
Coronal Knee Alignment and Tibial Rotation in Total Knee Arthroplasty: A Prospective Cohort Study of Patients with End-Stage Osteoarthritis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
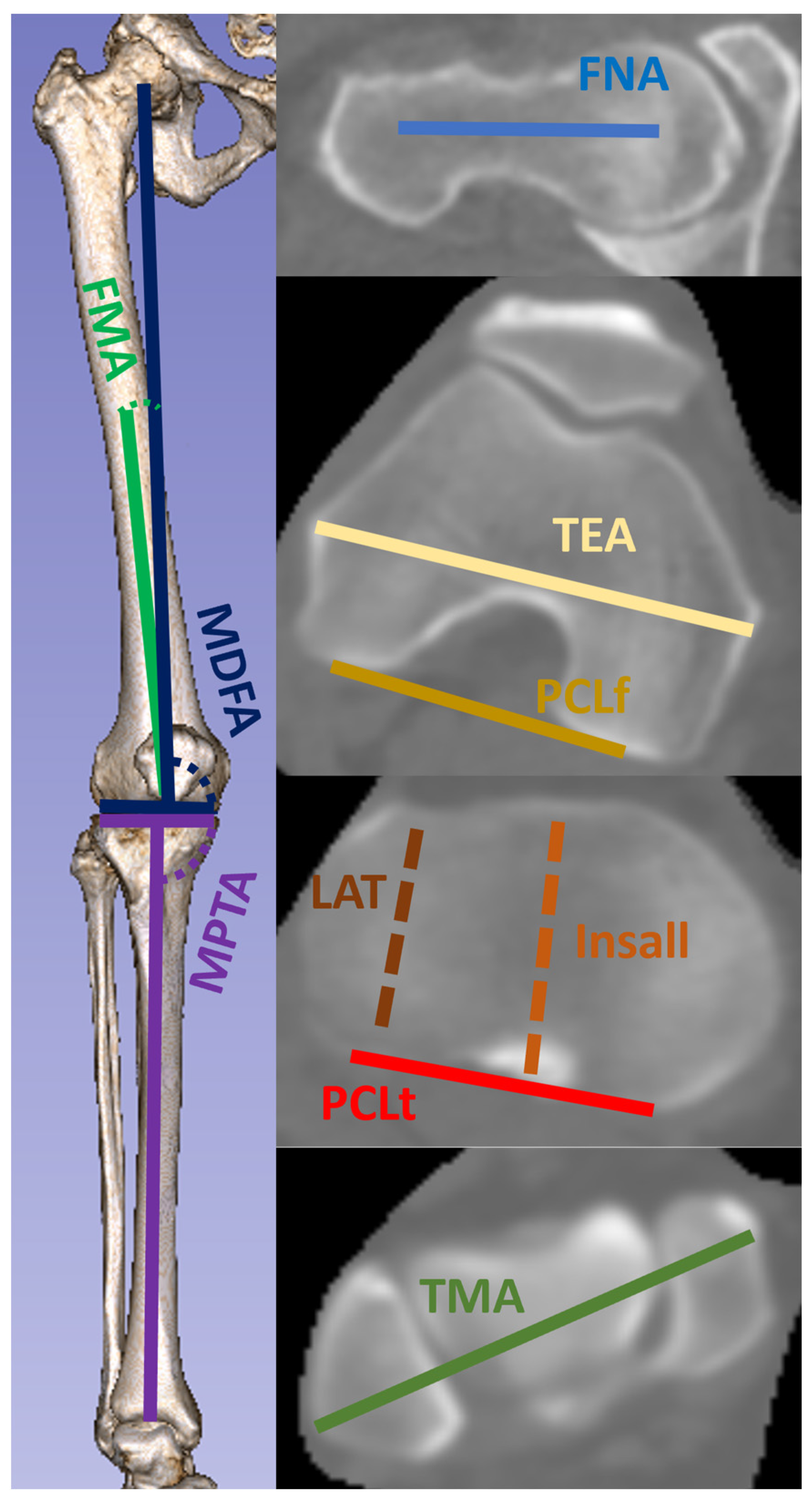
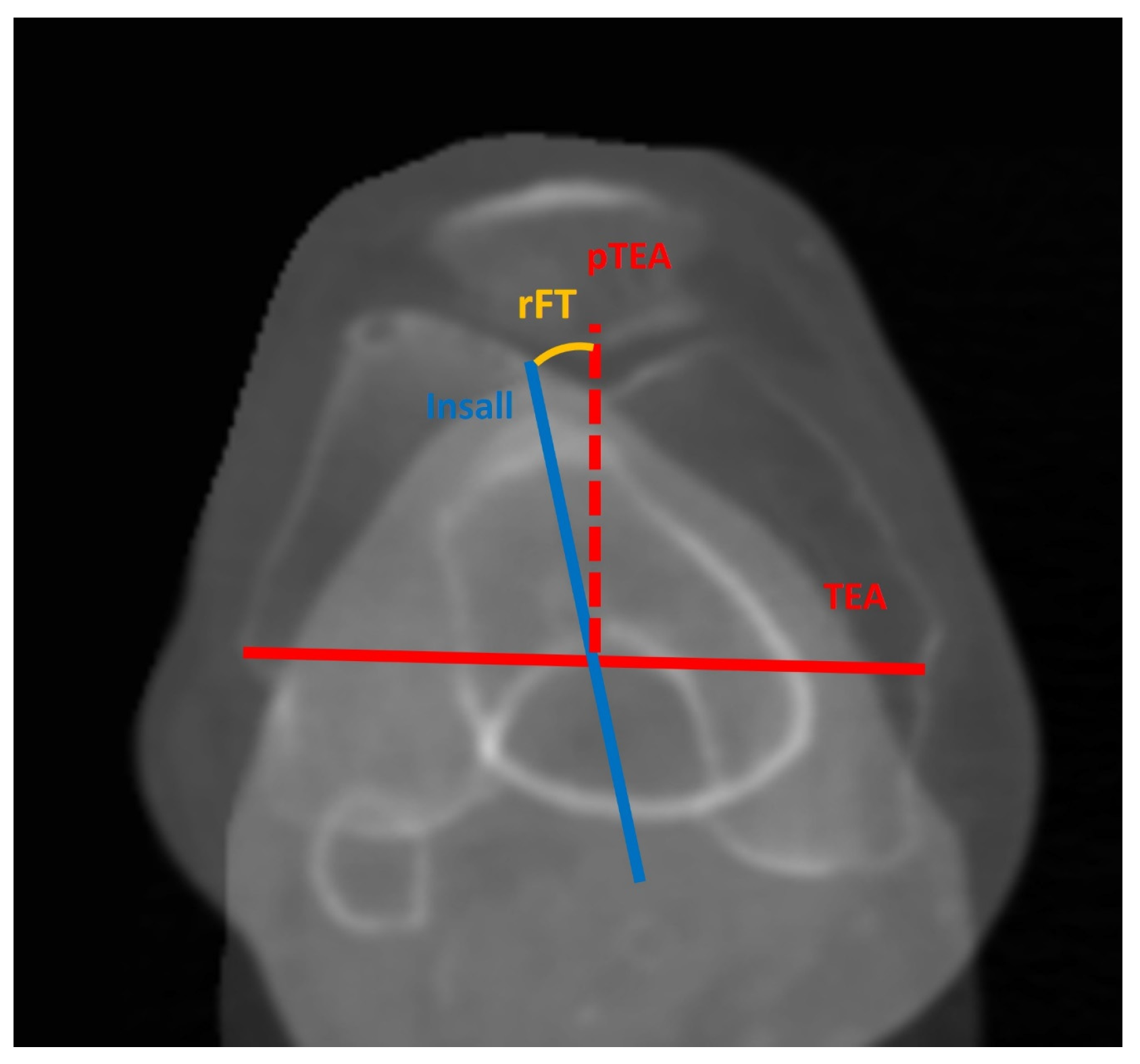
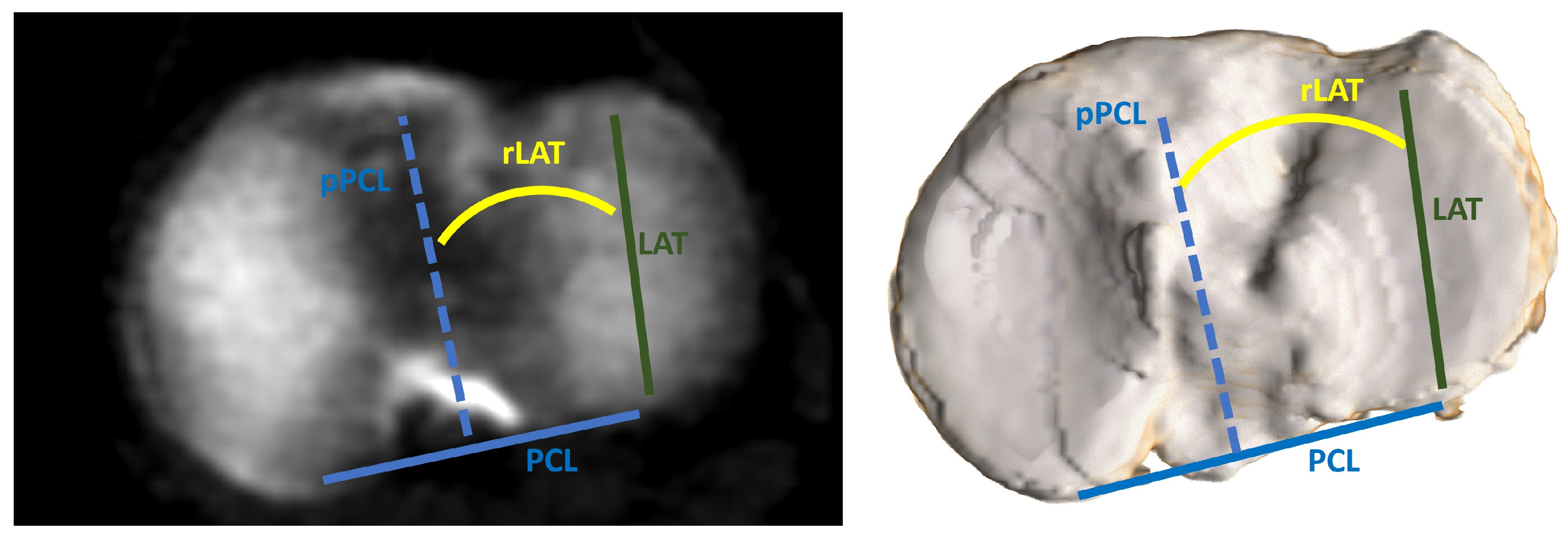
2.2. Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes 2021, 11, 854. [Google Scholar] [CrossRef] [PubMed]
- Guilak, F. Biomechanical factors in osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2011, 25, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Klug, A.; Gramlich, Y.; Rudert, M.; Drees, P.; Hoffmann, R.; Weißenberger, M.; Kutzner, K.P. The projected volume of primary and revision total knee arthroplasty will place an immense burden on future health care systems over the next 30 years. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 29, 3287–3298. [Google Scholar] [CrossRef] [PubMed]
- Panni, A.S.; Ascione, F.; Rossini, M.; Braile, A.; Corona, K.; Vasso, M.; Hirschmann, M.T. Tibial internal rotation negatively affects clinical outcomes in total knee arthroplasty: A systematic review. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 1636–1644. [Google Scholar] [CrossRef] [PubMed]
- Steinbrück, A.; Schröder, C.; Woiczinski, M.; Müller, T.; Müller, P.E.; Jansson, V.; Fottner, A. Influence of tibial rotation in total knee arthroplasty on knee kinematics and retropatellar pressure: An in vitro study. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, S.; Ishikawa, M.; Furu, M.; Ito, H.; Matsuda, S. Malrotated tibial component increases medial collateral ligament tension in total knee arthroplasty. J. Orthop. Res. 2014, 32, 1658–1666. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.W.; Young, P.; Drury, C.; Smith, J.; Anthony, I.; Jones, B.; Blyth, M.; McLean, A. Component rotational alignment in unexplained painful primary total knee arthroplasty. Knee 2014, 21, 272–277. [Google Scholar] [CrossRef]
- Bédard, M.; Vince, K.G.; Redfern, J.; Collen, S.R. Internal Rotation of the Tibial Component is Frequent in Stiff Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2011, 469, 2346–2355. [Google Scholar] [CrossRef]
- Abdelnasser, M.K.; Adi, M.M.; Elnaggar, A.A.; Tarabichi, S. Internal rotation of the tibial component in total knee arthroplasty can lead to extension deficit. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 2948–2952. [Google Scholar] [CrossRef]
- Nicoll, D.; Rowley, D.I. Internal rotational error of the tibial component is a major cause of pain after total knee replacement. J. Bone Jt. Surg. 2010, 92, 1238–1244. [Google Scholar] [CrossRef]
- Popescu, R.; Haritinian, E.G.; Cristea, S. Methods of intra- and post-operative determination of the position of the tibial component during total knee replacement. Int. Orthop. 2020, 44, 119–128. [Google Scholar] [CrossRef]
- Lützner, J.; Krummenauer, F.; Günther, K.-P.; Kirschner, S. Rotational alignment of the tibial component in total knee arthroplasty is better at the medial third of tibial tuberosity than at the medial border. BMC Musculoskelet. Disord. 2010, 11, 57. [Google Scholar] [CrossRef]
- Jang, E.S.; Davignon, R.; Geller, J.A.; Cooper, H.J.; Shah, R.P. Reference Axes for Tibial Component Rotation in Total Knee Arthroplasty: Computed Tomography-Based Study of 1351 Tibiae. J. Bone Jt. Surg. Am. 2023, 105, 1–8. [Google Scholar] [CrossRef]
- Ma, Y.; Mizu-Uchi, H.; Ushio, T.; Hamai, S.; Akasaki, Y.; Murakami, K.; Nakashima, Y. Bony landmarks with tibial cutting surface are useful to avoid rotational mismatch in total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 1570–1579. [Google Scholar] [CrossRef]
- Bonnin, M.P.; Saffarini, M.; Mercier, P.E.; Laurent, J.R.; Carrillon, Y. Is the anterior tibial tuberosity a reliable rotational landmark for the tibial component in total knee arthroplasty? J. Arthroplast. 2011, 26, 260–267.e1-2. [Google Scholar] [CrossRef] [PubMed]
- Howell, S.M.; Chen, J.; Hull, M.L. Variability of the location of the tibial tubercle affects the rotational alignment of the tibial component in kinematically aligned total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2013, 21, 2288–2295. [Google Scholar] [CrossRef]
- Nam, J.-H.; Koh, Y.-G.; Kim, P.S.; Kim, G.; Kwak, Y.H.; Kang, K.-T. Evaluation of tibial rotational axis in total knee arthroplasty using magnetic resonance imaging. Sci. Rep. 2020, 10, 14068. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Howell, S.M.; Hull, M.L. Does Malrotation of the Tibial and Femoral Components Compromise Function in Kinematically Aligned Total Knee Arthroplasty? Orthop. Clin. N. Am. 2016, 47, 41–50. [Google Scholar] [CrossRef]
- Siston, R.A.; Goodman, S.B.; Patel, J.J.; Delp, S.L.; Giori, N.J. The High Variability of Tibial Rotational Alignment in Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2006, 452, 65–69. [Google Scholar] [CrossRef]
- Baldini, A.; Indelli, P.F.; DELuca, L.; Mariani, P.C.; Marcucci, M. Rotational alignment of the tibial component in total knee arthroplasty: The anterior tibial cortex is a reliable landmark. Joints 2013, 1, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Akagi, M.; Oh, M.; Nonaka, T.; Tsujimoto, H.; Asano, T.; Hamanishi, C. An Anteroposterior Axis of the Tibia for Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2004, 420, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Feczko, P.Z.; Pijls, B.G.; van Steijn, M.J.; van Rhijn, L.W.; Arts, J.J.; Emans, P.J. Tibial component rotation in total knee arthroplasty. BMC Musculoskelet. Disord. 2016, 17, 87. [Google Scholar] [CrossRef] [PubMed]
- Ikeuchi, M.; Yamanaka, N.; Okanoue, Y.; Ueta, E.; Tani, T. Determining the rotational alignment of the tibial component at total knee replacement: A comparison of two techniques. J. Bone Jt. Surg. Br. 2007, 89, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Kawahara, S.; Okazaki, K.; Matsuda, S.; Mitsuyasu, H.; Nakahara, H.; Okamoto, S.; Iwamoto, Y. Medial sixth of the patellar tendon at the tibial attachment is useful for the anterior reference in rotational alignment of the tibial component. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1070–1075. [Google Scholar] [CrossRef] [PubMed]
- Saffarini, M.; Nover, L.; Tandogan, R.; Becker, R.; Moser, L.B.; Hirschmann, M.T.; Indelli, P.F. The original Akagi line is the most reliable: A systematic review of landmarks for rotational alignment of the tibial component in TKA. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- András, G.; Németh, G.; Oláh, C.Z.; Lénárt, G.; Drén, Z.; Papp, M. The personalized Berger method is usable to solve the problem of tibial rotation. J. Exp. Orthop. 2021, 8, 116. [Google Scholar] [CrossRef] [PubMed]
- Ohmori, T.; Kabata, T.; Kajino, Y.; Inoue, D.; Taga, T.; Yamamoto, T.; Takagi, T.; Yoshitani, J.; Ueno, T.; Ueoka, K.; et al. A proposed new rotating reference axis for the tibial component after proximal tibial resection in total knee arthroplasty. PLoS ONE 2018, 13, e0209317. [Google Scholar] [CrossRef]
- Booth, R.E. Rotational Issues in Total Knee Arthroplasty: Commentary on an article by Eugene S. Jang, MD, MS, et al.: “Reference Axes for Tibial Component Rotation in Total Knee Arthroplasty. Computed Tomography-Based Study of 1351 Tibiae”. J. Bone Jt. Surg. Am. 2023, 105, 87. [Google Scholar] [CrossRef]
- Chang, M.J.; Jeong, H.J.; Kang, S.-B.; Chang, C.B.; Yoon, C.; Shin, J.Y. Relationship Between Coronal Alignment and Rotational Profile of Lower Extremity in Patients With Knee Osteoarthritis. J. Arthroplast. 2018, 33, 3773–3777. [Google Scholar] [CrossRef]
- Luyckx, T.; Zambianchi, F.; Catani, F.; Bellemans, J.; Victor, J. Coronal alignment is a predictor of the rotational geometry of the distal femur in the osteo-arthritic knee. Knee Surg. Sport. Traumatol. Arthrosc. 2013, 21, 2331–2337. [Google Scholar] [CrossRef]
- Thienpont, E.; Schwab, P.-E.; Paternostre, F.; Koch, P. Rotational alignment of the distal femur: Anthropometric measurements with CT-based patient-specific instruments planning show high variability of the posterior condylar angle. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 2995–3002. [Google Scholar] [CrossRef]
- Ueyama, H.; Minoda, Y.; Sugama, R.; Ohta, Y.; Yamamura, K.; Nakamura, S.; Takemura, S.; Nakamura, H. Malrotation of the fixed-bearing posterior stabilized total knee prosthesis causes a postoperative rotational mismatch between the femur and tibia. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3810–3820. [Google Scholar] [CrossRef]
- Abdelnasser, M.K.; Elsherif, M.E.; Bakr, H.; Mahran, M.; Othman, M.H.M.; Khalifa, Y. All types of component malrotation affect the early patient-reported outcome measures after total knee arthroplasty. Knee Surg. Relat. Res. 2019, 31, 5. [Google Scholar] [CrossRef]
- Kawaguchi, K.; Inui, H.; Taketomi, S.; Yamagami, R.; Kono, K.; Sameshima, S.; Kage, T.; Tanaka, S. Preoperative tibiofemoral rotational alignment is a risk factor for component rotational mismatch in total knee arthroplasty. Knee 2021, 29, 448–456. [Google Scholar] [CrossRef]
- Howell, S.M.; Howell, S.J.; Kuznik, K.T.; Cohen, J.; Hull, M.L. Does a kinematically aligned total knee arthroplasty restore function without failure regardless of alignment category? Clin. Orthop. Relat. Res. 2013, 471, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Singh, A.K.; Howell, S.M.; Hull, M.L. Does Calipered Kinematically Aligned TKA Restore Native Left to Right Symmetry of the Lower Limb and Improve Function? J. Arthroplast. 2018, 33, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Rivière, C.; Iranpour, F.; Auvinet, E.; Howell, S.; Vendittoli, P.-A.; Cobb, J.; Parratte, S. Alignment options for total knee arthroplasty: A systematic review. Orthop. Traumatol. Surg. Res. 2017, 103, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Nedopil, A.J.; Howell, S.M.; Rudert, M.; Roth, J.; Hull, M.L. How frequent is rotational mismatch within 0° ± 10° in kinematically aligned total knee arthroplasty? Orthopedics 2013, 36, e1515–e1520. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Fürmetz, J.; Sass, J.; Ferreira, T.; Jalali, J.; Kovacs, L.; Mück, F.; Degen, N.; Thaller, P. Three-dimensional assessment of lower limb alignment: Accuracy and reliability. Knee 2019, 26, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Ariumi, A.; Sato, T.; Kobayashi, K.; Koga, Y.; Omori, G.; Minato, I.; Endo, N. Three-dimensional lower extremity alignment in the weight-bearing standing position in healthy elderly subjects. J. Orthop. Sci. 2010, 15, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Degen, N.; Sass, J.; Jalali, J.; Kovacs, L.; Euler, E.; Prall, W.; Böcker, W.; Thaller, P.; Fürmetz, J. Three-dimensional assessment of lower limb alignment: Reference values and sex-related differences. Knee 2020, 27, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Kadoya, Y.; Uehara, K.; Kobayashi, A.; Takaoka, K. Rotational deformity in varus osteoarthritis of the knee: Analysis with computed tomography. Clin. Orthop. Relat. Res. 2005, 433, 147–151. [Google Scholar] [CrossRef]
- Khan, M.S.; Seon, J.K.; Song, E.K. Rotational Profile of Lower Limb and Axis for Tibial Component Alignment in Varus Osteoarthritic Knees. J. Arthroplast. 2012, 27, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Nejima, S.; Akamatsu, Y.; Kobayashi, H.; Tsuji, M.; Mitsuhashi, S.; Sasaki, T.; Kumagai, K.; Inaba, Y. Relationship between lower limb torsion and coronal morphologies of the femur and tibia in patients with medial knee osteoarthritis. BMC Musculoskelet. Disord. 2020, 21, 254. [Google Scholar] [CrossRef]
- Huang, C.; Chan, P.-K.; Chiu, K.-Y.; Yan, C.-H.; Yeung, S.-S.; Lai, C.W.-K.; Leung, A.K.-L.; Fu, S.N. The association between tibial torsion, knee flexion excursion and foot progression during gait in people with knee osteoarthritis: A cross-sectional study. BMC Sport. Sci. Med. Rehabil. 2023, 15, 110. [Google Scholar] [CrossRef]
- Bretin, P.; O’loughlin, P.F.; Suero, E.M.; Kendoff, D.; Ostermeier, S.; Hüfner, T.; Krettek, C.; Citak, M. Influence of femoral malrotation on knee joint alignment and intra-articular contract pressures. Arch. Orthop. Trauma Surg. 2011, 131, 1115–1120. [Google Scholar] [CrossRef]
- Kenawey, M.; Liodakis, E.; Krettek, C.; Ostermeier, S.; Horn, T.; Hankemeier, S. Effect of the lower limb rotational alignment on tibiofemoral contact pressure. Knee Surg. Sport. Traumatol. Arthrosc. 2011, 19, 1851–1859. [Google Scholar] [CrossRef]
- Yazdi, H.; Mallakzadeh, M.; Farshidfar, S.S.; Givehchian, B.; Daneshparvar, H.; Behensky, H. The effect of tibial rotation on knee medial and lateral compartment contact pressure. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 79–83. [Google Scholar] [CrossRef]
- Nagamine, R.; Kawasaki, M.; Kim, K.-I.; Sakai, A.; Suguro, T. The posterior tibial slope is mainly created by the posterior rotation of the tibial condyles. J. Orthop. Surg. 2020, 28, 2309499020975580. [Google Scholar] [CrossRef]
- Lee, D.-H.; Seo, J.-G.; Moon, Y.-W. Synchronisation of tibial rotational alignment with femoral component in total knee arthroplasty. Int. Orthop. 2008, 32, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, F.; Yoneta, K.; Miyaji, T.; Kidera, K.; Yonekura, A.; Osaki, M.; Gamada, K. Knee kinematics of severe medial knee osteoarthritis showed tibial posterior translation and external rotation: A cross-sectional study. Aging Clin. Exp. Res. 2020, 32, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Misir, A.; Yildiz, K.I.; Kizkapan, T.B.; Incesoy, M.A. Kellgren–Lawrence grade of osteoarthritis is associated with change in certain morphological parameters. Knee 2020, 27, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Dong, T.; Chen, W.; Zhang, F.; Yin, B.; Tian, Y.; Zhang, Y. Radiographic measures of settlement phenomenon in patients with medial compartment knee osteoarthritis. Clin. Rheumatol. 2016, 35, 1573–1578. [Google Scholar] [CrossRef]
- Ma, W.; Wang, F.; Sun, S.; Ding, L.; Wang, L.; Yu, T.; Zhang, Y. Novel ideas for the comprehensive evaluation of varus knee osteoarthritis: Radiological measurements of the morphology of the lateral knee joint. J. Orthop. Surg. Res. 2023, 18, 196. [Google Scholar] [CrossRef]
- Wernecke, G.C.; Harrris, I.A.; Seeto, B.G.; Chen, D.B.; MacDessi, S.J. Normal Femorotibial Rotational Alignment and Implications for Total Knee Arthroplasty: An MRI Analysis. HSS J. 2016, 12, 216–222. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients, n | 112 |
| Knees, n | 199 |
| Age, years | 69.7 ± 7.9 (49–84) |
| Gender, female/male | 111/88 |
| Side, right/left | 100/99 |
| Kellgren–Lawrence, n-grade 2/3/4 | 20/67/112 |
| HKA-X, ° | 176.2 ± 7.0 (160.4–197.6) |
| aHKA, ° | 181.2 ± 4.1 (171.0–191.9) |
| MDFA, ° | 92.8 ± 2.5 (86.6–100.7) |
| MPTA, ° | 88.5 ± 2.6 (81.7–95.8) |
| FMA, ° | 6.1 ± 1.5 (2.6–11.4) |
| CTA, ° | 4.2 ± 1.7 (0.6–8.2) |
| tF, ° | 12.3 ± 7.7 (−13.2–34.2) |
| tT, ° | −25.9 ± 8.4 (−57.5–-4.4) |
| Medial tibial slope, ° | 82.8 ± 3.8 (70.7–92.7) |
| Lateral tibial slope, ° | 84.1 ± 3.7 (72.3–95.2) |
| rFT, ° | −6.7 ± 4.7 (−19.1–3.7) |
| rLAT, ° | −6.5 ± 3.3 (−13.0–3.8) |
| ICC | 95% Confidence Interval | |
|---|---|---|
| HKA-X | 0.99 | 0.98–1.0 |
| aHKA | 0.99 | 0.99–0.99 |
| MDFA | 0.99 | 0.99–1.0 |
| MPTA | 0.99 | 0.98–1.0 |
| FMA | 0.99 | 0.99–0.99 |
| CTA | 0.87 | 0.83–0.90 |
| tF | 0.97 | 0.97–0.98 |
| tT | 0.98 | 0.97–0.98 |
| rFT | 0.93 | 0.91–0.95 |
| LAT | 0.91 | 0.88–0.93 |
| rFT | rLAT | tF | tT | CTA | |
|---|---|---|---|---|---|
| HKA-X | 0.21, 0.005 | 0.14, 0.05 | 0.04, 0.56 | −0.05, 0.48 | 0.04, 0.55 |
| aHKA | 0.30, <0.001 | 0.23, 0.001 | −0.07, 0.35 | −0.01, 0.84 | −0.01, 0.99 |
| MDFA | 0.09, 0.21 | 0.04, 0.62 | 0.02, 0.74 | −0.22, 0.002 | 0.32, <0.001 |
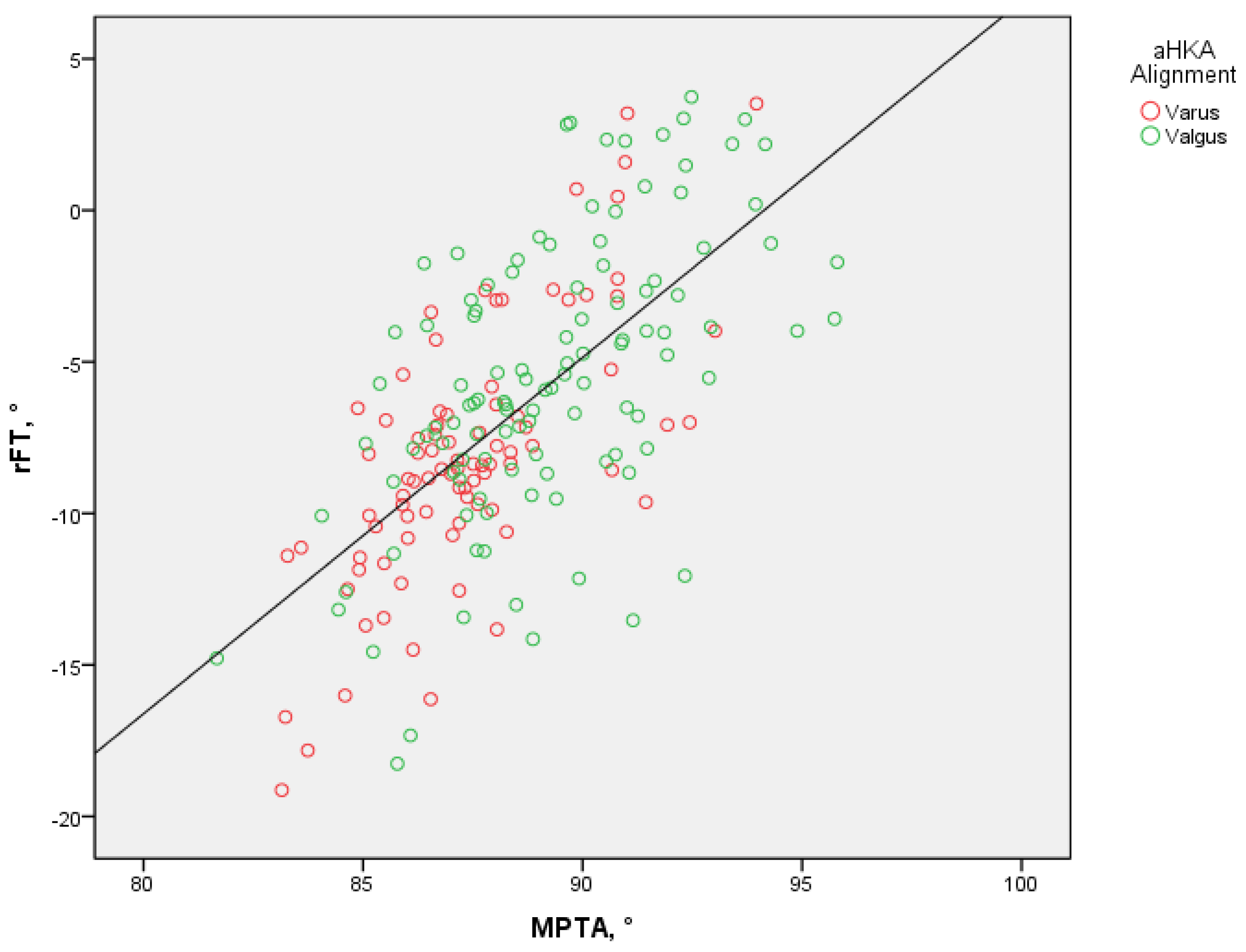
| MPTA | 0.66, <0.001 | 0.44, <0.001 | −0.29, <0.001 | 0.21, 0.003 | −0.07, 0.35 |
| FMA | −0.18, 0.01 | −0.15, 0.04 | 0.06, 0.39 | 0.04, 54 | −0.10, 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strahovnik, A.; Strahovnik, I.; Fokter, S.K. Coronal Knee Alignment and Tibial Rotation in Total Knee Arthroplasty: A Prospective Cohort Study of Patients with End-Stage Osteoarthritis. Bioengineering 2024, 11, 296. https://doi.org/10.3390/bioengineering11030296
Strahovnik A, Strahovnik I, Fokter SK. Coronal Knee Alignment and Tibial Rotation in Total Knee Arthroplasty: A Prospective Cohort Study of Patients with End-Stage Osteoarthritis. Bioengineering. 2024; 11(3):296. https://doi.org/10.3390/bioengineering11030296
Chicago/Turabian StyleStrahovnik, Andrej, Igor Strahovnik, and Samo Karel Fokter. 2024. "Coronal Knee Alignment and Tibial Rotation in Total Knee Arthroplasty: A Prospective Cohort Study of Patients with End-Stage Osteoarthritis" Bioengineering 11, no. 3: 296. https://doi.org/10.3390/bioengineering11030296
APA StyleStrahovnik, A., Strahovnik, I., & Fokter, S. K. (2024). Coronal Knee Alignment and Tibial Rotation in Total Knee Arthroplasty: A Prospective Cohort Study of Patients with End-Stage Osteoarthritis. Bioengineering, 11(3), 296. https://doi.org/10.3390/bioengineering11030296