Biomechanical Force Prediction for Lengthening of Small Intestine during Distraction Enterogenesis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
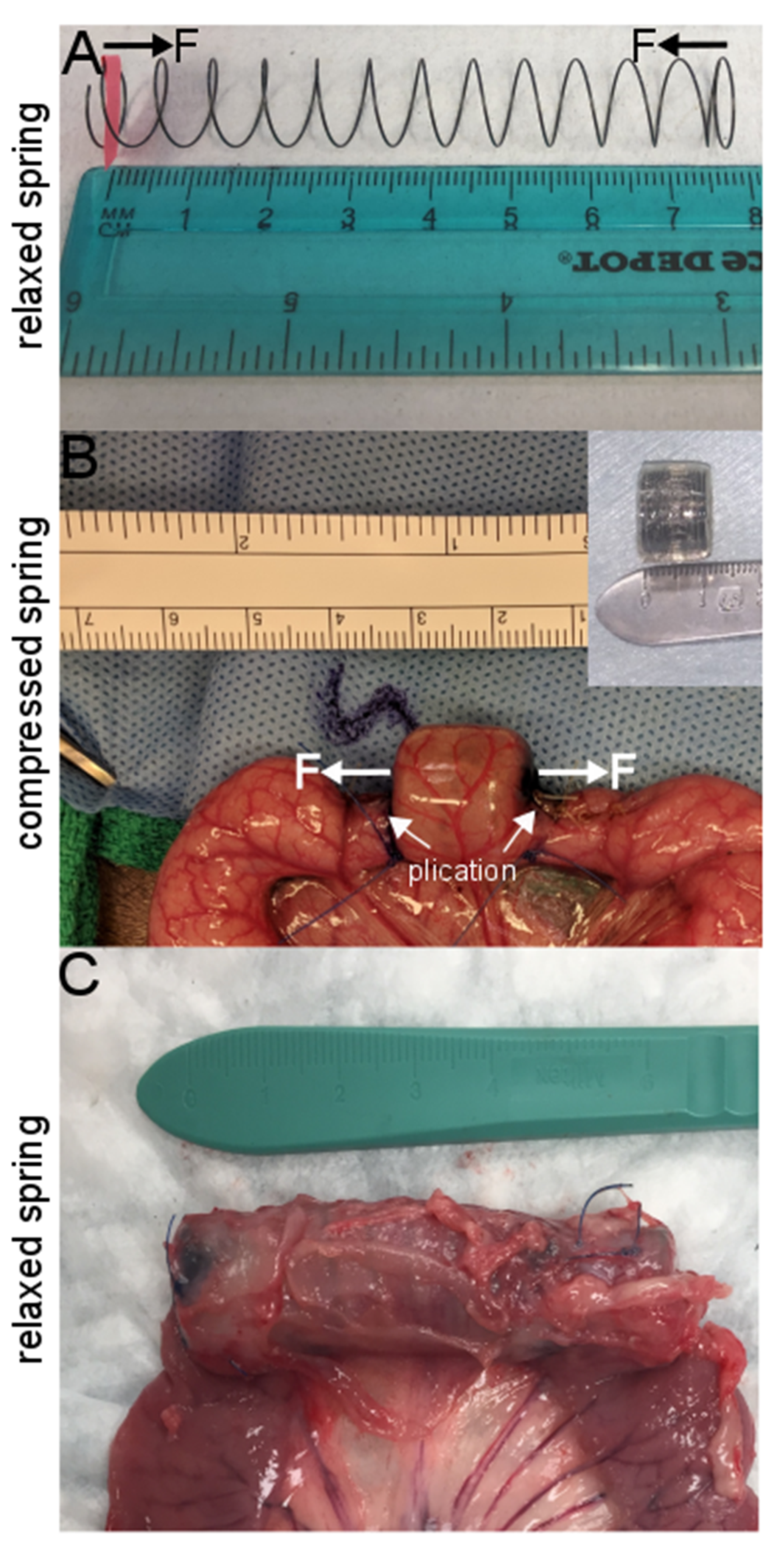
2.1. Spring Production and Encapsulation
2.2. Animal and Human Sample Preparation and Surgical Procedure
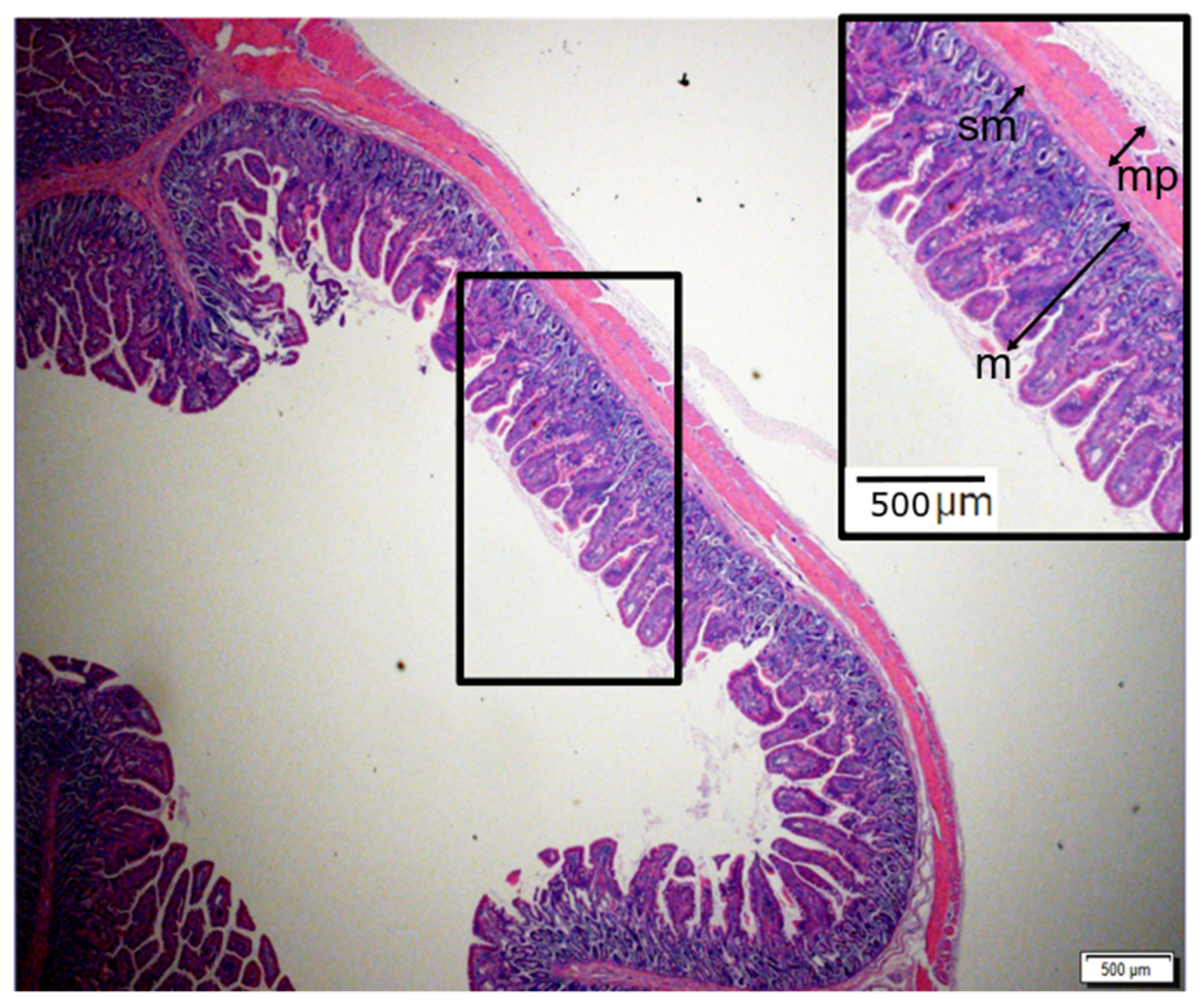
2.3. Geometrical and Histologic Evaluation
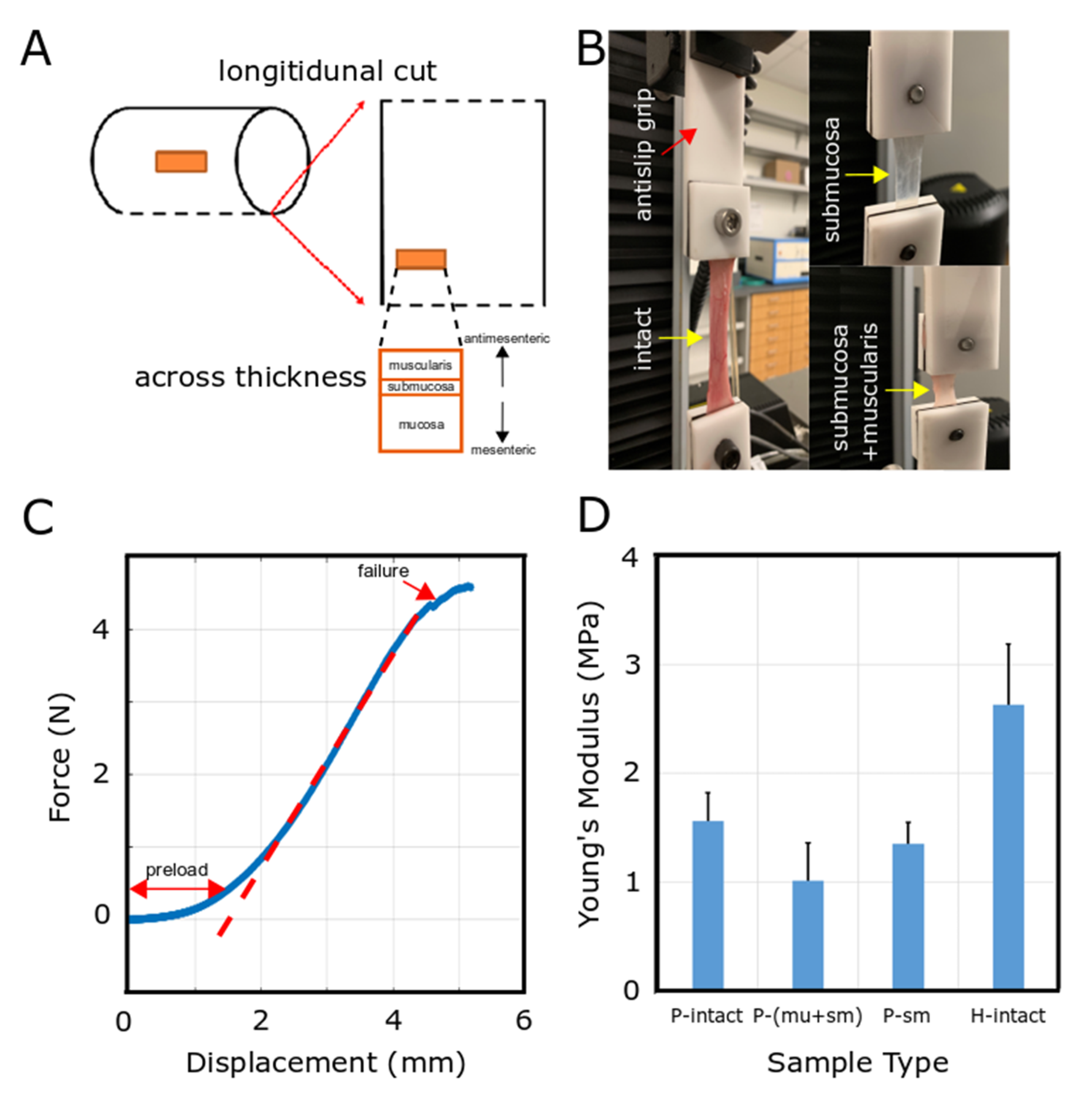
2.4. Mechanical Characterization
2.5. Computational Methods
2.5.1. Overview of Models
2.5.2. Theory
3. Results
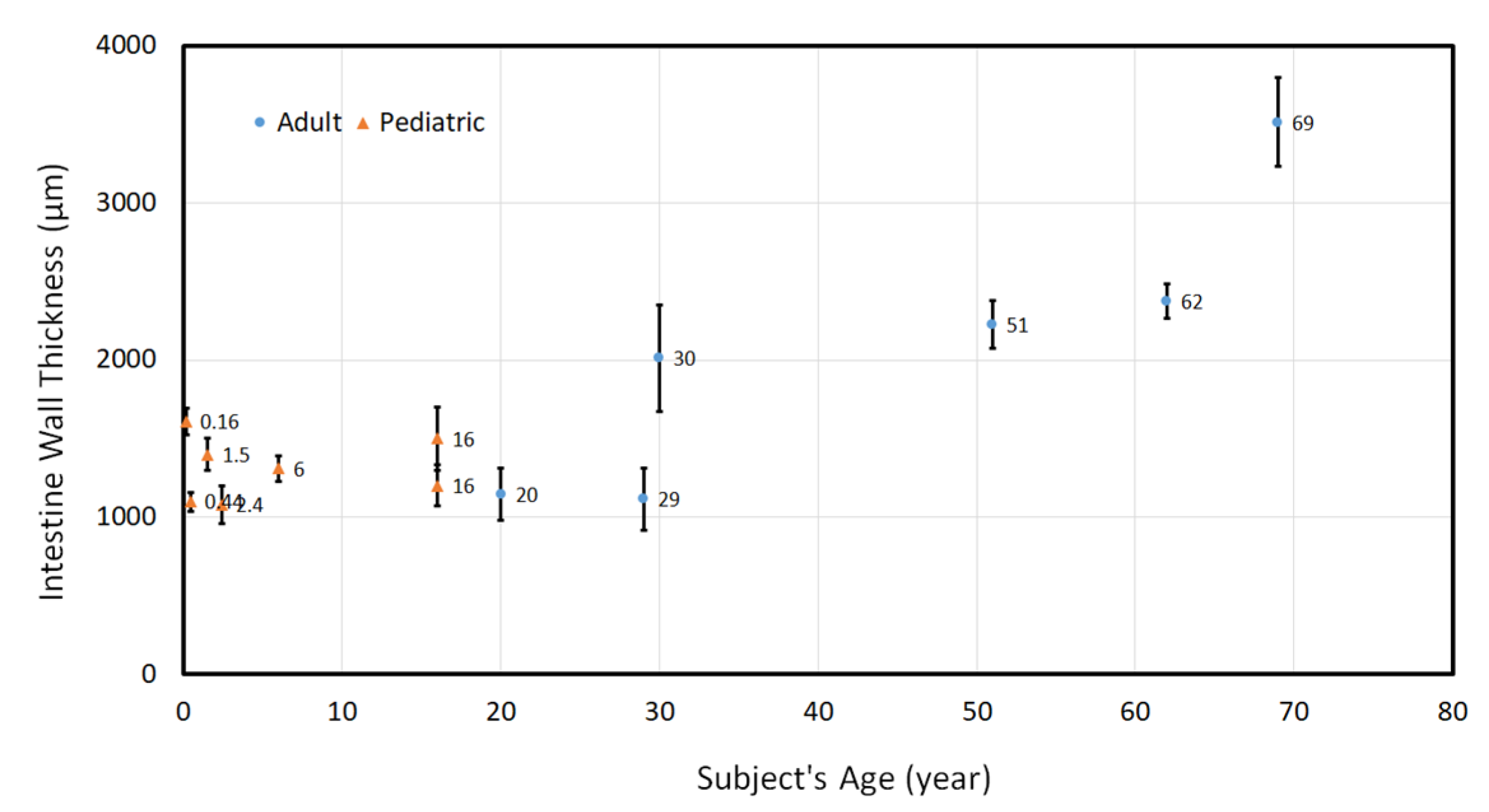
3.1. Geometrical Characteristics of Human Small Intestinal Tract
3.2. Mechanical Characterization of Small Intestinal Tissue
3.3. 3D Computational Model for Distraction Enterogenesis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Dual Publication Statement
References
- Pironi, L. Definitions of intestinal failure and the short bowel syndrome. Best Pract. Res. Clin. Gastroenterol. 2016, 30, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Reinshagen, K.; Adams, R.; Trunk, M.; Wessel, L.M. The chronic liver disease in patients with short bowel syndrome: Etiology and treatment. Minerva Pediatrica 2009, 61, 273–281. [Google Scholar] [PubMed]
- Duggan, C.P.; Jaksic, T. Pediatric Intestinal Failure. N. Engl. J. Med. 2017, 377, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Oke, S.; Walter, M.N.; Ansari, T.; Gabe, S.M. Growth factors and their use in short bowel. Curr. Opin. Gastroenterol. 2017, 33, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A. Intestinal loop lengthening—A technique for increasing small intestinal length. J. Pediatric Surg. 1980, 15, 145–151. [Google Scholar] [CrossRef]
- Chang, R.W.; Javid, P.J.; Oh, J.T.; Andreoli, S.; Kim, H.B.; Fauza, D.; Jaksic, T. Serial Transverse Enteroplasty Enhances Intestinal Function in a Model of Short Bowel Syndrome. Ann. Surg. 2006, 243, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Kosar, C.; Steinberg, K.; de Silva, N.; Avitzur, Y.; Wales, P.W. Cost of ambulatory care for the pediatric intestinal failure patient: One-year follow-up after primary discharge. J. Pediatric Surg. 2016, 51, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Lao, O.B.; Healey, P.J.; Perkins, J.D.; Horslen, S.; Reyes, J.D.; Goldin, A.B. Outcomes in Children after Intestinal Transplant. Pediatrics 2010, 125, e550–e558. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.M.; Skeans, M.A.; Horslen, S.P.; Edwards, E.B.; Harper, A.M.; Snyder, J.J.; Israni, A.K.; Kasiske, B.L. OPTN/SRTR 2015 Annual Data Report: Intestine. Am. J. Transplant. 2017, 17, 252–285. [Google Scholar] [CrossRef] [Green Version]
- Demehri, F.R.; Utter, B.; Freeman, J.J.; Fukatsu, Y.; Luntz, J.; Brei, D.; Teitelbaum, D.H. Development of an endoluminal intestinal attachment for a clinically applicable distraction enterogenesis device. J. Pediatric Surg. 2016, 51, 101–106. [Google Scholar] [CrossRef] [Green Version]
- Demehri, F.R.; Wong, P.M.; Freeman, J.J.; Fukatsu, Y.; Teitelbaum, D.H. A novel double-balloon catheter device for fully endoluminal intestinal lengthening. Pediatric Surg. Int. 2014, 30, 1223–1229. [Google Scholar] [CrossRef]
- Dionigi, B.; Brazzo, J., III; Connors, J.P.; Ahmed, A.; Fisher, J.G.; Zurakowski, D.; Fauza, D.O. Extraluminal helicoidal stretch (Helixtretch): A novel method of intestinal lengthening. J. Pediatric Surg. 2014, 49, 1787–1790. [Google Scholar] [CrossRef] [PubMed]
- Dubrovsky, G.; Huynh, N.; Thomas, A.L.; Shekherdimian, S.; Dunn, J.C. Intestinal lengthening via multiple in-continuity springs. J. Pediatric Surg. 2019, 54, 39–43. [Google Scholar] [CrossRef]
- Dubrovsky, G.; Huynh, N.; Thomas, A.L.; Shekherdimian, S.; Dunn, J.C. Double plication for spring-mediated intestinal lengthening of a defunctionalized Roux limb. J. Pediatric Surg. 2018, 53, 1806–1810. [Google Scholar] [CrossRef]
- Fisher, J.G.; Sparks, E.A.; Khan, F.A.; Dionigi, B.; Wu, H.; Brazzo, J., III; Fauza, D.; Modi, B.; Safranskid, D.L.; Jaksic, T. Extraluminal distraction enterogenesis using shape-memory polymer. J. Pediatric Surg. 2015, 50, 938–942. [Google Scholar] [CrossRef]
- Huynh, N.; Dubrovsky, G.; Rouch, J.D.; Scott, A.; Stelzner, M.; Shekherdimian, S.; Dunn, J.C. Feasibility and scalability of spring parameters in distraction enterogenesis in a murine model. J. Surg. Res. 2017, 215, 219–224. [Google Scholar] [CrossRef]
- Huynh, N.; Rouch, J.D.; Scott, A.; Chiang, E.; Wu, B.M.; Shekherdimian, S.; Dunn, J.C. Spring-mediated distraction enterogenesis in-continuity. J. Pediatric Surg. 2016, 51, 1983–1987. [Google Scholar] [CrossRef]
- Koga, H.; Sun, X.; Yang, H.; Nose, K.; Somara, S.; Bitar, K.N.; Owyang, C.; Okawada, M.; Teitelbaum, D.H. Distraction-Induced Intestinal Enterogenesis: Preservation of Intestinal Function and Lengthening After Reimplantation into Normal Jejunum. Ann. Surg. 2012, 255, 302–310. [Google Scholar] [CrossRef] [Green Version]
- Okawada, M.; Maria, H.M.; Teitelbaum, D.H. Distraction Induced Enterogenesis: A Unique Mouse Model Using Polyethylene Glycol1. J. Surg. Res. 2011, 170, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Sueyoshi, R.; Ralls, M.W.; Teitelbaum, D.H. Glucagon-like peptide 2 increases efficacy of distraction enterogenesis. J. Surg. Res. 2013, 184, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Sueyoshi, R.; Ignatoski, K.M.W.; Okawada, M.; Teitelbaum, D.H. Distraction-induced intestinal growth: The role of mechanotransduction mechanisms in a mouse model of short bowel syndrome. Tissue Eng. Part A 2014, 20, 830–841. [Google Scholar] [CrossRef] [Green Version]
- Demehri, F.R.; Freeman, J.J.; Fukatsu, Y.; Luntz, J.; Teitelbaum, D.H. Development of an endoluminal intestinal lengthening device using a geometric intestinal attachment approach. Surgery 2015, 158, 802–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, H.S.; Taylor, J.S.; Wood, L.S.; Dunn, J.C. Biomechanics of small intestine during distraction enterogenesis with an intraluminal spring. J. Mech. Behav. Biomed. Mater. 2020, 101, 103413. [Google Scholar] [CrossRef]
- Hosseini, H.S.; Wood, L.S.; Taylor, J.S.; Dubrovsky, G.; Portelli, K.I.; Thomas, A.L.; Dunn, J.C. Biomechanical signaling and collagen fiber reorientation during distraction enterogenesis. J. Mech. Behav. Biomed. Mater. 2020, 101, 103425. [Google Scholar] [CrossRef]
- Dubrovsky, G.; Huynh, N.; Thomas, A.L.; Shekherdimian, S.; Dunn, J.C. Double plication for spring-mediated in-continuity intestinal lengthening in a porcine model. Surgery 2019, 165, 389–392. [Google Scholar] [CrossRef]
- Scott, A.; Rouch, J.D.; Huynh, N.; Chiang, E.; Shekherdimian, S.; Lee, S.L.; Wu, B.M.; Dunn, J.C. Mechanical lengthening in multiple intestinal segments in-series. J. Pediatric Surg. 2016, 51, 957–959. [Google Scholar] [CrossRef]
- Azar, D.; Ohadi, D.; Rachev, A.; Eberth, J.F.; Uline, M.J.; Shazly, T. Mechanical and geometrical determinants of wall stress in abdominal aortic aneurysms: A computational study. PLoS ONE 2018, 13, e0192032. [Google Scholar] [CrossRef] [Green Version]
- Eskandari, M.; Javili, A.; Kuhl, E. Elastosis during airway wall remodeling explains multiple co-existing instability patterns. J. Theor. Biol. 2016, 403, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Eskandari, M.; Kuschner, W.G.; Kuhl, E. Patient-Specific Airway Wall Remodeling in Chronic Lung Disease. Ann. Biomed. Eng. 2015, 43, 2538–2551. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, H.S.; Beebe, D.C.; Taber, L.A. Mechanical effects of the surface ectoderm on optic vesicle morphogenesis in the chick embryo. J. Biomech. 2014, 47, 3837–3846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, H.S.; Garcia, K.E.; Taber, L.A. A new hypothesis for foregut and heart tube formation based on differential growth and actomyosin contraction. Development 2017, 144, 2381–2391. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, H.S.; Taber, L.A. How mechanical forces shape the developing eye. Prog. Biophys. Mol. Biol. 2018, 137, 25–36. [Google Scholar] [CrossRef]
- Hosseini, S.; Taber, L. Mechanics of Optic Vesicle Morphogenesis in the Chick Embryo. Biophys. J. 2015, 108, 629a. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, S.; Taber, L.A. Physical and Mechanical Forces that Shape Heart Tube in the Chick Embryo. Biophys. J. 2017, 112, 304a–305a. [Google Scholar] [CrossRef] [Green Version]
- Shahidian, A.; Ghorbanniahassankiadeh, A. Stress analysis of internal carotid artery with low stenosis level: The effect of material model and plaque geometry. J. Mech. Med. Biol. 2017, 17, 1750098. [Google Scholar] [CrossRef]
- Sharzehee, M.; Khalafvand, S.S.; Han, H.-C. Fluid-structure interaction modeling of aneurysmal arteries under steady-state and pulsatile blood flow: A stability analysis. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, E.K.; Hoger, A.; McCulloch, A.D. Stress-dependent finite growth in soft elastic tissues. J. Biomech. 1994, 27, 455–467. [Google Scholar] [CrossRef]
- Fung, Y.-C. Biomechanics: Mechanical Properties of Living Tissues; Springer Science & Business Media: Berlin, Germany, 2013. [Google Scholar]
- Taber, L.A. Nonlinear Theory of Elasticity: Applications in Biomechanics; World Scientific: Singapore City, Singapore, 2004. [Google Scholar]
- Bellini, C.; Glass, P.; Sitti, M.; Di Martino, E.S. Biaxial mechanical modeling of the small intestine. J. Mech. Behav. Biomed. Mater. 2011, 4, 1727–1740. [Google Scholar] [CrossRef]
- Carniel, E.L.; Gramigna, V.; Fontanella, C.G.; Frigo, A.; Stefanini, C.; Rubini, A.; Natali, A.N. Characterization of the anisotropic mechanical behaviour of colonic tissues: Experimental activity and constitutive formulation. Exp. Physiol. 2014, 99, 759–771. [Google Scholar] [CrossRef]
- Stavropoulou, E.A.; Dafalias, Y.F.; Sokolis, D.P. Biomechanical and histological characteristics of passive esophagus: Experimental investigation and comparative constitutive modeling. J. Biomech. 2009, 42, 2654–2663. [Google Scholar] [CrossRef]
- Liao, D.; Zhao, J.; Gregersen, H. 3d Mechanical properties of the partially obstructed guinea pig small intestine. J. Biomech. 2010, 43, 2079–2086. [Google Scholar] [CrossRef] [PubMed]
- Sokolis, D.P. Experimental study and biomechanical characterization for the passive small intestine: Identification of regional differences. J. Mech. Behav. Biomed. Mater. 2017, 74, 93–105. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini, H.S.; Dunn, J.C.Y. Biomechanical Force Prediction for Lengthening of Small Intestine during Distraction Enterogenesis. Bioengineering 2020, 7, 140. https://doi.org/10.3390/bioengineering7040140
Hosseini HS, Dunn JCY. Biomechanical Force Prediction for Lengthening of Small Intestine during Distraction Enterogenesis. Bioengineering. 2020; 7(4):140. https://doi.org/10.3390/bioengineering7040140
Chicago/Turabian StyleHosseini, Hadi S., and James C. Y. Dunn. 2020. "Biomechanical Force Prediction for Lengthening of Small Intestine during Distraction Enterogenesis" Bioengineering 7, no. 4: 140. https://doi.org/10.3390/bioengineering7040140
APA StyleHosseini, H. S., & Dunn, J. C. Y. (2020). Biomechanical Force Prediction for Lengthening of Small Intestine during Distraction Enterogenesis. Bioengineering, 7(4), 140. https://doi.org/10.3390/bioengineering7040140