

Evaluating the Haemodynamic Performance of Endografts for Complex Aortic Arch Repair


Abstract
:1. Introduction
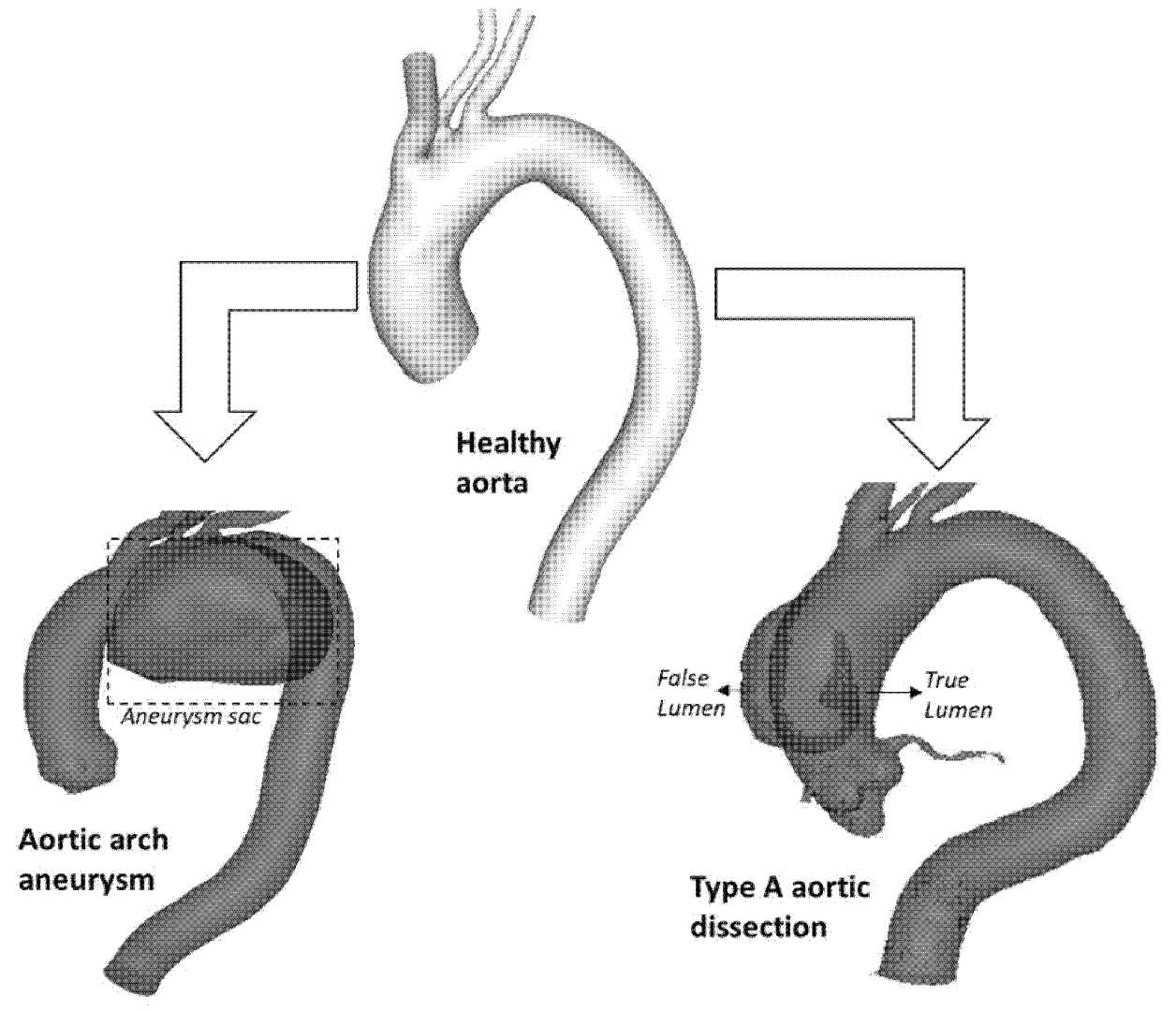
1.1. Aortic Arch Disease
1.2. Thoracic Endovascular Aortic Repair
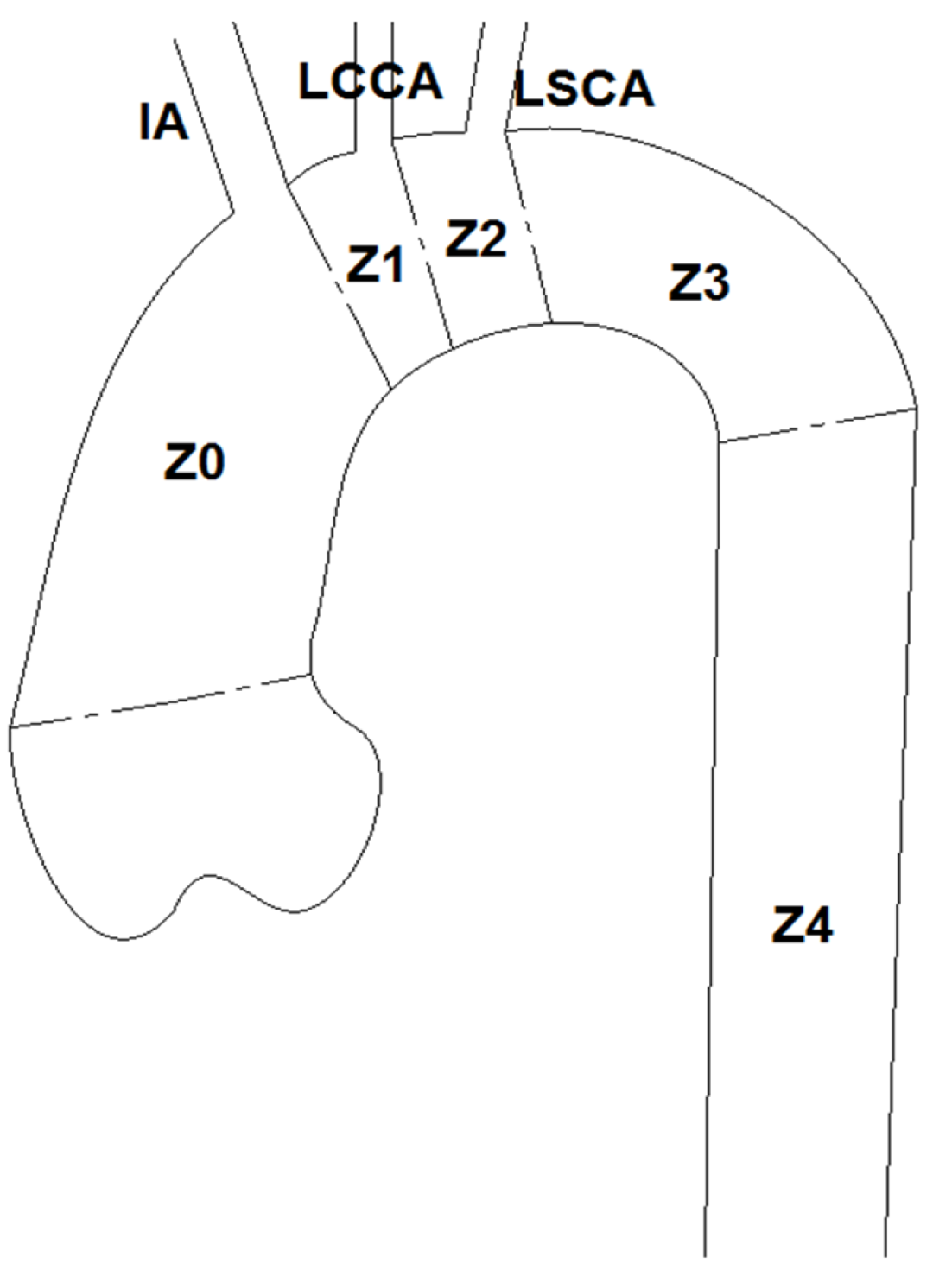
1.2.1. Challenges for TEVAR
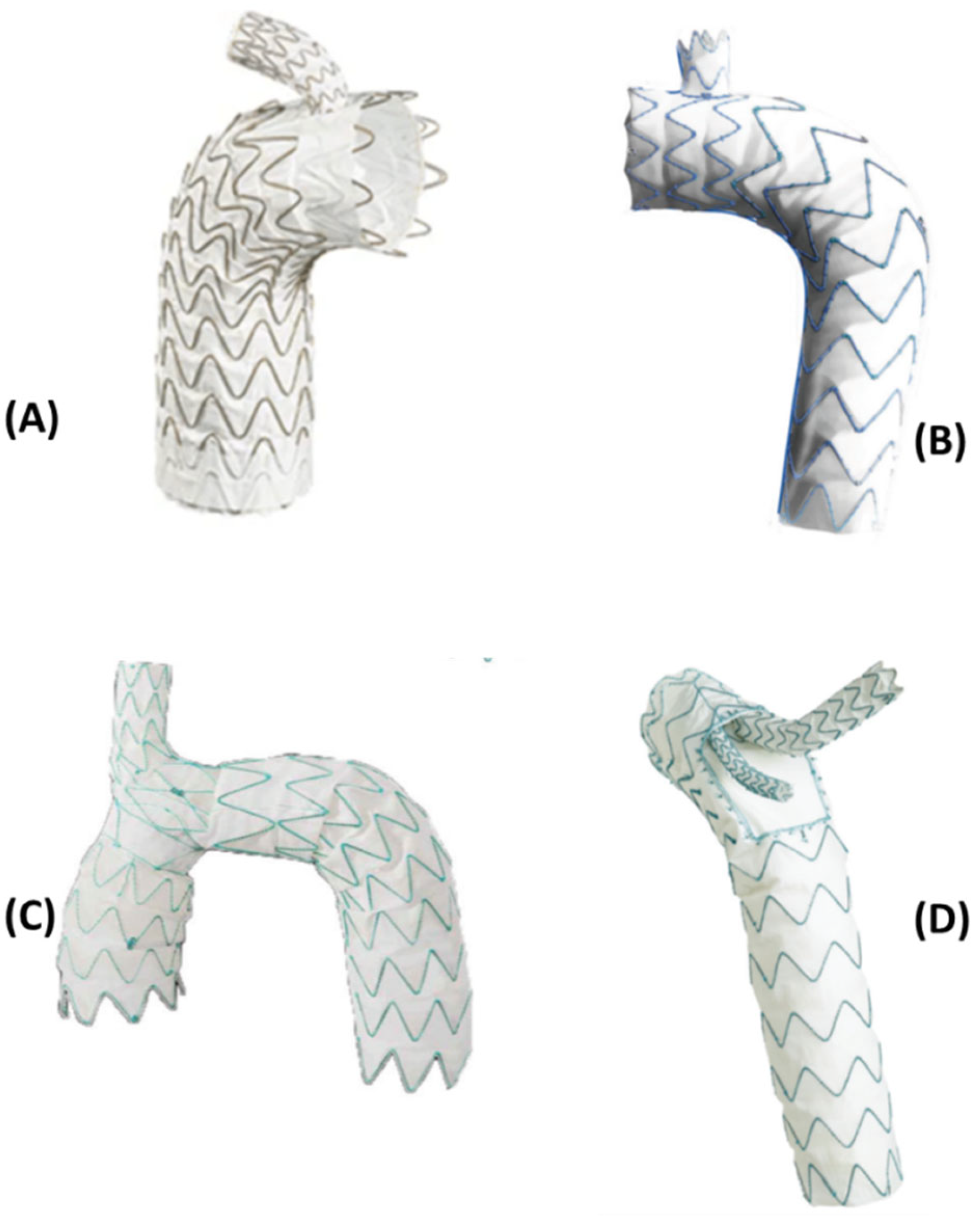
1.2.2. Endografts

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Manufacturer | Stent/Graft Material | No. of Branches | Landing Zone | Description |
|---|---|---|---|---|---|
| Inoue Stent Graft [37] | PTMC institute | Nickel titanium/Dacron | 1–3 | 0–2 | The ISG consists of a main body with up to three branches attached separately based on axial location of target vessels. The landing zone is dictated by the number of emerging branches and vice versa in order for cuffed rings to be able to secure the graft in place both proximally and distally. |
| RelayPlus [2,30,38] | Terumo Aortic | Nitinol/Polyester | 2 | 0 | The RelayPlus double-branched device is formed of three main components: the main graft body and the two branches extending out via a covered window in the superior aspect of the main body (incorporating the Relay®®Branch system). Tunnel branches originating in the proximal end and running along the device wall connects to the emerging branches which lead into the IA and LCCA. |
| Zenith Arch Branched Graft [30,39] | Cook medical | Nitinol/Polyester | 2 | 0 | The Zenith arch branched graft, as the name suggests is a branched endograft that can be used for Z0 endovascular repair. It consists of two inner branches that serve to preserve blood flow to the supra-aortic vessels. It is custom-made specifically for arch repair, with reportedly acceptable morbidity and mortality rates. |
| NexusTM Stent-Graft [30,34,39] | Endospan | Nitinol/PTFE | 1 | 0 | The NEXUSTM Aortic Arch Stent Graft System is a single-branched endograft allowing for Z0 fixation in the proximal aortic arch. It consists of a main module for the aortic arch and descending aorta with a side-branch for one supra-aortic vessel and a curved module for the ascending aorta that connects to the main module through a self-protecting sleeve and lands into the sinotubular junction. |
| Gore TAG/TBE [2,30] | W L Gore & Associates | Nitinol/PTFE | 1 | 2 | The Gore TAG device is a single-branched endograft designed primarily for Z2 deployment. It then served as inspiration for the Gore TBE (Thoracic Branch Endoprosthesis), aimed at treating distal aortic arch aneurysms. It consists of a main graft with a side-branch component. The side-branch is tapered with a retrograde orientation extending into the main graft body. |
| Valiant Mona LSA [30,34] | Medtronic | Nitinol/Polyester | 1 | 2 | The Valiant Mona LSA is a single-branched aortic endograft primarily for Z2 deployment. The functional sizing of the graft avoids the need for fenestrations as well as not covering the LSCA. The device consists of two components: a main stent graft (MSG) and a branch stent graft (BSG). This allows maintenance of LSCA perfusion and are arranged such that it has minimal thickness, thereby providing maximum lumen area. |
| Castor Aortic Branched Stent-Graft [2,30,34] | MicroPort Medical Co., Ltd. | Nitinol/Polyester | 1 | 2 | The Castor Aortic Branched Stent-Graft is a unibody endograft which an emerging branch that allows for LSCA vascularisation. It allows for Type B Aortic Dissection treatment with a Z2 by excluding the proximal entry tear whilst perfusing the LSCA. |

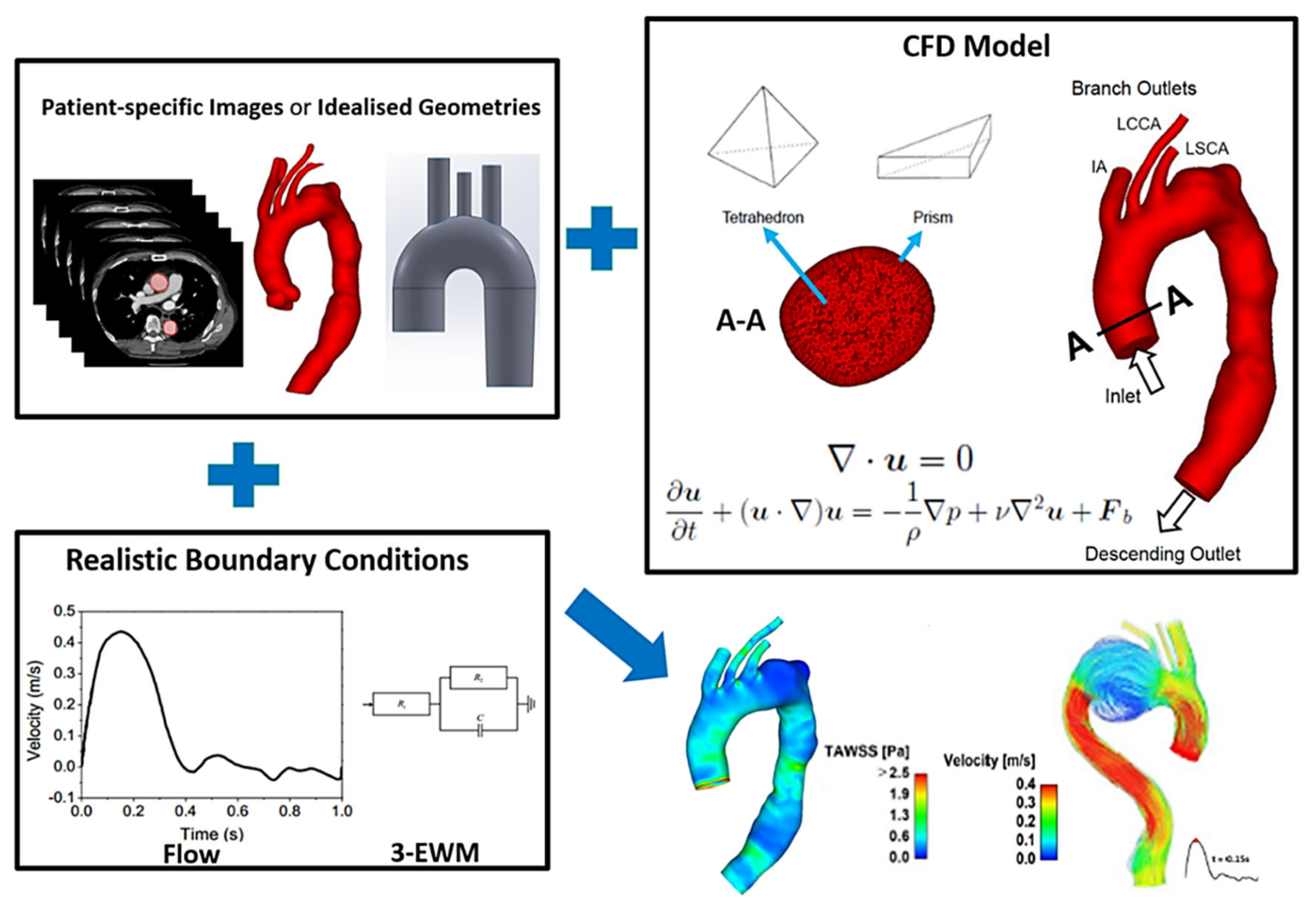
2. Modelling Methodology
2.1. Image Acquisition and Geometry Reconstruction
2.2. Computational Methods
2.3. Haemodynamic Metrics
3. CFD Analysis of Aortic Arch Repair
3.1. Idealised Models
3.2. Patient-Specific Modelling
3.3. Future Directions
3.3.1. Virtual Stent-Graft Deployment
3.3.2. Prediction of Stent-Graft Induced Thrombosis
3.3.3. Application to a Large Cohort
3.4. Clinical Relevance
4. Summary
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Desai, N.D.; Roselli, E.E. Complex aortic arch surgery. Ann. Cardiothorac. Surg. 2018, 7, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherrie, Z.A.; Victor, M.R. Upcoming Technology for Aortic Arch Aneurysms. Endovasc. Today. 2015, pp. 46–52. Available online: https://evtoday.com/2015/11/upcoming-technology-for-aortic-arch-aneurysms/ (accessed on 10 August 2021).
- Stankovic, Z.; Allen, B.D.; Garcia, J.; Jarvis, K.B.; Markl, M. 4D flow imaging with MRI. Cardiovasc. Diagn. Ther. 2014, 4, 173–192. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Sekine, T.; Ando, T.; Ishii, Y.; Kumita, S. Utility of 4D flow MRI in thoracic aortic diseases: A Literature Review of Clinical Applications and Current Evidence. Magn. Reson. Med. Sci. 2021, 21, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Juli, C.; Wood, N.B.; Gibbs, R.G.J.; Xu, X.Y. Predicting flow in aortic dissection: Comparison of computational model with PC-MRI velocity measurements. Med. Eng. Phys. 2014, 36, 1176–1184. [Google Scholar] [CrossRef]
- Armour, C.H.; Guo, B.; Saitta, S.; Pirola, S.; Liu, Y.; Dong, Z.; Xu, X.Y. Evaluation and verification of patient-specific modelling of type B aortic dissection. Comput. Biol. Med. 2022, 140, 105053. [Google Scholar] [CrossRef]
- Pirola, S.; Guo, B.; Menichini, C.; Saitta, S.; Fu, W.; Dong, Z.; Xu, X.Y. 4-D flow MRI-based computational analysis of blood flow in patient-specific aortic dissection. IEEE Trans. Biomed. Eng. 2019, 66, 3411–3419. [Google Scholar] [CrossRef] [Green Version]
- Guyton, A.C.; Hall, J.E. Textbook of Medical Physiology; Saunders: Philadelphia, PA, USA, 1986; Volume 548. [Google Scholar]
- Booher, A.M.; Eagle, K.A. Diagnosis and management issues in thoracic aortic aneurysm. Am. Heart J. 2011, 162, 38–46.e1. [Google Scholar] [CrossRef]
- Clouse, W.D.; Hallett, J.W.; Schaff, H.V.; Spittell, P.C.; Rowland, C.M.; Ilstrup, D.M.; Melton, L.J. Acute Aortic Dissection: Population-Based Incidence Compared With Degenerative Aortic Aneurysm Rupture. Mayo Clin. Proc. 2004, 79, 176–180. [Google Scholar] [CrossRef]
- Hebballi, R.; Swanevelder, J. Diagnosis and management of aortic dissection. Contin. Educ. Anaesth. Crit. Care Pain 2009, 9, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Shirakawa, Y.; Kuratani, T.; Shimamura, K.; Torikai, K.; Sakamoto, T.; Shijo, T.; Sawa, Y. The efficacy and short-term results of hybrid thoracic endovascular repair into the ascending aorta for aortic arch pathologies. Eur. J. Cardio-Thorac. Surg. 2014, 45, 298–304. [Google Scholar] [CrossRef]
- Nienaber, C.A.; Fattori, R.; Lund, G.; Dieckmann, C.; Wolf, W.; von Kodolitsch, Y.; Nicolas, V.; Pierangeli, A. Nonsurgical Reconstruction of Thoracic Aortic Dissection by Stent–Graft Placement. N. Engl. J. Med. 1999, 340, 1539–1545. [Google Scholar] [CrossRef]
- Bodell, B.D.; Taylor, A.C.; Patel, P.J. Thoracic Endovascular Aortic Repair: Review of Current Devices and Treatments Options. Tech. Vasc. Interv. Radiol. 2018, 21, 137–145. [Google Scholar] [CrossRef]
- Nardi, A.; Avrahami, I. Approaches for treatment of aortic arch aneurysm, a numerical study. J. Biomech. 2017, 50, 158–165. [Google Scholar] [CrossRef]
- Makaroun, M.S.; Dillavou, E.D.; Wheatley, G.H.; Cambria, R.P. Five-year results of endovascular treatment with the Gore TAG device compared with open repair of thoracic aortic aneurysms. J. Vasc. Surg. 2008, 47, 912–918. [Google Scholar] [CrossRef] [Green Version]
- Martin, G.; Riga, C.; Gibbs, R.; Jenkins, M.; Hamady, M.; Bicknell, C. Short- and Long-term Results of Hybrid Arch and Proximal Descending Thoracic Aortic Repair: A Benchmark for New Technologies. J. Endovasc. Ther. 2016, 23, 783–790. [Google Scholar] [CrossRef]
- Naughton, P.A.; Park, M.S.; Morasch, M.D.; Rodriguez, H.E.; Garcia-Toca, M.; Wang, C.E.; Eskandari, M.K. Emergent Repair of Acute Thoracic Aortic Catastrophes: A Comparative Analysis. Arch Surg. 2012, 147, 243–249. [Google Scholar] [CrossRef]
- Ishimaru, S. Endografting of the Aortic Arch. J. Endovasc. Ther. 2004, 11, II-62–II-71. [Google Scholar] [CrossRef]
- Waterford, S.D.; Chou, D.; Bombien, R.; Uzun, I.; Shah, A.; Khoynezhad, A. Left Subclavian Arterial Coverage and Stroke During Thoracic Aortic Endografting: A Systematic Review. Ann. Thorac. Surg. 2016, 101, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Zamor, K.C.; Eskandari, M.K.; Rodriguez, H.E.; Ho, K.J.; Morasch, M.D.; Hoel, A.W. Outcomes of Thoracic Endovascular Aortic Repair and Subclavian Revascularization Techniques. J. Am. Coll. Surg. 2015, 221, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Criado, F.J.; Clark, N.S.; Barnatan, M.F. Stent graft repair in the aortic arch and descending thoracic aorta: A 4-year experience. J. Vasc. Surg. 2002, 36, 1121–1128. [Google Scholar] [CrossRef]
- Ueda, T.; Fleischmann, D.; Dake, M.D.; Rubin, G.D.; Sze, D.Y. Incomplete endograft apposition to the aortic arch: Bird-beak configuration increases risk of endoleak formation after thoracic endovascular aortic repair. Radiology 2010, 255, 645–652. [Google Scholar] [CrossRef]
- Balm, R.; Reekers, J.A.; Jacobs, M.J. Classification of endovascular procedures for treating thoracic aortic aneurysms. In Surgical and Endovascular Treatment of Aortic Aneurysms; Futura Publishing Company: New York, NY, USA, 2000; pp. 19–26. [Google Scholar]
- Antoniou, G.A.; Sakka, K.M.E.; Hamady, M.; Wolfe, J.H.N. Hybrid Treatment of Complex Aortic Arch Disease with Supra-aortic Debranching and Endovascular Stent Graft Repair. Eur. J. Vasc. Endovasc. Surg. 2010, 39, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Zerwes, S.; Leissner, G.; Gosslau, Y.; Jakob, R.; Bruijnen, H.-K.; Oertl, F.; Woelfle, K. Clinical outcomes in hybrid repair procedures for pathologies involving the aortic arch. Vascular 2015, 23, 9–16. [Google Scholar] [CrossRef]
- Iba, Y.; Minatoya, K.; Matsuda, H.; Sasaki, H.; Tanaka, H.; Oda, T.; Kobayashi, J. How should aortic arch aneurysms be treated in the endovascular aortic repair era? A risk-adjusted comparison between open and hybrid arch repair using propensity score-matching analysis. Eur. J. Cardio-Thorac. Surg. 2014, 46, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Benedetto, U.; Melina, G.; Angeloni, E.; Codispoti, M.; Sinatra, R. Current results of open total arch replacement versus hybrid thoracic endovascular aortic repair for aortic arch aneurysm: A meta-analysis of comparative studies. J. Thorac. Cardiovasc. Surg. 2013, 145, 305–306. [Google Scholar] [CrossRef] [Green Version]
- Tokuda, Y.; Oshima, H.; Narita, Y.; Abe, T.; Araki, Y.; Mutsuga, M.; Fujimoto, K.; Terazawa, S.; Yagami, K.; Ito, H.; et al. Hybrid versus open repair of aortic arch aneurysms: Comparison of postoperative and mid-term outcomes with a propensity score-matching analysis. Eur. J. Cardio-Thorac. Surg. 2016, 49, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Heaton, D.H. The Next Generation of Aortic Endografts. Endovasc. Today. 2009, pp. 49–52. Available online: https://evtoday.com/2009/01/EVT0109_03.php (accessed on 21 August 2021).
- Haulon, S.; Greenberg, R.K.; Spear, R.; Eagleton, M.; Abraham, C.; Lioupis, C.; Verhoeven, E.; Ivancev, K.; Kolbel, T.; Stanley, B.; et al. Global experience with an inner branched arch endograft. J. Thorac. Cardiovasc. Surg. 2014, 148, 1709–1716. [Google Scholar] [CrossRef] [Green Version]
- Spear, R.; Haulon, S.; Ohki, T.; Tsilimparis, N.; Kanaoka, Y.; Milne, C.P.E.; Debus, S.; Takizawa, R.; Kölbel, T. Editor’s Choice—Subsequent Results for Arch Aneurysm Repair with Inner Branched Endografts. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Czerny, M.; Rylski, B.; Morlock, J.; Schröfel, H.; Beyersdorf, F.; Saint Lebes, B.; Meyrignac, O.; Mokrane, F.; Lescan, M.; Schlensak, C.; et al. Orthotopic branched endovascular aortic arch repair in patients who cannot undergo classical surgery. Eur. J. Cardio Thorac. Surg. 2018, 53, 1007–1012. [Google Scholar] [CrossRef] [Green Version]
- van Bakel, T.M.; de Beaufort, H.W.; Trimarchi, S.; Marrocco-Trischitta, M.M.; Bismuth, J.; Moll, F.L.; Patel, H.J.; van Herwaarden, J.A. Status of branched endovascular aortic arch repair. Ann. Cardiothorac. Surg. 2018, 7, 406–413. [Google Scholar] [CrossRef]
- Ferrer, C.; Cao, P. Endovascular arch replacement with a dual branched endoprosthesis. Ann. Cardiothorac. Surg. 2018, 7, 366–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, C.; Xiong, F.; Kabinejadian, F.; Praveen Kumar, G.; Cui, F.; Chen, G.; Ho, P.; Leo, H. Hemodynamic analysis of a novel stent graft design with slit perforations in thoracic aortic aneurysm. J. Biomech. 2019, 85, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Tazaki, J.; Inoue, K.; Higami, H.; Higashitani, N.; Toma, M.; Saito, N.; Kawatou, M.; Kimura, T. Thoracic endovascular aortic repair with branched Inoue Stent Graft for arch aortic aneurysms. J. Vasc. Surg. 2017, 66, 1340–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czerny, M.; Berger, T.; Kondov, S.; Siepe, M.; Saint Lebes, B.; Mokrane, F.; Rousseau, H.; Lescan, M.; Schlensak, C.; Andic, M.; et al. Results of endovascular aortic arch repair using the Relay Branch system. Eur. J. Cardio Thorac. Surg. 2021, 60, 662–668. [Google Scholar] [CrossRef]
- van Bakel, T.M.; Arthurs, C.J.; van Herwaarden, J.A.; Moll, F.L.; Eagle, K.A.; Patel, H.J.; Trimarchi, S.; Figueroa, C.A. A computational analysis of different endograft designs for Zone 0 aortic arch repair. Eur. J. Cardio-Thorac. Surg. 2018, 54, 389–396. [Google Scholar] [CrossRef] [Green Version]
- Nauta, F.J.; Lau, K.D.; Arthurs, C.J.; Eagle, K.A.; Williams, D.M.; Trimarchi, S.; Patel, H.J.; Figueroa, C.A. Computational fluid dynamics and aortic thrombus formation following thoracic endovascular aortic repair. Ann. Thorac. Surg. 2017, 103, 1914–1921. [Google Scholar] [CrossRef] [Green Version]
- Santos, I.C.; Rodrigues, A.; Figueiredo, L.; Rocha, L.A.; Tavares, J.M.R. Mechanical properties of stent–graft materials. Proc. Inst. Mech. Eng. 2012, 226, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Pirola, S.; Cheng, Z.; Jarral, O.A.; O’Regan, D.P.; Pepper, J.R.; Athanasiou, T.; Xu, X.Y. On the choice of outlet boundary conditions for patient-specific analysis of aortic flow using computational fluid dynamics. J. Biomech. 2017, 60, 15–21. [Google Scholar] [CrossRef]
- Buchanan, J.R.; Kleinstreuer, C.; Comer, J.K. Rheological effects on pulsatile hemodynamics in a stenosed tube. Comput. Fluids 2000, 29, 695–724. [Google Scholar] [CrossRef]
- Popel, A.S.; Enden, G. An analytical solution for steady flow of a Quemada fluid in a circular tube. Rheol. Acta 1993, 32, 422–426. [Google Scholar] [CrossRef]
- Biasetti, J.; Gasser, T.C.; Auer, M.; Hedin, U.; Labruto, F. Hemodynamics of the normal aorta compared to fusiform and saccular abdominal aortic aneurysms with emphasis on a potential thrombus formation mechanism. Ann. Biomed. Eng. 2010, 38, 380–390. [Google Scholar] [CrossRef]
- Perktold, K.; Resch, M.; Florian, H. Pulsatile Non-Newtonian Flow Characteristics in a Three-Dimensional Human Carotid Bifurcation Model. J. Biomech. Eng. 1991, 113, 464–475. [Google Scholar] [CrossRef]
- Cho, Y.I.; Kensey, K.R. Effects of the Non-Newtonian Viscosity of Blood on Flows in a Diseased Arterial Vessel. Part 1: Steady Flows. Biorheology 1991, 28, 241–262. [Google Scholar] [CrossRef]
- Lee, S.-W.; Steinman, D.A. On the relative importance of rheology for image-based cfd models of the carotid bifurcation. J. Biomech. Eng. 2007, 129, 273–278. [Google Scholar] [CrossRef]
- Nguyen, K.T.; Clark, C.D.; Chancellor, T.J.; Papavassiliou, D.V. Carotid geometry effects on blood flow and on risk for vascular disease. J. Biomech. 2008, 41, 11–19. [Google Scholar] [CrossRef]
- Polanczyk, A.; Podyma, M.; Stefanczyk, L.; Szubert, W.; Zbicinski, I. A 3D model of thrombus formation in a stent-graft after implantation in the abdominal aorta. J. Biomech. 2015, 48, 425–431. [Google Scholar] [CrossRef]
- Holmlund, P. Computational Fluid Dynamic Simulations of Pulsatile Flow in Stenotic Vessel Models. Master’s Thesis, Umeå University, Umeå, Sweden, 2013. [Google Scholar]
- Wood, N.B. Aspects of Fluid Dynamics Applied to the Larger Arteries. J. Theor. Biol. 1999, 199, 137–161. [Google Scholar] [CrossRef]
- Kousera, C.A.; Wood, N.B.; Seed, W.A.; Torii, R.; O’Regan, D.; Xu, X.Y. A Numerical Study of Aortic Flow Stability and Comparison With In Vivo Flow Measurements. J. Biomech. Eng. 2013, 135, 011003. [Google Scholar] [CrossRef]
- Nerem, R.M.; Seed, W.A.; Wood, N.B. An experimental study of the velocity distribution and transition to turbulence in the aorta. J. Fluid Mech. 1972, 52, 137–160. [Google Scholar] [CrossRef]
- Kandail, H.; Hamady, M.; Xu, X.Y. Patient-Specific Analysis of Displacement Forces Acting on Fenestrated Stent Grafts for Endovascular Aneurysm Repair. J. Biomech. 2014, 47, 3546–3554. [Google Scholar] [CrossRef]
- Di Achille, P.; Tellides, G.; Figueroa, C.A.; Humphrey, J.D. A Haemodynamic Predictor of Intraluminal Thrombus Formation in Abdominal Aortic Aneurysms. Proc. Math. Phys. Eng. 2014, 470, 20140163. [Google Scholar] [CrossRef] [Green Version]
- Morbiducci, U.; Ponzini, R.; Rizzo, G.; Cadioli, M.; Esposito, A.; De Cobelli, F.; Del Maschio, A.; Montevecchi, F.M.; Redaelli, A. In Vivo Quantification of Helical Blood Flow in Human Aorta by Time-Resolved Three-Dimensional Cine Phase Contrast Magnetic Resonance Imaging. Ann. Biomed. Eng. 2009, 37, 516–531. [Google Scholar] [CrossRef]
- Suess, T.; Anderson, J.; Danielson, L.; Pohlson, K.; Remund, T.; Blears, E.; Gent, S.; Kelly, P. Examination of Near-Wall Hemodynamic Parameters in the Renal Bridging Stent of Various Stent Graft Configurations for Repairing Visceral Branched Aortic Aneurysms. J. Vasc. Surg. 2016, 64, 788–796. [Google Scholar] [CrossRef] [Green Version]
- Mohamied, Y.; Sherwin, S.J.; Weinberg, P.D. Understanding the fluid mechanics behind transverse wall shear stress. J. Biomech. 2017, 50, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Tan, F.P.P.; Borghi, A.; Mohiaddin, R.H.; Wood, N.B.; Thom, S.; Xu, X.Y. Analysis of flow patterns in a patient-specific thoracic aortic aneurysm model. Comput. Struct. 2009, 87, 680–690. [Google Scholar] [CrossRef]
- Midulla, M.; Moreno, R.; Negre-Salvayre, A.; Beregi, J.-P.; Haulon, S.; Loffroy, R.; Dake, M.; Rousseau, H. Impact of Thoracic Endografting on the Hemodynamics of the Native Aorta: Pre-and Postoperative Assessments of Wall Shear Stress and Vorticity Using Computational Fluid Dynamics. J. Endovasc. Ther. 2021, 28, 63–69. [Google Scholar] [CrossRef]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef]
- Nobili, M.; Sheriff, J.; Morbiducci, U.; Redaelli, A.; Bluestein, D. Platelet Activation Due to Hemodynamic Shear Stresses: Damage Accumulation Model and Comparison to in Vitro Measurements. ASAIO J. 2008, 54, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Ekaterinaris, J.A.; Ioannou, C.V.; Katsamouris, A.N. Flow Dynamics in Expansions Characterizing Abdominal Aorta Aneurysms. Ann. Vasc. Surg. 2006, 20, 351–359. [Google Scholar] [CrossRef]
- Fry, D.L. Certain Histological and Chemical Responses of the Vascular Interface to Acutely Induced Mechanical Stress in the Aorta of the Dog. Circ. Res. 1969, 24, 93–108. [Google Scholar] [CrossRef]
- Liu, Z.; Teng, S.; Chen, G.; Wu, L.; Yang, J.; Cui, F.; Ho, P. A systematic approach to further improve stent-graft performance. Mater. Des. 2021, 211, 110144. [Google Scholar] [CrossRef]
- Liu, J.; Cai, X.; Zhan, Y.; Zhu, H.; Ao, H.; Wan, Y.; Luo, H.; Yang, Z.; Zhang, Q. Hemodynamic evaluation of different stent graft schemes in aortic arch covered stent implantation. Med. Nov. Technol. Devices 2022, 13, 100108. [Google Scholar] [CrossRef]
- Zhu, Y. Computational Analysis of the Hemodynamic Performance of Novel Endovascular and Surgical Procedures for Complex Aortic Diseases. Ph.D. Thesis, Imperial College, London, UK, 2020. [Google Scholar]
- Finlay, A.; Johnson, M.; Forbes, T.L. Surgically Relevant Aortic Arch Mapping Using Computed Tomography. Ann. Vasc. Surg. 2012, 26, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Chatzizisis, Y.S.; Coskun, A.U.; Jonas, M.; Edelman, E.R.; Feldman, C.L.; Stone, P.H. Role of Endothelial Shear Stress in the Natural History of Coronary Atherosclerosis and Vascular Remodeling: Molecular, Cellular, and Vascular Behavior. J. Am. Coll. Cardiol. 2007, 49, 2379–2393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, T.L.; Tang, A.Y.S.; Cheng, S.W.K.; Chow, K.W. Analysis of flow patterns on branched endografts for aortic arch aneurysms. Inform. Med. Unlocked 2018, 13, 62–70. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhan, W.; Hamady, M.; Xu, X.Y. A pilot study of aortic hemodynamics before and after thoracic endovascular repair with a double-branched endograft. Med. Nov. Technol. Devices 2019, 4, 100027. [Google Scholar] [CrossRef]
- Xiong, Z.; Yang, P.; Li, D.; Qiu, Y.; Zheng, T.; Hu, J. A computational fluid dynamics analysis of a patient with acute non-A-non-B aortic dissection after type I hybrid arch repair. Med. Eng. Phys. 2020, 77, 43–52. [Google Scholar] [CrossRef]
- Sengupta, S.; Hamady, M.; Xu, X.-Y. Haemodynamic Analysis of Branched Endografts for Complex Aortic Arch Repair. Bioengineering 2022, 9, 45. [Google Scholar] [CrossRef]
- Qiao, Y.; Mao, L.; Ding, Y.; Fan, J.; Zhu, T.; Luo, K. Hemodynamic consequences of TEVAR with in situ double fenestrations of left carotid artery and left subclavian artery. Med. Eng. Phys. 2020, 76, 32–39. [Google Scholar] [CrossRef]
- Auricchio, F.; Conti, M.; Lefieux, A.; Morganti, S.; Reali, A.; Sardanelli, F.; Secchi, F.; Trimarchi, S.; Veneziani, A. Patient-specific analysis of post-operative aortic hemodynamics: A focus on thoracic endovascular repair (TEVAR). Comput. Mech. 2014, 54, 943–953. [Google Scholar] [CrossRef]
- van Bakel, T.M.; Romarowski, R.M.; Morganti, S.; van Herwaarden, J.A.; Moll, F.L.; de Beaufort, H.W.; Marrocco-Trischitta, M.M.; Secchi, F.; Conti, M.; Auricchio, F.; et al. Blood flow after endovascular repair in the aortic arch: A computational analysis. Aorta 2018, 06, 081–087. [Google Scholar] [CrossRef] [Green Version]
- Tricarico, R.; Tran-Son-Tay, R.; Laquian, L.; Scali, S.T.; Lee, T.-C.; Beck, A.W.; Berceli, S.A.; He, Y. Haemodynamics of different configurations of a left subclavian artery stent graft for thoracic endovascular aortic repair. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 7–15. [Google Scholar] [CrossRef] [Green Version]
- De Bock, S.; Iannaccone, F.; De Santis, G.; De Beule, M.; Van Loo, D.; Devos, D.; Vermassen, F.; Segers, P.; Verhegghe, B. Virtual Evaluation of Stent Graft Deployment: A Validated Modeling and Simulation Study. J. Mech. Behav. Biomed. Mater. 2012, 13, 129–139. [Google Scholar] [CrossRef]
- Perrin, D.; Badel, P.; Orgéas, L.; Geindreau, C.; Dumenil, A.; Albertini, J.-N.; Avril, S. Patient-Specific Numerical Simulation of Stent-Graft Deployment: Validation on Three Clinical Cases. J. Biomech. 2015, 48, 1868–1875. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Wei, J.; Deng, Y.; Xu, H.; Li, Z.; Meng, H.; Han, X.; Wang, Y.; Wan, J.; Yan, T.; et al. Virtual Stenting with Simplex Mesh and Mechanical Contact Analysis for Real-Time Planning of Thoracic Endovascular Aortic Repair. Theranostics 2018, 8, 5758–5771. [Google Scholar] [CrossRef]
- Kan, X.; Ma, T.; Lin, J.; Wang, L.; Dong, Z.; Xu, X.Y. Patient-specific simulation of stent-graft deployment in type B aortic dissection: Model development and validation. Biomech. Model. Mechanobiol. 2021, 20, 2247–2258. [Google Scholar] [CrossRef]
- Wei, L.; Leo, H.L.; Chen, Q.; Li, Z. Structural and Hemodynamic Analyses of Different Stent Structures in Curved and Stenotic Coronary Artery. Front. Bioeng. Biotechnol. 2019, 7, 366. [Google Scholar] [CrossRef] [Green Version]
- Derycke, L.; Perrin, D.; Cochennec, F.; Albertini, J.-N.; Avril, S. Predictive numerical simulations of double branch stent-graft deployment in an aortic arch aneurysm. Ann. Biomed. Eng. 2019, 47, 1051–1062. [Google Scholar] [CrossRef] [Green Version]
- Romarowski, R.M.; Faggiano, E.; Conti, M.; Reali, A.; Morganti, S.; Auricchio, F. A novel computational framework to predict patient-specific hemodynamics after TEVAR: Integration of structural and fluid-dynamics analysis by image elaboration. Comput. Fluids 2019, 179, 806–819. [Google Scholar] [CrossRef]
- Buth, J.; Harris, P.L.; Hobo, R.; van Eps, R.; Cuypers, P.; Duijm, L.; Tielbeek, X. Neurologic Complications Associated with Endovascular Repair of Thoracic Aortic Pathology: Incidence and Risk Factors. A Study from the European Collaborators on Stent/Graft Techniques for Aortic Aneurysm Repair (EUROSTAR) Registry. J. Vasc. Surg. 2007, 46, 1103–1110. [Google Scholar] [CrossRef]
- Menichini, C.; Xu, X.Y. Mathematical modeling of thrombus formation in idealized models of aortic dissection: Initial findings and potential applications. J. Math. Biol. 2016, 73, 1205–1226. [Google Scholar] [CrossRef] [Green Version]
- Menichini, C.; Cheng, Z.; Gibbs, R.G.J.; Xu, X.Y. A Computational Model for False Lumen Thrombosis in Type B Aortic Dissection Following Thoracic Endovascular Repair. J. Biomech. 2018, 66, 36–43. [Google Scholar] [CrossRef]
- Arzani, A.; Wang, J.-X.; Sacks, M.S.; Shadden, S.C. Machine Learning for Cardiovascular Biomechanics Modeling: Challenges and Beyond. Ann. Biomed. Eng. 2022, 50, 615–627. [Google Scholar] [CrossRef]








| Metric | Mathematical Expression | Description |
|---|---|---|
| Displacement force [55] | Time dependent displacement force due to pressure and friction exerted by the flow of blood on the walls. | |
| Endothelial cell activation potential (ECAP) [56] | Synthetic metric to identify regions at a higher risk of thrombus formation. | |
| Helical flow index (HFI) [57] | Synthetic descriptor to quantify helicity of particles flowing through the fluid domain. | |
| Oscillatory shear index (OSI) [58] | Change of direction of the wall shear stress (WSS) vector from the primary direction of flow. | |
| Platelet activation potential (PLAP) [40] | Non-dimensional scalar index of magnitudes of shear rate that particles accumulate travelling through the domain. | |
| Time-averaged WSS (TAWSS) [58] | Average of the WSS magnitude over the cardiac cycle. | |
| Relative residence time (RRT) [58] | Amount of time that solutes and particles of the blood may spend near the vessel wall. | |
| Transverse WSS [59] | Average over the cardiac cycle of WSS components perpendicular to the temporal mean WSS vector. | |
| Turbulence intensity (Tu) [60] | Used to measure the level of turbulence and disturbance in flow. | |
| Vorticity [61] | Vector field that describes the circulation per unit area at a point in a fluid flow field. | |
| T is the time period of a cardiac cycle; τw is the wall shear stress vector; vx, vy, vz are the velocity fields in the x, y, and z components; k is the turbulence kinetic energy; V is the instantaneous localised velocity, is the local normalised helicity, is the Frobenius norm of the symmetric part of the spatial gradient of the velocity tensor. | ||
| Authors | Year | Landing Zone | Condition and Treatment/Device | Key Findings |
|---|---|---|---|---|
| Midulla et al. [61] | 2021 | 0–4 |
|
|
| van Bakel et al. [39] | 2018 | 0 |
|
|
| Chiu et al. [71] | 2018 | 0 |
|
|
| Zhu et al. [72] | 2019 | 0 |
|
|
| Xiong et al. [73] | 2020 | 0 |
|
|
| Sengupta et al. [74] | 2022 | 0 |
|
|
| Qiao et al. [75] | 2019 | 1 |
|
|
| Auricchio et al. [76] | 2014 | 2 |
|
|
| Nauta et al. [40] | 2017 | 2 |
|
|
| Van Bakel et al. [77] | 2018 | 2 |
|
|
| Tricarico et al. [78] | 2020 | 2 |
|
|
| FL—False lumen, OSI—Oscillatory shear index, PLAP—Platelet activation potential, RRT—Relative residence time, TAWSS—Time-averaged wall shear stress, TL—True lumen, WSS—Wall shear stress, TBAD—Type B aortic dissection, TEVAR—Thoracic endovascular aortic repair | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sengupta, S.; Zhu, Y.; Hamady, M.; Xu, X.Y. Evaluating the Haemodynamic Performance of Endografts for Complex Aortic Arch Repair. Bioengineering 2022, 9, 573. https://doi.org/10.3390/bioengineering9100573
Sengupta S, Zhu Y, Hamady M, Xu XY. Evaluating the Haemodynamic Performance of Endografts for Complex Aortic Arch Repair. Bioengineering. 2022; 9(10):573. https://doi.org/10.3390/bioengineering9100573
Chicago/Turabian StyleSengupta, Sampad, Yu Zhu, Mohamad Hamady, and Xiao Yun Xu. 2022. "Evaluating the Haemodynamic Performance of Endografts for Complex Aortic Arch Repair" Bioengineering 9, no. 10: 573. https://doi.org/10.3390/bioengineering9100573
APA StyleSengupta, S., Zhu, Y., Hamady, M., & Xu, X. Y. (2022). Evaluating the Haemodynamic Performance of Endografts for Complex Aortic Arch Repair. Bioengineering, 9(10), 573. https://doi.org/10.3390/bioengineering9100573