
Dynamic Acetabular Cup Orientation during Gait: A Study of Fast- and Slow-Walking Total Hip Replacement Patients

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Gait Data and Patient Selection
2.2. Computational Simulation
2.3. Data Analysis
3. Results
3.1. Patient-to-Patient Variation in Dynamic Cup Orientation
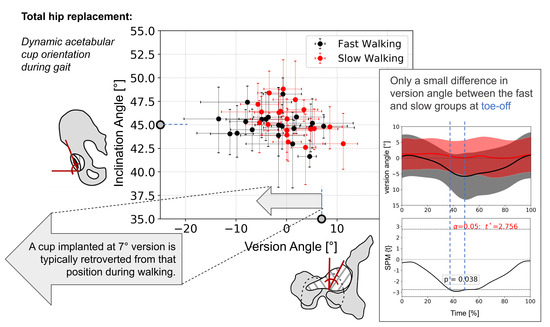
3.2. Comparison of Fast and Slow Walking Groups
3.3. Correlation of Pelvic Angles and Dynamic Cup Angles
4. Discussion
4.1. Discussion of Findings
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Joint Registry. NJR Annual Report 2020. Available online: http://www.njrreports.org.uk/ (accessed on 2 December 2021).
- Beverland, D.E.; O’Neill, C.K.; Rutherford, M.; Molloy, D.; Hill, J.C. Placement of the acetabular component. Bone Jt. J. 2016, 98 (1 Suppl. A), 37–43. [Google Scholar] [CrossRef]
- Zilkens, C.; Djalali, S.; Bittersohl, B.; Kalicke, T.; Kraft, C.N.; Krauspe, R.; Jager, M. Migration pattern of cementless press fit cups in the presence of stabilizing screws in total hip arthroplasty. Eur. J. Med. Res. 2011, 16, 127–132. [Google Scholar] [CrossRef]
- Zheng, G.Q.; Zhang, Y.G.; Chen, J.Y.; Wang, Y. Decision making regarding spinal osteotomy and total hip replacement for ankylosing spondylitis: Experience with 28 patients. Bone Jt. J. 2014, 96, 360–365. [Google Scholar] [CrossRef]
- Maratt, J.D.; Esposito, C.I.; McLawhorn, A.S.; Jerabek, S.A.; Padgett, D.E.; Mayman, D.J. Pelvic tilt in patients undergoing total hip arthroplasty: When does it matter? J. Arthroplast. 2015, 30, 387–391. [Google Scholar] [CrossRef]
- ISO 14242-1:2014; Implants for Surgery—Wear of Total Hip-Joint Prostheses—Part 1: Loading and Displacement Parameters for Wear-Testing Machines and Corresponding Environmental Conditions for Test. International Organisation for Standards: Geneva, Switzerland. Available online: https://www.iso.org/standard/63073.html (accessed on 1 December 2021).
- ISO 14242, 2014-2018; Implants for Surgery—Wear of Total Hip-Joint Prostheses—Part 4: Testing Hip Prostheses under variations in Component Positioning Which Results in Direct Edge Loading. International Organisation for Standards: Geneva, Switzerland. Available online: https://www.iso.org/standard/63835.html (accessed on 12 May 2021).
- ASTM F2582-20; Standard Test Method for Dynamic Impingement between Femoral and Acetabular Hip Components. ASTM International: West Conshohocken, PA, USA. Available online: https://www.astm.org/f2582-20.html (accessed on 13 January 2021).
- Bhaskar, D.; Rajpura, A.; Board, T. Current Concepts in Acetabular Positioning in Total Hip Arthroplasty. Indian J. Orthop. 2017, 51, 386–396. [Google Scholar] [CrossRef]
- Colombi, A.; Schena, D.; Castelli, C.C. Total hip arthroplasty planning. EFORT Open. Rev. 2019, 4, 626–632. [Google Scholar] [CrossRef]
- Mushtaq, N.; To, K.; Gooding, C.; Khan, W. Radiological Imaging Evaluation of the Failing Total Hip Replacement. Front. Surg. 2019, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Pierrepont, J.; Hawdon, G.; Miles, B.P.; O’Connor, B.; Baré, J.; Walter, L.R.; Marel, E.; Solomon, M.; McMahon, S.; Shimmin, A.J. Variation in functional pelvic tilt in patients undergoing total hip arthroplasty. Bone Jt. J. 2017, 99, 184–191. [Google Scholar] [CrossRef]
- Lazennec, J.Y.; Rousseau, M.A.; Brusson, A.; Folinais, D.; Amel, M.; Clarke, I.; Pour, A.E. Total Hip Prostheses in Standing, Sitting and Squatting Positions: An Overview of Our 8 Years Practice Using the EOS Imaging Technology. Open. Orthop. J. 2015, 9, 26–44. [Google Scholar] [CrossRef] [PubMed]
- Pierrepont, J.W.; Stambouzou, C.Z.; Miles, B.P.; O’Connor, P.B.; Walter, L.; Ellis, A.; Molnar, R.; Baré, J.V.; Solomon, M.; McMahon, S.; et al. Patient Specific Component Alignment in Total Hip Arthroplasty. Reconstr. Rev. 2016, 6, 27–33. [Google Scholar] [CrossRef]
- Niemeier, T.E.; Wills, B.W.; Theiss, S.M.; Strom, S.F. Sagittal Pelvic Kinematics in Hip Arthroplasty. Curr. Rev. Musculoskelet Med. 2020, 13, 240–246. [Google Scholar] [CrossRef]
- Caldwell, G.E.; Robertson, D.G.E.; Whittlesey, S.N. Forces and Their Measurement. In Research Methods in Biomechanics, 2014th ed.; Robertson, D.G.E., Caldwell, G.E., Hamill, J., Kamen, G., Whittlesey, S.N., Eds.; Bloomsbury Digital Resources: London, UK, 2004; Available online: https://www.humankineticslibrary.com (accessed on 2 December 2021). [CrossRef]
- De Pieri, E.; Lunn, D.E.; Chapman, G.J.; Rasmussen, K.P.; Ferguson, S.J.; Redmond, A.C. Patient characteristics affect hip contact forces during gait. Osteoarthr. Cartil. 2019, 27, 895–905. [Google Scholar] [CrossRef]
- Van Emmerik, R.E.; McDermott, W.J.; Haddad, J.M.; Van Wegen, E.E. Age-related changes in upper body adaptation to walking speed in human locomotion. Gait. Posture 2005, 22, 233–239. [Google Scholar] [CrossRef]
- Kim, M.-K.; Kim, S.-G.; Shin, Y.-J.; Choi, E.-H.; Choe, Y.-W. The relationship between anterior pelvic tilt and gait, balance in patient with chronic stroke. J. Phys. Ther. Sci. 2018, 30, 27–30. [Google Scholar] [CrossRef]
- Lunn, D.E.; Chapman, G.J.; Redmond, A.C. Hip kinematics and kinetics in total hip replacement patients stratified by age and functional capacity. J. Biomech. 2019, 87, 19–27. [Google Scholar] [CrossRef]
- Lunn, D.; Chapman, G.; Redmond, A. Motion Analysis in Total Hip Replacement Patients; University of Leeds: Leeds, UK, 2019. [Google Scholar] [CrossRef]
- Cappozzo, A.; Catani, F.; Croce, U.D.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Vasiljeva, K. ‘Pelvic-Acetabular-Motion-Convert’, Python Codes Calculating Acetabular Cup Orientation with Pelvic Motion Angles. Zenodo Data. 2021. Available online: https://zenodo.org/records/5846247 (accessed on 2 December 2021).
- Harrison, C.L.; Thomson, A.I.; Cutts, S.; Rowe, P.J. Riches PE. Research synthesis of recommended acetabular cup orientations for total hip arthroplasty. J. Arthroplast. 2014, 29, 377–382. [Google Scholar] [CrossRef]
- C-Motion WIKI Documentation. Pelvis Segment Angle. Available online: https://c-motion.com/v3dwiki/index.php?title=Pelvis_Segment_Angle (accessed on 2 December 2021).
- Friston, K. Chapter 2—Statistical parametric mapping. In Statistical Parametric Mapping; Penny, W.D., Friston, K.J., Ashburner, J.T., Kiebel, S.J., Nichols, T.E., Eds.; Academic Press: London, UK, 2007; pp. 10–31. [Google Scholar]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Zheng, N.; Hu, X.; Dimitriou, D.; Dai, K.; Guo, T.; Tsai, T.-Y. Well-placed acetabular component oriented outside the safe zone during weight-bearing daily activitites. Front. Bioeng. Biotechnol. 2021, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Snijders, T.E.; Schlösser, T.P.C.; van Stralen, M.; Castelein, R.M.; Stevenson, R.P.; Weinans, H.; de Gast, A. The effect of postural dynamics on the three-dimensional orientation of the acetabular cup in THA is patient specific. Clin. Orthop. Relat. Res. 2021, 479, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.; Murphy, W.S.; Ward, D.M.; Zheng, G.; Hayden, B.L.; Murphy, S.B. Effect of Pelvic Tilt and Rotation on Cup Orientation in Both Supine and Standing Positions. J. Arthroplast. 2018, 33, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. J. Bone Jt. Surg. Am. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Borhani, M.; McGregor, A.H.; Bull, A.M. An alternative technical marker set for the pelvis is more repeatable than the standard pelvic marker set. Gait Posture 2013, 38, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, N.M.; Atkinsa, P.R.; Kutschkea, M.J.; Goebela, J.M.; Bo Foremana, K.; Anderson, A.E. Soft tissue artifact causes significant errors in the calculation of joint angles and range of motion at the hip. Gait Posture 2017, 55, 184–190. [Google Scholar] [CrossRef]
- Vasiljeva, K.; Lunn, D.; Chapman, G.; Redmond, A.; Wang, L.; Thompson, J.; Williams, S.; Wilcox, R.K.; Jones, A.C. Dataset Supporting the Publication “Dynamic Acetabular Cup Orientation during Gait: A Study of Fast and Slow Walking Total Hip Replacement Patients”; University of Leeds: Leeds, UK, 2023. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Sex | Age (Years) Mean (s.d.), Range | Body Mass Index (kg/m2) Mean (s.d.), Range |
|---|---|---|---|
| Fast | 7 females, 13 males | 68 (6.7), 57–81 | 28 (3.5), 22–35 |
| Slow | 10 females, 9 males | 77 (6.2), 67–91 | 29 (4.3), 23–37 |
| Scenario: Inclination(o), Version (o) | 45°, 7° | 30°, 5° | 30°, 25° | 50°, 5° | 50°, 25° | |
|---|---|---|---|---|---|---|
| p-value [gait cycle points] | Inclination | NS * | NS * | NS * | NS * | NS * |
| Version | 0.038 [38–50] | 0.034 [39–59] | 0.042 [39–52] | 0.043 [38–46] | 0.047 [39–44] | |
| Tilt | Obliquity | Rotation | ||||
|---|---|---|---|---|---|---|
| Inclination | Fast: | −0.4 | Fast: | −1 | Fast: | - |
| Slow: | - | Slow: | −1 | Slow: | - | |
| Version | Fast: | +0.8 | Fast: | - | Fast: | +1 |
| Slow: | - | Slow: | - | Slow: | +0.8 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasiljeva, K.; Lunn, D.; Chapman, G.; Redmond, A.; Wang, L.; Thompson, J.; Williams, S.; Wilcox, R.; Jones, A. Dynamic Acetabular Cup Orientation during Gait: A Study of Fast- and Slow-Walking Total Hip Replacement Patients. Bioengineering 2024, 11, 151. https://doi.org/10.3390/bioengineering11020151
Vasiljeva K, Lunn D, Chapman G, Redmond A, Wang L, Thompson J, Williams S, Wilcox R, Jones A. Dynamic Acetabular Cup Orientation during Gait: A Study of Fast- and Slow-Walking Total Hip Replacement Patients. Bioengineering. 2024; 11(2):151. https://doi.org/10.3390/bioengineering11020151
Chicago/Turabian StyleVasiljeva, Ksenija, David Lunn, Graham Chapman, Anthony Redmond, Lin Wang, Jonathan Thompson, Sophie Williams, Ruth Wilcox, and Alison Jones. 2024. "Dynamic Acetabular Cup Orientation during Gait: A Study of Fast- and Slow-Walking Total Hip Replacement Patients" Bioengineering 11, no. 2: 151. https://doi.org/10.3390/bioengineering11020151
APA StyleVasiljeva, K., Lunn, D., Chapman, G., Redmond, A., Wang, L., Thompson, J., Williams, S., Wilcox, R., & Jones, A. (2024). Dynamic Acetabular Cup Orientation during Gait: A Study of Fast- and Slow-Walking Total Hip Replacement Patients. Bioengineering, 11(2), 151. https://doi.org/10.3390/bioengineering11020151