
Biomechanical Considerations in the Orthodontic Treatment of a Patient with Stabilised Stage IV Grade C Generalised Periodontitis: A Case Report

 ,
,
Abstract
:1. Introduction
2. Materials and methods
Case Report
3. Treatment Objectives
4. Treatment Progress
4.1. Pre-Orthodontic Dental Treatment Preparation
4.2. Anchorage Design
4.3. Biomechanical Planning
4.4. Additional Dental Treatments
4.5. Retention
5. Discussion
- (1)
- Challenges and precautions in maintaining stable periodontal health in patient with Stage IV grade C generalised periodontitis throughout the orthodontic treatment
- (1.1)
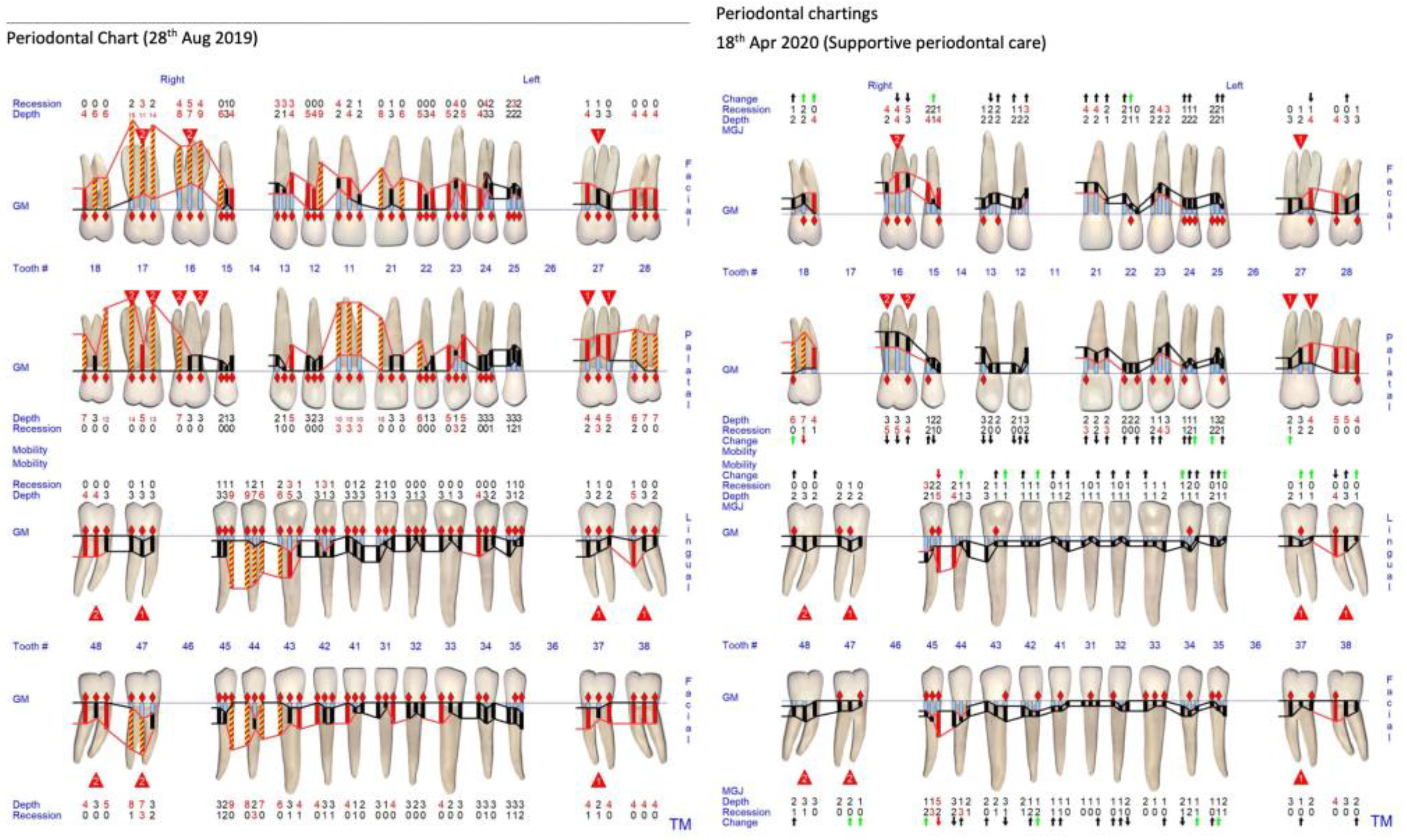
- Before beginning the orthodontic treatment, clinical and radiographic periodontal assessment was performed by the periodontal colleague to confirm that the patient’s periodontal condition had been stabilised after the series of non-surgical and surgical periodontal therapies. Clinical examination included full mouth probing, tooth mobility assessment, and measurement of the amount of gingival recession. The full mouth plaque and bleeding on probing scores were below 25% before beginning the orthodontic treatment [39,40].
- (1.2)
- During orthodontic treatment, oral hygiene instruction and motivation was performed after placement of the orthodontic appliance. The first stage of orthodontic treatment was to upright the buccally flared teeth 24 and 25 using the cantilever mechanics. In this stage, we placed a CoCr plate covering the palatal surface of teeth 24 and 25. The bulkiness of the CoCr plate will hinder the patient’s cleaning efficiency and predispose the area to food entrapment. Emphasising the importance of meticulous oral hygiene in this area became imperative. During every visit, the oral hygiene status of the patient was checked by the orthodontic colleague. Regular periodontal recall appointments were also carried out every three months by the periodontal colleague [39,40]. In the second stage of the orthodontic treatment, the upper and lower teeth were bonded with fixed labial orthodontic brackets. The usage of fixed labial orthodontic brackets and wire created a difficult situation for the patient in performing optimal oral hygiene. The gingival margins and interdental areas were often blocked by the orthodontic appliances. Additional oral hygiene aids including waterfloss and superfloss were used when the patient could not clean with regular aids, like a toothbrush, ID brush, or single tuft brush. At some particular point in time, gingivae may present with more marginal inflammation, thus slightly increased pocket depth due to edema. As precautions, supportive periodontal care was carried out strictly every 3 months, and all the sites with orthodontic appliances were deplaqued thoroughly, to maintain a reasonable periodontal health to prevent periodontal flare up during orthodontic treatment.
- (1.3)
- (2)
- Challenges and precautions in treating orthodontic case with supernumerary tooth
- (2.1)
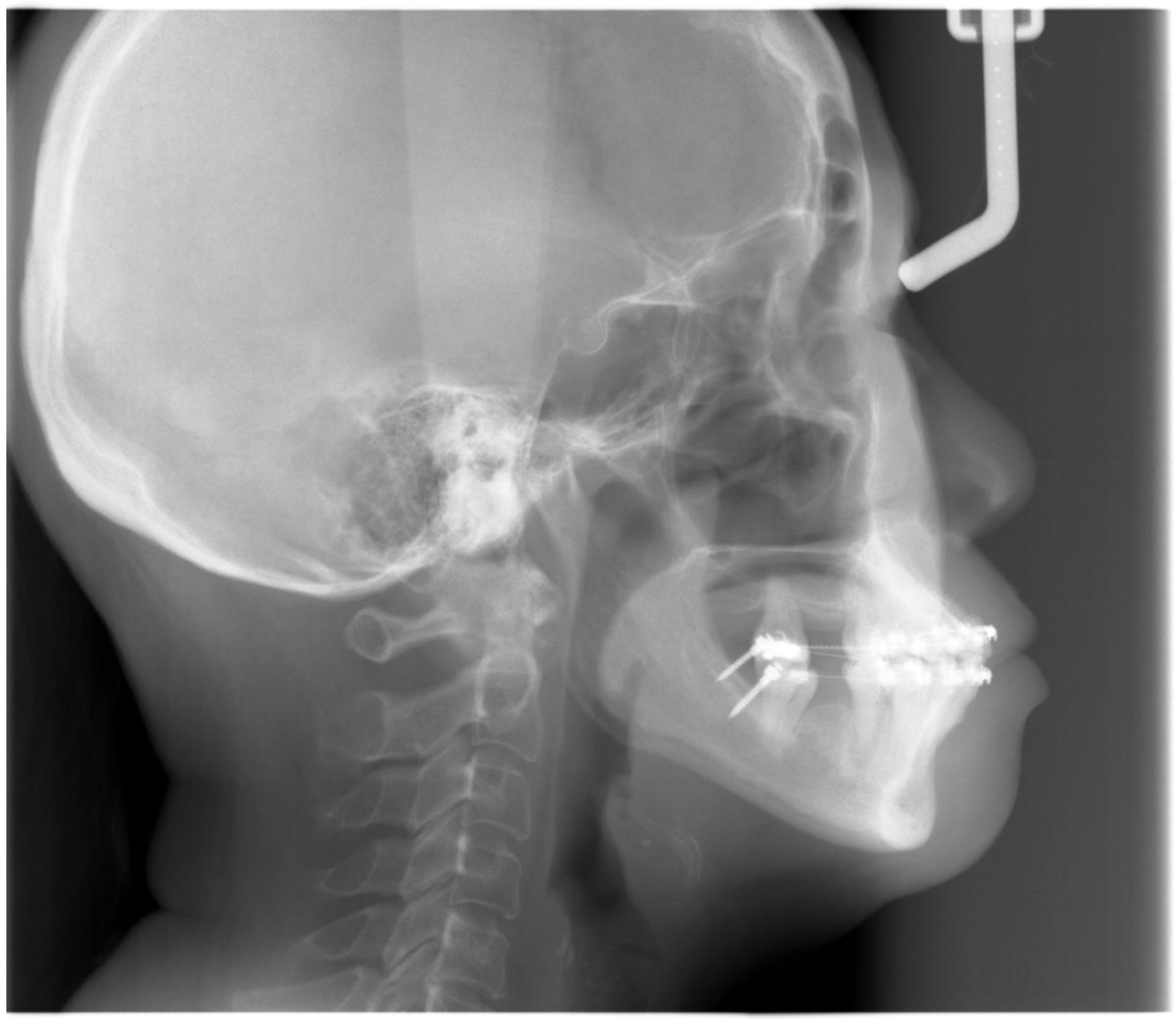
- The patient refused to surgically extract the supernumerary tooth as the supernumerary tooth was not associated with any pathology in the patient’s upper jaw for more than 59 years. The decision to keep the supernumerary tooth did affect the planned retraction of upper incisors. This meant that we could not retract the upper incisors as much as we had planned to based on the VTO. As a precaution, radiographs were taken regularly during the orthodontic treatment to ensure that there was no pathology with the supernumerary tooth and the supernumerary tooth did not affect the movement of the upper anterior teeth. As the mid-treatment orthopantomogram (Figure 12) showed that the root apex of tooth 23 was very close to the supernumerary tooth, we decided to stop further retracting the upper teeth.
- (3)
- Challenges in planning the orthodontic biomechanics when treating patient with Stage IV grade C generalised periodontitis
- (3.1)
- The first biomechanical challenge involves obtaining adequate dental anchorage for orthodontic movement, as patients often present with multiple missing teeth and reduced periodontal support due to periodontal disease [26]. In this case, the reinforcement of anchorage through alternative means, such as temporary anchorage devices (TADs) and using tooth 16 as free anchorage, was performed.
- (3.2)
- (3.3)
- The third biomechanical challenge relates to the apically shifted centre of resistance (Cres) of a periodontally compromised tooth, as the alveolar bone height is decreased, which increases the M/F [24,27]. Consequently, there is an increased tendency for such teeth to tip and rotate excessively in response to orthodontic forces, which are applied at the regular bracket level, leading to unwanted tooth movement and excessive friction during space closure with sliding mechanics.
- (3.4)
- During the treatment of this patient with Stage IV Grade C generalised periodontitis, we addressed the biomechanical challenges outlined in lists 3.1 to 3.3 at four specific time points.
- (3.4.1)
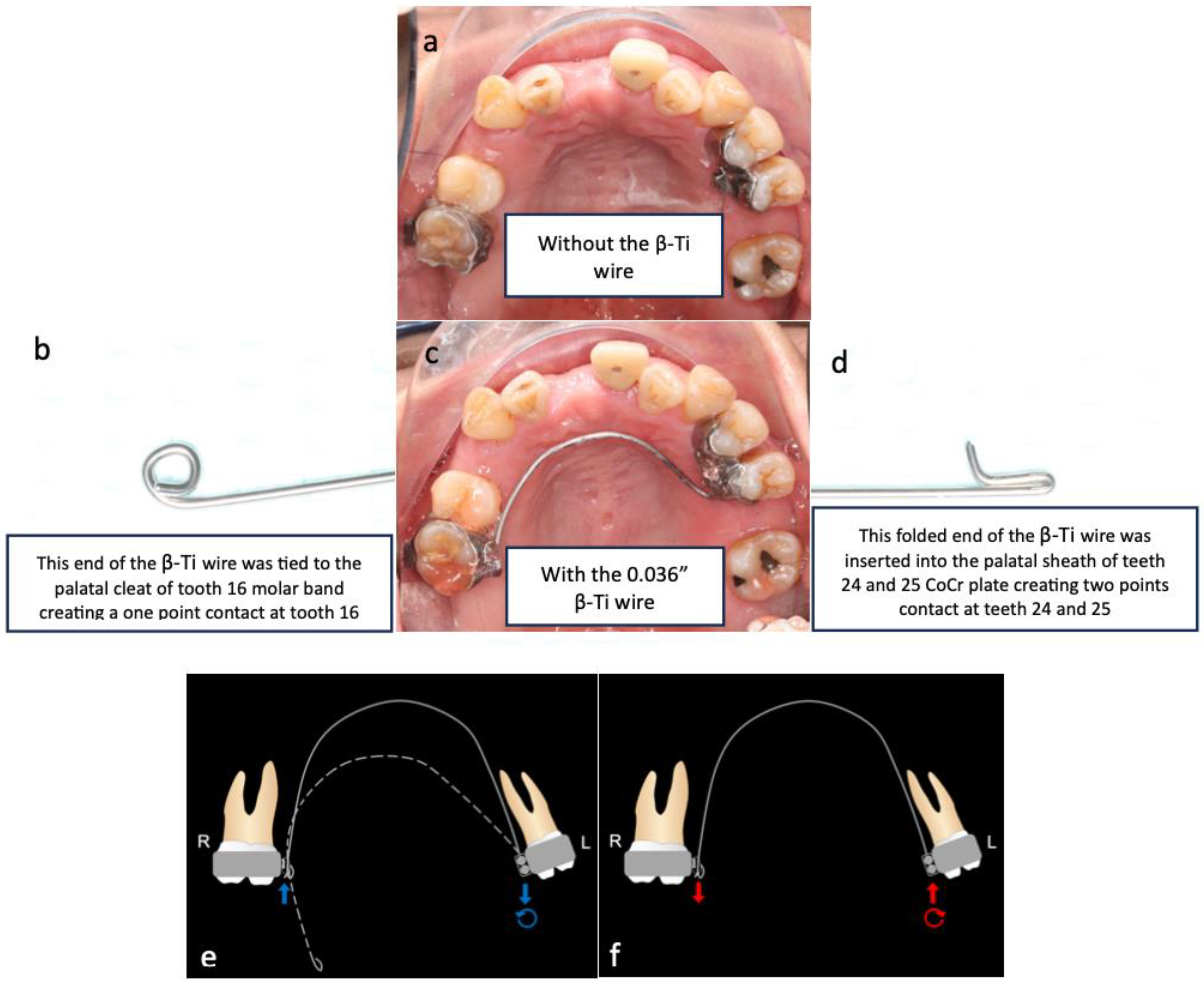
- As teeth 24 and 25 were significantly buccally displaced, sectional cantilever mechanics were used rather than direct bonding of the entire upper arch. There were two reasons for this. The first reason was to avoid creating unfavourable force systems on the other teeth due to the buccally displaced positions of teeth 24 and 25. Bonding brackets onto all upper teeth and engaging them with a straight wire could have resulted in an abnormal or skewed arch form. The second reason was that tooth 16 had a poor prognosis and was to be extracted in the future. Therefore, we decided to use tooth 16 as free anchorage to bring teeth 24 and 25 into the planned archform with cantilever mechanics, before proceeding with straight wire mechanics.
- (3.4.2)
- During the alignment and levelling stage, tooth 35’s crown was displaced distally and rotated disto-bucally, so a box loop capable of delivering the desired magnitude of force and precisely regulating the force direction was used. The box loop increased the total amount of wire between brackets of teeth 34 and 35, which produced a reduced load–deflection ratio and a greater range of action than any other loop type [41]. Furthermore, as the box loop was composed of a series of vertical and horizontal levers contoured to provide a short section of archwire that was freely movable in all planes in which it was activated, we used it to tip the crown of tooth 35 mesially and rotate tooth 35 mesio-lingually [41]. Moreover, sufficient anchorage was provided by the relatively rigid, continuous wire portion adjacent to the box loop, spanning from teeth 34 to 45, which effectively differentiated the active and reactive units.
- (3.4.3)
- As discussed in list 3.3, periodontally compromised teeth would tip excessively in response to orthodontic force which is applied at the regular bracket level. Therefore, if the aim is to achieve bodily retraction of incisors, it is best to bond the brackets as cervically as possible. However, since the pre-treatment upper and lower incisors were proclined, we aimed to achieve ‘uncontrolled tipping’ during retraction, and thus, the brackets were bonded at the regular positions on the upper and lower incisors [42].
- (3.4.4)
- The attempted placement of mini-screws on the upper alveolar bone resulted in dislodgement due to the low sinus floor. This was caused by sinus peumatization which was a continuous physiological process that increased the volume of the paranasal sinuses [43]. To address this, lower buccal shelf mini-screws were used instead to retract the upper arch with Class I elastics.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhong, H.; Jiang, H.J.; Pan, Y.Z. Aesthetic effect of orthodontics treatment combined with periodontal splint in the treatment of fan-shaped displacement of anterior teeth caused by periodontitis. Shanghai Kou Qiang Yi Xue 2019, 28, 417–421. [Google Scholar] [PubMed]
- Jin, L. Periodontic-orthodontic interactions-rationale, sequence and clinical implications. Hong Kong Dent. J. 2007, 4, 60–64. [Google Scholar]
- Feu, D. Orthodontic treatment of periodontal patients: Challenges and solutions, from planning to retention. Dent. Press J. Orthod. 2020, 25, 79–116. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: An overview. Periodontology 2000, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Brunsvold, M.A. Pathologic tooth migration. J. Periodontol. 2005, 76, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Melsen, B.; Agerbaek, N.; Asboe, V. The orthodontic treatment of malocclusion in patients with previous periodontal disease. Br. J. Orthod. 1982, 9, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Wagenberg, B.D.; Eskow, R.N.; Langer, B. Orthodontic procedures that improve the periodontal prognosis. J. Am. Dent. Assoc. 1980, 100, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Shi, J.; Xu, L.; Jiao, J.; Lu, R.F.; Meng, H.X. Clinical evaluation of periodontal-orthodontic treatment in patients with aggressive periodontitis and malocclusion. Beijing Da Xue Xue Bao Yi Xue Ban 2017, 49, 60–66. [Google Scholar]
- Long, H.; Wang, Y.; Jian, F.; Liao, L.; Yang, X.; Lai, W.L. Current advances in orthodontic pain. J. Oral. Sci. 2016, 8, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Kidd, E.A.M.; Smith, B.G.N.; Watson, T. Pickard’s Manual of Operative Dentistry, 6th ed.; Oxford Medical Publications: Oxford, UK, 1991. [Google Scholar]
- Goldstein, L.; Gilbert, S. Tooth loss in the chronic pain population. Pract. Pain Manag. 2019, 12. Available online: https://www.practicalpainmanagement.com/tooth-loss-chronic-pain-population (accessed on 25 March 2024).
- Uematsu, S.; Mogi, M.; Deguchi, T. Interleukin (IL)-1 beta, IL-6, tumor necrosis factor-alpha, epidermal growth factor, and beta 2-microglobulin levels are elevated in gingival crevicular fluid during human orthodontic tooth movement. J. Dent. Res. 1996, 75, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Yoshii, M.; Kasai, K. Relationship between substance P and interleukin-1beta in gingival crevicular fluid during orthodontic tooth movement in adults. Eur. J. Orthod. 2006, 28, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Sum, F.H.K.M.H.; Ren, C.; Gu, M.; Jin, L.; McGrath, C.; Yang, Y. Oral hygiene is associated with orthodontic pain in patients with treated and stabilised periodonntitis. Oral. Health Prev. Dent. 2021, 19, 555–564. [Google Scholar] [PubMed]
- Wennström, J.L.; Stokland, B.L.; Nyman, S.; Thilander, B. Periodontal tissue response to orthodontic movement of teeth with infrabony pockets. Am. J. Orthd. Dentofac. Orthop. 1993, 103, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Thilander, B. Orthodontic forces and recurrence of periodontal disease. An experimental study in the dog. Am. J. Orthod. 1978, 74, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Re, S.; Corrente, G.; Abundo, R.; Cardaropoli, D. Orthodontic treatment in periodontally compromised patients: 12-year report. Int. J. Periodontics Restor. Dent. 2000, 20, 31–39. [Google Scholar]
- Boyd, R.L.; Leggott, P.J.; Quinn, R.S.; Eakle, W.S.; Chambers, D. Periodontal implications of orthodontic treatment in adults with reduced or normal periodontal tissues versus those of adolescents. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 191–198. [Google Scholar] [CrossRef]
- Melsen, B.; Agerbaek, N.; Markenstam, G. Intrusion of incisors in adult patients with marginal bone loss. Am. J. Orthod. Dentofac. Orthop. 1989, 96, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Melsen, B.; Agerbaek, N.; Eriksen, J.; Terp, S. New attachment through periodontal treatment and orthodontic intrusion. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Gkantidis, N.; Christou, P.; Topouzelis, N. The orthodontic-periodontic interrelationship in integrated treatment challenges: A systematic review. J. Oral Rehabil. 2010, 37, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Zachrisson, B.U. Clinical implications of recent orthodontic-periodontic research findings. Semin. Orthod. 1996, 2, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Zasciurinskiene, E.; Lindsten, R.; Slotte, C.; Bjerklin, K. Orthodontic treatment in periodontitis-susceptible subjects: A systematic literature review. Clin. Exp. Dent. Res. 2016, 2, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kim, Y.H.; Lee, K.J.; Hwang, C.J. Effect of labiolingual inclination of a maxillary central incisor and surrounding alveolar bone loss on periodontal stress: A finite element analysis. Korean J. Orthod. 2016, 46, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Bondemark, L. Interdental bone changes after orthodontic treatment: A 5-year longitudinal study. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Gupta, S.; Chugh, V.K.; Jain, E.; Valiathan, A.; Nanda, R. Interdisciplinary treatment of a periodontally compromised adult patient with multiple missing posterior teeth. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Geramy, A. Alveolar bone resorption and the center of resistance modification (3-D analysis by means of the finite element method). Am. J. Orthod. Dentofac. Orthop. 2000, 117, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Ziahosseini, P.; Hussain, F.; Millar, B.J. Management of gingival black triangles. Br. Dent. J. 2014, 217, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.C.; Liao, Y.F.; Chan, C.P.; Ku, Y.C.; Pan, W.L.; Tu, Y.K. Factors influencing the presence of interproximal dental papillae between maxillary anterior teeth. J. Periodontol. 2010, 81, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Awartani, F.A.; Tatakis, D.N. Interdental papilla loss: Treatment by hyaluronic acid gel injection: A case series. Clin. Oral. Investig. 2016, 20, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Sharma, E.; Sharma, A.; Singh, K. The role of subepithelial connective tissue graft for reconstruction of interdental papilla: Clinical study. Singapore Dent. J. 2017, 38, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Sun, C.; Akcali, A.; Meng, X.; Tu, Y.K.; Donos, N. A retrospective study on periodontal disease progression in private practice. J. Clin. Periodontol. 2017, 44, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Kloukos, D.; Eliades, T.; Sculean, A.; Katsaros, C. Indication and timing of soft tissue augmentation at maxillary and mandibular incisors in orthodontic patients. A systematic review. Eur. J. Orthod. 2014, 36, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.S.; Wei, S.H. Cephalometric standards for the Southern Chinese. Eur. J. Orthod. 1988, 10, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Melsen, B. Adult Orthodontics, 1st ed.; Melsen, B., Ed.; Blackwell Publishing Ltd.: Hoboken, NJ, USA, 2012. [Google Scholar]
- She Tsang Tsang, F.; Abunevičiūtė, A.; Fiorelli, G. VIsualizing Treatment Objectives and Treatment Planning Using 2D and 3D Occlusograms. In 3D Diagnosis and Treatment Planning in Orthodontics; Retrouvey, J.M., Abdallah, M.N., Eds.; Springer: Cham, Switzerland, 2021; pp. 195–238. [Google Scholar]
- Lindauer, S.J.; Isaacson, R.J. One-couple orthodontic appliance systems. Semin. Orthod. 1995, 1, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Burstone, C.J.; Koeing, H.A. Force systems from an ideal arch. Am. J. Orthod. 1974, 65, 270–289. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Einy, S.; Zigdon, H.; Aizenbud, D.; Machtei, E.E. Guidelines for periodontal care and follow-up during orthodontic treatment in adolescents and young adults. J. Appl. Oral. Sci. 2012, 20, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Prato, G.P.P.P.; Chambrone, L. Orthodontic treatment in periodontal patients: The use of periodontal gold standards to overcome the “grey zone”. J. Periodontol. 2019, 91, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Prashar, A.; Kaur, S.; Kaur, R. Loops in orthodontics. Int. J. Health Sci. 2021, 5, 74–85. [Google Scholar] [CrossRef]
- Burstone, C.J.C.; Choy, K. The Biomechanical Foundation of Clinical Orthodontics. In The Biomechanical Foundation of Clinical Orthodontics; Huffman, L., Ed.; Quintessence Publishing Co, Inc.: Batavia, IL, USA, 2015; p. 514. [Google Scholar]
- Nimigean, V.; Nimigean, V.R.; Măru, N.; Sălăvăstru, D.I.; Bădiţă, D.; Tuculină, M.J. The maxillary sinus floor in the oral implantology. Rom. J. Morphol. Embryol. 2008, 49, 485–489. [Google Scholar] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Norm [34] | T0 | T1 |
|---|---|---|---|
| SNA | 82° ± 3.5 | * 88.8° | * 88.5° |
| SNB | 79° ± 3.0 | * 84.1° | * 83.9° |
| ANB | 3.0° ± 2.0 | 4.7° | 4.6° |
| MMPA | 26° ± 5 | 24.7° | 24.6° |
| Face height ratio | 55% ± 1.5 | * 52.9% | * 52.8% |
| SN to maxillary plane | 8° ± 3 | * 12.1° | * 11.9° |
| Upper incisor to maxillary plane | 118° ± 6 | ** 133.4° | * 129.1° |
| Lower incisor to mandibular plane | 97° ± 7 | * 105.7° | 100.7° |
| Interincisal angle | 115° ± 8 | ** 96.3° | * 105.6° |
| Wits appraisal | −4.5 mm ± 3.0 | * −0.4 mm | - |
| Lower incisor to APo line | 5.5 mm ± 2.5 | ** 11.4 mm | ** 9.5 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sum, F.H.K.M.H.; Shan, Z.; Chan, Y.H.D.; Chu, R.J.D.H.; Pelekos, G.; She, T.T. Biomechanical Considerations in the Orthodontic Treatment of a Patient with Stabilised Stage IV Grade C Generalised Periodontitis: A Case Report. Bioengineering 2024, 11, 403. https://doi.org/10.3390/bioengineering11040403
Sum FHKMH, Shan Z, Chan YHD, Chu RJDH, Pelekos G, She TT. Biomechanical Considerations in the Orthodontic Treatment of a Patient with Stabilised Stage IV Grade C Generalised Periodontitis: A Case Report. Bioengineering. 2024; 11(4):403. https://doi.org/10.3390/bioengineering11040403
Chicago/Turabian StyleSum, Fung Hou Kumoi Mineaki Howard, Zhiyi Shan, Yat Him Dave Chan, Ryan Julian Dick Hei Chu, George Pelekos, and Tsang Tsang She. 2024. "Biomechanical Considerations in the Orthodontic Treatment of a Patient with Stabilised Stage IV Grade C Generalised Periodontitis: A Case Report" Bioengineering 11, no. 4: 403. https://doi.org/10.3390/bioengineering11040403
APA StyleSum, F. H. K. M. H., Shan, Z., Chan, Y. H. D., Chu, R. J. D. H., Pelekos, G., & She, T. T. (2024). Biomechanical Considerations in the Orthodontic Treatment of a Patient with Stabilised Stage IV Grade C Generalised Periodontitis: A Case Report. Bioengineering, 11(4), 403. https://doi.org/10.3390/bioengineering11040403