

Bipedal Static Supination and Dynamic Forefoot Loading Characteristics in Taiwanese College Badminton Players: A Cross-Sectional Study


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Equipment
2.3. Plantar Pressure Assessment
2.4. Plantar Pressure Data Analysis
2.5. Rearfoot Postural Assessment
2.6. Statistical Analysis
3. Results and Discussion
3.1. Arch Index
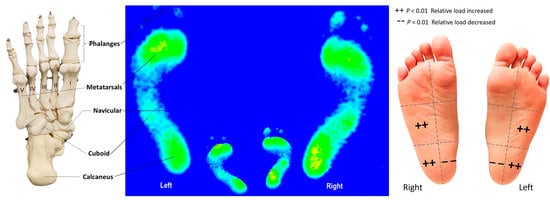
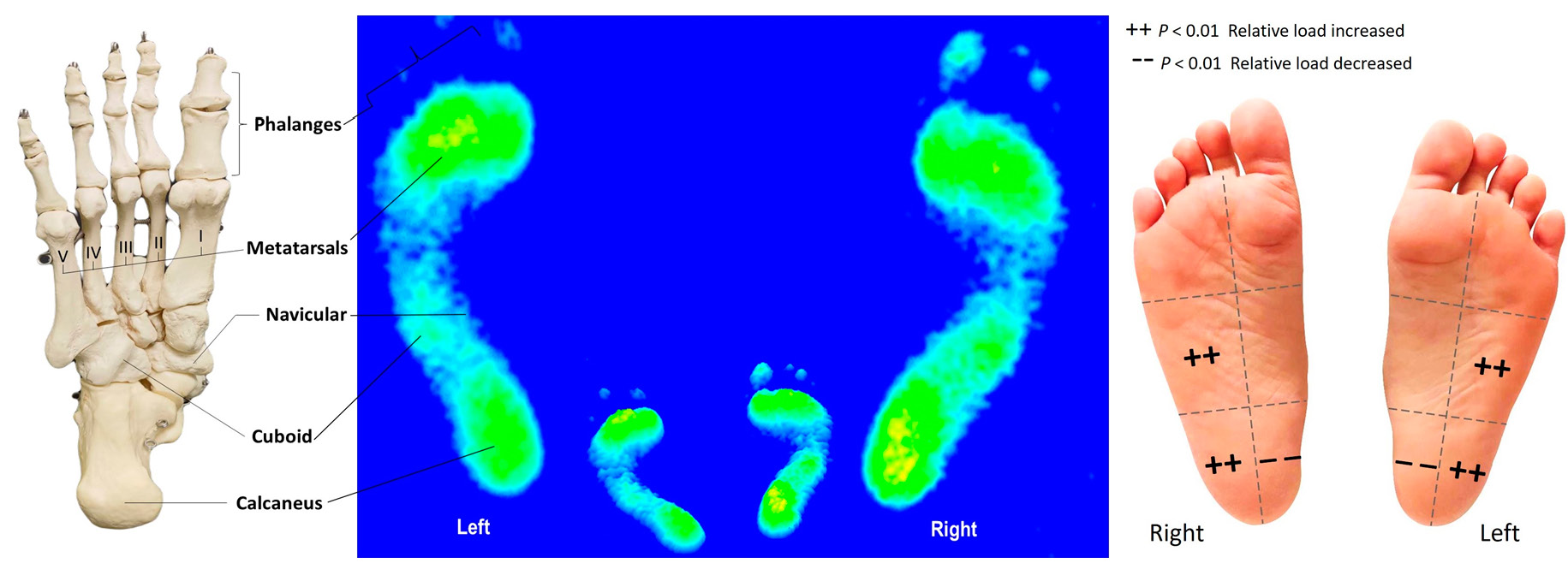
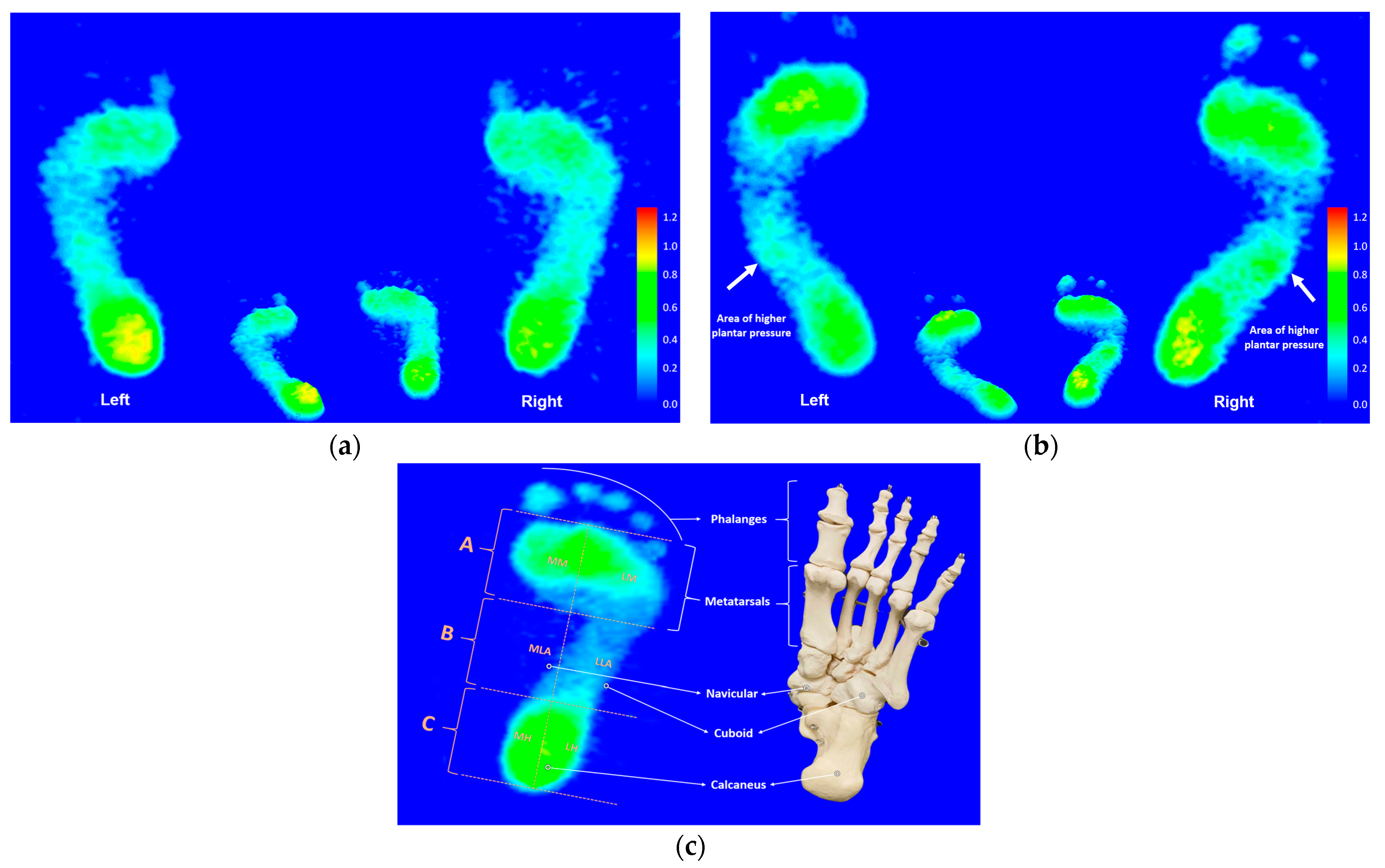
3.2. Three Regional Plantar Pressure Distributions under Static and Dynamic States
3.3. Six Subregional Plantar Pressure Distributions under Static and Dynamic States
3.4. Centers of Gravity Balance
3.5. Rearfoot Postural Alignment
3.6. Static Footprint Characteristics
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lam, W.K.; Wong, D.W.; Lee, W.C. Biomechanics of lower limb in badminton lunge: A systematic scoping review. Peer J. 2020, 8, e10300. [Google Scholar] [CrossRef] [PubMed]
- Phomsoupha, M.; Laffaye, G. The science of badminton: Game characteristics, anthropometry, physiology, visual fitness and biomechanics. Sport. Med. 2015, 45, 473–495. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Li, J.X.; Hong, Y.; Wang, L. Characteristics of plantar loads in maximum forward lunge tasks in badminton. PLoS ONE 2015, 10, e0137558. [Google Scholar] [CrossRef]
- Habelt, S.; Hasler, C.C.; Steinbrück, K.; Majewski, M. Sport injuries in adolescents. Orthop. Rev. 2011, 3, e18. [Google Scholar]
- Reeves, J.; Hume, P.A.; Gianotti, S.; Wilson, B.; Ikeda, E. A retrospective review from 2006 to 2011 of lower extremity injuries in badminton in New Zealand. Sports 2015, 3, 77–86. [Google Scholar] [CrossRef]
- Sighamoney, R.; Kad, R.; Yeole, U.L. Effect of core strengthening on dynamic balance and agility in badminton players. Int. J. Phys. Educ. Sport. Health 2018, 5, 86–88. [Google Scholar]
- Zhao, W.; Wang, C.; Bi, Y.; Chen, L. Effect of integrative neuromuscular training for injury prevention and sports performance of female badminton players. BioMed Res. Int. 2021, 2021, 5555853. [Google Scholar] [CrossRef] [PubMed]
- Lewson, E.B.; Pulsifer, M.S.E.; Mallette, J.P. Cuboid sling: A novel surgical repair of cuboid syndrome and literature review. Foot Ankle Surg. Tech. Rep. Cases 2021, 1, 100108. [Google Scholar] [CrossRef]
- Marshall, P.; Hamilton, W.G. Cuboid subluxation in ballet dancers. Am. J. Sport. Med. 1992, 20, 169–175. [Google Scholar] [CrossRef]
- Babu, D.; Bordoni, B. Anatomy, Bony Pelvis and Lower Limb, Medial Longitudinal Arch of the Foot; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Nagano, K.; Okuyama, R.; Taniguchi, N.; Yoshida, T. Gender difference in factors affecting the medial longitudinal arch height of the foot in healthy young adults. J. Phys. Ther. Sci. 2018, 30, 675–679. [Google Scholar] [CrossRef]
- Koldenhoven, R.M.; Feger, M.A.; Fraser, J.J.; Saliba, S.; Hertel, J. Surface electromyography and plantar pressure during walking in young adults with chronic ankle instability. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.D.; Elis, E.D.; Kernozek, T.W. Plantar loading characteristics during walking in females with and without patellofemoral pain. J. Am. Podiatr. Med. Assoc. 2015, 105, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Persiane, A.S.; Negrão, D.M.G.; Alves, R.D.P. Subtalar joint in neutral and relaxed positions for evaluation of medial longitudinal arch. Acta Ortop. Bras. 2021, 29, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, M.B.; Abián-Vicén, J.; Halstead, J.; Gijon-Nogueron, G. Effectiveness of neuromuscular taping on pronated foot posture and walking plantar pressures in amateur runners. J. Sci. Med. Sport 2016, 19, 348–353. [Google Scholar] [CrossRef]
- Lee, S.Y.; Hertel, J.; Lee, S.C. Rearfoot eversion has indirect effects on plantar fascia tension by changing the amount of arch collapse. Foot 2010, 20, 64–70. [Google Scholar] [CrossRef]
- McCrory, J.L.; Young, M.J.; Boulton, A.J.M.; Diamond, J.E. Arch index as a predictor of arch height. Foot 1997, 7, 79–81. [Google Scholar] [CrossRef]
- Mickle, K.J.; Steele, J.R.; Munro, B.J. The feet of overweight and obese young children: Are they flat or fat? Obesity 2006, 14, 1949–1953. [Google Scholar] [CrossRef]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Wearing, S.C.; Hills, A.P.; Byrne, N.M.; Hennig, E.M.; McDonald, M. The arch index: A measure of flat or fat feet? Foot Ankle Int. 2004, 25, 575–581. [Google Scholar] [CrossRef]
- Imhauser, C.W.; Siegler, S.; Abidi, N.A.; Frankel, D.Z. The effect of posterior tibialis tendon dysfunction on the plantar pressure characteristics and the kinematics of the arch and hindfoot. Clin. Biomech. 2004, 19, 161–169. [Google Scholar] [CrossRef]
- Ribeiro, A.P.; Sacco, I.C.; Dinato, R.C.; João, S.M. Relationships between static foot alignment and dynamic plantar loads in runners with acute and chronic stages of plantar fasciitis: A cross-sectional study. Braz. J. Phys. Ther. 2016, 20, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Birinci, T.; Demirbas, S.B. Relationship between the mobility of medial longitudinal arch and postural control. Acta Orthop. Et Traumatol. Turc. 2017, 51, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Koshino, Y.; Samukawa, M.; Chida, S.; Okada, S.; Tanaka, H.; Watanabe, K.; Chijimatsu, M.; Yamanaka, M.; Tohyama, H. Postural stability and muscle activation onset during double- to single-leg stance transition in flat-footed individuals. J. Sport. Sci. Med. 2020, 19, 662–669. [Google Scholar]
- Carroll, L.A.; Paulseth, S.; Martin, R.L. Forefoot injuries in athletes: Integration of the movement system. Int. J. Sport. Phys. Ther. 2022, 17, 81–89. [Google Scholar] [CrossRef]
- Woźniacka, R.; Oleksy, Ł.; Jankowicz-Szymańska, A.; Mika, A.; Kielnar, R.; Stolarczyk, A. The association between high-arched feet, plantar pressure distribution and body posture in young women. Sci. Rep. 2019, 9, 17187. [Google Scholar] [CrossRef] [PubMed]
- Truong, P.; You, S.; Ji, S.H.; Jeong, G.M. Adaptive accumulation of plantar pressure for ambulatory activity recognition and pedestrian identification. Sensors 2021, 21, 3842. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, W.; Chen, G.; Ji, A.; Song, Y. Effects of standing and walking on plantar pressure distribution in recreational runners before and after long-distance running. J. Biomech. 2021, 129, 110779. [Google Scholar] [CrossRef]
- Lung, C.W.; Liau, B.Y.; Peters, J.A.; He, L.; Townsend, R.; Jan, Y.K. Effects of various walking intensities on leg muscle fatigue and plantar pressure distributions. BMC Musculoskelet. Disord. 2021, 22, 831. [Google Scholar] [CrossRef]
- Rice, H.; Nunns, M.; House, C.; Fallowfield, J.; Allsopp, A.; Dixon, S. A narrow bimalleolar width is a risk factor for ankle inversion injury in male military recruits: A prospective study. Clin. Biomech. 2017, 41, 14–19. [Google Scholar] [CrossRef]
- Monteiro, R.L.; Sartor, C.D.; Ferreira, J.S.S.P.; Dantas, M.G.B.; Bus, S.A.; Sacco, I.C.N. Protocol for evaluating the effects of a foot-ankle therapeutic exercise program on daily activity, foot-ankle functionality, and biomechanics in people with diabetic polyneuropathy: A randomized controlled trial. BMC Musculoskelet. Disord. 2018, 19, 400. [Google Scholar] [CrossRef]
- Helili, M.; Geng, X.; Ma, X.; Chen, W.; Zhang, C.; Huang, J.; Wang, X. An investigation of regional plantar soft tissue hard-ness and its potential correlation with plantar pressure distribution in healthy adults. Appl. Bionics Biomech. 2021, 2021, 5566036. [Google Scholar] [CrossRef] [PubMed]
- Chuter, V.H.; Spink, M.J.; David, M.; Lanting, S.; Searle, A. Clinical foot measurements as a proxy for plantar pressure testing in people with diabetes. J. Foot Ankle Res. 2021, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Lu, Q. A current review of foot disorder and plantar pressure alternation in the Elderly. Phys. Act. Healthy 2020, 4, 95–106. [Google Scholar] [CrossRef]
- Hollander, K.; Zech, A.; Rahlf, A.L.; Orendurff, M.S.; Stebbins, J.; Heidt, C. The relationship between static and dynamic foot posture and running biomechanics: A systematic review and meta-analysis. Gait Posture 2019, 72, 109–122. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Wang, J.C. Characteristics of plantar pressures and related pain profiles in elite sprinters and recreational runners. J. Am. Podiatr. Med. Assoc. 2018, 108, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Tsai, W.C.; Lin, M.H. Plantar pressure profiles and possible foot syndromes of Taiwanese college elite basketball players. J. Am. Podiatr. Med. Assoc. 2021, 111, 5. [Google Scholar] [CrossRef] [PubMed]
- Chow, T.H.; Chen, Y.S.; Hsu, C.C.; Hsu, C.H. Characteristics of the plantar pressure with foot postures and lower limb pain profiles in the Taiwanese college elite rugby league athletes. Int. J. Environ. Res. Public Health 2022, 19, 1158. [Google Scholar] [CrossRef]
- Chow, T.H.; Chen, Y.S.; Hsu, C.C. Relationships between plantar pressure distribution and rearfoot alignment in the Taiwanese college athletes with plantar fasciopathy during static standing and walking. Int. J. Environ. Res. Public Health 2021, 18, 12942. [Google Scholar] [CrossRef]
- Faria, A.; Gabriel, R.; Abrantes, J.; Brás, R.; Moreira, H. The relationship of body mass index, age and triceps-surae musculotendinous stiffness with the foot arch structure of postmenopausal women. Clin. Biomech. 2010, 25, 588–593. [Google Scholar] [CrossRef]
- Jankowicz-Szymanska, A.; Mikolajczyk, E. Genu valgum and flat feet in children with healthy and excessive body weight. Pediatr. Phys. Ther. 2016, 28, 200–206. [Google Scholar] [CrossRef]
- Yan, S.; Li, R.; Shi, B.; Wang, R.; Yang, L. Mixed factors affecting plantar pressures and center of pressure in obese children: Obesity and flatfoot. Gait Posture 2020, 80, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Dommati, H.; Cheng, J. A Turnkey manufacturing solution for customized insoles using material extrusion process. In 3D Printing and Additive Manufacturing Technologies; Springer: Singapore, 2019; pp. 203–216. [Google Scholar]
- Zhao, Y.; Zheng, D.; Yan, S.; Liu, M.; Yang, L. Children with obesity experience different age-related changes in plantar pressure distributions: A follow-up study in China. Int. J. Environ. Res. Public Health 2020, 17, 6602. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ishikawa, H.; Shibuya, T.; Takai, C.; Nemoto, T.; Nomura, Y.; Abe, A.; Otani, H.; Ito, S.; Nakazono, K.; et al. The combination of modified Mitchell’s osteotomy and shortening oblique osteotomy for patients with rheumatoid arthritis: An analysis of changes in plantar pressure distribution. Int. J. Environ. Res. Public Health 2021, 18, 9948. [Google Scholar] [CrossRef] [PubMed]
- Hawrylak, A.; Brzeźna, A.; Chromik, K. Distribution of plantar pressure in soccer players. Int. J. Environ. Res. Public Health 2021, 18, 4173. [Google Scholar] [CrossRef] [PubMed]
- Cornwall, M.W.; McPoil, T.G. Influence of rearfoot postural alignment on rearfoot motion during walking. Foot 2004, 14, 133–138. [Google Scholar] [CrossRef]
- Hasegawa, H.; Yamauchi, T.; Kraemer, W.J. Foot strike patterns of runners at the 15-km point during an elite-level half marathon. J. Strength Cond. Res. 2007, 21, 888–893. [Google Scholar]
- Zhou, H. Is there a relationship between strike pattern and injury during running: A review. Phys. Act. Health 2019, 3, 127–134. [Google Scholar] [CrossRef]
- Guettler, J.H.; Ruskan, G.J.; Bytomski, J.R.; Brown, C.R.; Richardson, J.K.; Moorman, C.T., 3rd. Fifth metatarsal stress fractures in elite basketball players: Evaluation of forces acting on the fifth metatarsal. Am. J. Orthop. 2006, 35, 532–536. [Google Scholar]
- Yu, B.; Preston, J.J.; Queen, R.M.; Byram, I.R.; Hardaker, W.M.; Gross, M.T.; Davis, J.M.; Taft, T.N.; Garrett, W.E. Effects of wearing foot orthosis with medial arch support on the fifth metatarsal loading and ankle inversion angle in selected basketball tasks. J. Orthop. Sport. Phys. Ther. 2007, 37, 186–191. [Google Scholar] [CrossRef]
- Willems, T.M.; De Ridder, R.; Roosen, P. The effect of a long-distance run on plantar pressure distribution during running. Gait Posture 2012, 35, 405–409. [Google Scholar] [CrossRef]
- Fu, W.J. The role of footwear on plantar pressure performance during badminton movements. Appl. Mech. Mater. 2011, 55–57, 1675–1678. [Google Scholar] [CrossRef]
- Chua, Y.K.; Quek, R.K.; Kong, P.W. Basketball lay-up—Foot loading characteristics and the number of trials necessary to obtain stable plantar pressure variables. Sport. Biomech. 2017, 16, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Bisiaux, M.; Moretto, P. The effects of fatigue on plantar pressure distribution in walking. Gait Posture 2008, 28, 693–698. [Google Scholar] [CrossRef]
- Petrinović, L.; Štefan, L.; Munivrana, G. Some morphological differences between opposite sides of the body of elite European junior badminton players. Acta Kinesiol. 2015, 9, 67–71. [Google Scholar]
- Nadzalan, A.M.; Azmi, S.H.; Mohamad, N.I.; Lee, J.L.F.; Tan, K.; Chinnasee, C. Kinematics analysis of dominant and non-dominant lower limb during step and jump forward lunge in badminton. J. Fundam. Appl. Sci. 2018, 10, 232–242. [Google Scholar]
- Manolova, A. Lower-limb asymmetry in balance ability of young badminton players. J. Appl. Sport. Sci. 2018, 2, 35–42. [Google Scholar] [CrossRef]
- Klem, N.R.; Wild, C.Y.; Williams, S.; Ng, L. Effect of external ankle support on ankle and knee biomechanics during the cutting maneuver in basketball players. Am. J. Sport. Med. 2017, 45, 685–691. [Google Scholar] [CrossRef]
- Czerniecki, J.M. Foot and ankle biomechanics in walking and running. A review Am. J. Phys. Med. Rehabil. 1988, 67, 246–252. [Google Scholar]
- Chen, W.H.; Chiang, C.W.; Fiolo, N.J.; Fuchs, P.X.; Shiang, T.Y. Ideal combinations of acceleration-based intensity metrics and sensor positions to monitor exercise intensity under different types of sports. Sensors 2022, 22, 2583. [Google Scholar] [CrossRef]
- Gao, L.; Lu, Z.; Liang, M.; Baker, J.S.; Gu, Y. Influence of different load conditions on lower extremity biomechanics during the lunge squat in novice men. Bioengineering 2022, 9, 272. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | Recreational Group (n = 68) | Elite Group (n = 65) |
|---|---|---|
| Age (years) | 19.9 ± 0.8 | 20.2 ± 1.2 |
| Height (cm) | 170.3 ± 3.9 | 177.4 ± 4.6 * |
| Mass (kg) | 67.7 ± 3.2 | 72.6 ± 4.6 ** |
| BMI (kg/m2) | 23.3 ± 0.4 | 23.1 ± 0.7 ** |
| Badminton Training experience (years) | 3.1 ± 0.7 | 5.9 ± 1.1 ** |
| Recreational Group (n = 68) | Elite Group (n = 65) | p-Value | |
|---|---|---|---|
| Left foot | 0.21 ± 0.06 | 0.20 ± 0.07 | 0.057 |
| Right foot | 0.21 ± 0.05 | 0.20 ± 0.06 | 0.116 |
| Region | Recreational Group (n = 68) | Elite Group (n = 65) |
|---|---|---|
| Static standing | ||
| Left foot | ||
| Forefoot (%) | 21.37 ± 2.69 | 21.57 ± 2.34 |
| Midfoot (%) | 11.50 ± 10.62 | 12.27 ± 11.52 b |
| Rearfoot (%) | 17.13 ± 4.31 | 16.16 ± 8.10 b |
| Right foot | ||
| Forefoot (%) | 21.69 ± 2.81 | 21.57 ± 2.90 |
| Midfoot (%) | 11.59 ± 10.16 | 12.17 ± 11.47 b |
| Rearfoot (%) | 16.73 ± 5.46 | 16.26 ± 8.21 b |
| Midstance phase of walking | ||
| Left foot | ||
| Forefoot (%) | 21.96 ± 2.44 | 26.80 ± 4.41 b,c |
| Midfoot (%) | 11.03 ± 9.96 | 9.74 ± 9.57 d |
| Rearfoot (%) | 17.01 ± 4.25 | 13.43 ± 7.43 b,d |
| Right foot | ||
| Forefoot (%) | 22.19 ± 5.03 d | 25.30 ± 7.18 b,d |
| Midfoot (%) | 11.23 ± 10.62 | 10.63 ± 10.58 d |
| Rearfoot (%) | 16.86 ± 5.90 | 14.07 ± 7.70 b,d |
| Six Subregions | Static Standing | Midstance Phase of Walking | ||
|---|---|---|---|---|
| Left Foot | Right Foot | Left Foot | Right Foot | |
| Recreational group (n = 68) | ||||
| Lateral Metatarsal bone (LM) | 22.01 ± 2.80 | 22.05 ± 2.81 | 23.32 ± 1.65 d | 22.95 ± 5.18 c |
| Lateral Longitudinal Arch (LLA) | 21.67 ± 4.14 | 21.58 ± 1.86 | 20.58 ± 4.63 | 21.00 ± 5.74 d |
| Lateral Heel (LH) | 20.61 ± 1.80 | 20.69 ± 3.97 | 20.68 ± 4.56 d | 20.71 ± 5.51 c |
| Medial Metatarsal bone (MM) | 20.74 ± 2.44 | 21.33 ± 2.78 | 20.80 ± 1.77 | 21.42 ± 4.79 |
| Medial Longitudinal Arch (MLA) | 1.32 ± 0.41 | 1.60 ± 1.38 | 1.29 ± 0.40 | 1.45 ± 0.36 |
| Medial Heel (MH) | 13.66 ± 3.13 | 12.77 ± 3.55 | 13.23 ± 2.77 | 12.94 ± 3.00 |
| Elite group (n = 65) | ||||
| Lateral Metatarsal bone (LM) | 20.62 ± 2.42 | 21.31 ± 2.61 | 26.40 ± 2.26 a | 26.28 ± 7.17 a |
| Lateral Longitudinal Arch (LLA) | 23.58 ± 2.84 b | 23.42 ± 2.87 b | 18.63 ± 4.89 d | 20.28 ± 6.02 d |
| Lateral Heel (LH) | 23.85 ± 2.54 b | 24.01 ± 2.57 b | 19.87 ± 5.00 d | 20.36 ± 5.84 d |
| Medial Metatarsal bone (MM) | 22.51 ± 1.82 | 21.84 ± 3.17 | 27.19 ± 2.51 a | 24.33 ± 7.11 b |
| Medial Longitudinal Arch (MLA) | 0.97 ± 0.33 | 0.93 ± 0.32 | 0.85 ± 0.32 | 0.98 ± 0.34 |
| Medial Heel (MH) | 8.47 ± 2.36 b | 8.50 ± 2.65 b | 7.00 ± 1.44 b,d | 7.79 ± 2.29 d |
| Recreational Group (n = 68) | Elite Group (n = 65) | |
|---|---|---|
| Left foot | 50.83 ± 5.25 | 47.08 ± 9.41 * |
| Right foot | 49.17 ± 5.25 | 52.92 ± 9.41 * |
| Recreational Group (n = 68) | Elite Group (n = 65) | |
|---|---|---|
| Left foot | 4.04 ± 2.03 | 1.13 ± 0.64 * |
| Right foot | 4.57 ± 3.15 | 1.02 ± 0.53 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chow, T.-H.; Hsu, C.-C.; Chen, C.-C.; Hsu, C.-H. Bipedal Static Supination and Dynamic Forefoot Loading Characteristics in Taiwanese College Badminton Players: A Cross-Sectional Study. Bioengineering 2023, 10, 498. https://doi.org/10.3390/bioengineering10040498
Chow T-H, Hsu C-C, Chen C-C, Hsu C-H. Bipedal Static Supination and Dynamic Forefoot Loading Characteristics in Taiwanese College Badminton Players: A Cross-Sectional Study. Bioengineering. 2023; 10(4):498. https://doi.org/10.3390/bioengineering10040498
Chicago/Turabian StyleChow, Tong-Hsien, Chin-Chia Hsu, Chih-Cheng Chen, and Chin-Hsien Hsu. 2023. "Bipedal Static Supination and Dynamic Forefoot Loading Characteristics in Taiwanese College Badminton Players: A Cross-Sectional Study" Bioengineering 10, no. 4: 498. https://doi.org/10.3390/bioengineering10040498
APA StyleChow, T. -H., Hsu, C. -C., Chen, C. -C., & Hsu, C. -H. (2023). Bipedal Static Supination and Dynamic Forefoot Loading Characteristics in Taiwanese College Badminton Players: A Cross-Sectional Study. Bioengineering, 10(4), 498. https://doi.org/10.3390/bioengineering10040498