
Influence of Simulated State of Disc Degeneration and Axial Stiffness of Coupler in a Hybrid Performance Stabilisation System on the Biomechanics of a Spine Segment Model

 ,
, 
Abstract
:
1. Introduction
2. Methods
2.1. FE Model Construction
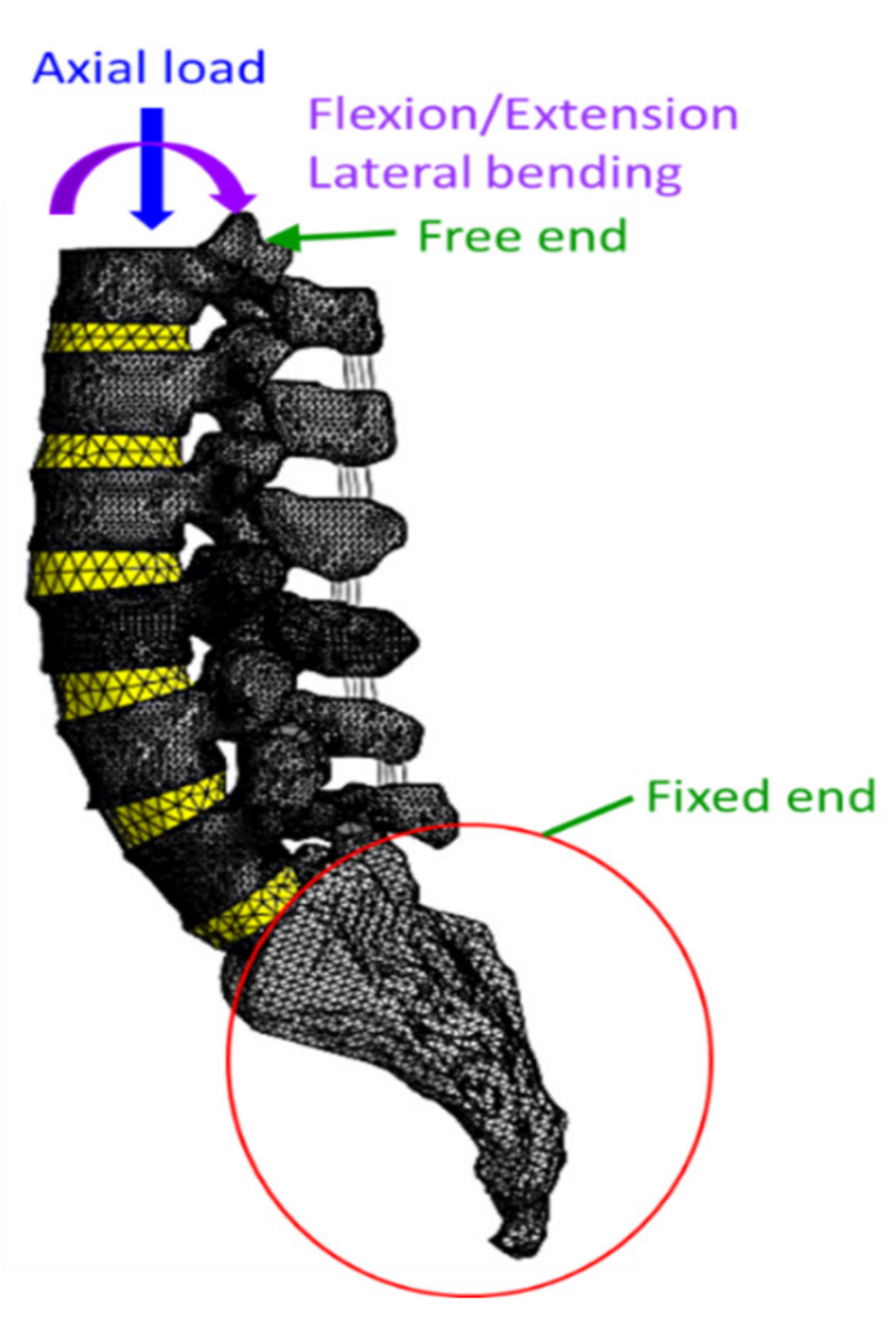
2.2. Boundary and Loading Conditions
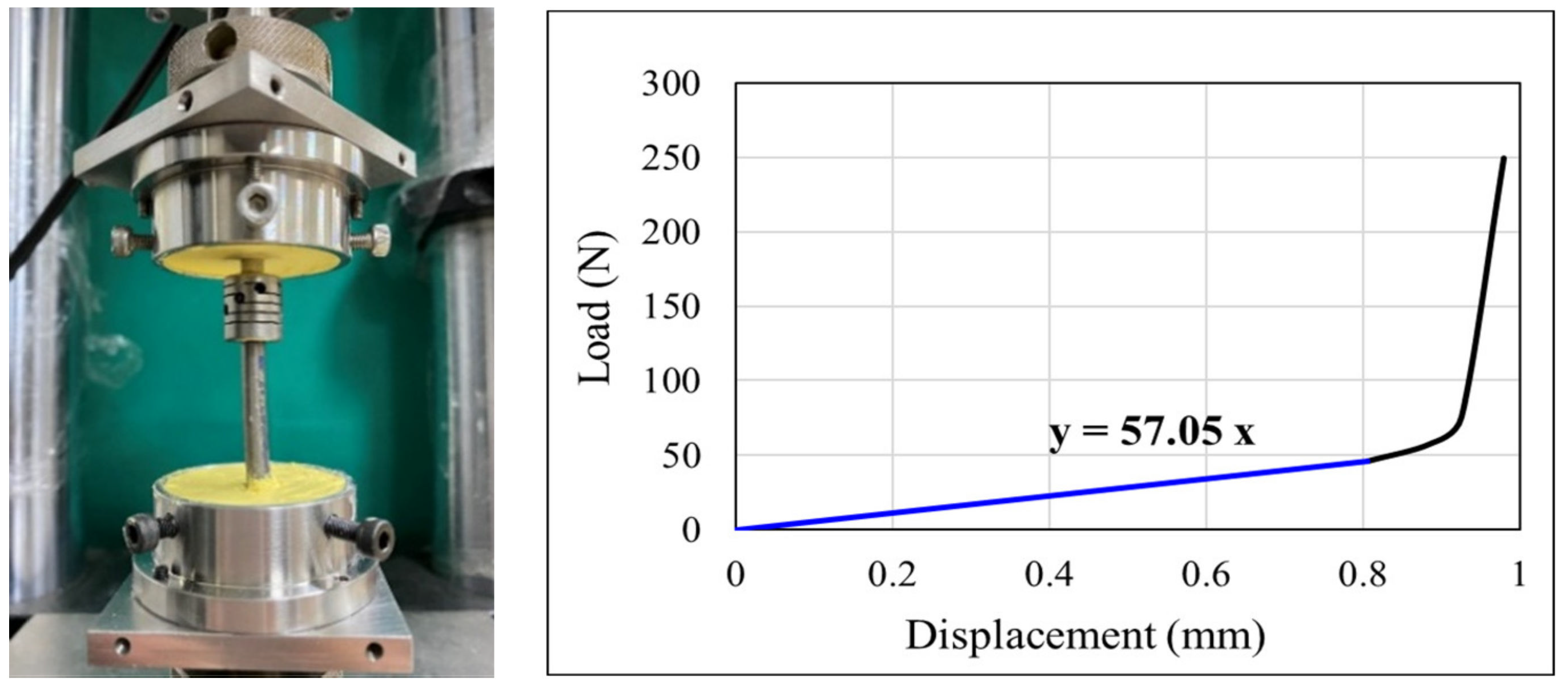
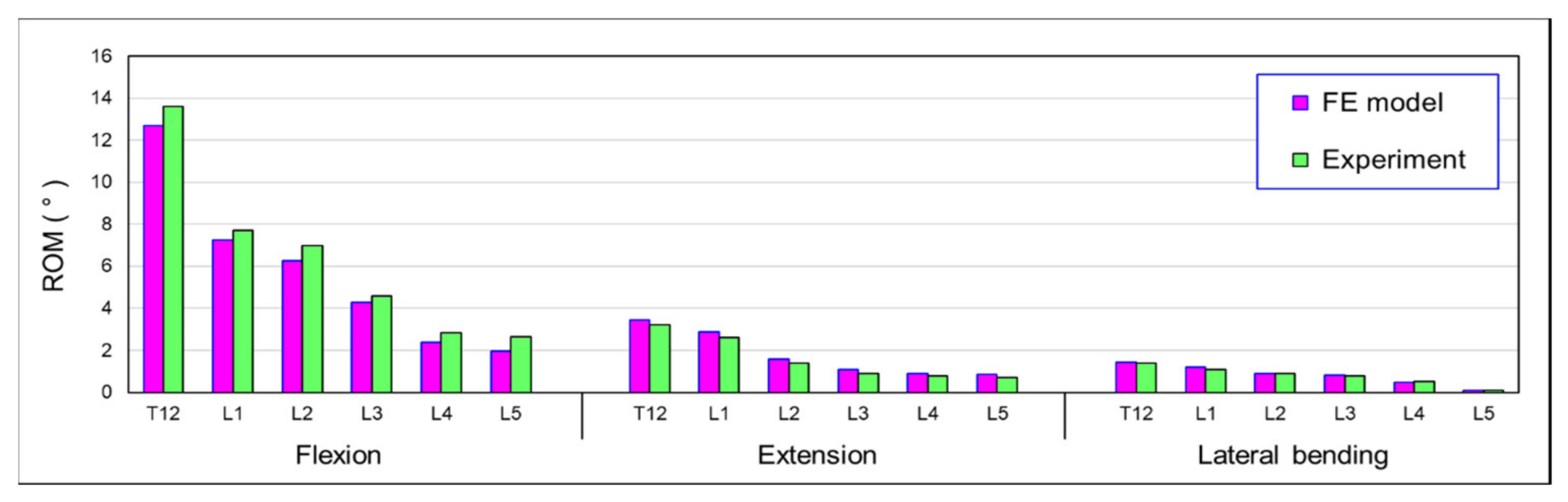
2.3. Validation of the FE Model
3. Results
3.1. Influence of Simulated State of Degeneration of L3/L4 and L4/L5 IVDs on von Mises Stress in IVDs
3.2. Influence of Simulated State of Degeneration of L3/L4 and L4/L5 IVDs on the Intersegmental Range of Motion (ROM)
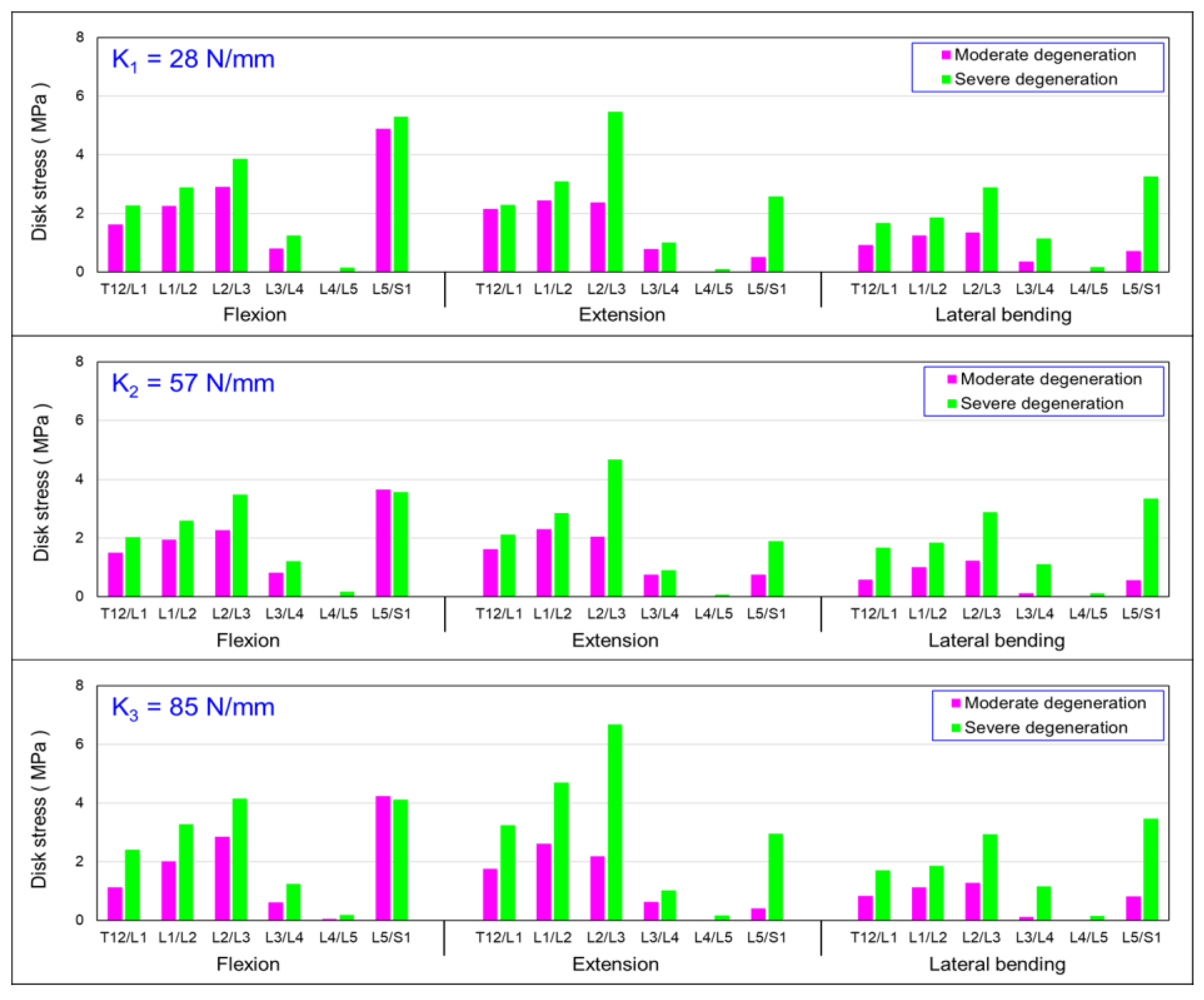
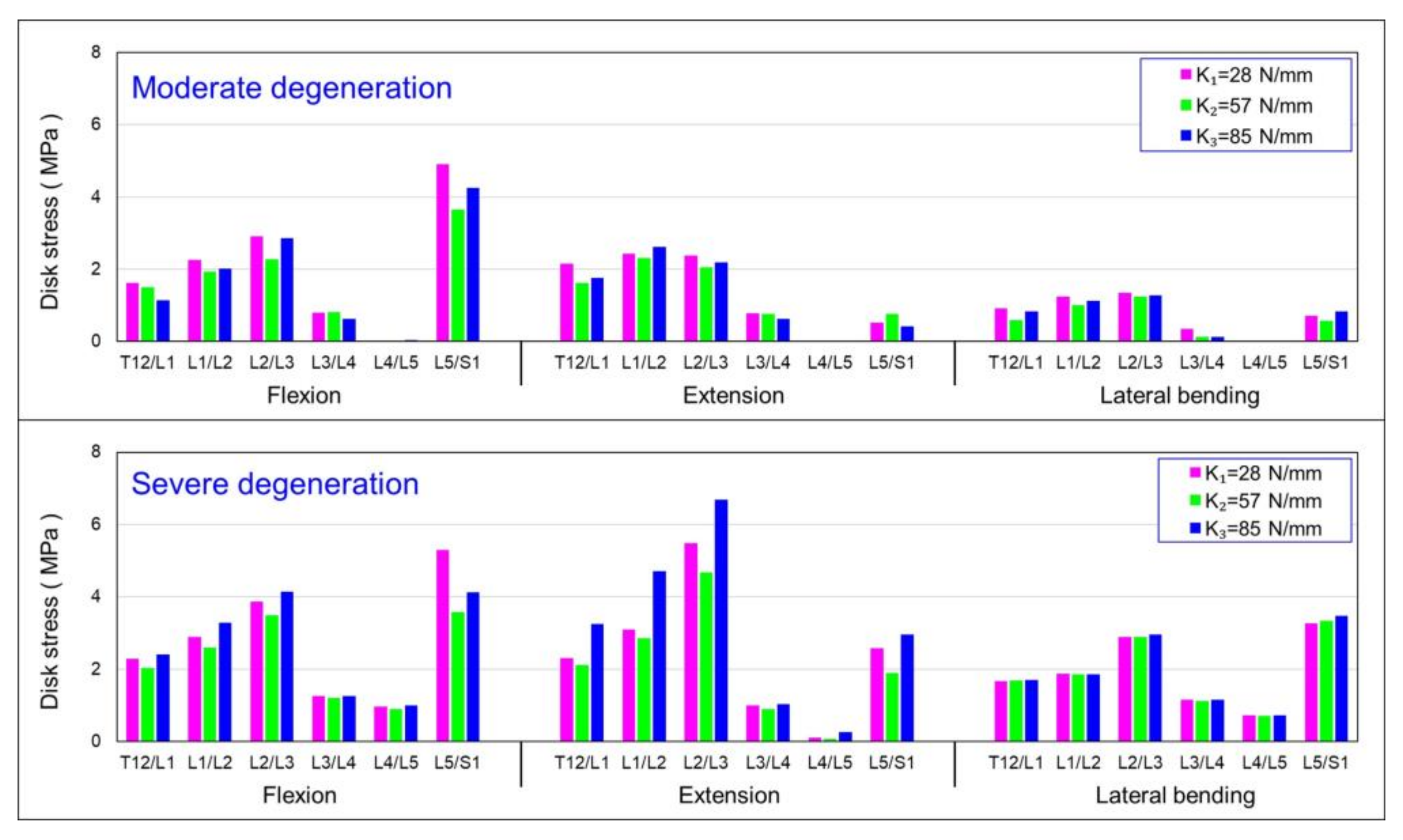
3.3. Influence of Axial Stiffness of Dynamic Coupler (K) on von Mises Stress in IVDs
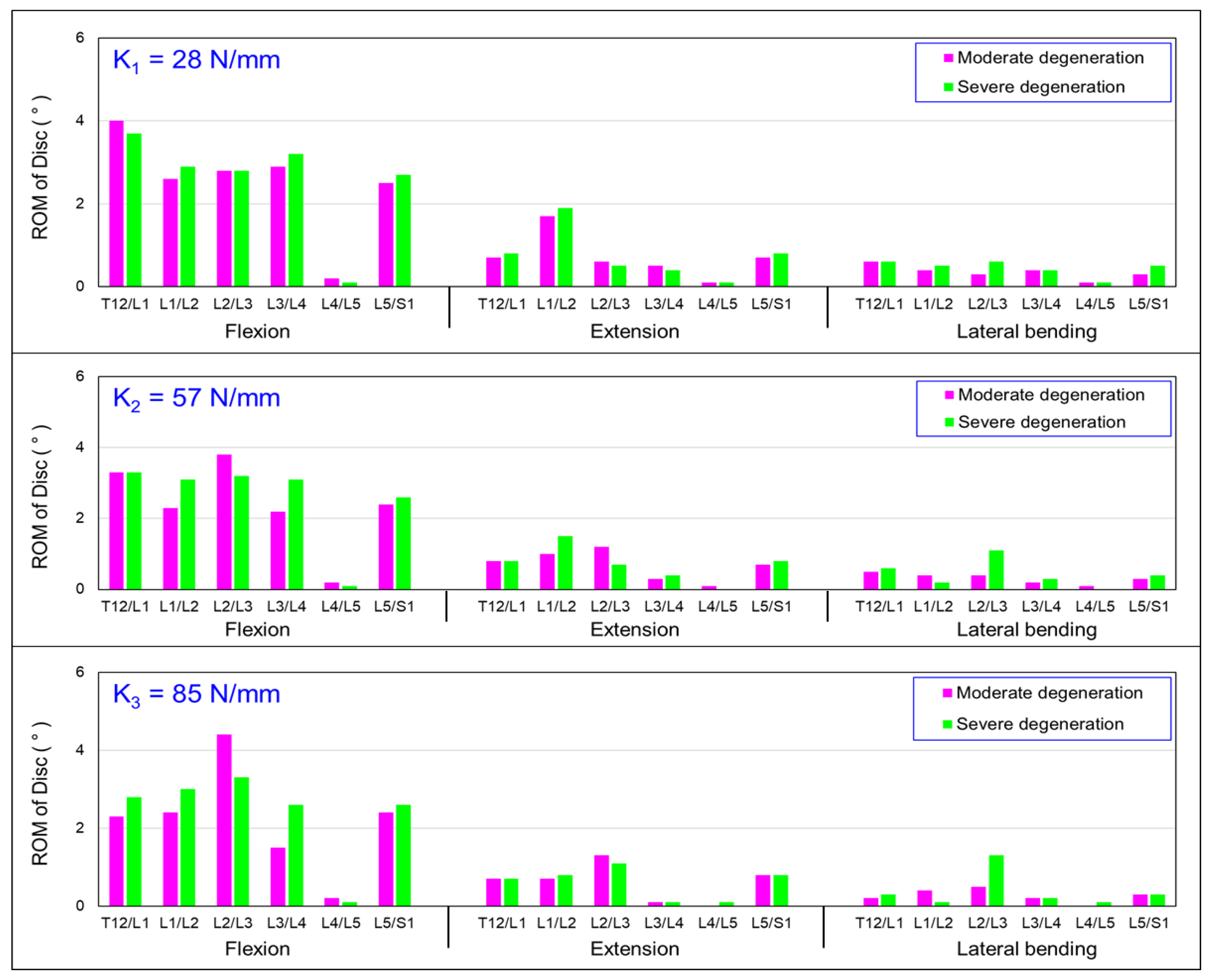
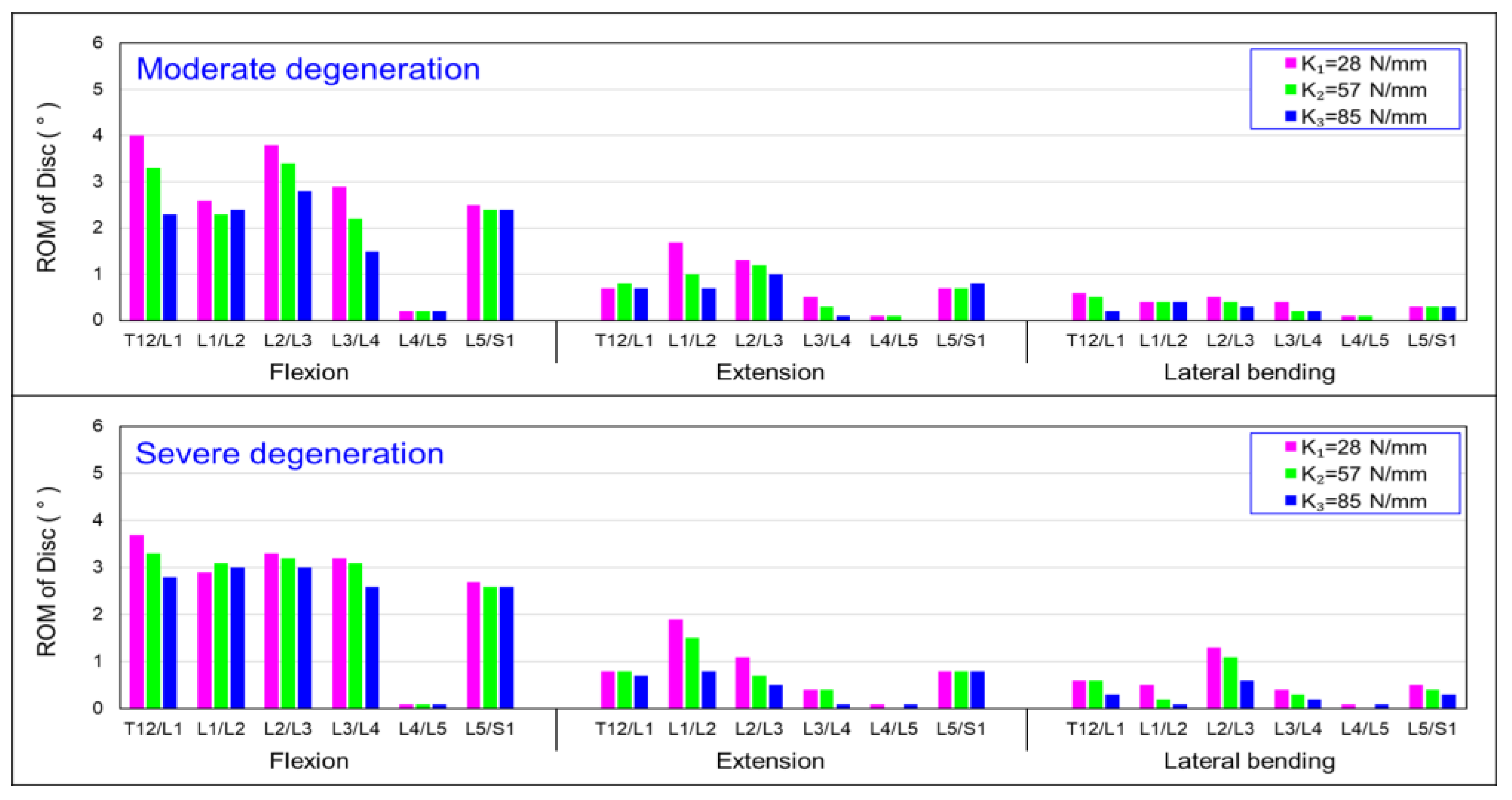
3.4. Influence of Axial Stiffness of Dynamic Coupler (K) on the Intersegmental Range of Motion (ROM)
4. Discussion
5. Conclusions
- (1)
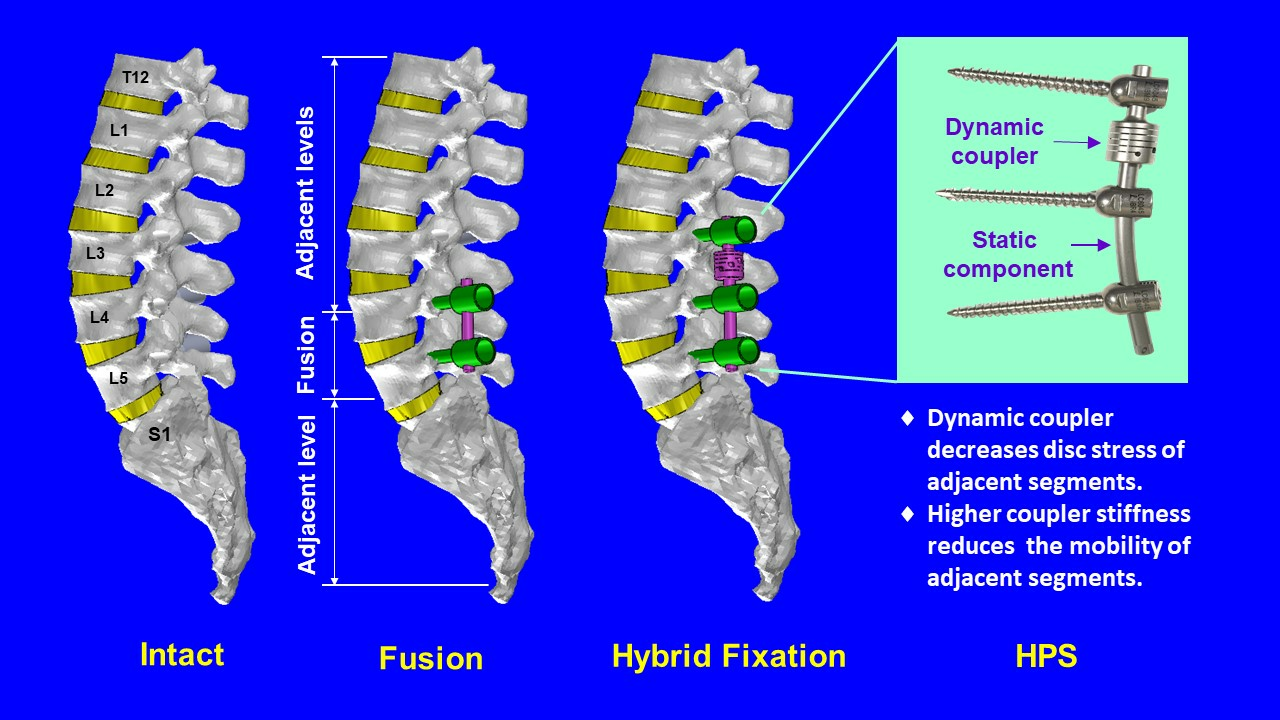
- For discs with moderate degeneration, increasing the coupler stiffness led to a decrease in disc mobility. However, in the case of severe disc degeneration, the effect on disc mobility by coupler stiffness was less pronounced. While considering the design and selection of coupler stiffness, the degeneration level of intervertebral discs should be considered to achieve the desired mobility characteristics;
- (2)
- Increasing the coupler stiffness led to higher stress on intervertebral discs with moderate degeneration, while its effect on stress was less pronounced for discs with severe degeneration. In flexion, extension, and lateral bending, higher coupler stiffness resulted in a reduction in the mobility of adjacent segments.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, T.; Wenyuan Ding, W. Risk factors for adjacent segment degeneration after posterior lumbar fusion surgery in treatment for degenerative lumbar disorders: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 582. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimkhani, M.; Arjmand, N.; Shirazi-Adl, A. Biomechanical effects of lumbar fusion surgery on adjacent segments using musculoskeletal models of the intact, degenerated and fused spine. Sci. Rep. 2021, 11, 17892. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.K.; Monroe, B.T.; Gilbertson, L.G.; Brinckmann, P. Interlaminar shear stresses and laminae separation in a disc. Finite element analysis of the L3–L4 motion segment subjected to axial compressive loads. Spine 1995, 20, 689–698. [Google Scholar] [CrossRef]
- Cammarata, M.; Aubin, C.E.; Wang, X.; Mac-Thiong, J.M. Biomechanical risk factors for proximal junctional kyphosis: A detailed numerical analysis of surgical instrumentation variables. Spine 2014, 39, E500–E507. [Google Scholar] [CrossRef]
- Guan, Y.; Yoganandan, N.; Zhang, J.; Pintar, F.A.; Cusick, J.F.; Wolfla, C.E.; Maiman, D.J. Validation of a clinical finite element model of the human lumbosacral spine. Med. Biol. Eng. Comput. 2006, 44, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Weinhoffer, S.L.; Guyer, R.D.; Herbert, M.; Griffith, S.L. Intradiscal pressure measurements above an instrumented fusion. A cadaveric study. Spine 1995, 20, 526–531. [Google Scholar] [CrossRef]
- Malakoutian, M.; Volkheimer, D.; Street, J.; Dvorak, M.F.; Wilke, H.J.; Oxland, T.R. Do in vivo kinematic studies provide insight into adjacent segment degeneration? A qualitative systematic literature review. Eur. Spine J. 2015, 24, 1865–1881. [Google Scholar] [CrossRef]
- Shirazi-Adl, A.; Ahmed, A.M.; Shrivastava, S.C. Mechanical response of a lumbar motion segment in axial torque alone and combined with compression. Spine 1986, 11, 914–927. [Google Scholar] [CrossRef]
- Ebrahimkhani, M.; Arjmand, N.; Shirazi-Adl, A. Adjacent segments biomechanics following lumbar fusion surgery: A musculoskeletal finite element model study. Eur. Spine J. 2022, 31, 1630–1639. [Google Scholar] [CrossRef]
- Hashimoto, K.; Aizawa, T.; Kanno, H.; Itoi, E. Adjacent segment degeneration after fusion spinal surgery-a systematic review. Int. Orthop. 2019, 43, 987–993. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent segment disease after lumbar or lumbosacral fusion: Review of the literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.L.; Zhong, Z.C.; Hsu, H.W.; Shih, S.L.; Wang, S.T.; Hung, C.; Chen, C.S. Effect of the cord pretension of the Dynesys dynamic stabilisation system on the biomechanics of the lumbar spine: A finite element analysis. Eur. Spine J. 2011, 20, 1850–1858. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Germay, B.; Schaerer, N.S.; Fennema, P.; Braunschweiler, R. Dynamic neutralization: A new concept for restabilization of the spine. In Lumbar Segmental Instability; Szalski, M., Gunzburg, R., Pope, M.H., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 1999; pp. 233–240. [Google Scholar]
- Freudiger, S.; Dubios, G.; Lorrain, M. Dynamic neutralization of the lumbar spine confirmed on a new lumbar spine simulator in vitro. Arch. Orthop. Trauma Surg. 1999, 199, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Grob, D.; Benini, A.; Junge, A.; Mannion, A.F. Clinical experience with the dynesys semirigid fixation system for the lumbar spine. Spine 2005, 30, 324–331. [Google Scholar] [CrossRef]
- Schmoelz, W.; Huber, J.F.; Nydegger, T.; Claes, L.; Wilke, H.J. Dynamic stabilization of the lumbar spine and its effects on adjacent segments. Spine 2003, 16, 418–423. [Google Scholar] [CrossRef]
- Hybrid Performance System HPS. Paradigm Spine. Available online: https://www.yumpu.com/de/document/read/32915740/hpstm-broschure-deutschpdf-paradigm-spine (accessed on 19 September 2019).
- Wilke, H.J.; Heuer, F.; Schmidt, H. Prospective design delineation and subsequent in vitro evaluation of a new posterior dynamic stabilization system. Spine 2009, 34, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Baracco, R.; Procura, A.; Nena, U.; Ruggieri, P. Lumbar Stabilization with DSS-HPS® System: Radiological Outcomes and Correlation with Adjacent Segment Degeneration. Diagnostics 2021, 11, 1891. [Google Scholar] [CrossRef]
- Fay, L.Y.; Wu, J.C.; Tsai, T.Y.; Wu, C.L.; Huang, W.C.; Cheng, H. Dynamic stabilization for degenerative spondylolisthesis: Evaluation of radiographic and clinical outcomes. Clin. Neurol. Neurosurg. 2013, 115, 535–541. [Google Scholar] [CrossRef]
- Demir, E.; Eltes, P.; Castro, A.P.; Lacroix, D.; Toktaş, İ. Finite element modelling of hybrid stabilization systems for the human lumbar spine. Proc. Inst. Mech. Eng. H 2020, 234, 1409–1420. [Google Scholar] [CrossRef]
- Yang, H.; Jekir, M.G.; Davis, M.W.; Keaveny, T.M. Effective modulus of the human intervertebral disc and its effect on vertebral bone stress. J. Biomech. 2016, 49, 1134–1140. [Google Scholar] [CrossRef]
- Antoniou, J.; Steffen, T.; Nelson, F.; Winterbottom, N.; Hollander, A.P.; Poole, R.A.; Aebi, M.; Alini, M. The human lumbar intervertebral disc: Evidence for changes in the biosynthesis and denaturation of the extracellular matrix with growth, maturation, ageing, and degeneration. J. Clin. Investig. 1996, 98, 996–1003. [Google Scholar] [CrossRef] [PubMed]
- Iatridis, J.C.; Setton, L.A.; Weidenbaum, M.; Mow, V.C. Alterations in the mechanical behavior of the human lumbar nucleus pulposus with degeneration and aging. J. Orthop. Res. 1997, 15, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Goto, K.; Tajima, N.; Chosa, E.; Totoribe, K.; Shinichiro, S.; Kuroki, H. Effect of lumbar spinal fusion on the other lumbar intervertebral levels (threedimensional finite element analysis). J. Orthop. Sci. 2003, 8, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Pei, B.; Xu, Y.; Zhao, Y.; Wu, X.; Lu, D.; Wang, H.; Wu, S. Biomechanical comparative analysis of conventional pedicle screws and cortical bone trajectory fixation in the lumbar spine: An in vitro and finite element study. Front. Bioeng. Biotechnol. 2023, 11, 1060059. [Google Scholar] [CrossRef] [PubMed]
- Ayturk, U.M.; Puttlitz, C.M. Parametric convergence sensitivity and validation of a finite element model of the human lumbar spine. Comput. Methods Biomech. Biomed. Eng. 2011, 14, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.C.; Wilcox, R.K. Finite element analysis of the spine: Towards a framework of verification, validation and sensitivity analysis. Med. Eng. Phys. 2008, 30, 1287–1304. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, C.K.; Tsai, Y.J.; Yen, C.Y.; Li, Y.C.; Hsiao, H.Y.; Tu, Y.K. Biomechanical Effect of Hybrid Dynamic Stabilization Implant on the Segmental Motion and Intradiscal Pressure in Human Lumbar Spine. Bioengineering 2022, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.Y.; Hsu, C.M.; Chiu, Y.W.; Wang, Z.Y.; Tu, Y.K.; Tsai, Y.J.; Hsiao, C.K. Influence Of Coupler Stiffness Of Hybrid Performance Stabilization System (Hps) On The Disc Stress Of Intrinsic Degenerated Spine: A Finite Element Study. In Proceedings of the XXIX Congress of International Society of Biomechanics (ISB), Fukuoka, Japan, 30 July–4 August 2023. [Google Scholar]
- Adams, M.A.; McNally, D.S.; Dolan, P. ‘Stress’ distributions inside intervertebral discs. The effects of age and degeneration. J. Bone Jt. Surg. 1996, 78, 965–972. [Google Scholar] [CrossRef]
- Chu, J.Y.; Skrzypiec, D.; Pollintine, P.; Adams, M.A. Can compressive stress be measured experimentally within the annulus fibrosus of degenerated intervertebral discs? Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2008, 222, 161–170. [Google Scholar] [CrossRef]
- Zahari, S.N.; Latif, M.J.A.; Rahim, N.R.A.; Kadir, M.R.A.; Kamarul, T. The effects of physiological biomechanical loading on intradiscal pressure and annulus stress in lumbar spine: A finite element analysis. J. Healthc. Eng. 2017, 2017, 9618940. [Google Scholar] [CrossRef]
- Ignasiak, D.; Peteler, T.; Fekete, T.F.; Haschtmann, D.; Ferguson, S.J. The influence of spinal fusion length on proximaljunction biomechanics: A parametric computationalstudy. Eur. Spine J. 2018, 27, 2262–2271. [Google Scholar] [CrossRef] [PubMed]
- McNally, D.S.; Adams, M.A.; Goodship, A.E. Development and validation of a new transducer for intradiscal pressure measurement. J. Biomed. Eng. 1992, 14, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A.; Freeman, B.J.; Morrison, H.P.; Nelson, I.W.; Dolan, P. Mechanical initiation of intervertebral disc degeneration. Spine 2000, 25, 1625–1636. [Google Scholar] [CrossRef] [PubMed]
- Dolan, P.; Adams, M.A. Recent advances in lumbar spinal mechanics and their significance for modelling. Clin. Biomech. 2001, 16, S8–S16. [Google Scholar] [CrossRef] [PubMed]
- Pollintine, P.; Przybyla, A.S.; Dolan, P.; Adams, M.A. Neural arch load-bearing in old and degenerated spines. J. Biomech. 2004, 37, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kang, K.T.; Chun, H.J.; Lee, C.K.; Chang, B.S.; Yeom, J.S. The influence of intrinsic disc degeneration of the adjacent segments on its stress distribution after one-level lumbar fusion. Eur. Spine J. 2015, 24, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Landham, P.R.; Gilbert, S.J.; Baker-Rand, H.L.; Pollintine, P.; Brown, K.A.R.; Adams, M.A.; Dolan, P. Pathogenesis of vertebral anterior wedge deformity: A 2-stage process? Spine 2015, 40, 902–908. [Google Scholar] [CrossRef]
- Panico, M.; Bassani, T.; Villa, T.M.T.; Galbusera, F. The Simulation of Muscles Forces Increases teh Stresses in Lumbar Fixation Implants with Respect to Pure Moment Loading. Front. Bioeng. Biotechnol. 2021, 9, 745703. [Google Scholar] [CrossRef]
- Ou, Y.; Xiao, Z.; Wei, J.; Jiang, H.; Li, Z. Upper and lower adjacent segment range of motion after fixation of different lumbar spine segments in the goat: An in vitro experiment. J. Int. Med. Res. 2021, 49, 3000605211020219. [Google Scholar] [CrossRef]
- White, A.A.; Panjabi, M.M. Clinical Biomechanics of the Spine, 2nd ed.; Lippincott: Philadelphia, PA, USA, 1990. [Google Scholar]
- Sayed, D.; Kasra Amirdelfan, K.; Ramana KNaidu, R.K.; Raji, O.R.; Steven Falowski, S. A Cadaver-Based Biomechanical Evaluation of a Novel Posterior Approach to Sacroiliac Joint Fusion: Analysis of the Fixation and Center of the Instantaneous Axis of Rotation. Med. Devices 2021, 14, 435–444. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material (Tissues) | Elastic Modulus (MPa) | Poisson’s Ratio | Element Number | Node Number |
|---|---|---|---|---|
| Cortical bone [25] | 12,000 | 0.3 | 31,562 | 15,632 |
| Cancellous bone [25] | 100 | 0.2 | 28,033 | 13,355 |
| Healthy annulus [25] | 8.4 | 0.45 | 20,238 | 16,856 |
| Nucleus pulposus [25] | 1 | 0.499 | -- | -- |
| Endplate [25] | 24 | 0.4 | 6035 | 4366 |
| Moderate degenerated disc (Em) [22] | 32 | 0.3 | 266,322 | 166,451 |
| Severely degenerated disc (Es) [22] | 20 | 0.3 | 266,322 | 166,451 |
| Ligament [26] | 8 | 0.3 | 8963 | 5647 |
| Screw, rod, and coupler [26] | 110,000 | 0.28 | 40,569 | 25,396 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, C.-K.; Hsiao, H.-Y.; Tsai, Y.-J.; Hsu, C.-M.; Tu, Y.-K. Influence of Simulated State of Disc Degeneration and Axial Stiffness of Coupler in a Hybrid Performance Stabilisation System on the Biomechanics of a Spine Segment Model. Bioengineering 2023, 10, 1042. https://doi.org/10.3390/bioengineering10091042
Hsiao C-K, Hsiao H-Y, Tsai Y-J, Hsu C-M, Tu Y-K. Influence of Simulated State of Disc Degeneration and Axial Stiffness of Coupler in a Hybrid Performance Stabilisation System on the Biomechanics of a Spine Segment Model. Bioengineering. 2023; 10(9):1042. https://doi.org/10.3390/bioengineering10091042
Chicago/Turabian StyleHsiao, Chih-Kun, Hao-Yuan Hsiao, Yi-Jung Tsai, Chao-Ming Hsu, and Yuan-Kun Tu. 2023. "Influence of Simulated State of Disc Degeneration and Axial Stiffness of Coupler in a Hybrid Performance Stabilisation System on the Biomechanics of a Spine Segment Model" Bioengineering 10, no. 9: 1042. https://doi.org/10.3390/bioengineering10091042
APA StyleHsiao, C. -K., Hsiao, H. -Y., Tsai, Y. -J., Hsu, C. -M., & Tu, Y. -K. (2023). Influence of Simulated State of Disc Degeneration and Axial Stiffness of Coupler in a Hybrid Performance Stabilisation System on the Biomechanics of a Spine Segment Model. Bioengineering, 10(9), 1042. https://doi.org/10.3390/bioengineering10091042