 | 35.93 ± 0.07 | 27.77 ± 0.02 | 22.37 ± 0.07 | 51.89 ± 0.19 | 0.35 ± 0.00 | 0.63 ± 0.00 | 0.46 ± 0.00 | ||
| 90 | 34.98 ± 0.05 | 26.93 ± 0.08 | 21.91 ± 0.13 | 54.41 ± 0.12 | 0.39 ± 0.00 | 0.65 ± 0.00 | 0.45 ± 0.00 | ||
| 120 | 34.91 ± 0.07 | 27.12 ± 0.16 | 22.19 ± 0.25 | 54.60 ± 0.19 | 0.39 ± 0.00 | 0.65 ± 0.00 | 0.45 ± 0.00 | ||
| PID | PH | LL | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | |||
| 540 | 30 | 30 | 23.48 ± 0.04 | 17.73 ± 0.03 | 12.88 ± 0.00 | 86.93 ± 0.04 | 0.67 ± 0.00 | 0.81 ± 0.00 | 0.28 ± 0.00 |
| 60 | 22.88 ± 0.13 | 17.45 ± 0.10 | 12.71 ± 0.04 | 87.60 ± 0.14 | 0.68 ± 0.00 | 0.81 ± 0.00 | 0.27 ± 0.00 | ||
| 90 | 23.41 ± 0.08 | 17.79 ± 0.04 | 12.84 ± 0.04 | 87.02 ± 0.09 | 0.68 ± 0.00 | 0.81 ± 0.00 | 0.28 ± 0.00 | ||
| 120 | 23.61 ± 0.13 | 17.92 ± 0.07 | 12.86 ± 0.02 | 86.79 ± 0.15 | 0.67 ± 0.00 | 0.81 ± 0.00 | 0.28 ± 0.00 | ||
| 60 | 30 | 40.74 ± 0.16 | 31.20 ± 0.15 | 23.55 ± 0.12 | 60.76 ± 0.32 | 0.49 ± 0.00 | 0.65 ± 0.00 | 0.45 ± 0.00 | |
| 60 | 39.84 ± 0.14 | 30.49 ± 0.12 | 22.96 ± 0.13 | 62.48 ± 0.27 | 0.52 ± 0.00 | 0.66 ± 0.00 | 0.44 ± 0.00 | ||
| 90 | 40.15 ± 0.16 | 30.68 ± 0.15 | 23.09 ± 0.14 | 61.90 ± 0.30 | 0.52 ± 0.01 | 0.66 ± 0.00 | 0.44 ± 0.00 | ||
| 120 | 40.38 ± 0.16 | 30.88 ± 0.14 | 23.16 ± 0.07 | 61.45 ± 0.31 | 0.52 ± 0.00 | 0.66 ± 0.00 | 0.44 ± 0.00 | ||
| 544 | 30 | 30 | 17.76 ± 0.06 | 12.45 ± 0.07 | 8.47 ± 0.07 | 87.73 ± 0.09 | 0.78 ± 0.00 | 0.91 ± 0.00 | 0.18 ± 0.00 |
| 60 | 17.37 ± 0.03 | 12.14 ± 0.03 | 8.21 ± 0.03 | 88.26 ± 0.04 | 0.78 ± 0.00 | 0.92 ± 0.00 | 0.18 ± 0.00 | ||
| 90 | 17.61 ± 0.03 | 12.42 ± 0.04 | 8.35 ± 0.03 | 87.94 ± 0.05 | 0.77 ± 0.00 | 0.91 ± 0.00 | 0.18 ± 0.00 | ||
| 120 | 17.78 ± 0.10 | 12.49 ± 0.04 | 8.39 ± 0.03 | 87.71 ± 0.13 | 0.77 ± 0.00 | 0.91 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 30 | 29.25 ± 0.08 | 21.79 ± 0.08 | 15.29 ± 0.08 | 66.61 ± 0.19 | 0.59 ± 0.00 | 0.75 ± 0.00 | 0.32 ± 0.00 | |
| 60 | 28.49 ± 0.03 | 20.74 ± 0.04 | 14.16 ± 0.05 | 68.32 ± 0.07 | 0.63 ± 0.00 | 0.78 ± 0.00 | 0.30 ± 0.00 | ||
| 90 | 28.92 ± 0.09 | 21.03 ± 0.02 | 14.29 ± 0.04 | 67.35 ± 0.20 | 0.63 ± 0.00 | 0.77 ± 0.00 | 0.30 ± 0.00 | ||
| 120 | 29.14 ± 0.12 | 21.12 ± 0.09 | 14.32 ± 0.04 | 66.86 ± 0.27 | 0.62 ± 0.00 | 0.77 ± 0.00 | 0.31 ± 0.00 | ||
| 552 | 30 | 30 | 14.06 ± 0.03 | 8.25 ± 0.11 | 6.48 ± 0.09 | 86.18 ± 0.05 | 0.75 ± 0.00 | 0.92 ± 0.00 | 0.14 ± 0.00 |
| 60 | 14.32 ± 0.08 | 8.91 ± 0.08 | 7.03 ± 0.06 | 85.67 ± 0.16 | 0.73 ± 0.00 | 0.91 ± 0.00 | 0.15 ± 0.00 | ||
| 90 | 14.47 ± 0.10 | 9.25 ± 0.09 | 7.30 ± 0.09 | 85.36 ± 0.20 | 0.72 ± 0.00 | 0.91 ± 0.00 | 0.15 ± 0.00 | ||
| 120 | 14.60 ± 0.08 | 9.42 ± 0.03 | 7.44 ± 0.03 | 85.09 ± 0.16 | 0.72 ± 0.00 | 0.91 ± 0.00 | 0.15 ± 0.00 | ||
| 60 | 30 | 23.83 ± 0.03 | 14.57 ± 0.10 | 11.75 ± 0.12 | 60.36 ± 0.09 | 0.64 ± 0.00 | 0.84 ± 0.00 | 0.22 ± 0.00 | |
| 60 | 23.71 ± 0.06 | 14.94 ± 0.06 | 12.07 ± 0.06 | 60.78 ± 0.18 | 0.63 ± 0.00 | 0.84 ± 0.00 | 0.22 ± 0.00 | ||
| 90 | 23.75 ± 0.08 | 15.44 ± 0.09 | 12.42 ± 0.06 | 60.66 ± 0.26 | 0.64 ± 0.00 | 0.84 ± 0.00 | 0.23 ± 0.00 | ||
| 120 | 23.87 ± 0.07 | 15.50 ± 0.09 | 12.47 ± 0.08 | 60.25 ± 0.22 | 0.64 ± 0.00 | 0.84 ± 0.00 | 0.23 ± 0.00 | ||
| 567 | 30 | 30 | 22.72 ± 0.04 | 16.47 ± 0.04 | 12.48 ± 0.03 | 84.80 ± 0.05 | 0.64 ± 0.00 | 0.80 ± 0.00 | 0.28 ± 0.00 |
| 60 | 22.98 ± 0.07 | 16.63 ± 0.07 | 12.93 ± 0.07 | 84.44 ± 0.10 | 0.64 ± 0.00 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 90 | 23.48 ± 0.18 | 17.24 ± 0.15 | 13.48 ± 0.12 | 83.77 ± 0.25 | 0.62 ± 0.00 | 0.79 ± 0.00 | 0.31 ± 0.00 | ||
| 120 | 24.18 ± 0.20 | 17.98 ± 0.15 | 14.18 ± 0.12 | 82.78 ± 0.29 | 0.61 ± 0.00 | 0.78 ± 0.00 | 0.32 ± 0.00 | ||
| 60 | 30 | 38.38 ± 0.02 | 29.51 ± 0.04 | 23.24 ± 0.06 | 56.68 ± 0.04 | 0.46 ± 0.00 | 0.64 ± 0.00 | 0.47 ± 0.00 | |
| 60 | 39.00 ± 0.07 | 29.36 ± 0.01 | 23.95 ± 0.01 | 55.27 ± 0.15 | 0.48 ± 0.00 | 0.64 ± 0.00 | 0.48 ± 0.00 | ||
| 90 | 39.46 ± 0.07 | 29.96 ± 0.01 | 24.71 ± 0.03 | 54.22 ± 0.17 | 0.46 ± 0.00 | 0.63 ± 0.00 | 0.49 ± 0.00 | ||
| 120 | 40.39 ± 0.15 | 30.91 ± 0.08 | 25.66 ± 0.09 | 52.01 ± 0.35 | 0.44 ± 0.00 | 0.62 ± 0.00 | 0.51 ± 0.00 | ||
| 584 | 30 | 30 | 23.25 ± 0.08 | 16.72 ± 0.06 | 11.00 ± 0.07 | 84.88 ± 0.10 | 0.76 ± 0.00 | 0.87 ± 0.00 | 0.23 ± 0.00 |
| 60 | 22.78 ± 0.04 | 16.92 ± 0.04 | 11.34 ± 0.03 | 85.49 ± 0.05 | 0.77 ± 0.00 | 0.87 ± 0.00 | 0.23 ± 0.00 | ||
| 90 | 22.80 ± 0.02 | 17.17 ± 0.03 | 11.51 ± 0.02 | 85.47 ± 0.03 | 0.76 ± 0.00 | 0.88 ± 0.00 | 0.24 ± 0.00 | ||
| 120 | 23.30 ± 0.10 | 17.59 ± 0.10 | 11.79 ± 0.08 | 84.82 ± 0.13 | 0.75 ± 0.00 | 0.87 ± 0.00 | 0.25 ± 0.00 | ||
| 60 | 30 | 37.53 ± 0.03 | 27.65 ± 0.22 | 18.33 ± 0.27 | 60.48 ± 0.07 | 0.59 ± 0.00 | 0.71 ± 0.01 | 0.37 ± 0.00 | |
| 60 | 35.99 ± 0.05 | 27.29 ± 0.02 | 18.40 ± 0.03 | 63.67 ± 0.11 | 0.60 ± 0.00 | 0.72 ± 0.00 | 0.37 ± 0.00 | ||
| 90 | 36.04 ± 0.06 | 27.64 ± 0.06 | 18.72 ± 0.07 | 63.56 ± 0.12 | 0.59 ± 0.00 | 0.72 ± 0.00 | 0.38 ± 0.00 | ||
| 120 | 36.39 ± 0.04 | 27.83 ± 0.09 | 18.84 ± 0.12 | 62.85 ± 0.08 | 0.58 ± 0.00 | 0.71 ± 0.00 | 0.38 ± 0.00 | ||
| 596 | 30 | 30 | 18.66 ± 0.09 | 13.47 ± 0.11 | 10.09 ± 0.10 | 85.82 ± 0.14 | 0.71 ± 0.00 | 0.89 ± 0.00 | 0.21 ± 0.00 |
| 60 | 17.87 ± 0.08 | 12.89 ± 0.06 | 9.67 ± 0.03 | 86.99 ± 0.12 | 0.74 ± 0.00 | 0.89 ± 0.00 | 0.20 ± 0.00 | ||
| 90 | 17.87 ± 0.09 | 12.93 ± 0.06 | 9.71 ± 0.03 | 86.99 ± 0.13 | 0.75 ± 0.00 | 0.89 ± 0.00 | 0.20 ± 0.00 | ||
| 120 | 17.95 ± 0.05 | 12.98 ± 0.03 | 9.76 ± 0.02 | 86.89 ± 0.07 | 0.74 ± 0.00 | 0.90 ± 0.00 | 0.20 ± 0.00 | ||
| 60 | 30 | 30.46 ± 0.10 | 22.78 ± 0.08 | 17.57 ± 0.08 | 62.29 ± 0.25 | 0.52 ± 0.00 | 0.78 ± 0.00 | 0.33 ± 0.00 | |
| 60 | 29.00 ± 0.13 | 21.43 ± 0.14 | 16.36 ± 0.13 | 65.83 ± 0.30 | 0.56 ± 0.00 | 0.80 ± 0.00 | 0.31 ± 0.00 | ||
| 90 | 28.79 ± 0.05 | 21.35 ± 0.07 | 16.28 ± 0.07 | 66.32 ± 0.13 | 0.57 ± 0.01 | 0.80 ± 0.00 | 0.31 ± 0.00 | ||
| 120 | 28.83 ± 0.16 | 21.37 ± 0.16 | 16.34 ± 0.16 | 66.22 ± 0.37 | 0.57 ± 0.01 | 0.81 ± 0.00 | 0.31 ± 0.00 | ||
| PID | PH | LL | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | |||
| 559 | 30 | 30 | 23.12 ± 0.43 | 16.60 ± 0.66 | 11.10 ± 0.63 | 87.19 ± 0.47 | 0.74 ± 0.01 | 0.86 ± 0.01 | 0.24 ± 0.01 |
| 60 | 23.51 ± 0.36 | 16.79 ± 0.54 | 11.02 ± 0.64 | 86.76 ± 0.40 | 0.74 ± 0.01 | 0.87 ± 0.01 | 0.23 ± 0.01 | ||
| 90 | 25.50 ± 1.19 | 17.44 ± 0.64 | 10.71 ± 0.13 | 84.39 ± 1.44 | 0.72 ± 0.03 | 0.87 ± 0.01 | 0.23 ± 0.00 | ||
| 120 | 32.86 ± 13.20 | 23.72 ± 10.60 | 15.55 ± 8.01 | 71.35 ± 23.13 | 0.63 ± 0.19 | 0.78 ± 0.16 | 0.31 ± 0.15 | ||
| 60 | 30 | 38.39 ± 0.82 | 27.05 ± 0.53 | 16.65 ± 0.21 | 64.46 ± 1.52 | 0.57 ± 0.01 | 0.75 ± 0.00 | 0.35 ± 0.00 | |
| 60 | 38.73 ± 4.41 | 27.75 ± 3.58 | 17.37 ± 1.50 | 63.53 ± 8.42 | 0.54 ± 0.07 | 0.73 ± 0.05 | 0.37 ± 0.05 | ||
| 90 | 37.77 ± 3.27 | 26.72 ± 2.04 | 16.92 ± 0.47 | 65.46 ± 6.01 | 0.58 ± 0.02 | 0.75 ± 0.01 | 0.35 ± 0.02 | ||
| 120 | 36.08 ± 1.47 | 25.38 ± 0.84 | 16.62 ± 0.25 | 68.60 ± 2.56 | 0.59 ± 0.02 | 0.75 ± 0.01 | 0.34 ± 0.01 | ||
| 563 | 30 | 30 | 21.59 ± 0.64 | 15.33 ± 0.45 | 9.69 ± 0.19 | 77.31 ± 1.34 | 0.72 ± 0.01 | 0.89 ± 0.00 | 0.22 ± 0.00 |
| 60 | 21.73 ± 0.46 | 15.52 ± 0.33 | 9.82 ± 0.32 | 77.03 ± 0.96 | 0.73 ± 0.00 | 0.89 ± 0.00 | 0.22 ± 0.01 | ||
| 90 | 24.91 ± 1.84 | 17.49 ± 1.38 | 10.96 ± 1.02 | 69.71 ± 4.55 | 0.69 ± 0.03 | 0.87 ± 0.02 | 0.24 ± 0.02 | ||
| 120 | 24.04 ± 1.89 | 16.94 ± 1.15 | 10.65 ± 0.72 | 71.79 ± 4.43 | 0.69 ± 0.01 | 0.87 ± 0.01 | 0.24 ± 0.01 | ||
| 60 | 30 | 33.02 ± 0.62 | 24.13 ± 0.61 | 15.07 ± 0.18 | 47.03 ± 2.01 | 0.51 ± 0.01 | 0.75 ± 0.02 | 0.33 ± 0.01 | |
| 60 | 34.44 ± 2.48 | 25.05 ± 2.24 | 15.80 ± 1.37 | 42.17 ± 8.46 | 0.48 ± 0.09 | 0.74 ± 0.06 | 0.35 ± 0.03 | ||
| 90 | 34.32 ± 1.23 | 24.45 ± 1.04 | 15.16 ± 0.63 | 42.73 ± 4.13 | 0.52 ± 0.01 | 0.77 ± 0.02 | 0.34 ± 0.01 | ||
| 120 | 34.13 ± 1.59 | 24.66 ± 1.10 | 15.27 ± 0.62 | 43.33 ± 5.27 | 0.50 ± 0.02 | 0.76 ± 0.02 | 0.34 ± 0.01 | ||
| 570 | 30 | 30 | 24.78 ± 3.96 | 18.97 ± 3.76 | 8.84 ± 1.30 | 86.33 ± 4.12 | 0.82 ± 0.01 | 0.94 ± 0.01 | 0.16 ± 0.02 |
| 60 | 25.83 ± 5.11 | 19.99 ± 4.76 | 9.28 ± 1.87 | 85.02 ± 5.59 | 0.81 ± 0.03 | 0.93 ± 0.02 | 0.17 ± 0.03 | ||
| 90 | 23.09 ± 2.28 | 17.15 ± 2.09 | 8.26 ± 0.74 | 88.25 ± 2.30 | 0.82 ± 0.01 | 0.94 ± 0.00 | 0.15 ± 0.01 | ||
| 120 | 22.92 ± 1.49 | 16.16 ± 1.15 | 8.04 ± 0.65 | 88.47 ± 1.52 | 0.81 ± 0.02 | 0.94 ± 0.01 | 0.15 ± 0.01 | ||
| 60 | 30 | 38.34 ± 2.65 | 29.98 ± 2.52 | 13.56 ± 0.95 | 67.77 ± 4.48 | 0.75 ± 0.01 | 0.88 ± 0.01 | 0.25 ± 0.02 | |
| 60 | 35.80 ± 1.50 | 26.75 ± 1.85 | 12.68 ± 0.43 | 71.95 ± 2.31 | 0.75 ± 0.00 | 0.88 ± 0.01 | 0.23 ± 0.01 | ||
| 90 | 37.00 ± 2.48 | 27.94 ± 1.86 | 13.17 ± 0.99 | 69.98 ± 4.09 | 0.75 ± 0.03 | 0.87 ± 0.02 | 0.24 ± 0.02 | ||
| 120 | 35.80 ± 2.62 | 25.82 ± 2.70 | 12.58 ± 0.95 | 71.89 ± 4.09 | 0.75 ± 0.02 | 0.88 ± 0.01 | 0.23 ± 0.02 | ||
| 575 | 30 | 30 | 27.20 ± 0.57 | 18.25 ± 0.45 | 13.14 ± 0.71 | 80.24 ± 0.82 | 0.69 ± 0.00 | 0.82 ± 0.02 | 0.28 ± 0.01 |
| 60 | 27.52 ± 0.76 | 18.26 ± 0.37 | 13.07 ± 0.32 | 79.77 ± 1.13 | 0.69 ± 0.01 | 0.82 ± 0.00 | 0.28 ± 0.01 | ||
| 90 | 28.37 ± 0.99 | 18.89 ± 0.88 | 13.78 ± 0.69 | 78.51 ± 1.51 | 0.68 ± 0.01 | 0.80 ± 0.01 | 0.30 ± 0.01 | ||
| 120 | 29.33 ± 1.12 | 19.83 ± 1.63 | 13.69 ± 0.60 | 77.03 ± 1.74 | 0.65 ± 0.05 | 0.80 ± 0.02 | 0.29 ± 0.01 | ||
| 60 | 30 | 38.09 ± 0.03 | 27.47 ± 0.52 | 20.48 ± 1.20 | 61.36 ± 0.07 | 0.54 ± 0.02 | 0.70 ± 0.00 | 0.41 ± 0.01 | |
| 60 | 39.96 ± 0.84 | 28.84 ± 0.27 | 21.39 ± 1.07 | 57.46 ± 1.78 | 0.55 ± 0.03 | 0.68 ± 0.01 | 0.44 ± 0.01 | ||
| 90 | 38.15 ± 0.52 | 27.58 ± 0.22 | 20.56 ± 0.49 | 61.24 ± 1.06 | 0.52 ± 0.01 | 0.68 ± 0.01 | 0.42 ± 0.01 | ||
| 120 | 39.47 ± 1.28 | 28.64 ± 0.43 | 21.35 ± 0.44 | 58.48 ± 2.69 | 0.54 ± 0.01 | 0.67 ± 0.01 | 0.43 ± 0.01 | ||
| 588 | 30 | 30 | 19.23 ± 0.11 | 14.16 ± 0.11 | 8.53 ± 0.12 | 83.77 ± 0.19 | 0.74 ± 0.00 | 0.92 ± 0.00 | 0.19 ± 0.00 |
| 60 | 19.60 ± 0.23 | 14.57 ± 0.15 | 8.83 ± 0.07 | 83.13 ± 0.39 | 0.74 ± 0.01 | 0.92 ± 0.00 | 0.19 ± 0.00 | ||
| 90 | 20.33 ± 0.86 | 15.00 ± 0.73 | 8.87 ± 0.36 | 81.84 ± 1.54 | 0.73 ± 0.01 | 0.92 ± 0.00 | 0.19 ± 0.01 | ||
| 120 | 21.99 ± 1.74 | 16.39 ± 1.07 | 9.64 ± 0.77 | 78.69 ± 3.39 | 0.69 ± 0.02 | 0.91 ± 0.02 | 0.20 ± 0.02 | ||
| 60 | 30 | 31.32 ± 0.53 | 23.12 ± 0.56 | 14.05 ± 0.68 | 57.00 ± 1.48 | 0.57 ± 0.01 | 0.79 ± 0.02 | 0.30 ± 0.02 | |
| 60 | 30.46 ± 0.60 | 22.48 ± 0.39 | 14.04 ± 0.23 | 59.33 ± 1.61 | 0.60 ± 0.01 | 0.79 ± 0.01 | 0.30 ± 0.01 | ||
| 90 | 32.01 ± 0.53 | 23.06 ± 0.33 | 14.11 ± 0.47 | 55.07 ± 1.48 | 0.58 ± 0.02 | 0.80 ± 0.01 | 0.30 ± 0.01 | ||
| 120 | 35.57 ± 4.21 | 25.60 ± 2.74 | 15.65 ± 1.69 | 44.02 ± 13.55 | 0.50 ± 0.08 | 0.76 ± 0.03 | 0.33 ± 0.03 | ||
| 591 | 30 | 30 | 26.00 ± 0.54 | 19.63 ± 0.54 | 15.81 ± 0.75 | 74.78 ± 1.04 | 0.58 ± 0.01 | 0.74 ± 0.00 | 0.35 ± 0.01 |
| 60 | 26.33 ± 0.42 | 19.55 ± 0.24 | 15.65 ± 0.40 | 74.16 ± 0.83 | 0.60 ± 0.00 | 0.75 ± 0.01 | 0.34 ± 0.01 | ||
| 90 | 27.44 ± 1.02 | 20.46 ± 0.58 | 15.63 ± 0.98 | 71.90 ± 2.10 | 0.55 ± 0.05 | 0.74 ± 0.01 | 0.34 ± 0.01 | ||
| 120 | 27.16 ± 0.88 | 20.13 ± 0.63 | 15.75 ± 0.85 | 72.48 ± 1.78 | 0.57 ± 0.03 | 0.74 ± 0.02 | 0.34 ± 0.01 | ||
| 60 | 30 | 36.51 ± 0.20 | 28.36 ± 0.26 | 23.32 ± 0.27 | 50.32 ± 0.54 | 0.37 ± 0.02 | 0.63 ± 0.00 | 0.47 ± 0.00 | |
| 60 | 37.52 ± 0.93 | 28.36 ± 0.32 | 22.47 ± 0.57 | 47.52 ± 2.58 | 0.36 ± 0.04 | 0.63 ± 0.01 | 0.47 ± 0.00 | ||
| 90 | 37.92 ± 1.44 | 29.32 ± 1.16 | 24.31 ± 1.51 | 46.38 ± 4.10 | 0.39 ± 0.04 | 0.63 ± 0.01 | 0.48 ± 0.01 | ||
| 120 | 37.07 ± 1.67 | 28.38 ± 1.14 | 22.37 ± 0.89 | 48.73 ± 4.57 | 0.37 ± 0.02 | 0.63 ± 0.02 | 0.47 ± 0.02 | ||
| PID | PH | LL | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | |||
| 540 | 30 | 30 | 25.76 ± 1.26 | 19.38 ± 0.62 | 14.84 ± 0.24 | 84.25 ± 1.55 | 0.67 ± 0.01 | 0.79 ± 0.00 | 0.31 ± 0.00 |
| 60 | 24.84 ± 0.42 | 18.48 ± 0.70 | 13.81 ± 1.24 | 85.37 ± 0.49 | 0.67 ± 0.02 | 0.80 ± 0.01 | 0.29 ± 0.02 | ||
| 90 | 28.02 ± 3.64 | 21.40 ± 2.68 | 15.98 ± 2.30 | 81.18 ± 4.68 | 0.63 ± 0.03 | 0.76 ± 0.03 | 0.33 ± 0.04 | ||
| 120 | 27.92 ± 1.82 | 21.00 ± 1.99 | 15.38 ± 2.29 | 81.48 ± 2.40 | 0.63 ± 0.02 | 0.76 ± 0.02 | 0.32 ± 0.04 | ||
| 60 | 30 | 42.60 ± 1.15 | 31.84 ± 0.41 | 23.25 ± 0.53 | 57.07 ± 2.32 | 0.48 ± 0.02 | 0.64 ± 0.01 | 0.45 ± 0.00 | |
| 60 | 41.36 ± 0.58 | 30.69 ± 0.37 | 22.40 ± 0.20 | 59.56 ± 1.12 | 0.50 ± 0.02 | 0.66 ± 0.00 | 0.44 ± 0.00 | ||
| 90 | 43.78 ± 2.80 | 32.44 ± 2.02 | 23.51 ± 1.66 | 54.55 ± 5.78 | 0.50 ± 0.04 | 0.64 ± 0.02 | 0.45 ± 0.02 | ||
| 120 | 48.17 ± 1.39 | 34.62 ± 2.09 | 24.69 ± 2.33 | 45.10 ± 3.15 | 0.48 ± 0.04 | 0.63 ± 0.03 | 0.48 ± 0.03 | ||
| 544 | 30 | 30 | 21.23 ± 0.53 | 15.00 ± 0.49 | 9.93 ± 0.35 | 82.45 ± 0.87 | 0.76 ± 0.01 | 0.89 ± 0.00 | 0.21 ± 0.01 |
| 60 | 20.66 ± 0.31 | 14.71 ± 0.43 | 9.99 ± 0.53 | 83.40 ± 0.50 | 0.75 ± 0.01 | 0.88 ± 0.02 | 0.22 ± 0.01 | ||
| 90 | 22.55 ± 0.45 | 15.56 ± 0.37 | 10.40 ± 0.27 | 80.21 ± 0.79 | 0.72 ± 0.01 | 0.88 ± 0.01 | 0.22 ± 0.00 | ||
| 120 | 23.38 ± 2.94 | 16.49 ± 1.81 | 11.35 ± 1.30 | 78.51 ± 5.18 | 0.71 ± 0.04 | 0.84 ± 0.03 | 0.24 ± 0.03 | ||
| 60 | 30 | 31.43 ± 0.05 | 23.19 ± 0.08 | 15.59 ± 0.16 | 61.46 ± 0.12 | 0.58 ± 0.01 | 0.76 ± 0.00 | 0.32 ± 0.00 | |
| 60 | 30.45 ± 0.12 | 22.09 ± 0.45 | 14.81 ± 0.52 | 63.83 ± 0.29 | 0.59 ± 0.02 | 0.78 ± 0.01 | 0.31 ± 0.01 | ||
| 90 | 32.39 ± 0.61 | 22.91 ± 0.32 | 15.40 ± 0.39 | 59.04 ± 1.55 | 0.57 ± 0.01 | 0.76 ± 0.01 | 0.33 ± 0.01 | ||
| 120 | 36.19 ± 1.38 | 25.61 ± 0.40 | 17.44 ± 0.10 | 48.85 ± 3.94 | 0.52 ± 0.04 | 0.74 ± 0.01 | 0.36 ± 0.01 | ||
| 552 | 30 | 30 | 16.72 ± 0.44 | 10.31 ± 0.24 | 8.04 ± 0.22 | 80.45 ± 1.01 | 0.71 ± 0.02 | 0.90 ± 0.01 | 0.16 ± 0.01 |
| 60 | 21.54 ± 3.51 | 14.67 ± 3.62 | 11.21 ± 2.37 | 66.99 ± 10.53 | 0.59 ± 0.14 | 0.85 ± 0.04 | 0.22 ± 0.04 | ||
| 90 | 18.81 ± 1.50 | 12.58 ± 1.52 | 9.73 ± 0.98 | 75.16 ± 3.97 | 0.69 ± 0.01 | 0.89 ± 0.01 | 0.19 ± 0.01 | ||
| 120 | 20.91 ± 5.44 | 14.00 ± 4.23 | 11.01 ± 3.87 | 68.05 ± 17.09 | 0.69 ± 0.08 | 0.85 ± 0.10 | 0.22 ± 0.08 | ||
| 60 | 30 | 25.47 ± 0.30 | 16.27 ± 0.24 | 13.02 ± 0.27 | 54.73 ± 1.05 | 0.61 ± 0.01 | 0.83 ± 0.01 | 0.24 ± 0.01 | |
| 60 | 27.15 ± 1.00 | 18.20 ± 0.92 | 15.02 ± 0.93 | 48.51 ± 3.76 | 0.58 ± 0.03 | 0.78 ± 0.02 | 0.28 ± 0.02 | ||
| 90 | 27.51 ± 2.98 | 17.70 ± 1.96 | 14.55 ± 1.73 | 46.78 ± 11.78 | 0.56 ± 0.06 | 0.80 ± 0.04 | 0.27 ± 0.04 | ||
| 120 | 40.75 ± 25.37 | 32.17 ± 26.99 | 26.17 ± 21.83 | 45.82 ± 170.04 | 0.33 ± 0.44 | 0.60 ± 0.38 | 0.53 ± 0.49 | ||
| 567 | 30 | 30 | 26.21 ± 1.00 | 18.74 ± 1.00 | 14.41 ± 1.01 | 79.74 ± 1.56 | 0.61 ± 0.01 | 0.77 ± 0.01 | 0.32 ± 0.02 |
| 60 | 25.54 ± 0.32 | 18.38 ± 0.28 | 13.83 ± 0.55 | 80.78 ± 0.48 | 0.61 ± 0.01 | 0.78 ± 0.00 | 0.31 ± 0.01 | ||
| 90 | 24.64 ± 0.97 | 17.85 ± 0.81 | 13.48 ± 0.66 | 82.10 ± 1.41 | 0.60 ± 0.01 | 0.78 ± 0.01 | 0.31 ± 0.01 | ||
| 120 | 27.89 ± 3.45 | 20.96 ± 3.26 | 16.17 ± 2.94 | 76.86 ± 5.47 | 0.57 ± 0.05 | 0.74 ± 0.04 | 0.35 ± 0.06 | ||
| 60 | 30 | 43.16 ± 1.27 | 32.69 ± 1.21 | 27.34 ± 1.23 | 45.19 ± 3.24 | 0.44 ± 0.02 | 0.60 ± 0.02 | 0.53 ± 0.02 | |
| 60 | 40.13 ± 1.22 | 30.57 ± 1.14 | 25.05 ± 1.96 | 52.61 ± 2.86 | 0.45 ± 0.01 | 0.62 ± 0.02 | 0.50 ± 0.03 | ||
| 90 | 42.89 ± 2.29 | 32.84 ± 2.03 | 26.97 ± 2.57 | 45.79 ± 5.74 | 0.41 ± 0.01 | 0.60 ± 0.02 | 0.53 ± 0.03 | ||
| 120 | 45.08 ± 4.52 | 34.30 ± 3.01 | 26.78 ± 0.56 | 39.83 ± 12.30 | 0.40 ± 0.06 | 0.58 ± 0.04 | 0.54 ± 0.04 | ||
| 584 | 30 | 30 | 26.87 ± 0.77 | 19.56 ± 0.72 | 13.10 ± 0.55 | 79.81 ± 1.16 | 0.72 ± 0.02 | 0.84 ± 0.01 | 0.26 ± 0.01 |
| 60 | 25.31 ± 1.32 | 18.27 ± 0.95 | 11.49 ± 0.52 | 82.05 ± 1.89 | 0.75 ± 0.01 | 0.86 ± 0.01 | 0.23 ± 0.01 | ||
| 90 | 25.93 ± 1.03 | 19.25 ± 0.82 | 13.00 ± 0.65 | 81.19 ± 1.47 | 0.74 ± 0.01 | 0.85 ± 0.01 | 0.26 ± 0.01 | ||
| 120 | 27.62 ± 0.80 | 20.65 ± 1.21 | 13.36 ± 0.35 | 78.66 ± 1.24 | 0.72 ± 0.02 | 0.84 ± 0.01 | 0.27 ± 0.00 | ||
| 60 | 30 | 41.45 ± 1.58 | 31.50 ± 1.91 | 21.43 ± 2.17 | 51.75 ± 3.64 | 0.55 ± 0.03 | 0.67 ± 0.04 | 0.42 ± 0.04 | |
| 60 | 42.14 ± 1.60 | 32.72 ± 1.78 | 23.12 ± 1.60 | 50.12 ± 3.74 | 0.55 ± 0.01 | 0.64 ± 0.04 | 0.45 ± 0.03 | ||
| 90 | 41.75 ± 0.90 | 32.60 ± 0.83 | 22.86 ± 1.00 | 51.08 ± 2.11 | 0.56 ± 0.01 | 0.65 ± 0.02 | 0.44 ± 0.02 | ||
| 120 | 47.83 ± 3.54 | 37.15 ± 4.34 | 25.97 ± 4.37 | 35.58 ± 9.66 | 0.46 ± 0.05 | 0.59 ± 0.07 | 0.50 ± 0.08 | ||
| 596 | 30 | 30 | 19.96 ± 0.28 | 14.31 ± 0.03 | 10.83 ± 0.18 | 83.78 ± 0.45 | 0.70 ± 0.01 | 0.87 ± 0.00 | 0.23 ± 0.00 |
| 60 | 21.15 ± 0.65 | 15.31 ± 0.40 | 11.64 ± 0.41 | 81.77 ± 1.12 | 0.69 ± 0.01 | 0.86 ± 0.01 | 0.24 ± 0.01 | ||
| 90 | 22.54 ± 0.82 | 16.38 ± 0.95 | 12.32 ± 0.90 | 79.29 ± 1.50 | 0.66 ± 0.04 | 0.85 ± 0.01 | 0.25 ± 0.01 | ||
| 120 | 33.46 ± 10.29 | 25.29 ± 8.45 | 19.64 ± 6.92 | 51.54 ± 25.67 | 0.50 ± 0.16 | 0.75 ± 0.10 | 0.36 ± 0.11 | ||
| 60 | 30 | 30.97 ± 0.19 | 22.79 ± 0.17 | 17.23 ± 0.22 | 61.02 ± 0.48 | 0.52 ± 0.01 | 0.78 ± 0.00 | 0.33 ± 0.00 | |
| 60 | 30.28 ± 0.72 | 22.17 ± 0.71 | 16.97 ± 0.45 | 62.72 ± 1.77 | 0.56 ± 0.02 | 0.79 ± 0.00 | 0.32 ± 0.01 | ||
| 90 | 31.70 ± 1.25 | 23.44 ± 1.22 | 17.94 ± 1.21 | 59.12 ± 3.24 | 0.52 ± 0.03 | 0.78 ± 0.01 | 0.34 ± 0.02 | ||
| 120 | 36.31 ± 9.68 | 27.21 ± 8.48 | 21.03 ± 6.87 | 43.87 ± 30.66 | 0.43 ± 0.21 | 0.71 ± 0.13 | 0.40 ± 0.11 | ||
References
- DiMeglio, L.A.; Evans-Molina, C.; Oram, R.A. Type 1 Diabetes. Lancet 2018, 391, 2449–2462. [Google Scholar] [CrossRef] [PubMed]
- Melin, J.; Lynch, K.F.; Lundgren, M.; Aronsson, C.A.; Larsson, H.E.; Johnson, S.B.; Rewers, M.; Barbour, A.; Bautista, K.; Baxter, J.; et al. Is Staff Consistency Important to Parents’ Satisfaction in a Longitudinal Study of Children at Risk for Type 1 Diabetes: The TEDDY Study. BMC Endocr. Disord. 2022, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Khadem, H.; Nemat, H.; Elliott, J.; Benaissa, M. Interpretable Machine Learning for Inpatient COVID-19 Mortality Risk Assessments: Diabetes Mellitus Exclusive Interplay. Sensors 2022, 22, 8757. [Google Scholar] [CrossRef] [PubMed]
- Yamada, T.; Shojima, N.; Noma, H.; Yamauchi, T.; Kadowaki, T. Sodium-Glucose Co-Transporter-2 Inhibitors as Add-on Therapy to Insulin for Type 1 Diabetes Mellitus: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Diabetes Obes. Metab. 2018, 20, 1755–1761. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Harris, C. Type 1 Diabetes: Management Strategies. Am. Fam. Physician 2018, 98, 154–162. [Google Scholar]
- Hamilton, K.; Stanton-Fay, S.H.; Chadwick, P.M.; Lorencatto, F.; de Zoysa, N.; Gianfrancesco, C.; Taylor, C.; Coates, E.; Breckenridge, J.P.; Cooke, D.; et al. Sustained Type 1 Diabetes Self-Management: Specifying the Behaviours Involved and Their Influences. Diabet. Med. 2021, 38, e14430. [Google Scholar] [CrossRef]
- Campbell, F.; Lawton, J.; Rankin, D.; Clowes, M.; Coates, E.; Heller, S.; De Zoysa, N.; Elliott, J.; Breckenridge, J.P. Follow-Up Support for Effective Type 1 Diabetes Self-Management (The FUSED Model): A Systematic Review and Meta-Ethnography of the Barriers, Facilitators and Recommendations for Sustaining Self-Management Skills after Attending a Structured Education Programme. BMC Health Serv. Res. 2018, 18, 898. [Google Scholar] [CrossRef]
- Cummings, C.; Benjamin, N.E.; Prabhu, H.Y.; Cohen, L.B.; Goddard, B.J.; Kaugars, A.S.; Humiston, T.; Lansing, A.H. Habit and Diabetes Self-Management in Adolescents With Type 1 Diabetes. Health Psychol. 2022, 41, 13–22. [Google Scholar] [CrossRef]
- McCarthy, M.M.; Grey, M. Type 1 Diabetes Self-Management From Emerging Adulthood Through Older Adulthood. Diabetes Care 2018, 41, 1608–1614. [Google Scholar] [CrossRef]
- Saoji, N.; Palta, M.; Young, H.N.; Moreno, M.A.; Rajamanickam, V.; Cox, E.D. The Relationship of Type 1 Diabetes Self-Management Barriers to Child and Parent Quality of Life: A US Cross-Sectional Study. Diabet. Med. 2018, 35, 1523–1530. [Google Scholar] [CrossRef]
- Butler, A.M.; Weller, B.E.; Rodgers, C.R.R.; Teasdale, A.E. Type 1 Diabetes Self-Management Behaviors among Emerging Adults: Racial/Ethnic Differences. Pediatr. Diabetes 2020, 21, 979–986. [Google Scholar] [CrossRef]
- Dai, X.; Luo, Z.C.; Zhai, L.; Zhao, W.P.; Huang, F. Artificial Pancreas as an Effective and Safe Alternative in Patients with Type 1 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Ther. 2018, 9, 1269–1277. [Google Scholar] [CrossRef]
- Bekiari, E.; Kitsios, K.; Thabit, H.; Tauschmann, M.; Athanasiadou, E.; Karagiannis, T.; Haidich, A.B.; Hovorka, R.; Tsapas, A. Artificial Pancreas Treatment for Outpatients with Type 1 Diabetes: Systematic Review and Meta-Analysis. BMJ 2018, 361, 1310. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, J.; Liu, L.; Qiao, H. A Review of Biosensor Technology and Algorithms for Glucose Monitoring. J. Diabetes Complicat. 2021, 35, 107929. [Google Scholar] [CrossRef]
- Choudhary, P.; Amiel, S.A. Hypoglycaemia in Type 1 Diabetes: Technological Treatments, Their Limitations and the Place of Psychology. Diabetologia 2018, 61, 761–769. [Google Scholar] [CrossRef]
- Tagougui, S.; Taleb, N.; Rabasa-Lhoret, R. The Benefits and Limits of Technological Advances in Glucose Management around Physical Activity in Patients Type 1 Diabetes. Front. Endocrinol. 2019, 10, 818. [Google Scholar] [CrossRef]
- Laffel, L.M.; Kanapka, L.G.; Beck, R.W.; Bergamo, K.; Clements, M.A.; Criego, A.; Desalvo, D.J.; Goland, R.; Hood, K.; Liljenquist, D.; et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adolescents and Young Adults With Type 1 Diabetes: A Randomized Clinical Trial. JAMA 2020, 323, 2388–2396. [Google Scholar] [CrossRef]
- Martens, T.; Beck, R.W.; Bailey, R.; Ruedy, K.J.; Calhoun, P.; Peters, A.L.; Pop-Busui, R.; Philis-Tsimikas, A.; Bao, S.; Umpierrez, G.; et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Patients With Type 2 Diabetes Treated With Basal Insulin: A Randomized Clinical Trial. JAMA 2021, 325, 2262–2272. [Google Scholar] [CrossRef]
- Pickup, J.C. Is Insulin Pump Therapy Effective in Type 1 Diabetes? Diabet. Med. 2019, 36, 269–278. [Google Scholar] [CrossRef]
- Ranjan, A.G.; Rosenlund, S.V.; Hansen, T.W.; Rossing, P.; Andersen, S.; Nørgaard, K. Improved Time in Range Over 1 Year Is Associated With Reduced Albuminuria in Individuals With Sensor-Augmented Insulin Pump–Treated Type 1 Diabetes. Diabetes Care 2020, 43, 2882–2885. [Google Scholar] [CrossRef]
- Mian, Z.; Hermayer, K.L.; Jenkins, A. Continuous Glucose Monitoring: Review of an Innovation in Diabetes Management. Am. J. Med. Sci. 2019, 358, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Pathak, S.; Goyal, R. Clinical and Economic Outcomes of Continuous Glucose Monitoring System (CGMS) in Patients with Diabetes Mellitus: A Systematic Literature Review. Diabetes Res. Clin. Pract. 2022, 186, 109825. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, M.A.; Smith, G.J.; Cooper, M.N.; Jones, T.W.; Davis, E.A. Real-World Outcomes of Insulin Pump Compared to Injection Therapy in a Population-Based Sample of Children with Type 1 Diabetes. Pediatr. Diabetes 2018, 19, 1459–1466. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Hernandez, R.; Schwandt, A.; Alkandari, H.; Bratke, H.; Chobot, A.; Coles, N.; Corathers, S.; Goksen, D.; Goss, P.; Imane, Z.; et al. Glycemic Outcome Associated With Insulin Pump and Glucose Sensor Use in Children and Adolescents With Type 1 Diabetes. Data From the International Pediatric Registry SWEET. Diabetes Care 2021, 44, 1176–1184. [Google Scholar] [CrossRef]
- Rytter, K.; Schmidt, S.; Rasmussen, L.N.; Pedersen-Bjergaard, U.; Nørgaard, K. Education Programmes for Persons with Type 1 Diabetes Using an Insulin Pump: A Systematic Review. Diabetes. Metab. Res. Rev. 2021, 37, e3412. [Google Scholar] [CrossRef]
- Vashist, S.K. Non-Invasive Glucose Monitoring Technology in Diabetes Management: A Review. Anal. Chim. Acta 2012, 750, 16–27. [Google Scholar] [CrossRef]
- Alrezj, O.; Benaissa, M.; Alshebeili, S.A. Digital Bandstop Filtering in the Quantitative Analysis of Glucose from Near-Infrared and Midinfrared Spectra. J. Chemom. 2020, 34, e3206. [Google Scholar] [CrossRef]
- Khadem, H.; Nemat, H.; Elliott, J.; Benaissa, M. Signal Fragmentation Based Feature Vector Generation in a Model Agnostic Framework with Application to Glucose Quantification Using Absorption Spectroscopy. Talanta 2022, 243, 123379. [Google Scholar] [CrossRef]
- Khadem, H.; Eissa, M.R.; Nemat, H.; Alrezj, O.; Benaissa, M. Classification before Regression for Improving the Accuracy of Glucose Quantification Using Absorption Spectroscopy. Talanta 2020, 211, 120740. [Google Scholar] [CrossRef]
- Vettoretti, M.; Cappon, G.; Facchinetti, A.; Sparacino, G. Advanced Diabetes Management Using Artificial Intelligence and Continuous Glucose Monitoring Sensors. Sensors 2020, 20, 3870. [Google Scholar] [CrossRef]
- Nemat, H.; Khadem, H.; Elliott, J.; Benaissa, M. Causality Analysis in Type 1 Diabetes Mellitus with Application to Blood Glucose Level Prediction. Comput. Biol. Med. 2023, 153, 106535. [Google Scholar] [CrossRef]
- Xie, J.; Wang, Q. Benchmarking Machine Learning Algorithms on Blood Glucose Prediction for Type i Diabetes in Comparison with Classical Time-Series Models. IEEE Trans. Biomed. Eng. 2020, 67, 3101–3124. [Google Scholar] [CrossRef]
- Nemat, H.; Khadem, H.; Elliott, J.; Benaissa, M. Data Fusion of Activity and CGM for Predicting Blood Glucose Levels. In Knowledge Discovery in Healthcare Data 2020, Proceedings of the 5th International Workshop on Knowledge Discovery in Healthcare Data Co-Located with 24th European Conference on Artificial Intelligence (ECAI 2020), Santiago de Compostela, Spain (virtual), 29–30 August 2020; Bach, K., Bunescu, R., Marling, C., Wiratunga, N., Eds.; CEUR Workshop Proceedings: Aachen, Germany, 2020; Volume 2675, pp. 120–124. [Google Scholar]
- Woldaregay, A.Z.; Årsand, E.; Botsis, T.; Albers, D.; Mamykina, L.; Hartvigsen, G. Data-Driven Blood Glucose Pattern Classification and Anomalies Detection: Machine-Learning Applications in Type 1 Diabetes. J. Med. Internet Res. 2019, 21, e11030. [Google Scholar] [CrossRef]
- Khadem, H.; Nemat, H.; Elliott, J.; Benaissa, M. Multi-Lag Stacking for Blood Glucose Level Prediction. In Knowledge Discovery in Healthcare Data 2020, Proceedings of the 5th International Workshop on Knowledge Discovery in Healthcare Data Co-Located with 24th European Conference on Artificial Intelligence (ECAI 2020), Santiago de Compostela, Spain (virtual), 29–30 August 2020; Bach, K., Bunescu, R., Marling, C., Wiratunga, N., Eds.; CEUR Workshop Proceedings: Aachen, Germany, 2020; Volume 2675, pp. 146–150. [Google Scholar]
- Boughton, C.K.; Hovorka, R. Is an Artificial Pancreas (Closed-Loop System) for Type 1 Diabetes Effective? Diabet. Med. 2019, 36, 279–286. [Google Scholar] [CrossRef]
- Bremer, A.A.; Arreaza-Rubín, G. Analysis of “Artificial Pancreas (AP) Systems for People With Type 2 Diabetes: Conception and Design of the European CLOSE Project”. J. Diabetes Sci. Technol. 2019, 13, 268–270. [Google Scholar] [CrossRef]
- Woldaregay, A.Z.; Årsand, E.; Walderhaug, S.; Albers, D.; Mamykina, L.; Botsis, T.; Hartvigsen, G. Data-Driven Modeling and Prediction of Blood Glucose Dynamics: Machine Learning Applications in Type 1 Diabetes. Artif. Intell. Med. 2019, 98, 109–134. [Google Scholar] [CrossRef]
- Nemat, H.; Khadem, H.; Eissa, M.R.; Elliott, J.; Benaissa, M. Blood Glucose Level Prediction: Advanced Deep-Ensemble Learning Approach. IEEE J. Biomed. Health Inform. 2022, 26, 2758–2769. [Google Scholar] [CrossRef]
- Felizardo, V.; Garcia, N.M.; Pombo, N.; Megdiche, I. Data-Based Algorithms and Models Using Diabetics Real Data for Blood Glucose and Hypoglycaemia Prediction—A Systematic Literature Review. Artif. Intell. Med. 2021, 118, 102120. [Google Scholar] [CrossRef]
- Semenoglou, A.-A.; Spiliotis, E.; Assimakopoulos, V. Image-Based Time Series Forecasting: A Deep Convolutional Neural Network Approach. Neural Netw. 2023, 157, 39–53. [Google Scholar] [CrossRef]
- Garg, A.; Zhang, W.; Samaran, J.; Savitha, R.; Foo, C.S. An Evaluation of Anomaly Detection and Diagnosis in Multivariate Time Series. IEEE Trans. Neural Netw. Learn. Syst. 2022, 33, 2508–2517. [Google Scholar] [CrossRef]
- De Oliveira, J.F.L.; Silva, E.G.; De Mattos Neto, P.S.G. A Hybrid System Based on Dynamic Selection for Time Series Forecasting. IEEE Trans. Neural Netw. Learn. Syst. 2022, 33, 3251–3263. [Google Scholar] [CrossRef] [PubMed]
- Cichos, F.; Gustavsson, K.; Mehlig, B.; Volpe, G. Machine Learning for Active Matter. Nat. Mach. Intell. 2020, 2, 94–103. [Google Scholar] [CrossRef]
- Lim, B.; Zohren, S. Time-Series Forecasting with Deep Learning: A Survey. Philos. Trans. R. Soc. A 2021, 379, 20200209. [Google Scholar] [CrossRef]
- Ismail Fawaz, H.; Forestier, G.; Weber, J.; Idoumghar, L.; Muller, P.A. Deep Learning for Time Series Classification: A Review. Data Min. Knowl. Discov. 2019, 33, 917–963. [Google Scholar] [CrossRef]
- Zhu, T.; Wang, W.; Yu, M. A Novel Blood Glucose Time Series Prediction Framework Based on a Novel Signal Decomposition Method. Chaos Solitons Fractals 2022, 164, 112673. [Google Scholar] [CrossRef]
- Tejedor, M.; Woldaregay, A.Z.; Godtliebsen, F. Reinforcement Learning Application in Diabetes Blood Glucose Control: A Systematic Review. Artif. Intell. Med. 2020, 104, 101836. [Google Scholar] [CrossRef]
- Aiello, E.M.; Lisanti, G.; Magni, L.; Musci, M.; Toffanin, C. Therapy-Driven Deep Glucose Forecasting. Eng. Appl. Artif. Intell. 2020, 87, 103255. [Google Scholar] [CrossRef]
- Asad, M.; Qamar, U. A Review of Continuous Blood Glucose Monitoring and Prediction of Blood Glucose Level for Diabetes Type 1 Patient in Different Prediction Horizons (PH) Using Artificial Neural Network (ANN). Adv. Intell. Syst. Comput. 2020, 1038, 684–695. [Google Scholar] [CrossRef]
- Li, K.; Daniels, J.; Liu, C.; Herrero, P.; Georgiou, P. Convolutional Recurrent Neural Networks for Glucose Prediction. IEEE J. Biomed. Health Inform. 2020, 24, 603–613. [Google Scholar] [CrossRef]
- Zhang, M.; Flores, K.B.; Tran, H.T. Deep Learning and Regression Approaches to Forecasting Blood Glucose Levels for Type 1 Diabetes. Biomed. Signal Process. Control 2021, 69, 102923. [Google Scholar] [CrossRef]
- Tena, F.; Garnica, O.; Lanchares, J.; Hidalgo, J.I.; Cappon, G.; Herrero, P.; Sacchi, L.; Coltro, W. Ensemble Models of Cutting-Edge Deep Neural Networks for Blood Glucose Prediction in Patients with Diabetes. Sensors 2021, 21, 7090. [Google Scholar] [CrossRef]
- Wadghiri, M.Z.; Idri, A.; El Idrissi, T.; Hakkoum, H. Ensemble Blood Glucose Prediction in Diabetes Mellitus: A Review. Comput. Biol. Med. 2022, 147, 105674. [Google Scholar] [CrossRef]
- Daniels, J.; Herrero, P.; Georgiou, P. A Multitask Learning Approach to Personalized Blood Glucose Prediction. IEEE J. Biomed. Health Inform. 2022, 26, 436–445. [Google Scholar] [CrossRef]
- Yang, T.; Yu, X.; Ma, N.; Wu, R.; Li, H. An Autonomous Channel Deep Learning Framework for Blood Glucose Prediction. Appl. Soft Comput. 2022, 120, 108636. [Google Scholar] [CrossRef]
- Zhu, T.; Li, K.; Chen, J.; Herrero, P.; Georgiou, P. Dilated Recurrent Neural Networks for Glucose Forecasting in Type 1 Diabetes. J. Healthc. Inform. Res. 2020, 4, 308–324. [Google Scholar] [CrossRef]
- Martinsson, J.; Schliep, A.; Eliasson, B.; Mogren, O. Blood Glucose Prediction with Variance Estimation Using Recurrent Neural Networks. J. Healthc. Inform. Res. 2020, 4, 1–18. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, I.; Rodríguez, J.V.; Molina-García-Pardo, J.M.; Zamora-Izquierdo, M.Á.; Martínez-Inglés, M.T. A Comparison of Different Models of Glycemia Dynamics for Improved Type 1 Diabetes Mellitus Management with Advanced Intelligent Analysis in an Internet of Things Context. Appl. Sci. 2020, 10, 4381. [Google Scholar] [CrossRef]
- Marling, C.; Bunescu, R. The OhioT1DM Dataset for Blood Glucose Level Prediction: Update 2020. In Proceedings of the 5th International Workshop on Knowledge Discovery in Healthcare Data Co-Located with 24th European Conference on Artificial Intelligence, KDH@ECAI 2020, Santiago de Compostela, Spain & Virtually, 29–30 August 2020; NIH Public Access: Bethesda, MD, USA, 2020; Volume 2675, pp. 71–74. [Google Scholar]
- Kwiatkowski, D.; Phillips, P.C.B.; Schmidt, P.; Shin, Y. Testing the Null Hypothesis of Stationarity against the Alternative of a Unit Root: How Sure Are We That Economic Time Series Have a Unit Root? J. Econom. 1992, 54, 159–178. [Google Scholar] [CrossRef]
- Dickey, D.A.; Fuller, W.A. Distribution of the Estimators for Autoregressive Time Series with a Unit Root. J. Am. Stat. Assoc. 2012, 74, 427–431. [Google Scholar] [CrossRef]
- Sagi, O.; Rokach, L. Ensemble Learning: A Survey. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2018, 8, e1249. [Google Scholar] [CrossRef]
- Breiman, L. Stacked Regressions. Mach. Learn. 1996, 24, 49–64. [Google Scholar] [CrossRef]
- Zhu, Q. On the Performance of Matthews Correlation Coefficient (MCC) for Imbalanced Dataset. Pattern Recognit. Lett. 2020, 136, 71–80. [Google Scholar] [CrossRef]
- Klonoff, D.C.; Lias, C.; Vigersky, R.; Clarke, W.; Parkes, J.L.; Sacks, D.B.; Kirkman, M.S.; Kovatchev, B. The Surveillance Error Grid. J. Diabetes Sci. Technol. 2014, 8, 658–672. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M. A Comparison of Alternative Tests of Significance for the Problem of m Rankings on JSTOR. Ann. Math. Stat. 1940, 11, 86–92. [Google Scholar] [CrossRef]
- Fisher, R. Statistical Methods and Scientific Induction. J. R. Stat. Soc. Ser. B 1955, 17, 69–78. [Google Scholar] [CrossRef]
- Nemenyi, P.B. Distribution-Free Multiple Comparisons; Princeton University: Princeton, NJ, USA, 1963. [Google Scholar]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Demšar, J. Statistical Comparisons of Classifiers over Multiple Data Sets. J. Mach. Learn. Res. 2006, 7, 1–30. [Google Scholar]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009; ISBN 1441412697. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. Tensorflow: A System for Large-Scale Machine Learning. In Proceedings of the 12th Symposium on Operating Systems Design and Implementation, Savannah, GA, USA, 2–4 November 2016; pp. 265–283. [Google Scholar]
- McKinney, W. Data Structures for Statistical Computing in Python. In Proceedings of the the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; Volume 445, pp. 51–56. [Google Scholar]
- Harris, C.R.; Millman, K.J.; van der Walt, S.J.; Gommers, R.; Virtanen, P.; Cournapeau, D.; Wieser, E.; Taylor, J.; Berg, S.; Smith, N.J.; et al. Array Programming with {NumPy}. Nature 2020, 585, 357–362. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef]
- Seabold, S.; Perktold, J. Statsmodels: Econometric and Statistical Modeling with Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010. [Google Scholar]
- Terpilowski, M. Scikit-Posthocs: Pairwise Multiple Comparison Tests in Python. J. Open Source Softw. 2019, 4, 1169. [Google Scholar] [CrossRef]
- Benavoli, A.; Corani, G.; Mangili, F. Should We Really Use Post-Hoc Tests Based on Mean-Ranks? J. Mach. Learn. Res. 2016, 17, 152–161. [Google Scholar]


| Dataset | PID | Sex | Age | Set | Blood Glucose Data | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Count | Range (mg/dL) | Mean (mg/dL) | SD (mg/dL) | MR (%) | HOR (%) | ER (%) | HRR (%) | |||||
| 2018 | 559 | female | 40–60 | Train | 10,655 | 40–400 | 167.53 | 70.44 | 12.06 | 3.65 | 55.98 | 40.37 |
| Test | 2444 | 45–400 | 168.93 | 67.78 | 14.81 | 3.03 | 59.86 | 37.11 | ||||
| 563 | male | 40–60 | Train | 11,013 | 40–400 | 146.94 | 50.51 | 8.80 | 2.82 | 72.81 | 24.36 | |
| Test | 2569 | 62–313 | 167.38 | 46.15 | 4.71 | 0.70 | 60.45 | 38.85 | ||||
| 570 | male | 40–60 | Train | 10,981 | 46–377 | 187.5 | 62.33 | 5.73 | 1.97 | 42.97 | 55.07 | |
| Test | 2672 | 60–388 | 215.71 | 66.99 | 5.05 | 0.41 | 29.04 | 70.55 | ||||
| 575 | female | 40–60 | Train | 11,865 | 40–400 | 141.77 | 60.27 | 10.43 | 8.71 | 68.62 | 22.66 | |
| Test | 2589 | 40–342 | 150.49 | 60.53 | 4.94 | 5.37 | 63.50 | 31.13 | ||||
| 588 | female | 40–60 | Train | 12,639 | 40–400 | 164.99 | 50.51 | 3.69 | 1.04 | 63.56 | 35.40 | |
| Test | 2606 | 66–354 | 175.98 | 48.66 | 3.42 | 0.15 | 53.26 | 46.58 | ||||
| 591 | female | 40–60 | Train | 10,846 | 40–397 | 156.01 | 58.03 | 17.59 | 3.94 | 63.97 | 32.09 | |
| Test | 2759 | 43–291 | 144.83 | 51.42 | 3.15 | 5.18 | 67.27 | 27.55 | ||||
| 2020 | 540 | male | 20–40 | Train | 11,914 | 40–369 | 136.78 | 54.75 | 9.76 | 7.08 | 72.66 | 20.25 |
| Test | 2360 | 52–400 | 149.94 | 66.46 | 6.74 | 5.64 | 68.18 | 26.19 | ||||
| 544 | male | 40–60 | Train | 10,533 | 48–400 | 165.12 | 60.08 | 19.11 | 1.47 | 63.78 | 34.75 | |
| Test | 2715 | 62–335 | 156.48 | 54.14 | 15.47 | 1.22 | 68.29 | 30.50 | ||||
| 552 | male | 20–40 | Train | 8661 | 45–345 | 146.88 | 54.63 | 22.30 | 3.89 | 72.05 | 24.06 | |
| Test | 1792 | 47–305 | 138.11 | 50.23 | 85.71 | 3.57 | 80.02 | 16.41 | ||||
| 567 | female | 20–40 | Train | 10,750 | 40–400 | 154.43 | 60.88 | 24.91 | 6.75 | 63.40 | 29.84 | |
| Test | 2388 | 40–351 | 146.25 | 55.00 | 20.18 | 8.33 | 67.38 | 24.29 | ||||
| 584 | male | 40–60 | Train | 12,027 | 40–400 | 192.34 | 65.29 | 9.13 | 0.80 | 47.69 | 51.51 | |
| Test | 2661 | 41–400 | 170.48 | 60.76 | 12.40 | 1.01 | 61.86 | 37.13 | ||||
| 596 | male | 60–80 | Train | 10,858 | 40–367 | 147.17 | 49.34 | 25.35 | 2.08 | 73.99 | 23.93 | |
| Test | 2663 | 49–305 | 146.98 | 50.79 | 9.76 | 2.78 | 75.07 | 22.16 | ||||
| Dataset | PID | Learner | PH | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | ||||
| 2018 | 559 | MLP | 30 | 19.65 ± 0.06 | 13.56 ± 0.03 | 8.78 ± 0.03 | 90.75 ± 0.05 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 |
| 60 | 31.36 ± 0.06 | 22.78 ± 0.06 | 15.18 ± 0.07 | 76.30 ± 0.08 | 0.63 ± 0.00 | 0.79 ± 0.00 | 0.31 ± 0.00 | |||
| LSTM | 30 | 23.12 ± 0.43 | 16.60 ± 0.66 | 11.10 ± 0.63 | 87.19 ± 0.47 | 0.74 ± 0.01 | 0.86 ± 0.01 | 0.24 ± 0.01 | ||
| 60 | 36.08 ± 1.47 | 25.38 ± 0.84 | 16.62 ± 0.25 | 68.60 ± 2.56 | 0.59 ± 0.02 | 0.75 ± 0.01 | 0.34 ± 0.01 | |||
| 563 | MLP | 30 | 18.71 ± 0.05 | 13.46 ± 0.06 | 8.47 ± 0.04 | 82.97 ± 0.09 | 0.74 ± 0.00 | 0.91 ± 0.00 | 0.19 ± 0.00 | |
| 60 | 30.65 ± 0.01 | 21.69 ± 0.04 | 13.46 ± 0.04 | 54.36 ± 0.04 | 0.57 ± 0.01 | 0.81 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 21.59 ± 0.64 | 15.33 ± 0.45 | 9.69 ± 0.19 | 77.31 ± 1.34 | 0.72 ± 0.01 | 0.89 ± 0.00 | 0.22 ± 0.00 | ||
| 60 | 33.02 ± 0.62 | 24.13 ± 0.61 | 15.07 ± 0.18 | 47.03 ± 2.01 | 0.51 ± 0.01 | 0.75 ± 0.02 | 0.33 ± 0.01 | |||
| 570 | MLP | 30 | 17.44 ± 0.03 | 12.47 ± 0.03 | 6.38 ± 0.03 | 93.34 ± 0.03 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | |
| 60 | 29.00 ± 0.14 | 20.97 ± 0.13 | 10.73 ± 0.04 | 81.62 ± 0.18 | 0.79 ± 0.00 | 0.91 ± 0.00 | 0.20 ± 0.00 | |||
| LSTM | 30 | 22.92 ± 1.49 | 16.16 ± 1.15 | 8.04 ± 0.65 | 88.47 ± 1.52 | 0.81 ± 0.02 | 0.94 ± 0.01 | 0.15 ± 0.01 | ||
| 60 | 35.80 ± 1.50 | 26.75 ± 1.85 | 12.68 ± 0.43 | 71.95 ± 2.31 | 0.75 ± 0.00 | 0.88 ± 0.01 | 0.23 ± 0.01 | |||
| 575 | MLP | 30 | 24.12 ± 0.06 | 16.05 ± 0.10 | 11.43 ± 0.09 | 84.48 ± 0.07 | 0.73 ± 0.00 | 0.86 ± 0.00 | 0.24 ± 0.00 | |
| 60 | 35.63 ± 0.17 | 25.66 ± 0.20 | 18.91 ± 0.17 | 66.19 ± 0.32 | 0.57 ± 0.01 | 0.71 ± 0.00 | 0.38 ± 0.00 | |||
| LSTM | 30 | 27.20 ± 0.57 | 18.25 ± 0.45 | 13.14 ± 0.71 | 80.24 ± 0.82 | 0.69 ± 0.00 | 0.82 ± 0.02 | 0.28 ± 0.01 | ||
| 60 | 38.09 ± 0.03 | 27.47 ± 0.52 | 20.48 ± 1.20 | 61.36 ± 0.07 | 0.54 ± 0.02 | 0.70 ± 0.00 | 0.41 ± 0.01 | |||
| 588 | MLP | 30 | 18.07 ± 0.35 | 13.50 ± 0.15 | 8.29 ± 0.01 | 85.66 ± 0.56 | 0.76 ± 0.01 | 0.93 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 30.36 ± 0.11 | 22.68 ± 0.13 | 14.16 ± 0.12 | 59.60 ± 0.28 | 0.58 ± 0.00 | 0.77 ± 0.00 | 0.31 ± 0.00 | |||
| LSTM | 30 | 19.23 ± 0.11 | 14.16 ± 0.11 | 8.53 ± 0.12 | 83.77 ± 0.19 | 0.74 ± 0.00 | 0.92 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 30.46 ± 0.60 | 22.48 ± 0.39 | 14.04 ± 0.23 | 59.33 ± 1.61 | 0.60 ± 0.01 | 0.79 ± 0.01 | 0.30 ± 0.01 | |||
| 591 | MLP | 30 | 22.98 ± 0.11 | 16.61 ± 0.05 | 12.99 ± 0.03 | 80.32 ± 0.18 | 0.65 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | |
| 60 | 34.98 ± 0.05 | 26.93 ± 0.08 | 21.91 ± 0.13 | 54.41 ± 0.12 | 0.39 ± 0.00 | 0.65 ± 0.00 | 0.45 ± 0.00 | |||
| LSTM | 30 | 26.33 ± 0.42 | 19.55 ± 0.24 | 15.65 ± 0.40 | 74.16 ± 0.83 | 0.60 ± 0.00 | 0.75 ± 0.01 | 0.34 ± 0.01 | ||
| 60 | 36.51 ± 0.20 | 28.36 ± 0.26 | 23.32 ± 0.27 | 50.32 ± 0.54 | 0.37 ± 0.02 | 0.63 ± 0.00 | 0.47 ± 0.00 | |||
| 2020 | 540 | MLP | 30 | 22.88 ± 0.13 | 17.45 ± 0.10 | 12.71 ± 0.04 | 87.60 ± 0.14 | 0.68 ± 0.00 | 0.81 ± 0.00 | 0.27 ± 0.00 |
| 60 | 39.84 ± 0.14 | 30.49 ± 0.12 | 22.96 ± 0.13 | 62.48 ± 0.27 | 0.52 ± 0.00 | 0.66 ± 0.00 | 0.44 ± 0.00 | |||
| LSTM | 30 | 24.84 ± 0.42 | 18.48 ± 0.70 | 13.81 ± 1.24 | 85.37 ± 0.49 | 0.67 ± 0.02 | 0.80 ± 0.01 | 0.29 ± 0.02 | ||
| 60 | 41.36 ± 0.58 | 30.69 ± 0.37 | 22.40 ± 0.20 | 59.56 ± 1.12 | 0.50 ± 0.02 | 0.66 ± 0.00 | 0.44 ± 0.00 | |||
| 544 | MLP | 30 | 17.37 ± 0.03 | 12.14 ± 0.03 | 8.21 ± 0.03 | 88.26 ± 0.04 | 0.78 ± 0.00 | 0.92 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 28.49 ± 0.03 | 20.74 ± 0.04 | 14.16 ± 0.05 | 68.32 ± 0.07 | 0.63 ± 0.00 | 0.78 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 21.23 ± 0.53 | 15.00 ± 0.49 | 9.93 ± 0.35 | 82.45 ± 0.87 | 0.76 ± 0.01 | 0.89 ± 0.00 | 0.21 ± 0.01 | ||
| 60 | 30.45 ± 0.12 | 22.09 ± 0.45 | 14.81 ± 0.52 | 63.83 ± 0.29 | 0.59 ± 0.02 | 0.78 ± 0.01 | 0.31 ± 0.01 | |||
| 552 | MLP | 30 | 14.06 ± 0.03 | 8.25 ± 0.11 | 6.48 ± 0.09 | 86.18 ± 0.05 | 0.75 ± 0.00 | 0.92 ± 0.00 | 0.14 ± 0.00 | |
| 60 | 23.83 ± 0.03 | 14.57 ± 0.10 | 11.75 ± 0.12 | 60.36 ± 0.09 | 0.64 ± 0.00 | 0.84 ± 0.00 | 0.22 ± 0.00 | |||
| LSTM | 30 | 16.72 ± 0.44 | 10.31 ± 0.24 | 8.04 ± 0.22 | 80.45 ± 1.01 | 0.71 ± 0.02 | 0.90 ± 0.01 | 0.16 ± 0.01 | ||
| 60 | 25.47 ± 0.30 | 16.27 ± 0.24 | 13.02 ± 0.27 | 54.73 ± 1.05 | 0.61 ± 0.01 | 0.83 ± 0.01 | 0.24 ± 0.01 | |||
| 567 | MLP | 30 | 22.72 ± 0.04 | 16.47 ± 0.04 | 12.48 ± 0.03 | 84.80 ± 0.05 | 0.64 ± 0.00 | 0.80 ± 0.00 | 0.28 ± 0.00 | |
| 60 | 38.38 ± 0.02 | 29.51 ± 0.04 | 23.24 ± 0.06 | 56.68 ± 0.04 | 0.46 ± 0.00 | 0.64 ± 0.00 | 0.47 ± 0.00 | |||
| LSTM | 30 | 24.64 ± 0.97 | 17.85 ± 0.81 | 13.48 ± 0.66 | 82.10 ± 1.41 | 0.60 ± 0.01 | 0.78 ± 0.01 | 0.31 ± 0.01 | ||
| 60 | 40.13 ± 1.22 | 30.57 ± 1.14 | 25.05 ± 1.96 | 52.61 ± 2.86 | 0.45 ± 0.01 | 0.62 ± 0.02 | 0.50 ± 0.03 | |||
| 584 | MLP | 30 | 22.78 ± 0.04 | 16.92 ± 0.04 | 11.34 ± 0.03 | 85.49 ± 0.05 | 0.77 ± 0.00 | 0.87 ± 0.00 | 0.23 ± 0.00 | |
| 60 | 35.99 ± 0.05 | 27.29 ± 0.02 | 18.40 ± 0.03 | 63.67 ± 0.11 | 0.60 ± 0.00 | 0.72 ± 0.00 | 0.37 ± 0.00 | |||
| LSTM | 30 | 25.31 ± 1.32 | 18.27 ± 0.95 | 11.49 ± 0.52 | 82.05 ± 1.89 | 0.75 ± 0.01 | 0.86 ± 0.01 | 0.23 ± 0.01 | ||
| 60 | 41.45 ± 1.58 | 31.50 ± 1.91 | 21.43 ± 2.17 | 51.75 ± 3.64 | 0.55 ± 0.03 | 0.67 ± 0.04 | 0.42 ± 0.04 | |||
| 596 | MLP | 30 | 17.87 ± 0.08 | 12.89 ± 0.06 | 9.67 ± 0.03 | 86.99 ± 0.12 | 0.74 ± 0.00 | 0.89 ± 0.00 | 0.20 ± 0.00 | |
| 60 | 35.99 ± 0.05 | 27.29 ± 0.02 | 18.40 ± 0.03 | 63.67 ± 0.11 | 0.60 ± 0.00 | 0.72 ± 0.00 | 0.37 ± 0.00 | |||
| LSTM | 30 | 19.96 ± 0.28 | 14.31 ± 0.03 | 10.83 ± 0.18 | 83.78 ± 0.45 | 0.70 ± 0.01 | 0.87 ± 0.00 | 0.23 ± 0.00 | ||
| 60 | 30.28 ± 0.72 | 22.17 ± 0.71 | 16.97 ± 0.45 | 62.72 ± 1.77 | 0.56 ± 0.02 | 0.79 ± 0.00 | 0.32 ± 0.01 | |||
| Dataset | PID | Learner | PH | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | ||||
| 2018 | 559 | MLP | 30 | 19.00 ± 0.11 | 13.19 ± 0.08 | 8.79 ± 0.05 | 91.35 ± 0.10 | 0.78 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 |
| 60 | 31.25 ± 0.41 | 22.67 ± 0.22 | 15.22 ± 0.24 | 76.46 ± 0.61 | 0.64 ± 0.00 | 0.79 ± 0.00 | 0.31 ± 0.00 | |||
| LSTM | 30 | 22.90 ± 0.49 | 15.77 ± 0.17 | 9.97 ± 0.09 | 87.43 ± 0.54 | 0.76 ± 0.01 | 0.89 ± 0.00 | 0.21 ± 0.00 | ||
| 60 | 34.95 ± 0.17 | 24.99 ± 0.11 | 16.61 ± 0.05 | 70.56 ± 0.29 | 0.61 ± 0.01 | 0.76 ± 0.00 | 0.33 ± 0.00 | |||
| 563 | MLP | 30 | 18.54 ± 0.05 | 13.03 ± 0.03 | 8.10 ± 0.00 | 83.28 ± 0.08 | 0.74 ± 0.01 | 0.92 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 29.87 ± 0.18 | 21.22 ± 0.14 | 13.36 ± 0.04 | 56.67 ± 0.51 | 0.58 ± 0.01 | 0.81 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 21.25 ± 0.05 | 14.97 ± 0.06 | 9.38 ± 0.02 | 78.05 ± 0.11 | 0.73 ± 0.00 | 0.89 ± 0.00 | 0.21 ± 0.00 | ||
| 60 | 33.20 ± 0.16 | 23.55 ± 0.07 | 14.44 ± 0.02 | 46.46 ± 0.53 | 0.52 ± 0.00 | 0.78 ± 0.00 | 0.32 ± 0.00 | |||
| 570 | MLP | 30 | 17.49 ± 0.11 | 12.43 ± 0.10 | 6.36 ± 0.03 | 93.30 ± 0.09 | 0.86 ± 0.01 | 0.96 ± 0.00 | 0.12 ± 0.00 | |
| 60 | 28.65 ± 0.08 | 20.90 ± 0.07 | 10.91 ± 0.04 | 82.06 ± 0.10 | 0.78 ± 0.00 | 0.91 ± 0.00 | 0.20 ± 0.00 | |||
| LSTM | 30 | 21.58 ± 1.50 | 15.59 ± 1.55 | 7.70 ± 0.49 | 89.77 ± 1.44 | 0.84 ± 0.01 | 0.94 ± 0.00 | 0.14 ± 0.01 | ||
| 60 | 32.48 ± 0.69 | 23.55 ± 0.62 | 11.82 ± 0.06 | 76.93 ± 0.98 | 0.76 ± 0.00 | 0.89 ± 0.00 | 0.22 ± 0.00 | |||
| 575 | MLP | 30 | 24.21 ± 0.04 | 15.70 ± 0.09 | 11.25 ± 0.19 | 84.36 ± 0.05 | 0.74 ± 0.00 | 0.86 ± 0.00 | 0.24 ± 0.00 | |
| 60 | 36.42 ± 0.41 | 26.35 ± 0.77 | 19.85 ± 1.57 | 64.68 ± 0.79 | 0.57 ± 0.02 | 0.71 ± 0.00 | 0.40 ± 0.02 | |||
| LSTM | 30 | 27.73 ± 0.12 | 18.09 ± 0.09 | 12.67 ± 0.09 | 79.48 ± 0.18 | 0.66 ± 0.00 | 0.82 ± 0.00 | 0.27 ± 0.00 | ||
| 60 | 38.34 ± 0.09 | 27.48 ± 0.06 | 19.59 ± 0.12 | 60.86 ± 0.18 | 0.54 ± 0.00 | 0.68 ± 0.00 | 0.41 ± 0.00 | |||
| 588 | MLP | 30 | 18.24 ± 0.19 | 13.51 ± 0.12 | 8.17 ± 0.02 | 85.39 ± 0.30 | 0.75 ± 0.01 | 0.93 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 29.65 ± 0.21 | 21.84 ± 0.18 | 13.14 ± 0.08 | 61.46 ± 0.55 | 0.57 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | |||
| LSTM | 30 | 18.91 ± 0.08 | 14.03 ± 0.14 | 8.43 ± 0.25 | 84.30 ± 0.13 | 0.75 ± 0.00 | 0.92 ± 0.00 | 0.18 ± 0.01 | ||
| 60 | 30.67 ± 0.20 | 22.29 ± 0.25 | 13.54 ± 0.49 | 58.76 ± 0.54 | 0.60 ± 0.01 | 0.81 ± 0.01 | 0.29 ± 0.01 | |||
| 591 | MLP | 30 | 22.88 ± 0.07 | 16.60 ± 0.04 | 13.03 ± 0.06 | 80.49 ± 0.12 | 0.65 ± 0.00 | 0.80 ± 0.00 | 0.29 ± 0.00 | |
| 60 | 34.43 ± 0.06 | 26.80 ± 0.05 | 22.09 ± 0.09 | 55.84 ± 0.14 | 0.41 ± 0.00 | 0.65 ± 0.00 | 0.45 ± 0.00 | |||
| LSTM | 30 | 25.51 ± 0.01 | 18.80 ± 0.05 | 14.79 ± 0.08 | 75.73 ± 0.03 | 0.59 ± 0.00 | 0.76 ± 0.00 | 0.33 ± 0.00 | ||
| 60 | 36.68 ± 0.16 | 28.44 ± 0.05 | 23.78 ± 0.03 | 49.87 ± 0.44 | 0.42 ± 0.00 | 0.64 ± 0.00 | 0.47 ± 0.00 | |||
| 2020 | 540 | MLP | 30 | 22.34 ± 0.02 | 17.13 ± 0.03 | 12.58 ± 0.03 | 88.18 ± 0.02 | 0.68 ± 0.00 | 0.82 ± 0.00 | 0.27 ± 0.00 |
| 60 | 39.40 ± 0.09 | 30.32 ± 0.13 | 22.95 ± 0.10 | 63.29 ± 0.17 | 0.52 ± 0.00 | 0.66 ± 0.00 | 0.44 ± 0.00 | |||
| LSTM | 30 | 24.13 ± 0.14 | 18.24 ± 0.06 | 13.57 ± 0.03 | 86.20 ± 0.17 | 0.66 ± 0.00 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 60 | 40.86 ± 0.05 | 30.62 ± 0.11 | 23.06 ± 0.18 | 60.53 ± 0.09 | 0.51 ± 0.00 | 0.66 ± 0.00 | 0.44 ± 0.00 | |||
| 544 | MLP | 30 | 16.96 ± 0.02 | 12.01 ± 0.05 | 8.14 ± 0.08 | 88.81 ± 0.03 | 0.79 ± 0.00 | 0.92 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 28.36 ± 0.17 | 20.72 ± 0.04 | 14.21 ± 0.08 | 68.62 ± 0.37 | 0.64 ± 0.00 | 0.78 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 20.85 ± 0.25 | 14.84 ± 0.20 | 10.01 ± 0.14 | 83.08 ± 0.40 | 0.73 ± 0.00 | 0.88 ± 0.00 | 0.22 ± 0.00 | ||
| 60 | 31.30 ± 0.23 | 22.55 ± 0.10 | 15.44 ± 0.07 | 61.77 ± 0.57 | 0.59 ± 0.00 | 0.76 ± 0.00 | 0.33 ± 0.00 | |||
| 552 | MLP | 30 | 14.19 ± 0.03 | 9.00 ± 0.06 | 7.10 ± 0.03 | 85.92 ± 0.05 | 0.72 ± 0.00 | 0.91 ± 0.00 | 0.15 ± 0.00 | |
| 60 | 23.78 ± 0.04 | 15.52 ± 0.20 | 12.62 ± 0.18 | 60.53 ± 0.14 | 0.61 ± 0.01 | 0.84 ± 0.00 | 0.23 ± 0.00 | |||
| LSTM | 30 | 17.65 ± 0.22 | 11.92 ± 0.20 | 9.79 ± 0.21 | 78.23 ± 0.53 | 0.69 ± 0.00 | 0.88 ± 0.01 | 0.19 ± 0.01 | ||
| 60 | 26.93 ± 0.23 | 17.97 ± 0.17 | 15.04 ± 0.14 | 49.39 ± 0.85 | 0.58 ± 0.01 | 0.78 ± 0.00 | 0.28 ± 0.00 | |||
| 567 | MLP | 30 | 22.67 ± 0.22 | 16.17 ± 0.22 | 12.39 ± 0.21 | 84.86 ± 0.29 | 0.64 ± 0.01 | 0.81 ± 0.00 | 0.28 ± 0.00 | |
| 60 | 37.82 ± 0.24 | 28.14 ± 0.18 | 22.42 ± 0.23 | 57.94 ± 0.52 | 0.48 ± 0.00 | 0.66 ± 0.00 | 0.46 ± 0.00 | |||
| LSTM | 30 | 23.74 ± 0.09 | 16.86 ± 0.14 | 12.96 ± 0.14 | 83.41 ± 0.13 | 0.62 ± 0.00 | 0.79 ± 0.00 | 0.30 ± 0.00 | ||
| 60 | 38.75 ± 0.41 | 29.24 ± 0.31 | 23.40 ± 0.46 | 55.84 ± 0.92 | 0.47 ± 0.01 | 0.64 ± 0.01 | 0.48 ± 0.01 | |||
| 584 | MLP | 30 | 21.89 ± 0.09 | 15.96 ± 0.14 | 10.64 ± 0.13 | 86.60 ± 0.11 | 0.77 ± 0.00 | 0.89 ± 0.00 | 0.22 ± 0.00 | |
| 60 | 35.42 ± 0.42 | 26.73 ± 0.52 | 17.97 ± 0.53 | 64.79 ± 0.83 | 0.60 ± 0.01 | 0.73 ± 0.01 | 0.36 ± 0.01 | |||
| LSTM | 30 | 24.79 ± 0.06 | 18.21 ± 0.08 | 12.51 ± 0.13 | 82.82 ± 0.08 | 0.76 ± 0.00 | 0.86 ± 0.00 | 0.25 ± 0.00 | ||
| 60 | 38.65 ± 0.29 | 29.33 ± 0.12 | 20.14 ± 0.01 | 58.09 ± 0.63 | 0.60 ± 0.00 | 0.70 ± 0.00 | 0.39 ± 0.00 | |||
| 596 | MLP | 30 | 17.76 ± 0.09 | 12.85 ± 0.09 | 9.71 ± 0.11 | 87.16 ± 0.13 | 0.75 ± 0.00 | 0.90 ± 0.00 | 0.20 ± 0.00 | |
| 60 | 28.80 ± 0.19 | 21.37 ± 0.13 | 16.53 ± 0.11 | 66.29 ± 0.44 | 0.59 ± 0.01 | 0.80 ± 0.00 | 0.31 ± 0.00 | |||
| LSTM | 30 | 19.06 ± 0.16 | 13.55 ± 0.08 | 10.27 ± 0.06 | 85.21 ± 0.24 | 0.72 ± 0.00 | 0.88 ± 0.00 | 0.22 ± 0.00 | ||
| 60 | 30.01 ± 0.10 | 22.25 ± 0.10 | 17.31 ± 0.16 | 63.39 ± 0.25 | 0.56 ± 0.00 | 0.80 ± 0.00 | 0.32 ± 0.00 | |||
| Dataset | PID | Learner | PH | Evaluation Metric | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RMSE ± SD (mg/dL) | MAE ± SD (mg/dL) | MAPE ± SD (%) | r2 ± SD (%) | MCC ± SD (%) | SE < 0.5 ± SD (%) | ASE ± SD | ||||
| 2018 | 559 | MLP | 30 | 19.67 ± 0.05 | 13.54 ± 0.05 | 8.89 ± 0.03 | 90.72 ± 0.05 | 0.79 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 |
| 60 | 33.44 ± 0.28 | 23.54 ± 0.16 | 15.27 ± 0.04 | 73.05 ± 0.46 | 0.63 ± 0.00 | 0.78 ± 0.00 | 0.31 ± 0.00 | |||
| LSTM | 30 | 19.69 ± 0.19 | 13.51 ± 0.18 | 8.83 ± 0.17 | 90.71 ± 0.18 | 0.79 ± 0.00 | 0.90 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 33.93 ± 0.48 | 23.82 ± 0.28 | 15.31 ± 0.05 | 72.25 ± 0.79 | 0.63 ± 0.01 | 0.78 ± 0.00 | 0.31 ± 0.00 | |||
| 563 | MLP | 30 | 18.85 ± 0.10 | 13.15 ± 0.08 | 8.27 ± 0.02 | 82.72 ± 0.19 | 0.76 ± 0.01 | 0.91 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 31.82 ± 0.54 | 22.38 ± 0.38 | 13.84 ± 0.11 | 50.81 ± 1.66 | 0.55 ± 0.01 | 0.80 ± 0.01 | 0.30 ± 0.00 | |||
| LSTM | 30 | 19.00 ± 0.07 | 13.24 ± 0.06 | 8.31 ± 0.03 | 82.44 ± 0.13 | 0.76 ± 0.01 | 0.91 ± 0.00 | 0.19 ± 0.00 | ||
| 60 | 31.65 ± 0.51 | 22.37 ± 0.61 | 13.79 ± 0.10 | 51.35 ± 1.59 | 0.55 ± 0.03 | 0.80 ± 0.01 | 0.31 ± 0.01 | |||
| 570 | MLP | 30 | 18.34 ± 0.11 | 12.85 ± 0.08 | 6.58 ± 0.05 | 92.64 ± 0.09 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | |
| 60 | 31.09 ± 0.28 | 22.21 ± 0.14 | 11.54 ± 0.03 | 78.88 ± 0.38 | 0.77 ± 0.00 | 0.89 ± 0.00 | 0.21 ± 0.00 | |||
| LSTM | 30 | 18.57 ± 0.22 | 13.11 ± 0.12 | 6.65 ± 0.08 | 92.45 ± 0.18 | 0.86 ± 0.00 | 0.96 ± 0.00 | 0.12 ± 0.00 | ||
| 60 | 31.61 ± 0.60 | 22.60 ± 0.54 | 11.53 ± 0.02 | 78.16 ± 0.84 | 0.77 ± 0.00 | 0.90 ± 0.00 | 0.21 ± 0.00 | |||
| 575 | MLP | 30 | 26.18 ± 0.09 | 16.60 ± 0.19 | 12.40 ± 0.27 | 81.71 ± 0.12 | 0.73 ± 0.00 | 0.84 ± 0.00 | 0.26 ± 0.01 | |
| 60 | 36.98 ± 0.33 | 26.43 ± 0.50 | 19.46 ± 1.39 | 63.57 ± 0.65 | 0.54 ± 0.01 | 0.70 ± 0.01 | 0.40 ± 0.02 | |||
| LSTM | 30 | 26.01 ± 0.91 | 16.47 ± 0.32 | 12.02 ± 0.66 | 81.93 ± 1.25 | 0.73 ± 0.00 | 0.84 ± 0.01 | 0.25 ± 0.01 | ||
| 60 | 37.05 ± 0.62 | 26.29 ± 0.28 | 18.96 ± 0.13 | 63.44 ± 1.22 | 0.54 ± 0.00 | 0.70 ± 0.00 | 0.39 ± 0.00 | |||
| 588 | MLP | 30 | 18.50 ± 0.11 | 13.63 ± 0.08 | 8.11 ± 0.05 | 84.98 ± 0.17 | 0.74 ± 0.00 | 0.93 ± 0.00 | 0.18 ± 0.00 | |
| 60 | 29.43 ± 0.07 | 21.42 ± 0.17 | 13.01 ± 0.42 | 62.05 ± 0.17 | 0.62 ± 0.00 | 0.82 ± 0.01 | 0.28 ± 0.01 | |||
| LSTM | 30 | 18.26 ± 0.14 | 13.56 ± 0.27 | 8.23 ± 0.32 | 85.37 ± 0.22 | 0.76 ± 0.01 | 0.93 ± 0.00 | 0.18 ± 0.01 | ||
| 60 | 29.54 ± 0.28 | 21.33 ± 0.21 | 12.84 ± 0.09 | 61.77 ± 0.74 | 0.62 ± 0.01 | 0.82 ± 0.00 | 0.27 ± 0.00 | |||
| 591 | MLP | 30 | 23.07 ± 0.09 | 16.48 ± 0.04 | 12.89 ± 0.06 | 80.16 ± 0.15 | 0.64 ± 0.01 | 0.80 ± 0.00 | 0.29 ± 0.00 | |
| 60 | 35.68 ± 0.11 | 27.65 ± 0.08 | 23.12 ± 0.07 | 52.56 ± 0.29 | 0.42 ± 0.00 | 0.65 ± 0.00 | 0.46 ± 0.00 | |||
| LSTM | 30 | 23.08 ± 0.10 | 16.52 ± 0.07 | 12.98 ± 0.08 | 80.14 ± 0.17 | 0.63 ± 0.00 | 0.80 ± 0.00 | 0.29 ± 0.00 | ||
| 60 | 35.68 ± 0.21 | 27.69 ± 0.12 | 23.16 ± 0.08 | 52.57 ± 0.55 | 0.42 ± 0.00 | 0.65 ± 0.01 | 0.46 ± 0.00 | |||
| 2020 | 540 | MLP | 30 | 22.36 ± 0.03 | 16.96 ± 0.05 | 12.59 ± 0.03 | 88.15 ± 0.03 | 0.67 ± 0.00 | 0.82 ± 0.00 | 0.27 ± 0.00 |
| 60 | 38.81 ± 0.26 | 29.34 ± 0.14 | 22.04 ± 0.10 | 64.38 ± 0.47 | 0.53 ± 0.01 | 0.68 ± 0.00 | 0.43 ± 0.00 | |||
| LSTM | 30 | 22.39 ± 0.11 | 16.99 ± 0.09 | 12.61 ± 0.08 | 88.12 ± 0.12 | 0.67 ± 0.01 | 0.81 ± 0.00 | 0.27 ± 0.00 | ||
| 60 | 38.74 ± 0.18 | 29.32 ± 0.18 | 22.05 ± 0.15 | 64.52 ± 0.33 | 0.53 ± 0.01 | 0.68 ± 0.00 | 0.43 ± 0.00 | |||
| 544 | MLP | 30 | 16.86 ± 0.11 | 11.89 ± 0.06 | 8.02 ± 0.06 | 88.94 ± 0.14 | 0.78 ± 0.00 | 0.92 ± 0.00 | 0.17 ± 0.00 | |
| 60 | 28.92 ± 0.14 | 20.88 ± 0.05 | 14.33 ± 0.02 | 67.36 ± 0.31 | 0.63 ± 0.00 | 0.77 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 16.96 ± 0.15 | 11.95 ± 0.11 | 8.07 ± 0.09 | 88.80 ± 0.19 | 0.78 ± 0.01 | 0.92 ± 0.00 | 0.18 ± 0.00 | ||
| 60 | 28.84 ± 0.19 | 20.81 ± 0.10 | 14.34 ± 0.13 | 67.54 ± 0.42 | 0.63 ± 0.00 | 0.77 ± 0.00 | 0.30 ± 0.00 | |||
| 552 | MLP | 30 | 13.87 ± 0.16 | 8.88 ± 0.32 | 7.07 ± 0.24 | 86.56 ± 0.32 | 0.72 ± 0.01 | 0.92 ± 0.00 | 0.15 ± 0.01 | |
| 60 | 24.61 ± 0.11 | 16.04 ± 0.36 | 13.43 ± 0.30 | 57.73 ± 0.38 | 0.60 ± 0.00 | 0.82 ± 0.00 | 0.25 ± 0.00 | |||
| LSTM | 30 | 13.86 ± 0.02 | 9.00 ± 0.06 | 7.13 ± 0.06 | 86.58 ± 0.03 | 0.72 ± 0.00 | 0.92 ± 0.00 | 0.15 ± 0.00 | ||
| 60 | 23.97 ± 0.44 | 15.47 ± 0.32 | 12.76 ± 0.38 | 59.91 ± 1.47 | 0.61 ± 0.00 | 0.83 ± 0.01 | 0.24 ± 0.01 | |||
| 567 | MLP | 30 | 21.81 ± 0.28 | 15.58 ± 0.14 | 11.71 ± 0.30 | 86.00 ± 0.35 | 0.65 ± 0.01 | 0.82 ± 0.01 | 0.27 ± 0.01 | |
| 60 | 37.50 ± 0.18 | 27.95 ± 0.13 | 21.97 ± 0.18 | 58.65 ± 0.39 | 0.49 ± 0.00 | 0.66 ± 0.00 | 0.46 ± 0.00 | |||
| LSTM | 30 | 22.02 ± 0.07 | 15.70 ± 0.05 | 11.96 ± 0.07 | 85.72 ± 0.08 | 0.64 ± 0.00 | 0.82 ± 0.00 | 0.27 ± 0.00 | ||
| 60 | 37.77 ± 0.25 | 28.19 ± 0.22 | 22.38 ± 0.36 | 58.05 ± 0.55 | 0.48 ± 0.00 | 0.66 ± 0.00 | 0.46 ± 0.00 | |||
| 584 | MLP | 30 | 22.35 ± 0.58 | 16.74 ± 0.67 | 11.54 ± 0.54 | 86.03 ± 0.73 | 0.77 ± 0.01 | 0.88 ± 0.01 | 0.24 ± 0.01 | |
| 60 | 35.77 ± 0.49 | 27.25 ± 0.49 | 18.79 ± 0.44 | 64.11 ± 0.99 | 0.61 ± 0.01 | 0.73 ± 0.01 | 0.37 ± 0.01 | |||
| LSTM | 30 | 22.19 ± 0.11 | 16.54 ± 0.17 | 11.38 ± 0.17 | 86.24 ± 0.13 | 0.77 ± 0.00 | 0.88 ± 0.00 | 0.23 ± 0.00 | ||
| 60 | 36.02 ± 0.06 | 27.37 ± 0.12 | 18.91 ± 0.14 | 63.60 ± 0.12 | 0.61 ± 0.00 | 0.72 ± 0.00 | 0.37 ± 0.00 | |||
| 596 | MLP | 30 | 17.78 ± 0.24 | 12.67 ± 0.13 | 9.52 ± 0.10 | 87.13 ± 0.35 | 0.74 ± 0.00 | 0.89 ± 0.00 | 0.20 ± 0.00 | |
| 60 | 28.54 ± 0.24 | 20.79 ± 0.09 | 15.74 ± 0.27 | 66.89 ± 0.55 | 0.58 ± 0.02 | 0.81 ± 0.00 | 0.30 ± 0.00 | |||
| LSTM | 30 | 17.57 ± 0.25 | 12.49 ± 0.14 | 9.35 ± 0.09 | 87.43 ± 0.36 | 0.75 ± 0.01 | 0.89 ± 0.00 | 0.20 ± 0.00 | ||
| 60 | 28.68 ± 0.37 | 20.97 ± 0.07 | 15.96 ± 0.31 | 66.55 ± 0.87 | 0.58 ± 0.02 | 0.81 ± 0.00 | 0.31 ± 0.00 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khadem, H.; Nemat, H.; Elliott, J.; Benaissa, M. Blood Glucose Level Time Series Forecasting: Nested Deep Ensemble Learning Lag Fusion. Bioengineering 2023, 10, 487. https://doi.org/10.3390/bioengineering10040487
Khadem H, Nemat H, Elliott J, Benaissa M. Blood Glucose Level Time Series Forecasting: Nested Deep Ensemble Learning Lag Fusion. Bioengineering. 2023; 10(4):487. https://doi.org/10.3390/bioengineering10040487
Chicago/Turabian StyleKhadem, Heydar, Hoda Nemat, Jackie Elliott, and Mohammed Benaissa. 2023. "Blood Glucose Level Time Series Forecasting: Nested Deep Ensemble Learning Lag Fusion" Bioengineering 10, no. 4: 487. https://doi.org/10.3390/bioengineering10040487
APA StyleKhadem, H., Nemat, H., Elliott, J., & Benaissa, M. (2023). Blood Glucose Level Time Series Forecasting: Nested Deep Ensemble Learning Lag Fusion. Bioengineering, 10(4), 487. https://doi.org/10.3390/bioengineering10040487