

A Highly Sensitive Urinary Exosomal miRNAs Biosensor Applied to Evaluation of Prostate Cancer Progression

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Urine Samples Collection
2.2. Reagents and Chemicals
2.3. Methods and Apparatus
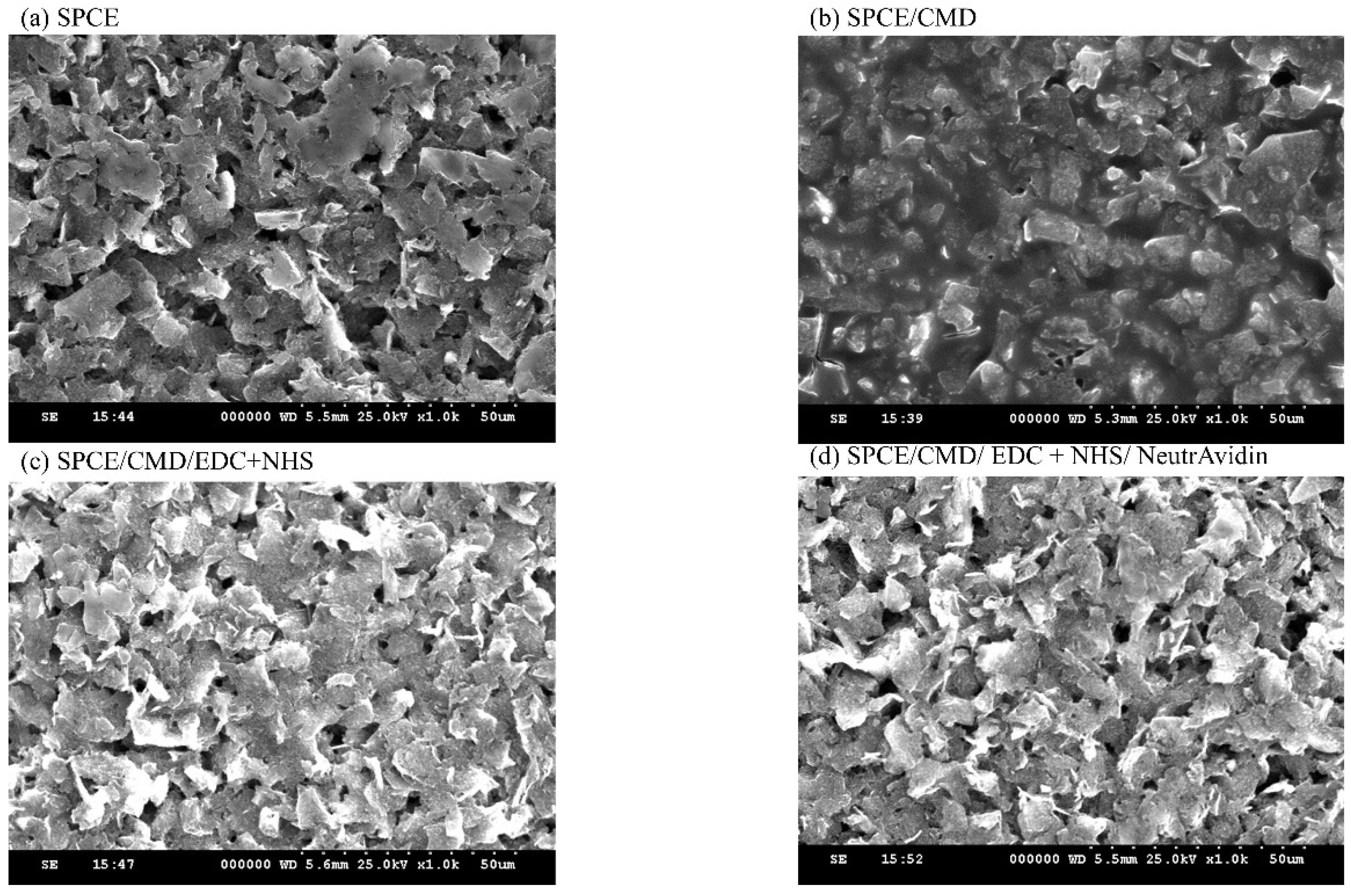
2.3.1. Characterization of SPCE by SEM
2.3.2. Electrochemical Analysis
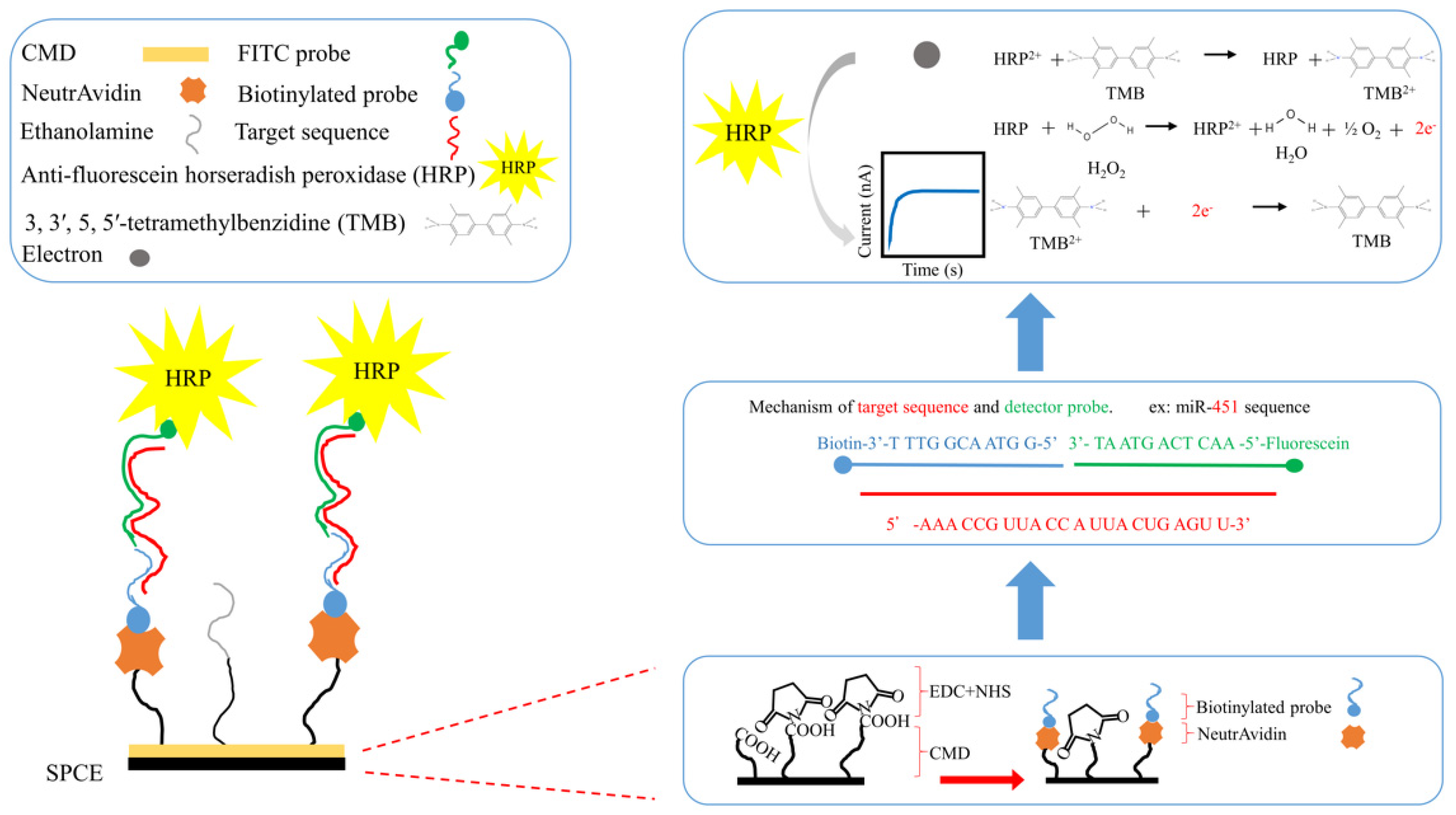
2.3.3. Biotinylated Capture Probe and FITC Detector Probe Design
2.3.4. Modification of SPCE
2.4. Isolation and Quantification of MicroRNAs from Urinary Exosomes
2.5. Statistical Evaluation
3. Results
3.1. Characterization of exomiR-SPCE-Based Biosensor
3.1.1. Characterization of Modified SPCE by Scanning Electron Microscopy (SEM)
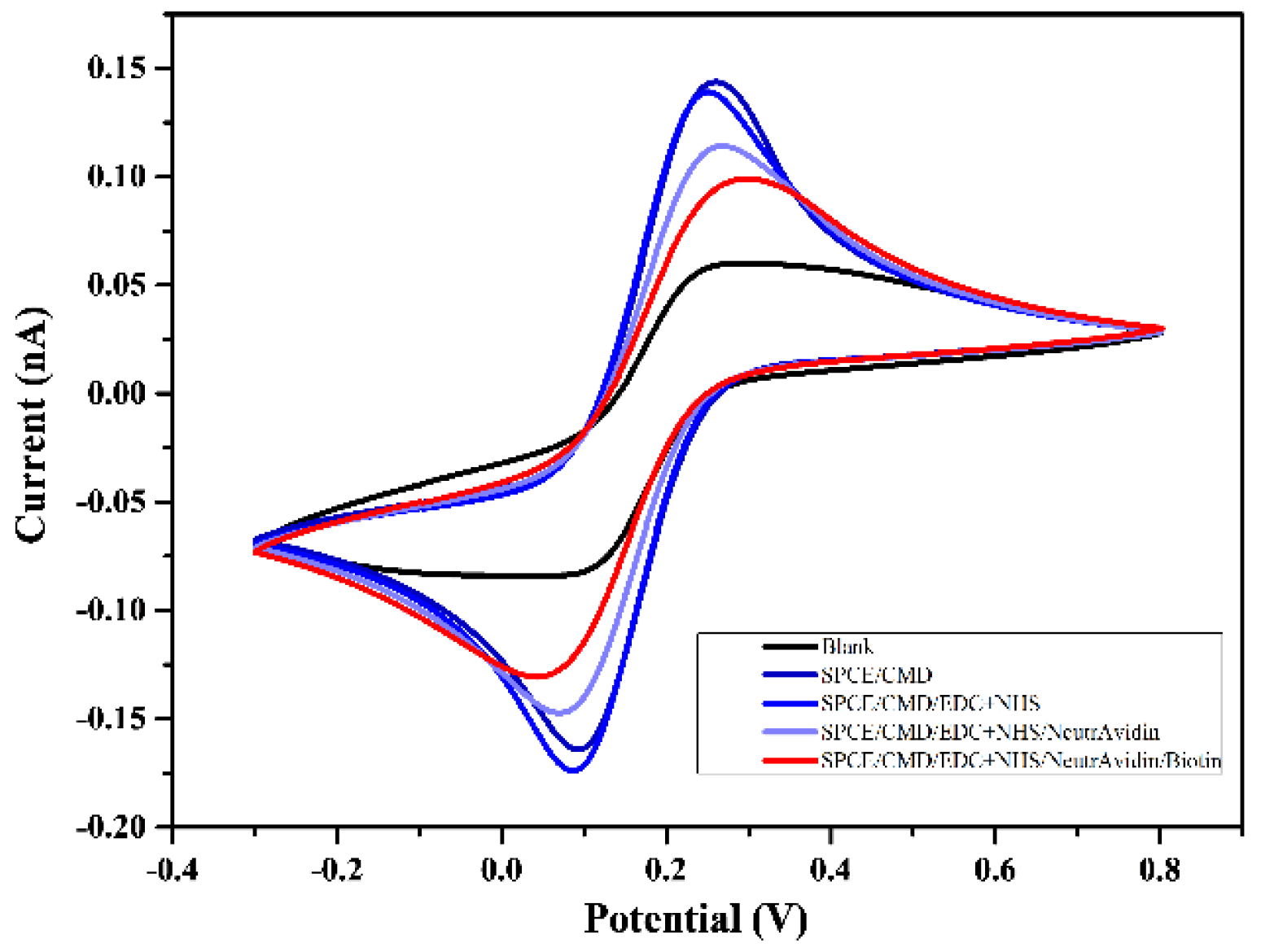
3.1.2. Characterization of ExomiR-SPCE by Cyclic Voltammetry
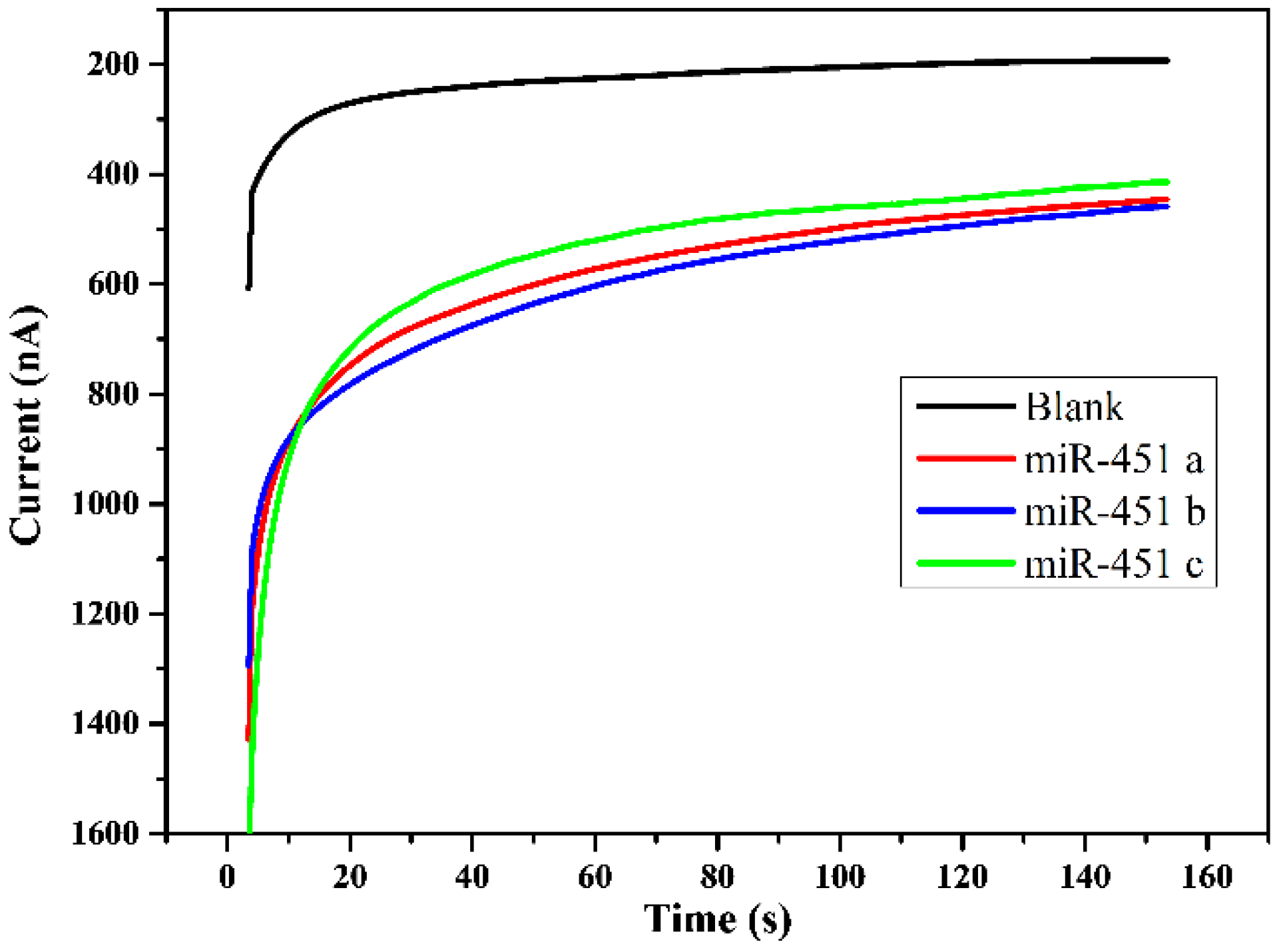
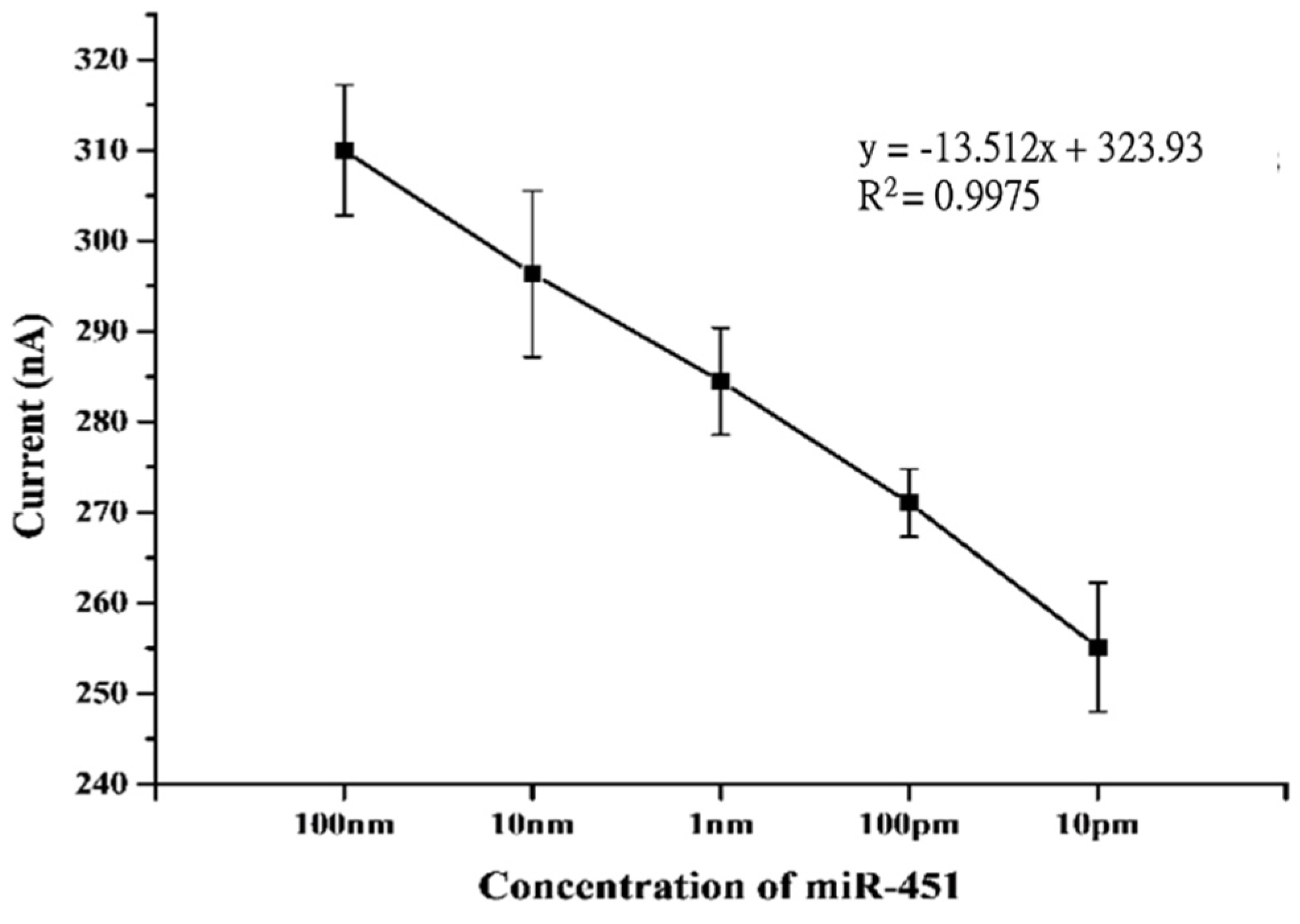
3.2. Characterization of Biosensor Sensitivity
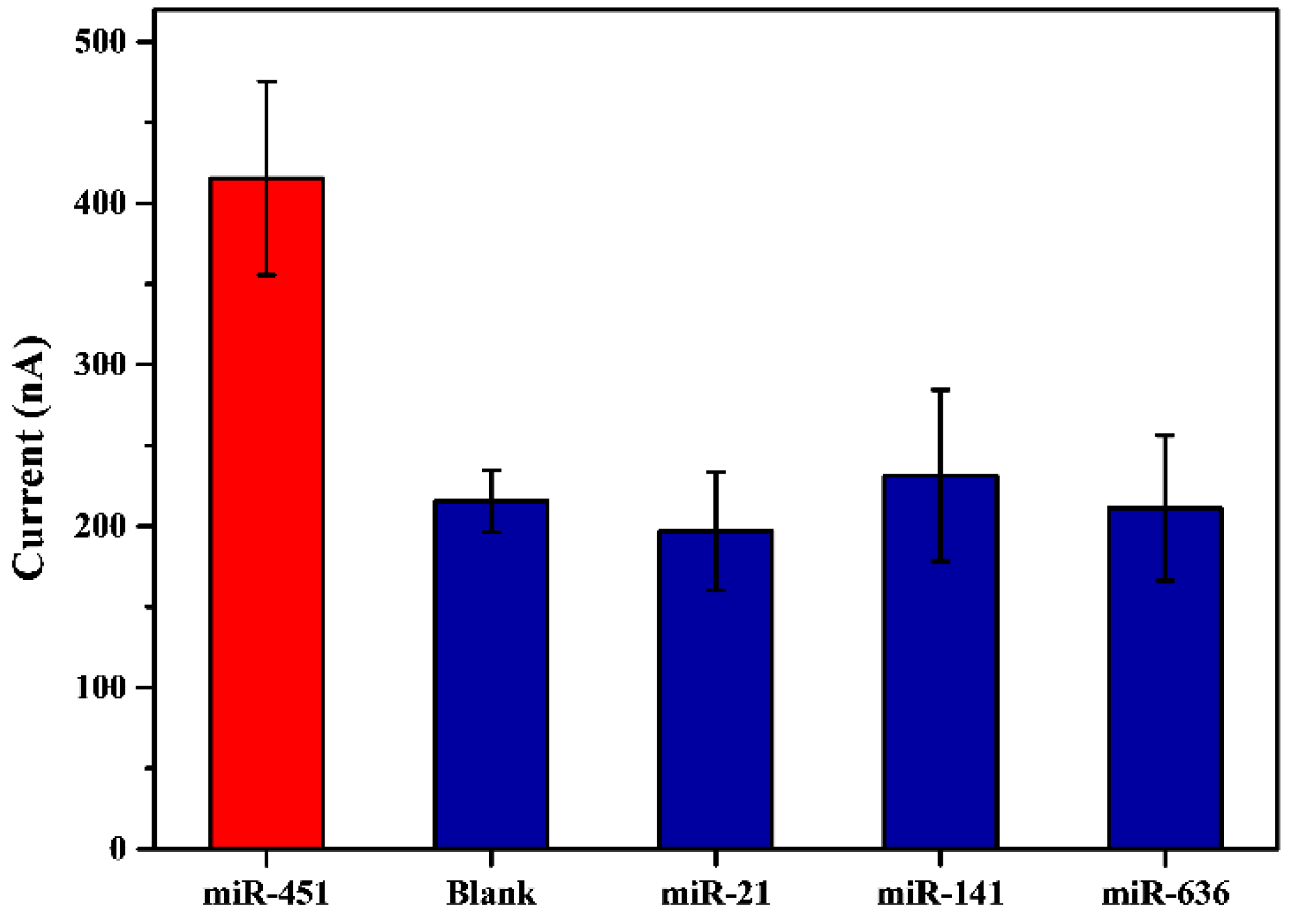
3.3. Characterization of Sensor Selectivity
3.4. Test for Concentration of Urinary ExomiRNAs by exomiR-biosensor
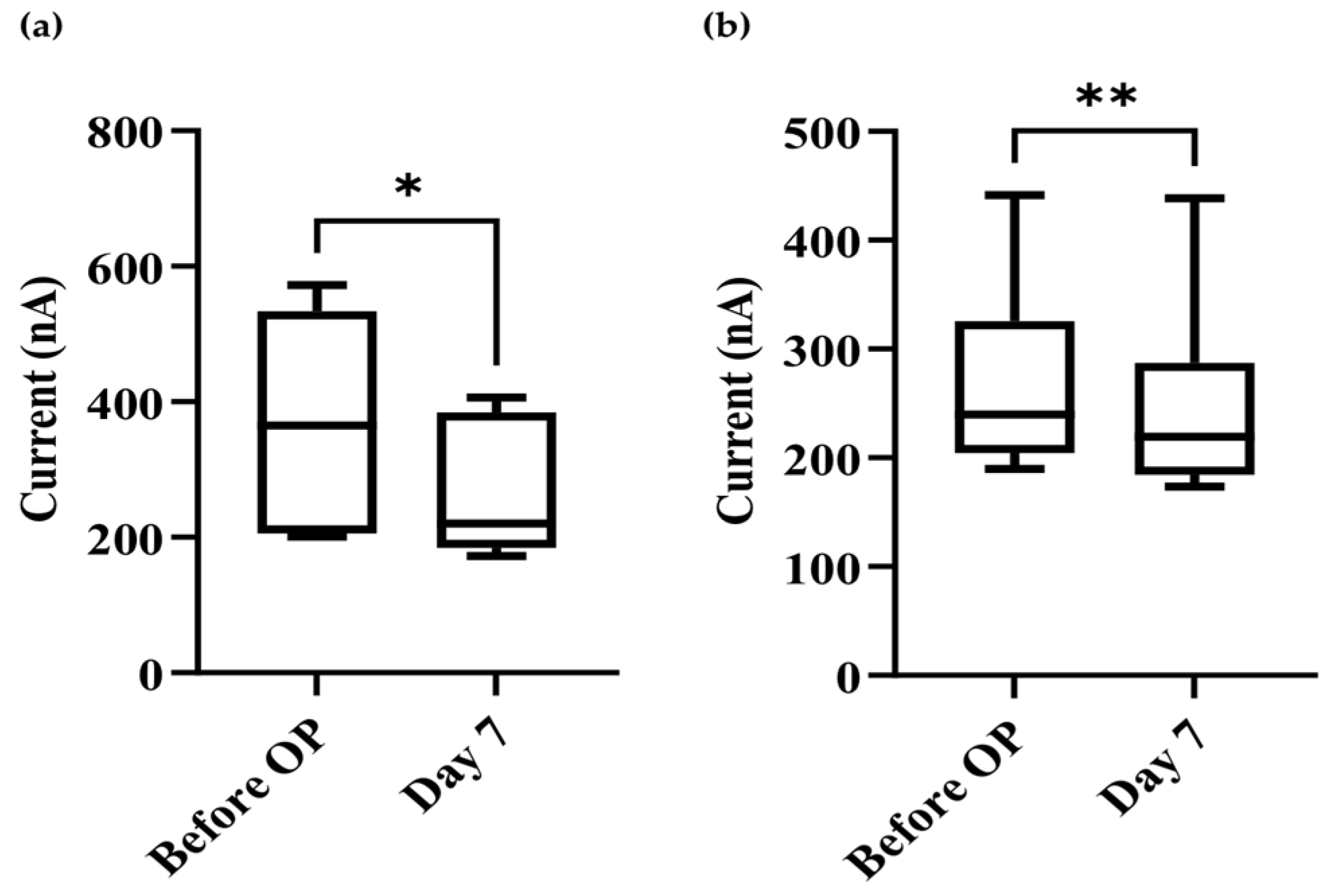
3.5. Comparison of Preoperative and Postoperative (7 Days) Levels of exomiR-21 and exomiR-451
3.6. Statistical Analysis of Correlation between Clinical Characteristics and exomiR-21 and exomiR-451 Expression in Urine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Van Poppel, H.; Hogenhout, R.; Albers, P.; van den Bergh, R.C.N.; Barentsz, J.O.; Roobol, M.J. Early Detection of Prostate Cancer in 2020 and Beyond: Facts and Recommendations for the European Union and the European Commission. Eur. Urol. 2021, 79, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Cush, J.J. Rheumatoid Arthritis: Early Diagnosis and Treatment. Rheum. Dis. Clin. North Am. 2022, 48, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Schatten, H. Brief Overview of Prostate Cancer Statistics, Grading, Diagnosis and Treatment Strategies. Adv. Exp. Med. Biol. 2018, 1095, 1–14. [Google Scholar] [CrossRef]
- Egevad, L.; Granfors, T.; Karlberg, L.; Bergh, A.; Stattin, P. Prognostic value of the Gleason score in prostate cancer. BJU Int. 2002, 89, 538–542. [Google Scholar] [CrossRef]
- Ilic, D.; Djulbegovic, M.; Jung, J.H.; Hwang, E.C.; Zhou, Q.; Cleves, A.; Agoritsas, T.; Dahm, P. Prostate cancer screening with prostate-specific antigen (PSA) test: A systematic review and meta-analysis. BMJ 2018, 362, k3519. [Google Scholar] [CrossRef] [Green Version]
- Djulbegovic, M.; Beyth, R.J.; Neuberger, M.M.; Stoffs, T.L.; Vieweg, J.; Djulbegovic, B.; Dahm, P. Screening for prostate cancer: Systematic review and meta-analysis of randomised controlled trials. BMJ 2010, 341, c4543. [Google Scholar] [CrossRef] [Green Version]
- Byrnes, C.A.; Morton, A.S.; Liss, C.L.; Lippert, M.C.; Gillenwater, J.Y. Efficacy, tolerability, and effect on health-related quality of life of finasteride versus placebo in men with symptomatic benign prostatic hyperplasia: A community-based study. Clin. Ther. 1995, 17, 956–969. [Google Scholar] [CrossRef]
- Oremek, G.M.; Seiffert, U.B. Physical activity releases prostate-specific antigen (PSA) from the prostate gland into blood and increases serum PSA concentrations. Clin. Chem. 1996, 42, 691–695. [Google Scholar] [CrossRef]
- Tchetgen, M.-B.; Song, J.T.; Strawderman, M.; Jacobsen, S.J.; Oesterling, J.E. Ejaculation increases the serum prostate-specific antigen concentration. Urology 1996, 47, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Collin, S.M.; Metcalfe, C.; Donovan, J.; Lane, J.A.; Davis, M.; Neal, D.; Hamdy, F.; Martin, R.M. Associations of lower urinary tract symptoms with prostate-specific antigen levels, and screen-detected localized and advanced prostate cancer: A case-control study nested within the UK population-based ProtecT (Prostate testing for cancer and Treatment) study. BJU Int. 2008, 102, 1400–1406. [Google Scholar] [CrossRef]
- Alimo-Metcalfe, B.; Alban-Metcalfe, J.; Bradley, M.; Mariathasan, J.; Samele, C. The impact of engaging leadership on performance, attitudes to work and wellbeing at work: A longitudinal study. J. Health Organ. Manag. 2008, 22, 586–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coker, T.J.; Dierfeldt, D.M. Acute Bacterial Prostatitis: Diagnosis and Management. Am. Fam. Physician 2016, 93, 114–120. [Google Scholar] [PubMed]
- Hakimian, F.; Ghourchian, H.; Hashemi, A.s.; Arastoo, M.R.; Behnam Rad, M. Ultrasensitive optical biosensor for detection of miRNA-155 using positively charged Au nanoparticles. Sci. Rep. 2018, 8, 2943. [Google Scholar] [CrossRef] [Green Version]
- Palchetti, I.; Mascini, M. Nucleic acid biosensors for environmental pollution monitoring. Analyst 2008, 133, 846–854. [Google Scholar] [CrossRef]
- Pang, S.N.; Lin, Y.L.; Yu, K.J.; Chiou, Y.E.; Leung, W.H.; Weng, W.H. An Effective SARS-CoV-2 Electrochemical Biosensor with Modifiable Dual Probes Using a Modified Screen-Printed Carbon Electrode. Micromachines 2021, 12, 1171. [Google Scholar] [CrossRef]
- Jayanthi, V.S.P.K.S.A.; Das, A.B.; Saxena, U. Recent advances in biosensor development for the detection of cancer biomarkers. Biosensors Bioelectron. 2017, 91, 15–23. [Google Scholar] [CrossRef]
- Catuogno, S.; Esposito, C.L.; Quintavalle, C.; Cerchia, L.; Condorelli, G.; De Franciscis, V. Recent Advance in Biosensors for microRNAs Detection in Cancer. Cancers 2011, 3, 1877–1898. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef]
- Shen, J.; Wang, A.; Wang, Q.; Gurvich, I.; Siegel, A.B.; Remotti, H.; Santella, R.M. Exploration of genome-wide circulating microRNA in hepatocellular carcinoma: MiR-483-5p as a potential biomarker. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 2364–2373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Dutta, A. MicroRNAs in cancer. Annu. Rev. Pathol. 2009, 4, 199–227. [Google Scholar] [CrossRef] [PubMed]
- Mall, C.; Rocke, D.M.; Durbin-Johnson, B.; Weiss, R.H. Stability of miRNA in human urine supports its biomarker potential. Biomark. Med. 2013, 7, 623–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O'Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieckowski, E.; Whiteside, T.L. Human tumor-derived vs dendritic cell-derived exosomes have distinct biologic roles and molecular profiles. Immunol. Res. 2006, 36, 247–254. [Google Scholar] [CrossRef]
- Lodes, M.J.; Caraballo, M.; Suciu, D.; Munro, S.; Kumar, A.; Anderson, B. Detection of cancer with serum miRNAs on an oligonucleotide microarray. PLoS ONE 2009, 4, e6229. [Google Scholar] [CrossRef]
- Pang, S.N.; Lin, Y.L.; Chiou, Y.E.; Leung, W.H.; Weng, W.H. Urinary MicroRNA Sensing Using Electrochemical Biosensor to Evaluate Colorectal Cancer Progression. Biomedicines 2022, 10, 1434. [Google Scholar] [CrossRef]
- Wen, Y.; Li, L.; Li, J.; Lin, M.; Liu, G.; Liang, W.; Xu, L.; Li, Y.; Zuo, X.; Ren, S.; et al. DNA Framework-Mediated Electrochemical Biosensing Platform for Amplification-Free MicroRNA Analysis. Anal. Chem. 2020, 92, 4498–4503. [Google Scholar] [CrossRef]
- Xu, J.; Zhao, J.; Zhang, R. Four microRNAs Signature for Survival Prognosis in Colon Cancer using TCGA Data. Sci. Rep. 2016, 6, 38306. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Park, Y.H.; Jung, S.H.; Jang, S.H.; Kim, M.Y.; Lee, J.Y.; Chung, Y.J. Urinary exosome microRNA signatures as a noninvasive prognostic biomarker for prostate cancer. NPJ Genom. Med. 2021, 6, 45. [Google Scholar] [CrossRef]
- Santhanam, M.; Algov, I.; Alfonta, L. DNA/RNA Electrochemical Biosensing Devices a Future Replacement of PCR Methods for a Fast Epidemic Containment. Sensors 2020, 20, 4648. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.-H.; Pang, C.-C.; Pang, S.-N.; Weng, S.-X.; Lin, Y.-L.; Chiou, Y.-E.; Pang, S.-T.; Weng, W.-H. High-Sensitivity Dual-Probe Detection of Urinary miR-141 in Cancer Patients via a Modified Screen-Printed Carbon Electrode-Based Electrochemical Biosensor. Sensors 2021, 21, 3183. [Google Scholar] [CrossRef] [PubMed]
- El Aamri, M.; Yammouri, G.; Mohammadi, H.; Amine, A.; Korri-Youssoufi, H. Electrochemical Biosensors for Detection of MicroRNA as a Cancer Biomarker: Pros and Cons. Biosensors 2020, 10, 186. [Google Scholar] [CrossRef] [PubMed]
- Yasui, T.; Yanagida, T.; Ito, S.; Konakade, Y.; Takeshita, D.; Naganawa, T.; Nagashima, K.; Shimada, T.; Kaji, N.; Nakamura, Y.; et al. Unveiling massive numbers of cancer-related urinary-microRNA candidates via nanowires. Sci. Adv. 2017, 3, e1701133. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Current Value | exomiR-451 | p-Value | exomiR-21 | p-Value | |||
|---|---|---|---|---|---|---|---|
| Clinical Characteristics | ≦220 nA | >220 nA | ≦220 nA | >220 nA | |||
| Case Number (n) | Case Number (n) | ||||||
| Disease type | |||||||
| Adenocarcinoma | (3) | (19) | 0.005 | (4) | (18) | 0.492 | |
| BPH | (2) | (1) | (1) | ||||
| Normal | (10) | (10) | |||||
| PSA | |||||||
| ≤4 | (12) | 0.001 | (1) | (11) | 0.504 | ||
| >4 | (3) | (19) | (4) | (18) | |||
| ≤10 | (13) | (4) | 0.037 | (2) | (6) | 0.525 | |
| >10 | (2) | (15) | (3) | (14) | |||
| Age | |||||||
| ≤63 | (12) | (7) | 0.455 | (3) | (16) | 0.301 | |
| ˃63 | (3) | (12) | (2) | (13) | |||
| miRNAs | exomiR-451 | exomiR-21 | Comparison of | ||||
|---|---|---|---|---|---|---|---|
| Current Variation | |||||||
| Tumor Status | Before OP. * | After OP. | Before OP. | After OP. | exomiR-451 | exomiR-21 | |
| pT stage | |||||||
| T2 (5) | 0.184 | 0.105 | 0.971 | 0.0525 | |||
| T3a (3) | |||||||
| T3b (2) | 0.591 | 0.566 | 0.016 | 0.907 | |||
| Lymphatic metastasis | |||||||
| Yes (3) | 0.218 | 0.158 | 0.15 | 0.504 | 0.789 | 0.042 | |
| No (7) | |||||||
| Tumor stage | |||||||
| Group 3, 4 (5) | 0.985 | 0.591 | 0.811 | 0.352 | |||
| Group 1, 2 (5) | 0.031 | 0.748 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiou, Y.-E.; Yu, K.-J.; Pang, S.-N.; Yang, Y.-L.; Pang, S.-T.; Weng, W.-H. A Highly Sensitive Urinary Exosomal miRNAs Biosensor Applied to Evaluation of Prostate Cancer Progression. Bioengineering 2022, 9, 803. https://doi.org/10.3390/bioengineering9120803
Chiou Y-E, Yu K-J, Pang S-N, Yang Y-L, Pang S-T, Weng W-H. A Highly Sensitive Urinary Exosomal miRNAs Biosensor Applied to Evaluation of Prostate Cancer Progression. Bioengineering. 2022; 9(12):803. https://doi.org/10.3390/bioengineering9120803
Chicago/Turabian StyleChiou, Yueh-Er, Kai-Jie Yu, Sow-Neng Pang, Yan-Lin Yang, See-Tong Pang, and Wen-Hui Weng. 2022. "A Highly Sensitive Urinary Exosomal miRNAs Biosensor Applied to Evaluation of Prostate Cancer Progression" Bioengineering 9, no. 12: 803. https://doi.org/10.3390/bioengineering9120803
APA StyleChiou, Y. -E., Yu, K. -J., Pang, S. -N., Yang, Y. -L., Pang, S. -T., & Weng, W. -H. (2022). A Highly Sensitive Urinary Exosomal miRNAs Biosensor Applied to Evaluation of Prostate Cancer Progression. Bioengineering, 9(12), 803. https://doi.org/10.3390/bioengineering9120803