



A Deep Learning Approach for Detecting Stroke from Brain CT Images Using OzNet



Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
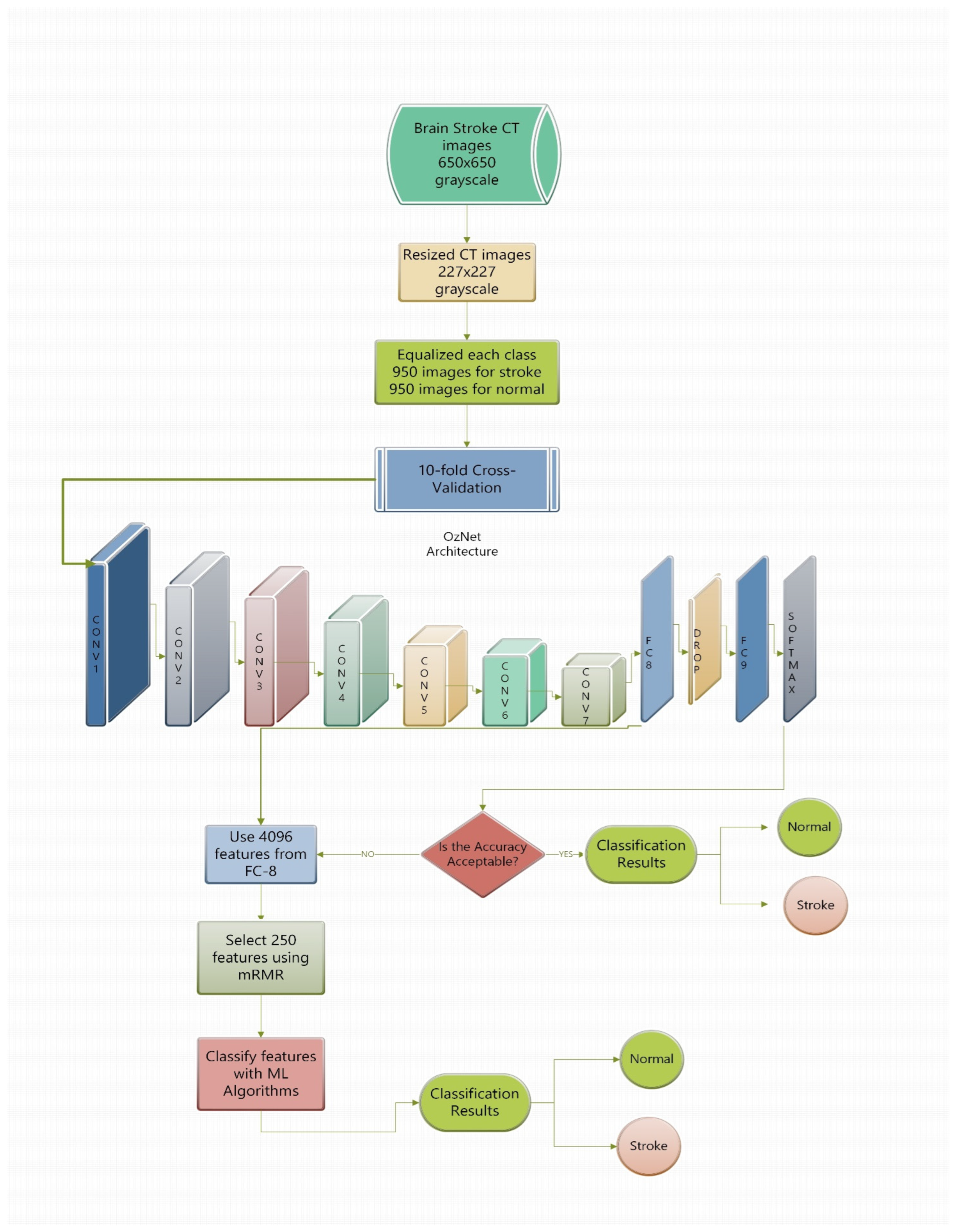
3.1. Dataset
3.2. A Novel CNN Architecture
3.3. Minimum Redundancy Maximum Relevance (mRMR) Method
3.4. Decision Tree (DT)
3.5. k-Nearest Neighbor (kNN)
3.6. Linear Discriminant Analysis (LDA)
3.7. Naïve Bayes (NB)
3.8. Support Vector Machine (SVM)
4. Results and Discussion
4.1. Performance Metrics
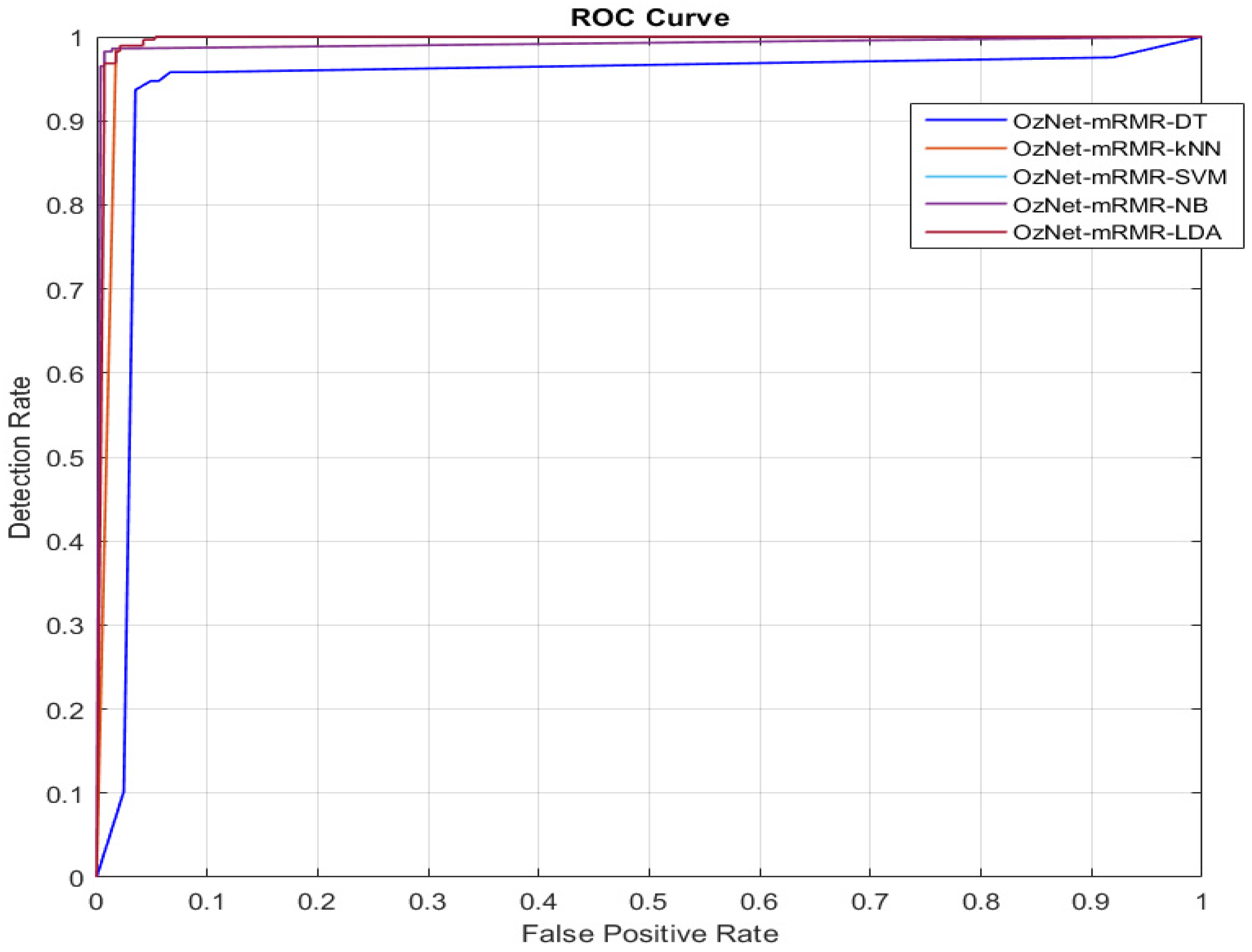
4.2. Receiver Operating Characteristic (ROC) Curve
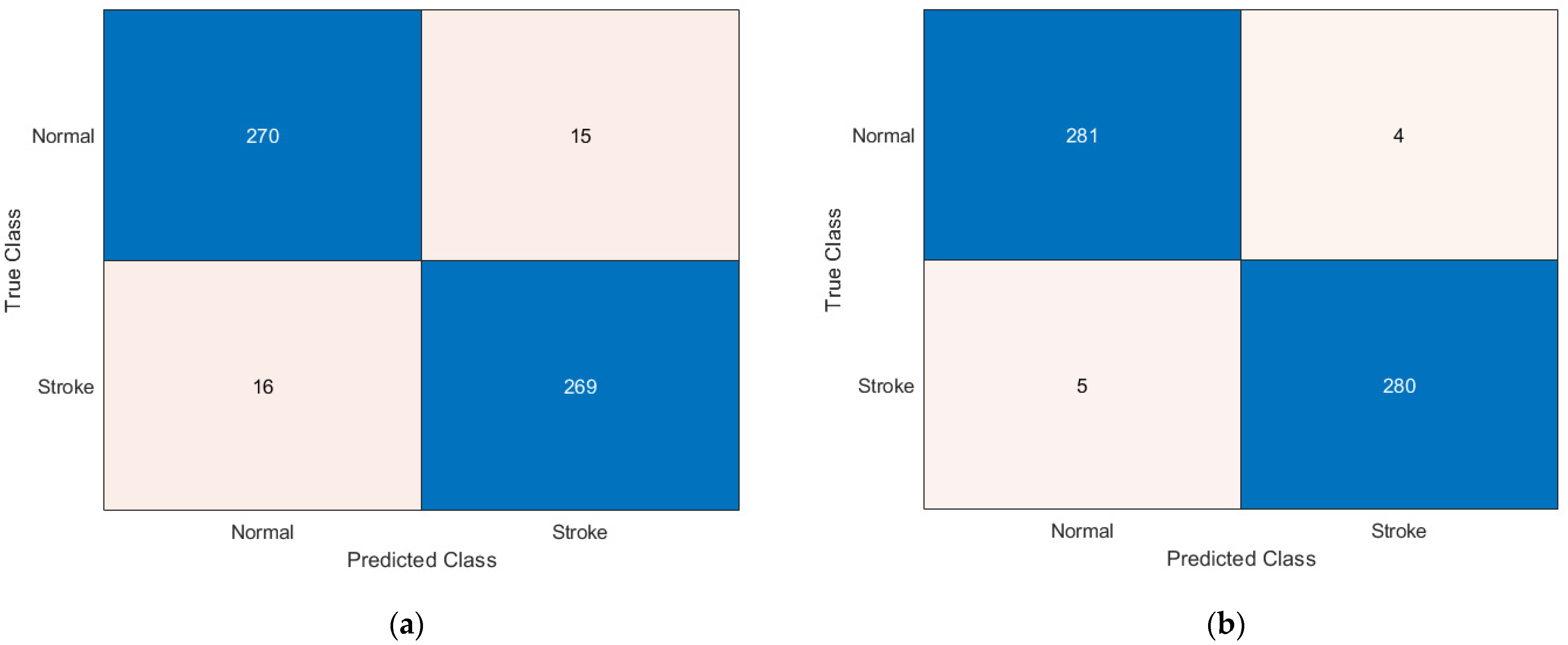
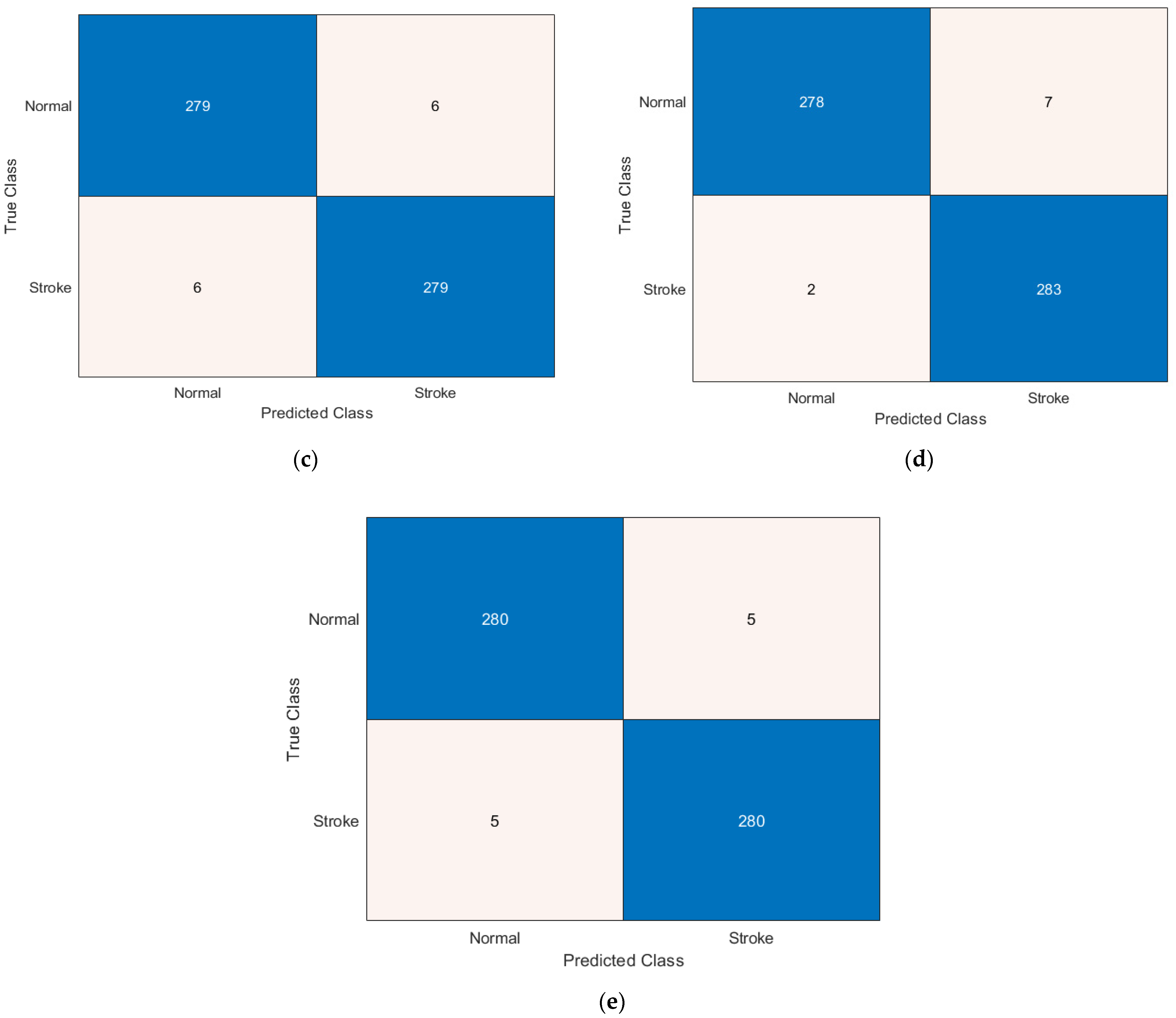
4.3. Experimental Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merino, J.G. Clinical stroke challenges: A practical approach. Neurol. Clin. Pr. 2014, 4, 376–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overgaard, K. The Effects of Citicoline on Acute Ischemic Stroke: A Review. J. Stroke Cerebrovasc. Dis. 2014, 23, 1764–1769. [Google Scholar] [CrossRef] [Green Version]
- Sirsat, M.S.; Fermé, E.; Câmara, J. Machine learning for brain stroke: A review. J. Stroke Cerebrovasc. Dis. 2020, 29, 105162. [Google Scholar] [CrossRef]
- Gao, X.W.; Hui, R.; Tian, Z. Classification of CT brain images based on deep learning networks. Comput. Methods Programs Biomed. 2017, 138, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wei, M.; Liu, B.; Atchaneeyasakul, K.; Zhou, F.; Pan, Z.; Kumar, S.A.; Zhang, J.Y.; Pu, Y.; Liebeskind, D.S.; et al. Deep Learning for Hemorrhagic Lesion Detection and Segmentation on Brain CT Images. IEEE J. Biomed. Health Inform. 2020, 25, 1646–1659. [Google Scholar] [CrossRef]
- Srikrishna, M.; Pereira, J.B.; Heckemann, R.A.; Volpe, G.; van Westen, D.; Zettergren, A.; Kern, S.; Wahlund, L.-O.; Westman, E.; Skoog, I.; et al. Deep learning from MRI-derived labels enables automatic brain tissue classification on human brain CT. Neuroimage 2021, 244, 118606. [Google Scholar] [CrossRef]
- Ozaltin, O.; Coskun, O.; Yeniay, O.; Subasi, A. Classification of brain hemorrhage computed tomography images using OzNet hybrid algorithm. Int. J. Imaging Syst. Technol. 2022. [Google Scholar] [CrossRef]
- Jayachitra, S.; Prasanth, A. Multi-Feature Analysis for Automated Brain Stroke Classification Using Weighted Gaussian Naïve Bayes Classifier. J. Circuits Syst. Comput. 2021, 30, 2150178. [Google Scholar] [CrossRef]
- Subudhi, A.; Dash, M.; Sabut, S. Automated segmentation and classification of brain stroke using expectation-maximization and random forest classifier. Biocybern. Biomed. Eng. 2020, 40, 277–289. [Google Scholar] [CrossRef]
- Bento, M.; Souza, R.; Salluzzi, M.; Rittner, L.; Zhang, Y.; Frayne, R. Automatic identification of atherosclerosis subjects in a heterogeneous MR brain imaging data set. Magn. Reson. Imaging 2019, 62, 18–27. [Google Scholar] [CrossRef]
- Kasabov, N.; Feigin, V.L.; Hou, Z.-G.; Chen, Y.; Liang, L.; Krishnamurthi, R.; Othman, M.; Parmar, P. Evolving spiking neural networks for personalised modelling, classification and prediction of spatio-temporal patterns with a case study on stroke. Neurocomputing 2014, 134, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Karthik, R.; Gupta, U.; Jha, A.; Rajalakshmi, R.; Menaka, R. A deep supervised approach for ischemic lesion segmentation from multimodal MRI using Fully Convolutional Network. Appl. Soft Comput. 2019, 84, 105685. [Google Scholar] [CrossRef]
- Filho, P.P.R.; Sarmento, R.M.; Holanda, G.B.; Lima, D.D.A. New approach to detect and classify stroke in skull CT images via analysis of brain tissue densities. Comput. Methods Programs Biomed. 2017, 148, 27–43. [Google Scholar] [CrossRef]
- Vargas, J.; Spiotta, A.; Chatterjee, A.R. Initial Experiences with Artificial Neural Networks in the Detection of Computed Tomography Perfusion Deficits. World Neurosurg. 2019, 124, e10–e16. [Google Scholar] [CrossRef]
- Dourado, C.M., Jr.; da Silva, S.P.P.; da Nóbrega, R.V.M.; Barros, A.C.D.S.; Filho, P.P.R.; de Albuquerque, V.H.C. Deep learning IoT system for online stroke detection in skull computed tomography images. Comput. Netw. 2019, 152, 25–39. [Google Scholar] [CrossRef]
- Li, X.; Wu, M.; Sun, C.; Zhao, Z.; Wang, F.; Zheng, X.; Ge, W.; Zhou, J. Using machine learning to predict stroke-associated pneumonia in Chinese acute ischaemic stroke patients. Eur. J. Neurol. 2020, 27, 1656–1663. [Google Scholar] [CrossRef]
- Gautam, A.; Raman, B. Towards effective classification of brain hemorrhagic and ischemic stroke using CNN. Biomed. Signal Process. Control. 2020, 63, 102178. [Google Scholar] [CrossRef]
- Bacchi, S.; Zerner, T.; Oakden-Rayner, L.; Kleinig, T.; Patel, S.; Jannes, J. Deep learning in the prediction of ischaemic stroke thrombolysis functional outcomes: A pilot study. Acad. Radiol. 2019, 27, e19–e23. [Google Scholar] [CrossRef]
- Saritha, M.; Joseph, K.P.; Mathew, A.T. Classification of MRI brain images using combined wavelet entropy based spider web plots and probabilistic neural network. Pattern Recognit. Lett. 2013, 34, 2151–2156. [Google Scholar] [CrossRef]
- El-Dahshan, E.-S.A.; Hosny, T.; Salem, A.-B.M. Hybrid intelligent techniques for MRI brain images classification. Digit. Signal Process. 2010, 20, 433–441. [Google Scholar] [CrossRef]
- Xu, Y.; Holanda, G.; Souza, L.F.d.F.; Silva, H.; Gomes, A.; Silva, I.; Ferreira, M.; Jia, C.; Han, T.; de Albuquerque, V.H.C.; et al. Deep Learning-Enhanced Internet of Medical Things to Analyze Brain CT Scans of Hemorrhagic Stroke Patients: A New Approach. IEEE Sens. J. 2020, 21, 24941–24951. [Google Scholar] [CrossRef]
- Feng, R.; Badgeley, M.; Mocco, J.; Oermann, E.K. Deep learning guided stroke management: A review of clinical applications. J. NeuroInterventional Surg. 2018, 10, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Savaş, S.; Topaloğlu, N.; Kazcı, Ö.; Koşar, P.N. Classification of carotid artery intima media thickness ultrasound images with deep learning. J. Med. Syst. 2019, 43, 8. [Google Scholar] [CrossRef] [PubMed]
- Han, T.; Nunes, V.X.; Souza, L.F.D.F.; Marques, A.G.; Silva, I.C.L.; Junior, M.A.A.F.; Sun, J.; Filho, P.P.R. Internet of Medical Things—Based on Deep Learning Techniques for Segmentation of Lung and Stroke Regions in CT Scans. IEEE Access 2020, 8, 71117–71135. [Google Scholar] [CrossRef]
- Zhu, G.; Bialkowski, A.; Guo, L.; Mohammed, B.; Abbosh, A. Stroke Classification in Simulated Electromagnetic Imaging Using Graph Approaches. IEEE J. Electromagn. RF Microw. Med. Biol. 2020, 5, 46–53. [Google Scholar] [CrossRef]
- Chin, C.-L.; Lin, B.-J.; Wu, G.-R.; Weng, T.-C.; Yang, C.-S.; Su, R.-C.; Pan, Y.-J. An automated early ischemic stroke detection system using CNN deep learning algorithm. In Proceedings of the 2017 IEEE 8th International Conference on Awareness Science and Technology (iCAST), Taichung, Taiwan, 8–10 November 2017; pp. 368–372. [Google Scholar]
- Acharya, U.R.; Meiburger, K.M.; Faust, O.; Koh, J.E.W.; Oh, S.L.; Ciaccio, E.J.; Subudhi, A.K.; Jahmunah, V.; Sabut, S. Automatic detection of ischemic stroke using higher order spectra features in brain MRI images. Cogn. Syst. Res. 2019, 58, 134–142. [Google Scholar] [CrossRef]
- Adam, S.Y.; Yousif, A.; Bashir, M.B. Classification of ischemic stroke using machine learning algorithms. Int. J. Comput. Appl. 2016, 149, 26–31. [Google Scholar]
- Gamberger, D.; Lavrač, N.; Krstačić, A.; Krstačić, G. Clinical data analysis based on iterative subgroup discovery: Experiments in brain ischaemia data analysis. Appl. Intell. 2007, 27, 205–217. [Google Scholar] [CrossRef]
- Kyriacou, E.; Pattichis, M.S.; Pattichis, C.S.; Mavrommatis, A.; Christodoulou, C.I.; Kakkos, S.; Nicolaides, A. Classification of atherosclerotic carotid plaques using morphological analysis on ultrasound images. Appl. Intell. 2009, 30, 3–23. [Google Scholar] [CrossRef]
- Kobus, M.; Sobczak, K.; Jangas, M.; Świątek, A.; Strzelecki, M. Discrimination Between Stroke and Brain Tumour in CT Images Based on the Texture Analysis. In Proceedings of the International Conference on Information Technologies in Biomedicine, Kamień Śląski, Poland, 20–22 June 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 168–180. [Google Scholar]
- Afridi, M.A.R.; Ali, Z.; Muhammad, R.; Ahmad, A.; Alam, I. Age and gender specific stroke risk factors in a teaching hospital in khyber pakhtunkhwa. J. Postgrad. Med. Inst. 2015, 29, 2. [Google Scholar]
- Weng, L.; Zhang, H.; Chen, H.; Song, Z.; Hsieh, C.J.; Daniel, L.; Dhillon, I. Towards fast computation of certified robustness for relu networks. In Proceedings of the International Conference on Machine Learning, Stockholm, Sweden, 10–15 July 2018; PMLR: Bejing, China, 2018; pp. 5276–5285. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Adam, H. Mobilenets: Efficient 465 convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Peng, H.; Long, F.; Ding, C. Feature selection based on mutual information criteria of max-dependency, max-relevance, and min-redundancy. IEEE Trans. Pattern Anal. Mach. Intell. 2005, 27, 1226–1238. [Google Scholar] [CrossRef]
- Ding, C.; Peng, H. Minimum Redundancy Feature Selection from Microarray Gene Expression Data. J. Bioinform. Comput. Biol. 2005, 3, 185–205. [Google Scholar] [CrossRef] [PubMed]
- Toğaçar, M.; Ergen, B.; Cömert, Z.; Özyurt, F. A deep feature learning model for pneumonia detection applying a combination of mRMR feature selection and machine learning models. IRBM 2020, 41, 212–222. [Google Scholar] [CrossRef]
- Jiang, H. Machine Learning Fundamentals: A Concise Introduction; Cambridge University Press: Cambridge, MA, USA, 2021. [Google Scholar]
- Quinlan, J.R. C4. 5: Programs for Machine Learning; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Subasi, A.; Balfaqih, M.; Balfagih, Z.; Alfawwaz, K. A Comparative Evaluation of Ensemble Classifiers for Malicious Webpage Detection. Procedia Comput. Sci. 2021, 194, 272–279. [Google Scholar] [CrossRef]
- Cichosz, P. Data Mining Algorithms: Explained Using R; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Quinlan, J.R. Learning decision tree classifiers. ACM Comput. Surv. 1996, 28, 71–72. [Google Scholar] [CrossRef]
- Koklu, M.; Sabanci, K. Estimation of Credit Card Customers Payment Status by Using kNN and MLP. Int. J. Intell. Syst. Appl. Eng. 2016, 4, 249–251. [Google Scholar] [CrossRef]
- Keller, J.M.; Gray, M.R.; Givens, J.A. A fuzzy K-nearest neighbor algorithm. IEEE Trans. Syst. Man Cybern. 1985, SMC-15, 580–585. [Google Scholar] [CrossRef]
- Cover, T.; Hart, P. Nearest neighbor pattern classification. IEEE Trans. Inf. Theory 1967, 13, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Pei, J.; Kamber, M. Data Mining: Concepts and Techniques; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Xanthopoulos, P.; Pardalos, P.M.; Trafalis, T.B. Linear discriminant analysis. In Robust Data Mining; Springer: Berlin/Heidelberg, Germany, 2013; pp. 27–33. [Google Scholar]
- Balakrishnama, S.; Ganapathiraju, A. Linear discriminant analysis-a brief tutorial. Inst. Signal Inf. Process. 1998, 18, 1–8. [Google Scholar]
- Koklu, M.; Unal, Y. Analysis of a population of diabetic patients databases with classifiers. Int. J. Biomed. Biol. Eng. 2013, 7, 481–483. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Barstugan, M.; Ozkaya, U.; Ozturk, S. Coronavirus (COVID-19) classification using ct images by machine learning methods. arXiv 2020, arXiv:2003.09424. [Google Scholar]
- Koklu, M.; Ozkan, I.A. Multiclass classification of dry beans using computer vision and machine learning techniques. Comput. Electron. Agric. 2020, 174, 105507. [Google Scholar] [CrossRef]
- Arlot, S.; Celisse, A. A survey of cross-validation procedures for model selection. Stat. Surv. 2010, 4, 40–79. [Google Scholar] [CrossRef]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F.; et al. Fusion of convolution neural network, support vector machine and Sobel filter for accurate detection of COVID-19 patients using X-ray images. Biomed. Signal Process. Control. 2021, 68, 102622. [Google Scholar] [CrossRef]
- Singh, D.; Taspinar, Y.S.; Kursun, R.; Cinar, I.; Koklu, M.; Ozkan, I.A.; Lee, H.-N. Classification and Analysis of Pistachio Species with Pre-Trained Deep Learning Models. Electronics 2022, 11, 981. [Google Scholar] [CrossRef]
- Rajinikanth, V.; Raj, A.N.J.; Thanaraj, K.P.; Naik, G.R. A Customized VGG19 Network with Concatenation of Deep and Handcrafted Features for Brain Tumor Detection. Appl. Sci. 2020, 10, 3429. [Google Scholar] [CrossRef]
- Taspinar, Y.S.; Cinar, I.; Koklu, M. Classification by a stacking model using CNN features for COVID-19 infection diagnosis. J. X-ray Sci. Technol. 2021, 30, 73–88. [Google Scholar] [CrossRef]
- Özaltın, Ö.; Yeniay, Ö. Ecg classification performing feature extraction automatically using a hybrid cnn-svm algorithm. In Proceedings of the 2021 3rd International Congress on Human-Computer Interaction, Optimization and Robotic Applications (HORA), Online, 11–13 June 2021; IEEE: Ankara, Turkey, 2021; pp. 1–5. [Google Scholar]
- Shalikar, A.; Ashouri, M.R.; Shahraki, M.H.N. A CAD system for automatic classification of brain strokes in CT images. Int. J. Mechatron. Electr. Comput. Technol. 2014, 10, 67–85. [Google Scholar]
- Marbun, J.T.; Seniman; Andayani, U. Classification of stroke disease using convolutional neural network. J. Phys. Conf. Ser. 2018, 978, 012092. [Google Scholar] [CrossRef]
- Diker, A.; Elen, A.; Subasi, A. Brain stroke detection from CT images using deep learning algorithms. In Applications of Artificial Intelligence in Medical Imaging; Subasi, A., Ed.; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Raghavendra, U.; Pham, T.-H.; Gudigar, A.; Vidhya, V.; Rao, B.N.; Sabut, S.; Wei, J.K.E.; Ciaccio, E.J.; Acharya, U.R. Novel and accurate non-linear index for the automated detection of haemorrhagic brain stroke using CT images. Complex Intell. Syst. 2021, 7, 929–940. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Name | Type | Size | Filters | Stride | Padding | Output |
|---|---|---|---|---|---|---|
| Input | Input | 227 × 227 × 3 | ||||
| Conv-1 | Convolution 2D | 64 | 5 × 5 | 1 | 1 | 225 × 225 × 64 |
| MaxPool-1 | Max Pooling | 3 × 3 | 2 | 0 | 112 × 112 × 64 | |
| Conv-2 | Convolution 2D | 128 | 3 × 3 | 1 | 1 | 112 × 112 × 128 |
| MaxPool-2 | Max Pooling | 3 × 3 | 2 | 0 | 55 × 55 × 128 | |
| Conv-3 | Convolution 2D | 128 | 13 × 13 | 1 | 0 | 55 × 55 × 128 |
| MaxPool-3 | Max Pooling | 3 × 3 | 2 | 0 | 27 × 27 × 128 | |
| Conv-4 | Convolution 2D | 256 | 7 × 7 | 1 | 1 | 27 × 27 × 256 |
| MaxPool-4 | Max Pooling | 2 × 2 | 2 | 0 | 13 × 13 × 256 | |
| Conv-5 | Convolution 2D | 128 | 3 × 3 | 1 | 1 | 13 × 13 × 128 |
| MaxPool-5 | Max Pooling | 3 × 3 | 2 | 0 | 6 × 6 × 128 | |
| Conv-6 | Convolution 2D | 128 | 3 × 3 | 1 | 1 | 6 × 6 × 128 |
| MaxPool-6 | Max Pooling | 3 × 3 | 2 | 0 | 3 × 3 × 128 | |
| Conv-7 | Convolution 2D | 128 | 3 × 3 | 1 | 1 | 3 × 3 × 128 |
| MaxPool-7 | Max Pooling | - | 2 × 2 | 2 | 0 | 1 × 1 × 128 |
| FC-8 | Fully Connected | 4096 | 1 × 1 × 4096 | |||
| Drop-8 | Dropout | 50% | ||||
| FC-9 | Fully Connected | number of classes | 1 × 1 × (number of classes) | |||
| Softmax | Softmax | 1 × 1 × (number of classes) | ||||
| Output | Classification | entropy |
| Performance Metrics | Equations |
|---|---|
| Accuracy | |
| F1-Score | |
| G-Mean | |
| Precision | |
| Sensitivity | |
| Specificity |
| Architectures | Performance Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Precision | F1-Score | G-Mean | Accuracy | AUC | |
| GoogleNet | 0.8095 | 0.7789 | 0.7855 | 0.7973 | 0.7941 | 0.7942 | 0.8761 |
| Inceptionv3 | 0.7526 | 0.7621 | 0.7598 | 0.7562 | 0.7574 | 0.7574 | 0.8399 |
| MobileNetv2 | 0.8768 | 0.8705 | 0.8713 | 0.8740 | 0.8736 | 0.8736 | 0.9407 |
| OzNet | 0.8716 | 0.8779 | 0.8771 | 0.8743 | 0.8747 | 0.8747 | 0.9488 |
| Algorithms | Performance Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Precision | F1-Score | G-Mean | Accuracy | AUC | |
| OzNet | 0.8716 | 0.8779 | 0.8771 | 0.8743 | 0.8747 | 0.8747 | 0.9488 |
| OzNet-DT | 0.9023 | 0.9053 | 0.9050 | 0.9036 | 0.9038 | 0.9038 | 0.9238 |
| OzNet-kNN | 0.9489 | 0.9579 | 0.9575 | 0.9532 | 0.9534 | 0.9534 | 0.9534 |
| OzNet-LDA | 0.9669 | 0.9609 | 0.9611 | 0.9640 | 0.9639 | 0.9639 | 0.9937 |
| OzNet-NB | 0.9774 | 0.9489 | 0.9503 | 0.9637 | 0.9631 | 0.9632 | 0.9674 |
| OzNet-SVM | 0.9594 | 0.9714 | 0.9711 | 0.9652 | 0.9654 | 0.9654 | 0.9921 |
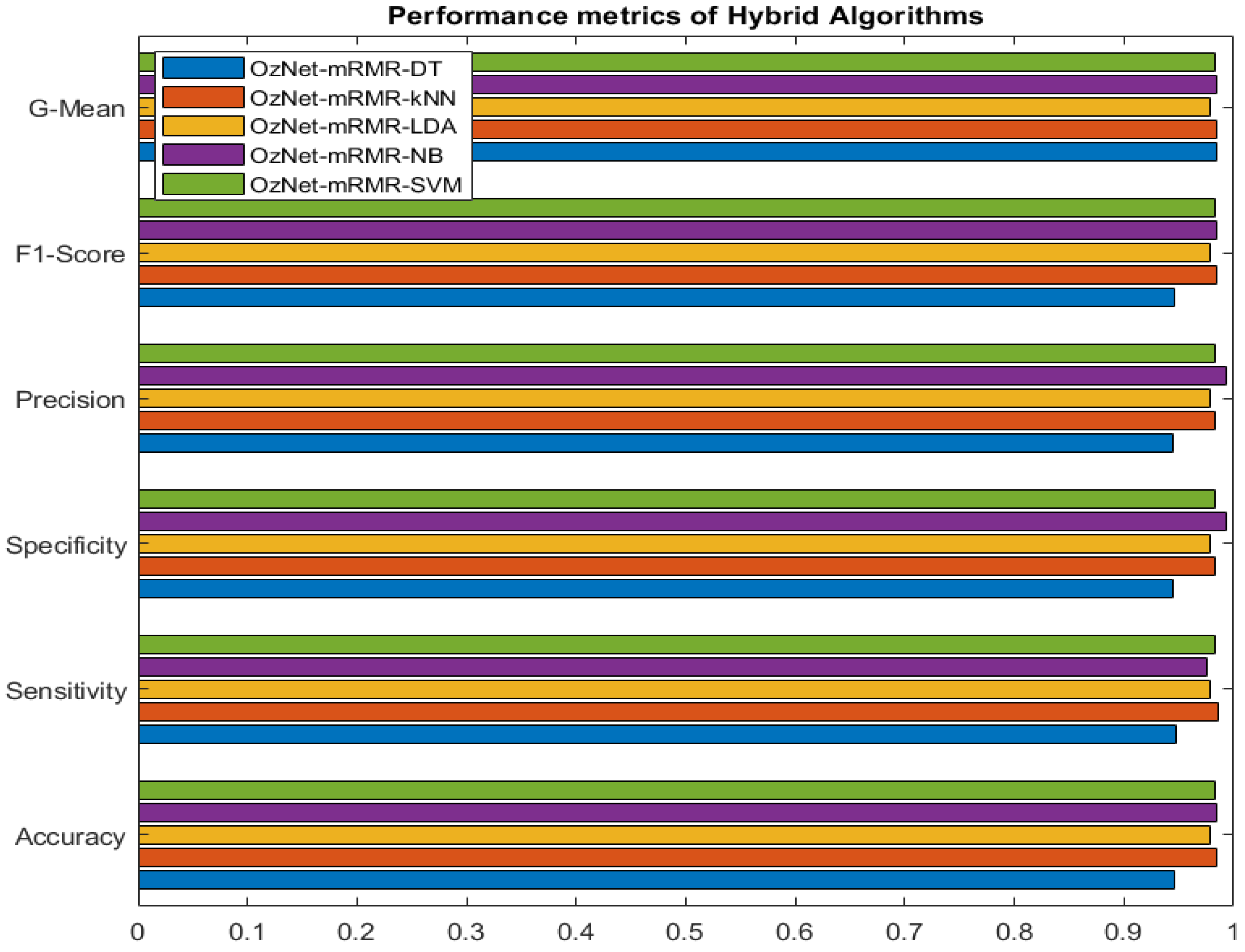
| Algorithms | Performance Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Precision | F1-Score | G-Mean | Accuracy | AUC | |
| OzNet-mRMR-DT | 0.9474 | 0.9439 | 0.9441 | 0.9457 | 0.9456 | 0.9456 | 0.9403 |
| OzNet-mRMR-kNN | 0.9860 | 0.9825 | 0.9825 | 0.9842 | 0.9842 | 0.9842 | 0.9842 |
| OzNet-mRMR-LDA | 0.9789 | 0.9789 | 0.9789 | 0.9789 | 0.9789 | 0.9789 | 0.9984 |
| OzNet-mRMR-NB | 0.9754 | 0.9930 | 0.9929 | 0.9841 | 0.9842 | 0.9842 | 0.9909 |
| OzNet-mRMR-SVM | 0.9825 | 0.9825 | 0.9825 | 0.9825 | 0.9825 | 0.9825 | 0.9956 |
| Works | Data Type | Classifier | Accuracy |
|---|---|---|---|
| Chin et al. [26] | Brain CT | CNN | 90% |
| Shalikar et al. [61] | Brain CT | SVM | 90% |
| Marbun et al. [62] | Brain CT | CNN | 90% |
| Diker et al. [63] | Brain CT | VGG-19 | 97.06% |
| Raghavendra et al. [64] | Brain CT | PNN (Probabilistic Neural Network) | 94.37% |
| This study | Brain CT | OzNet-mRMR-NB | 98.42% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozaltin, O.; Coskun, O.; Yeniay, O.; Subasi, A. A Deep Learning Approach for Detecting Stroke from Brain CT Images Using OzNet. Bioengineering 2022, 9, 783. https://doi.org/10.3390/bioengineering9120783
Ozaltin O, Coskun O, Yeniay O, Subasi A. A Deep Learning Approach for Detecting Stroke from Brain CT Images Using OzNet. Bioengineering. 2022; 9(12):783. https://doi.org/10.3390/bioengineering9120783
Chicago/Turabian StyleOzaltin, Oznur, Orhan Coskun, Ozgur Yeniay, and Abdulhamit Subasi. 2022. "A Deep Learning Approach for Detecting Stroke from Brain CT Images Using OzNet" Bioengineering 9, no. 12: 783. https://doi.org/10.3390/bioengineering9120783
APA StyleOzaltin, O., Coskun, O., Yeniay, O., & Subasi, A. (2022). A Deep Learning Approach for Detecting Stroke from Brain CT Images Using OzNet. Bioengineering, 9(12), 783. https://doi.org/10.3390/bioengineering9120783