
3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups

 ,
,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
- -
- impacted and supernumerary teeth;
- -
- bicuspid tooth implant needs;
- -
- obstructive sleep disorders breathing and apnea syndrome;
- -
- orthognathic surgery;
- -
- trauma not involving mandibular or maxillary position;
- -
- foreign objects.
- no cross-bite;
- full dentition;
- absence of orthodontic appliances;
- absence of known craniofacial syndromes in the clinical history of the patient.
2.2. Age and Sex Distribution
- pre-growth peak (CS1-CS2) and (I-III period);
- growth peak (CS3) and (IV period);
- post-growth peak (CS4-CS5-CS6) and (V-VI period).
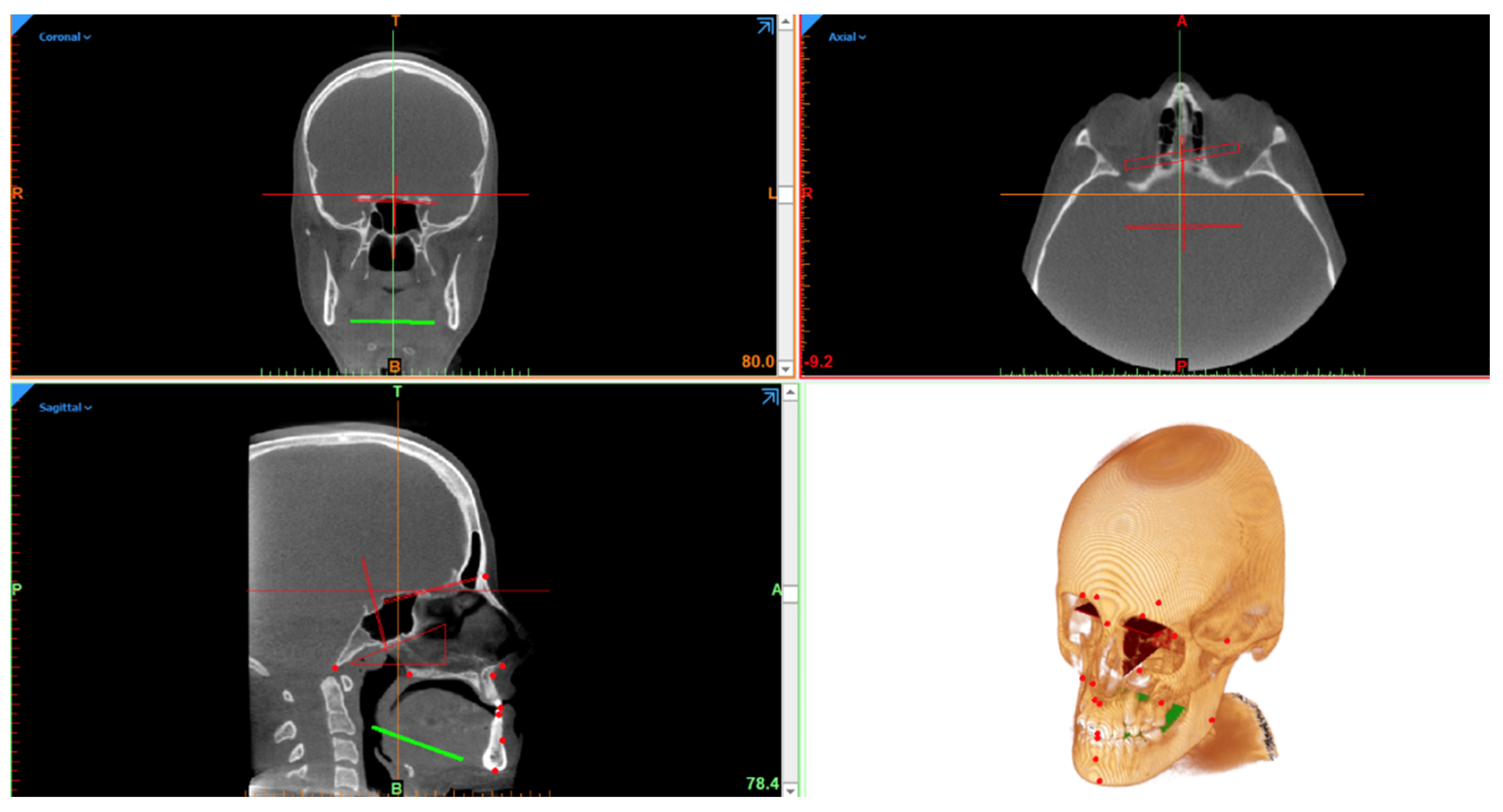
2.3. Scanning Protocol
2.4. Data Elaboration
2.5. 3D Cephalometrics
- Ten unpaired landmarks lying on the midsagittal plane:
- Four paired landmarks divided into right and left:
- Three Sagittal Angular Measurements:
- Seven Vertical Linear Measurements:
- Twelve Vertical Angular Measurements:
- Ten Transverse measurements:
2.6. Data Reliability
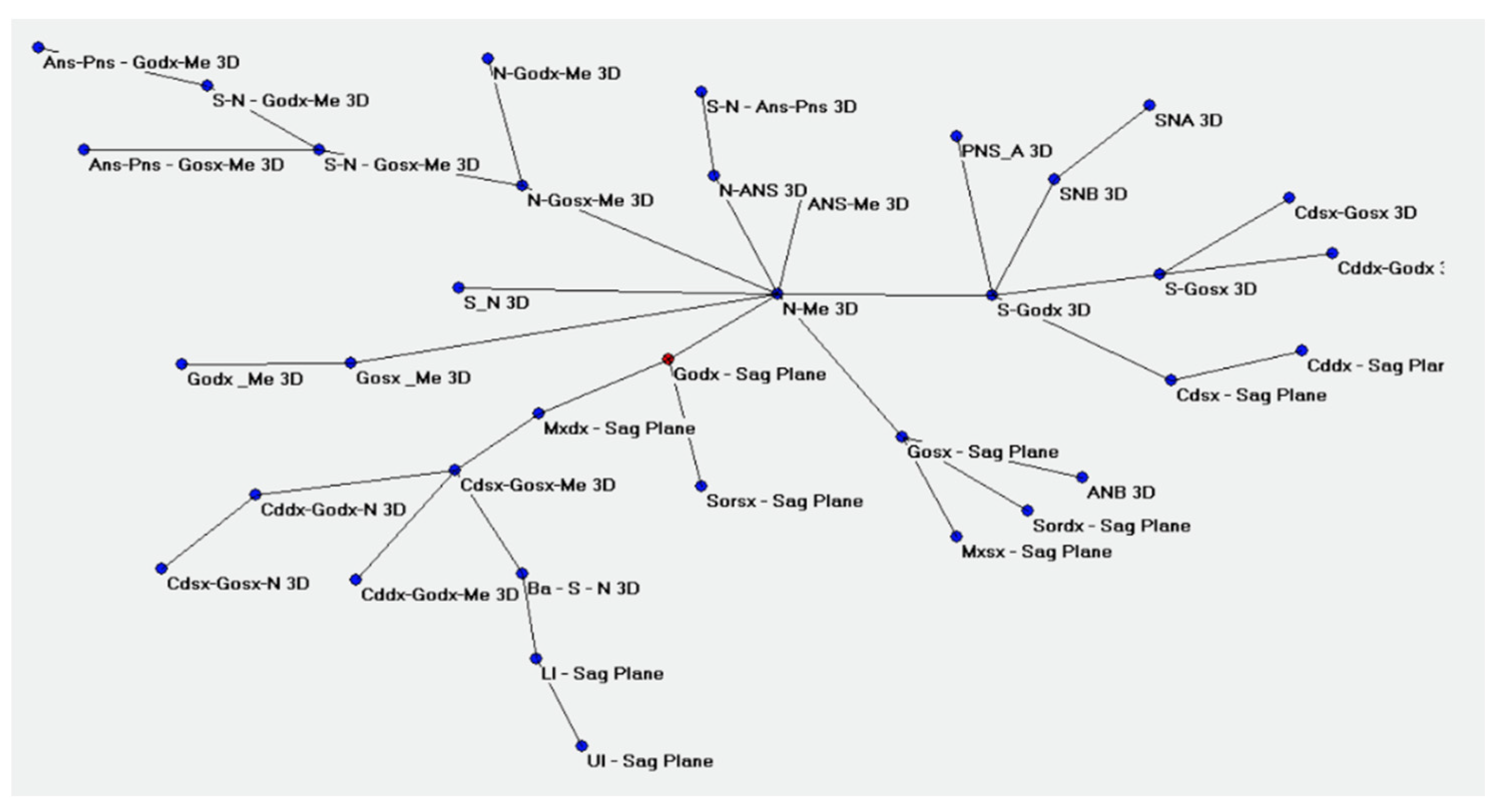
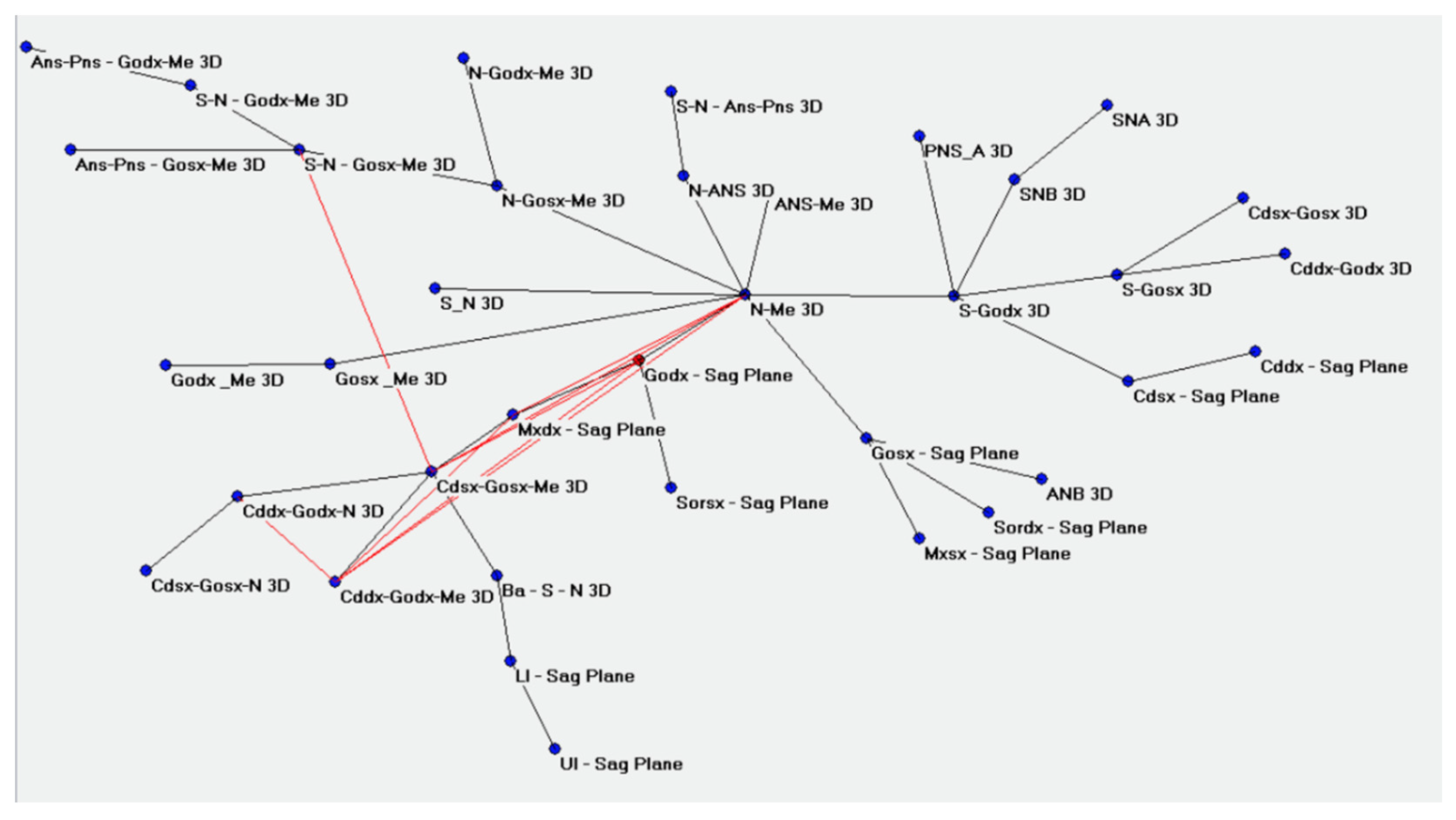
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh Rathore, A.; Dhar, V.; Arora, R.; Diwanji, A. Cephalometric Norms for Mewari Children using Steiner’s Analysis. Int. J. Clin. Pediatr. Dent. 2012, 5, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Oz, U.; Orhan, K.; Abe, N. Comparison of linear and angular measurements using two-dimensional conventional methods and three-dimensional cone beam CT images reconstructed from a volumetric rendering program in vivo. Dento Maxillo Facial Radiol. 2011, 40, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Dobai, A.; Vizkelety, T.; Markella, Z.; Rosta, A.; Kucsera, Á.; Barabás, J. Lower face cephalometry based on quadrilateral analysis with cone-beam computed tomography: A clinical pilot study. Oral Maxillofac. Surg. 2017, 21, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Gateno, J.; Xia, J.J.; Teichgraeber, J.F. New 3-dimensional cephalometric analysis for orthognathic surgery. J. Oral Maxillofac. Surg. 2011, 69, 606–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- d’Apuzzo, F.; Minervini, G.; Grassia, V.; Rotolo, R.P.; Perillo, L.; Nucci, L. Mandibular coronoid process hypertrophy: Diagnosis and 20-year follow-up with CBCT, MRI and EMG evaluations. Appl. Sci. 2021, 11, 4504. [Google Scholar] [CrossRef]
- Scarfe, W.C.; Farman, A.G.; Levin, M.D.; Gane, D. Essentials of maxillofacial cone beam computed tomography. Alpha Omegan 2010, 103, 62–67. [Google Scholar] [CrossRef]
- van Vlijmen, O.J.; Bergé, S.J.; Swennen, G.R.; Bronkhorst, E.M.; Katsaros, C.; Kuijpers-Jagtman, A.M. Comparison of cephalometric radiographs obtained from cone-beam computed tomography scans and conventional radiographs. J. Oral Maxillofac. Surg. 2009, 67, 92–97. [Google Scholar] [CrossRef]
- Venezia, P.; Nucci, L.; Moschitto, S.; Malgioglio, A.; Isola, G.; Ronsivalle, V.; Venticinque, V.; Leonardi, R.; Lagraverè, M.O.; Lo Giudice, A. Short-Term and Long-Term Changes of Nasal Soft Tissue after Rapid Maxillary Expansion (RME) with Tooth-Borne and Bone-Borne Devices. A CBCT Retrospective Study. Diagnostics 2022, 12, 875. [Google Scholar] [CrossRef]
- Ye, H.; Ye, J.; Wang, S.; Wang, Z.; Geng, J.; Wang, Y.; Liu, Y.; Sun, Y.; Zhou, Y. Comparison of the accuracy (trueness and precision) of virtual dentofacial patients digitized by three different methods based on 3D facial and dental images. J. Prosthet. Dent. 2022, in press. [CrossRef]
- Kim, S.H.; Kim, K.B.; Choo, H. New Frontier in Advanced Dentistry: CBCT, Intraoral Scanner, Sensors, and Artificial Intelligence in Dentistry. Sensors 2022, 22, 2942. [Google Scholar] [CrossRef]
- Buscema, M.; Grossi, E. The semantic connectivity map: An adapting self-organising knowledge discovery method in data bases. Experience in gastro-oesophageal reflux disease. Int. J. Data Min. Bioinform. 2008, 2, 362–404. [Google Scholar] [CrossRef] [PubMed]
- Buscema, M.; Grossi, E.; Snowdon, D.; Antuono, P. Auto-Contractive Maps: An artificial adaptive system for data mining. An application to Alzheimer disease. Curr. Alzheimer Res. 2008, 5, 481–498. [Google Scholar] [CrossRef] [PubMed]
- Khanagar, S.B.; Al-Ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, application, and performance of artificial intelligence in dentistry—A systematic review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef] [PubMed]
- Abdulghani, E.A.; Alhammadi, M.S.; Al-Sosowa, A.A.; Almashraqi, A.A.; Sharhan, H.M.; Al-Fakeh, H.; Cao, B. Three-dimensional assessment of the favorability of maxillary posterior teeth intrusion in different facial patterns limited by the vertical relationship with the maxillary sinus floor. Clin. Oral Investig. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Hwang, H.S.; Youn, I.S.; Lee, K.H.; Lim, H.J. Classification of facial asymmetry by cluster analysis. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 279.e1–279.e6. [Google Scholar] [CrossRef]
- Kavitha, L.; Karthik, K. Comparison of cephalometric norms of caucasians and non-caucasians: A forensic aid in ethnic determination. J. Forensic Dent. Sci. 2012, 4, 53–55. [Google Scholar] [PubMed]
- Cicchetti, D.V.; Sparrow, S.A. Developing criteria for establishing interrater reliability of specific items: Applications to assessment of adaptive behavior. Am. J. Ment. Defic. 1981, 86, 127–137. [Google Scholar]
- D’Ettorre, G.; Farronato, M.; Candida, E.; Quinzi, V.; Grippaudo, C. A comparison between stereophotogrammetry and smartphone structured light technology for three-dimensional face scanning. Angle Orthod. 2022, 92, 358–363. [Google Scholar] [CrossRef]
- Farronato, G.; Garagiola, U.; Dominici, A.; Periti, G.; de Nardi, S.; Carletti, V.; Farronato, D. “Ten-point” 3D cephalometric analysis using low-dosage cone beam computed tomography. Prog. Orthod. 2010, 11, 2–12. [Google Scholar] [CrossRef]
- Lou, L.; Lagravere, M.O.; Compton, S.; Major, P.W.; Flores-Mir, C. Accuracy of measurements and reliability of landmark identification with computed tomography (CT) techniques in the maxillofacial area: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 402–411. [Google Scholar] [CrossRef]
- Gu, M.; Savoldi, F.; Chan, E.; Tse, C.; Lau, M.; Wey, M.C.; Hägg, U.; Yang, Y. Changes in the upper airway, hyoid bone and craniofacial morphology between patients treated with headgear activator and Herbst appliance: A retrospective study on lateral cephalometry. Orthod. Craniofacial Res. 2021, 24, 360–369. [Google Scholar] [CrossRef]
- Savoldi, F.; Del Re, F.; Tonni, I.; Gu, M.; Dalessandri, D.; Visconti, L. Appropriateness of standard cephalometric norms for the assessment of dentofacial characteristics in patients with cleidocranial dysplasia. Dento Maxillo Facial Radiol. 2022, 51, 20210015. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D cephalometry on reduced FOV CBCT: Skeletal class assessment through AF-BF on Frankfurt plane-validity and reliability through comparison with 2D measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef] [PubMed]
- Kochel, J.; Meyer-Marcotty, P.; Strnad, F.; Kochel, M.; Stellzig-Eisenhauer, A. 3D soft tissue analysis—Part 1: Sagittal parameters. J. Orofac. Orthop. Fortschr. Kieferorthopadie 2010, 71, 40–52. [Google Scholar] [CrossRef] [PubMed]
- Gribel, B.F.; Gribel, M.N.; Frazäo, D.C.; McNamara, J.A., Jr.; Manzi, F.R. Accuracy and reliability of craniometric measurements on lateral cephalometry and 3D measurements on CBCT scans. Angle Orthod. 2011, 81, 26–35. [Google Scholar] [CrossRef]
- Lee, M.; Kanavakis, G.; Miner, R.M. Newly defined landmarks for a three-dimensionally based cephalometric analysis: A retrospective cone-beam computed tomography scan review. Angle Orthod. 2015, 85, 3–10. [Google Scholar] [CrossRef]
- Hariharan, A.; Diwakar, N.R.; Jayanthi, K.; Hema, H.M.; Deepukrishna, S.; Ghaste, S.R. The reliability of cephalometric measurements in oral and maxillofacial imaging: Cone beam computed tomography versus two-dimensional digital cephalograms. Indian J. Dent. Res. 2016, 27, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Ludlow, J.B.; Mol, A.; Cevidanes, L. Comparison of conventional and cone beam CT synthesized cephalograms. Dento Maxillo Facial Radiol. 2007, 36, 263–269. [Google Scholar] [CrossRef]
- Ponce-Garcia, C.; Ruellas, A.; Cevidanes, L.; Flores-Mir, C.; Carey, J.P.; Lagravere-Vich, M. Measurement error and reliability of three available 3D superimposition methods in growing patients. Head Face Med. 2020, 16, 1. [Google Scholar] [CrossRef]
- Lagravère, M.O.; Gordon, J.M.; Guedes, I.H.; Flores-Mir, C.; Carey, J.P.; Heo, G.; Major, P.W. Reliability of traditional cephalometric landmarks as seen in three-dimensional analysis in maxillary expansion treatments. Angle Orthod. 2009, 79, 1047–1056. [Google Scholar] [CrossRef]
- Alsino, H.I.; Hajeer, M.Y.; Alkhouri, I.; Murad, R. The Diagnostic Accuracy of Cone-Beam Computed Tomography (CBCT) Imaging in Detecting and Measuring Dehiscence and Fenestration in Patients with Class I Malocclusion: A Surgical-Exposure-Based Validation Study. Cureus 2022, 14, e22789. [Google Scholar] [CrossRef]
- Cattaneo, P.M.; Bloch, C.B.; Calmar, D.; Hjortshøj, M.; Melsen, B. Comparison between conventional and cone-beam computed tomography-generated cephalograms. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 798–802. [Google Scholar] [CrossRef]
- Moshiri, M.; Scarfe, W.C.; Hilgers, M.L.; Scheetz, J.P.; Silveira, A.M.; Farman, A.G. Accuracy of linear measurements from imaging plate and lateral cephalometric images derived from cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 550–560. [Google Scholar] [CrossRef]
- Maspero, C.; Abate, A.; Bellincioni, F.; Cavagnetto, D.; Lanteri, V.; Costa, A.; Farronato, M. Comparison of a tridimensional cephalometric analysis performed on 3T-MRI compared with CBCT: A pilot study in adults. Prog. Orthod. 2019, 20, 40. [Google Scholar] [CrossRef] [PubMed]
- Van Duijn, M.H.M. Software for social network analysis. Model Methods Soc. Netw. Anal. 2005, 28. [Google Scholar]
- Pettey, W.B.; Toth, D.J.; Redd, A.; Carter, M.E.; Samore, M.H.; Gundlapalli, A.V. Using network projections to explore co-incidence and context in large clinical datasets: Application to homelessness among U.S. Veterans. J. Biomed. Inform. 2016, 61, 203–213. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Intra-Rater of Each Observer | Overall | |||||
|---|---|---|---|---|---|---|
| N of Measurements | ICC | 95% CI | ||||
| LL | UL | p | ||||
| 3D | Rater 1 | 3 | 1.00 | 0.997 | 1.00 | <0.001 *** |
| Rater 2 | 3 | 1.00 | 0.997 | 1.00 | <0.001 *** | |
| Rater 3 | 3 | 1.00 | 0.998 | 1.00 | <0.001 *** | |
| 2D | Rater 1 | 3 | 1.00 | 0.998 | 1.00 | <0.001 *** |
| Rater 2 | 3 | 1.00 | 0.999 | 1.00 | <0.001 *** | |
| Rater 3 | 3 | 1.00 | 0.999 | 1.00 | <0.001 *** | |
| Variables | 3D Variables | 2D Variables | Comparison | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Orientation | Measurement | Units | Mean | SD | SEM | Lower | Upper | Mean | SD | SEM | Lower | Upper | p-Value | R Value |
| Antero-posterior | S—N | mm | 63.66 | 3.38 | 0.46 | 62.73 | 64.59 | 63.66 | 3.41 | 0.47 | 62.72 | 64.60 | 0.97 | 1.00 |
| PNS—A | mm | 42.71 | 3.07 | 0.42 | 41.86 | 43.55 | 42.69 | 3.07 | 0.42 | 41.85 | 43.54 | 0.00 *** | 1.00 | |
| GoL—Me | mm | 74.83 | 4.94 | 0.68 | 73.47 | 76.19 | 62.78 | 4.70 | 0.65 | 61.48 | 64.08 | 0.00 *** | 0.93 | |
| GoR—Me | mm | 75.00 | 4.71 | 0.65 | 73.71 | 76.30 | 62.84 | 4.97 | 0.68 | 61.47 | 64.21 | 0.00 *** | 0.91 | |
| Sagittal angular | SNA | deg | 80.35 | 2.86 | 0.39 | 79.56 | 81.14 | 80.35 | 2.86 | 0.39 | 79.56 | 81.14 | 0.79 | 1.00 |
| SNB | deg | 77.84 | 2.65 | 0.36 | 77.11 | 78.57 | 77.83 | 2.65 | 0.36 | 77.10 | 78.56 | 0.36 | 1.00 | |
| ANB | deg | 2.60 | 1.02 | 0.14 | 2.32 | 2.88 | 2.52 | 1.04 | 0.14 | 2.23 | 2.80 | 0.01 ** | 0.98 | |
| Vertical linear | N—Me | mm | 101.47 | 7.46 | 1.02 | 99.42 | 103.53 | 101.46 | 7.46 | 1.02 | 99.40 | 103.51 | 0.02 * | 1.00 |
| N—ANS | mm | 45.94 | 3.64 | 0.50 | 44.94 | 46.95 | 45.93 | 3.64 | 0.50 | 44.93 | 46.93 | 0.01 ** | 1.00 | |
| ANS—Me | mm | 56.72 | 5.18 | 0.71 | 55.29 | 58.14 | 56.70 | 5.18 | 0.71 | 55.27 | 58.13 | 0.00 *** | 1.00 | |
| CdL—GoL | mm | 55.77 | 3.94 | 0.54 | 54.68 | 56.86 | 49.14 | 4.24 | 0.58 | 47.98 | 50.31 | 0.00 *** | 0.89 | |
| CdR—GoR | mm | 55.87 | 3.96 | 0.54 | 54.78 | 56.96 | 49.59 | 4.36 | 0.60 | 48.39 | 50.79 | 0.00 *** | 0.94 | |
| S—GoL | mm | 75.10 | 5.92 | 0.81 | 73.47 | 76.73 | 63.26 | 5.62 | 0.77 | 61.71 | 64.81 | 0.00 *** | 0.97 | |
| S—GoR | mm | 75.23 | 5.50 | 0.76 | 73.72 | 76.75 | 63.13 | 5.57 | 0.77 | 61.59 | 64.66 | 0.00 *** | 0.96 | |
| Vertical angular | Ba—S—N | deg | 130.13 | 4.94 | 0.68 | 128.77 | 131.49 | 130.16 | 4.95 | 0.68 | 128.79 | 131.52 | 0.00 *** | 1.00 |
| S-N—ANS-PNS | deg | 7.94 | 2.84 | 0.39 | 7.16 | 8.73 | 7.83 | 2.87 | 0.39 | 7.04 | 8.62 | 0.00 *** | 1.00 | |
| S-N—GoL-Me | deg | 46.90 | 3.53 | 0.49 | 45.92 | 47.87 | 35.37 | 4.21 | 0.58 | 34.21 | 36.53 | 0.00 *** | 0.92 | |
| S-N—GoR-Me | deg | 46.84 | 3.81 | 0.52 | 45.79 | 47.88 | 35.53 | 4.27 | 0.59 | 34.35 | 36.70 | 0.00 *** | 0.90 | |
| CdL—GoL—Me | deg | 120.85 | 4.77 | 0.66 | 119.53 | 122.16 | 123.18 | 5.99 | 0.82 | 121.53 | 124.83 | 0.00 *** | 0.91 | |
| CdR—GoR—Me | deg | 120.66 | 5.00 | 0.69 | 119.28 | 122.04 | 123.76 | 6.62 | 0.91 | 121.93 | 125.58 | 0.00 *** | 0.94 | |
| CdL—GoL—N | deg | 46.19 | 4.58 | 0.63 | 44.93 | 47.46 | 45.88 | 4.68 | 0.64 | 44.59 | 47.17 | 0.00 *** | 1.00 | |
| CdR—GoR—N | deg | 46.46 | 4.72 | 0.65 | 45.16 | 47.76 | 46.22 | 4.72 | 0.65 | 44.92 | 47.53 | 0.00 *** | 1.00 | |
| N—GoL—Me | deg | 65.20 | 3.74 | 0.51 | 64.17 | 66.23 | 74.04 | 5.15 | 0.71 | 72.62 | 75.46 | 0.00 *** | 0.98 | |
| N—GoR—Me | deg | 65.07 | 3.72 | 0.51 | 64.04 | 66.10 | 74.16 | 5.15 | 0.71 | 72.74 | 75.58 | 0.00 *** | 0.96 | |
| ANS-PNS—GoL-Me | deg | 27.54 | 4.49 | 0.62 | 41.23 | 43.11 | 42.17 | 3.42 | 0.47 | 26.30 | 28.77 | 0.00 *** | 0.84 | |
| ANS-PNS—GoR-Me | deg | 41.89 | 3.61 | 0.50 | 40.90 | 42.89 | 27.69 | 4.44 | 0.61 | 26.47 | 28.92 | 0.00 *** | 0.86 | |
| Transverse | SorL—Sag Plane | mm | 23.31 | 3.17 | 0.44 | 22.44 | 24.18 | 23.31 | 3.17 | 0.44 | 22.44 | 24.18 | N/A | N/A |
| SorR—Sag Plane | mm | 23.35 | 2.82 | 0.39 | 22.58 | 24.13 | 23.35 | 2.82 | 0.39 | 22.58 | 24.13 | N/A | N/A | |
| MxL—Sag Plane | mm | 28.24 | 2.14 | 0.29 | 27.65 | 28.83 | 28.24 | 2.14 | 0.29 | 27.65 | 28.83 | N/A | N/A | |
| MxR—Sag Plane | mm | 28.25 | 3.19 | 0.44 | 27.37 | 29.13 | 28.25 | 3.19 | 0.44 | 27.37 | 29.13 | N/A | N/A | |
| CdL—Sag Plane | mm | 45.15 | 2.92 | 0.40 | 44.34 | 45.95 | 45.15 | 2.92 | 0.40 | 44.34 | 45.95 | N/A | N/A | |
| CdR—Sag Plane | mm | 44.81 | 2.91 | 0.40 | 44.01 | 45.62 | 44.81 | 2.91 | 0.40 | 44.01 | 45.62 | N/A | N/A | |
| GoL—Sag Plane | mm | 40.69 | 3.48 | 0.48 | 39.73 | 41.65 | 40.69 | 3.48 | 0.48 | 39.73 | 41.65 | N/A | N/A | |
| GoR—Sag Plane | mm | 40.44 | 3.76 | 0.52 | 39.40 | 41.47 | 40.44 | 3.76 | 0.52 | 39.40 | 41.47 | N/A | N/A | |
| UI—Sag Plane | mm | 2.37 | 2.06 | 0.28 | 1.80 | 2.94 | 2.37 | 2.06 | 0.28 | 1.80 | 2.94 | N/A | N/A | |
| LI—Sag Plane | mm | 2.49 | 2.23 | 0.31 | 1.87 | 3.10 | 2.49 | 2.23 | 0.31 | 1.87 | 3.10 | N/A | N/A | |
| Variables | 3D Variables | 2D Variables | Comparison | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Orientation | Measurement | Units | Mean | SD | SEM | Lower | Upper | Mean | SD | SEM | Lower | Upper | p-Value | R Value |
| Antero-posterior | S—N | mm | 64.87 | 3.54 | 0.58 | 63.69 | 66.05 | 64.89 | 3.62 | 0.60 | 63.69 | 66.10 | 0.58 | 1.00 |
| PNS—A | mm | 44.29 | 3.18 | 0.52 | 43.23 | 45.35 | 44.27 | 3.19 | 0.52 | 43.21 | 45.33 | 0.00 *** | 1.00 | |
| GoL—Me | mm | 76.96 | 5.54 | 0.91 | 75.12 | 78.81 | 65.35 | 5.44 | 0.89 | 63.54 | 67.17 | 0.00 *** | 0.96 | |
| GoR—Me | mm | 77.58 | 5.16 | 0.85 | 75.86 | 79.30 | 64.84 | 5.54 | 0.91 | 62.99 | 66.69 | 0.00 *** | 0.96 | |
| Sagittal angular | SNA | deg | 80.84 | 4.12 | 0.68 | 79.47 | 82.22 | 78.41 | 3.82 | 0.63 | 77.14 | 79.69 | 1.00 | 1.00 |
| SNB | deg | 80.84 | 4.13 | 0.68 | 79.47 | 82.22 | 78.42 | 3.82 | 0.63 | 77.14 | 79.69 | 0.58 | 1.00 | |
| ANB | deg | 2.58 | 1.23 | 0.20 | 2.18 | 2.99 | 2.49 | 1.21 | 0.20 | 2.09 | 2.90 | 0.00 *** | 0.99 | |
| Vertical linear | N—Me | mm | 106.27 | 7.45 | 1.23 | 103.79 | 108.76 | 106.25 | 7.45 | 1.22 | 103.76 | 108.73 | 0.01 ** | 1.00 |
| N—ANS | mm | 48.56 | 3.65 | 0.60 | 47.34 | 49.77 | 48.54 | 3.65 | 0.60 | 47.32 | 49.76 | 0.01 ** | 1.00 | |
| ANS—Me | mm | 58.83 | 4.95 | 0.81 | 57.18 | 60.48 | 58.80 | 4.93 | 0.81 | 57.16 | 60.45 | 0.00 *** | 1.00 | |
| CdL—GoL | mm | 52.15 | 12.84 | 2.11 | 47.86 | 56.43 | 50.21 | 5.64 | 0.93 | 48.33 | 52.09 | 0.23 | 0.72 | |
| CdR—GoR | mm | 51.80 | 11.92 | 1.96 | 47.82 | 55.77 | 50.19 | 5.78 | 0.95 | 48.26 | 52.12 | 0.22 | 0.83 | |
| S—GoL | mm | 79.84 | 6.30 | 1.04 | 77.74 | 81.94 | 67.98 | 6.47 | 1.06 | 65.82 | 70.13 | 0.00 *** | 0.98 | |
| S—GoR | mm | 79.74 | 6.11 | 1.01 | 77.70 | 81.78 | 68.15 | 6.60 | 1.08 | 65.95 | 70.34 | 0.00 *** | 0.97 | |
| Vertical angular | Ba—S—N | deg | 129.62 | 6.07 | 1.00 | 127.59 | 131.64 | 129.65 | 6.08 | 1.00 | 127.62 | 131.67 | 0.01 ** | 1.00 |
| S-N—ANS-PNS | deg | 8.59 | 3.57 | 0.59 | 7.40 | 9.79 | 8.45 | 3.67 | 0.60 | 7.23 | 9.68 | 0.00 *** | 1.00 | |
| S-N—GoL-Me | deg | 46.06 | 3.72 | 0.61 | 44.82 | 47.30 | 34.36 | 5.09 | 0.84 | 32.67 | 36.06 | 0.00 *** | 0.92 | |
| S-N—GoR-Me | deg | 46.11 | 4.28 | 0.70 | 44.68 | 47.54 | 34.43 | 5.68 | 0.93 | 32.54 | 36.32 | 0.00 *** | 0.93 | |
| CdL—GoL—Me | deg | 119.48 | 9.51 | 1.56 | 116.31 | 122.65 | 122.45 | 6.43 | 1.06 | 120.30 | 124.59 | 0.01 ** | 0.72 | |
| CdR—GoR—Me | deg | 119.47 | 8.93 | 1.47 | 116.49 | 122.45 | 122.91 | 6.53 | 1.07 | 120.73 | 125.09 | 0.00 *** | 0.80 | |
| CdL—GoL—N | deg | 54.62 | 3.95 | 0.65 | 53.30 | 55.94 | 47.99 | 3.85 | 0.63 | 46.71 | 49.27 | 0.00 *** | 0.93 | |
| CdR—GoR—N | deg | 54.82 | 3.38 | 0.56 | 53.69 | 55.95 | 48.09 | 3.61 | 0.59 | 46.88 | 49.29 | 0.00 *** | 0.89 | |
| N—GoL—Me | deg | 66.24 | 4.70 | 0.77 | 64.67 | 67.80 | 74.46 | 4.98 | 0.82 | 72.80 | 76.11 | 0.00 *** | 0.92 | |
| N—GoR—Me | deg | 65.75 | 4.22 | 0.69 | 64.34 | 67.16 | 74.82 | 5.47 | 0.90 | 72.99 | 76.64 | 0.00 *** | 0.97 | |
| ANS-PNS—GoL-Me | deg | 40.87 | 2.76 | 0.45 | 39.95 | 41.79 | 25.93 | 4.07 | 0.67 | 24.57 | 27.29 | 0.00 *** | 0.79 | |
| ANS-PNS—GoR-Me | deg | 40.94 | 2.91 | 0.48 | 39.97 | 41.91 | 26.00 | 4.44 | 0.73 | 24.52 | 27.48 | 0.01 ** | 0.71 | |
| Transverse | SorL—Sag Plane | mm | 24.17 | 2.74 | 0.45 | 23.26 | 25.08 | 24.17 | 2.74 | 0.45 | 23.26 | 25.08 | N/A | N/A |
| SorR—Sag Plane | mm | 24.66 | 3.35 | 0.55 | 23.54 | 25.77 | 24.66 | 3.35 | 0.55 | 23.54 | 25.77 | N/A | N/A | |
| MxL—Sag Plane | mm | 29.34 | 2.53 | 0.42 | 28.50 | 30.19 | 29.34 | 2.53 | 0.42 | 28.50 | 30.19 | N/A | N/A | |
| MxR—Sag Plane | mm | 29.74 | 3.55 | 0.58 | 28.56 | 30.93 | 29.74 | 3.55 | 0.58 | 28.56 | 30.93 | N/A | N/A | |
| CdL—Sag Plane | mm | 46.97 | 2.48 | 0.41 | 46.14 | 47.80 | 46.97 | 2.48 | 0.41 | 46.14 | 47.80 | N/A | N/A | |
| CdR—Sag Plane | mm | 46.45 | 2.72 | 0.45 | 45.55 | 47.36 | 46.45 | 2.72 | 0.45 | 45.55 | 47.36 | N/A | N/A | |
| GoL—Sag Plane | mm | 41.02 | 2.97 | 0.49 | 40.03 | 42.01 | 41.02 | 2.97 | 0.49 | 40.03 | 42.01 | N/A | N/A | |
| GoR—Sag Plane | mm | 41.81 | 2.78 | 0.46 | 40.88 | 42.74 | 41.81 | 2.78 | 0.46 | 40.88 | 42.74 | N/A | N/A | |
| UI—Sag Plane | mm | 2.54 | 1.82 | 0.30 | 1.94 | 3.15 | 2.54 | 1.82 | 0.30 | 1.94 | 3.15 | N/A | N/A | |
| LI—Sag Plane | mm | 2.47 | 1.64 | 0.27 | 1.93 | 3.02 | 2.47 | 1.64 | 0.27 | 1.93 | 3.02 | N/A | N/A | |
| Variables | 3D Variables | 2D Variables | Comparison | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Orientation | Measurement | Units | Mean | SD | SEM | Lower | Upper | Mean | SD | SEM | Lower | Upper | p-Value | R Value |
| Antero-posterior | S—N | mm | 66.92 | 4.74 | 0.95 | 64.97 | 68.88 | 67.00 | 4.86 | 0.97 | 64.99 | 69.01 | 0.17 | 1.00 |
| PNS—A | mm | 45.98 | 3.28 | 0.66 | 44.62 | 47.33 | 45.97 | 3.28 | 0.66 | 44.62 | 47.33 | 0.00 *** | 1.00 | |
| GoL—Me | mm | 81.81 | 4.24 | 0.85 | 80.06 | 83.56 | 69.32 | 4.50 | 0.90 | 67.46 | 71.18 | 0.00 *** | 0.91 | |
| GoR—Me | mm | 82.48 | 4.86 | 0.97 | 80.47 | 84.49 | 69.25 | 5.44 | 1.09 | 67.00 | 71.49 | 0.00 *** | 0.94 | |
| Sagittal angular | SNA | deg | 80.20 | 2.77 | 0.55 | 79.06 | 81.34 | 80.20 | 2.77 | 0.55 | 79.06 | 81.35 | 0.55 | 1.00 |
| SNB | deg | 78.40 | 2.90 | 0.58 | 77.20 | 79.60 | 78.40 | 2.90 | 0.58 | 77.20 | 79.60 | 0.41 | 1.00 | |
| ANB | deg | 2.30 | 0.88 | 0.18 | 1.94 | 2.66 | 2.03 | 0.93 | 0.19 | 1.65 | 2.41 | 0.02 * | 0.83 | |
| Vertical linear | N—Me | mm | 114.27 | 7.40 | 1.48 | 111.22 | 117.33 | 114.25 | 7.39 | 1.48 | 111.20 | 117.30 | 0.00 *** | 1.00 |
| N—ANS | mm | 51.59 | 2.99 | 0.60 | 50.36 | 52.83 | 51.58 | 2.99 | 0.60 | 50.34 | 52.81 | 0.00 *** | 1.00 | |
| ANS—Me | mm | 63.61 | 5.45 | 1.09 | 61.36 | 65.85 | 63.57 | 5.44 | 1.09 | 61.33 | 65.81 | 0.01 ** | 1.00 | |
| CdL—GoL | mm | 55.05 | 7.33 | 1.47 | 52.03 | 58.08 | 54.86 | 7.34 | 1.47 | 51.83 | 57.89 | 0.83 | 0.94 | |
| CdR—GoR | mm | 55.16 | 6.99 | 1.40 | 52.28 | 58.05 | 54.99 | 6.98 | 1.40 | 52.12 | 57.87 | 0.00 *** | 0.87 | |
| S—GoL | mm | 85.16 | 9.04 | 1.81 | 81.43 | 88.89 | 72.84 | 9.54 | 1.91 | 68.90 | 76.78 | 0.00 *** | 0.98 | |
| S—GoR | mm | 85.44 | 8.25 | 1.65 | 82.03 | 88.84 | 73.13 | 8.91 | 1.78 | 69.45 | 76.80 | 0.00 *** | 0.99 | |
| Vertical angular | Ba—S—N | deg | 129.70 | 6.18 | 1.24 | 127.15 | 132.25 | 129.71 | 6.18 | 1.24 | 127.15 | 132.26 | 0.21 | 1.00 |
| S-N—ANS-PNS | deg | 8.61 | 3.02 | 0.60 | 7.36 | 9.85 | 8.53 | 3.08 | 0.62 | 7.26 | 9.81 | 0.02 * | 1.00 | |
| S-N—GoL-Me | deg | 46.78 | 4.25 | 0.85 | 45.02 | 48.53 | 35.64 | 6.09 | 1.22 | 33.13 | 38.16 | 0.00 *** | 0.93 | |
| S-N—GoR-Me | deg | 46.91 | 4.53 | 0.91 | 45.04 | 48.78 | 35.55 | 5.93 | 1.19 | 33.11 | 38.00 | 0.00 *** | 0.93 | |
| CdL—GoL—Me | deg | 118.84 | 4.74 | 0.95 | 116.88 | 120.79 | 122.29 | 6.08 | 1.22 | 119.78 | 124.80 | 0.00 *** | 0.91 | |
| CdR—GoR—Me | deg | 118.22 | 5.21 | 1.04 | 116.07 | 120.37 | 122.18 | 7.09 | 1.42 | 119.25 | 125.10 | 0.00 *** | 0.93 | |
| CdL—GoL—N | deg | 51.72 | 4.45 | 0.89 | 49.88 | 53.55 | 45.98 | 4.77 | 0.95 | 44.02 | 47.95 | 0.00 *** | 0.93 | |
| CdR—GoR—N | deg | 51.56 | 4.04 | 0.81 | 49.89 | 53.23 | 45.86 | 4.60 | 0.92 | 43.96 | 47.76 | 0.00 *** | 0.93 | |
| N—GoL—Me | deg | 67.35 | 3.75 | 0.75 | 65.80 | 68.89 | 76.30 | 4.85 | 0.97 | 74.30 | 78.31 | 0.00 *** | 0.96 | |
| N—GoR—Me | deg | 67.06 | 4.18 | 0.84 | 65.34 | 68.79 | 76.32 | 5.66 | 1.13 | 73.98 | 78.66 | 0.00 *** | 0.97 | |
| ANS-PNS—GoL-Me | deg | 41.60 | 3.44 | 0.69 | 40.18 | 43.02 | 27.18 | 5.81 | 1.16 | 24.79 | 29.58 | 0.00 *** | 0.83 | |
| ANS-PNS—GoR-Me | deg | 41.54 | 4.40 | 0.88 | 39.73 | 43.36 | 27.09 | 5.64 | 1.13 | 24.76 | 29.42 | 0.00 *** | 0.87 | |
| Transverse | SorL—Sag Plane | mm | 24.93 | 3.36 | 0.67 | 23.54 | 26.32 | 24.93 | 3.36 | 0.67 | 23.54 | 26.32 | N/A | N/A |
| SorR—Sag Plane | mm | 25.71 | 4.07 | 0.81 | 24.03 | 27.38 | 25.71 | 4.07 | 0.81 | 24.03 | 27.38 | N/A | N/A | |
| MxL—Sag Plane | mm | 29.32 | 2.50 | 0.50 | 28.29 | 30.35 | 29.32 | 2.50 | 0.50 | 28.29 | 30.35 | N/A | N/A | |
| MxR—Sag Plane | mm | 28.94 | 3.20 | 0.64 | 27.62 | 30.26 | 28.94 | 3.20 | 0.64 | 27.62 | 30.26 | N/A | N/A | |
| CdL—Sag Plane | mm | 47.28 | 2.98 | 0.60 | 46.05 | 48.51 | 47.28 | 2.98 | 0.60 | 46.05 | 48.51 | N/A | N/A | |
| CdR—Sag Plane | mm | 47.09 | 2.59 | 0.52 | 46.02 | 48.16 | 47.09 | 2.59 | 0.52 | 46.02 | 48.16 | N/A | N/A | |
| GoL—Sag Plane | mm | 44.10 | 3.53 | 0.71 | 42.64 | 45.55 | 44.10 | 3.53 | 0.71 | 42.64 | 45.55 | N/A | N/A | |
| GoR—Sag Plane | mm | 43.77 | 3.21 | 0.64 | 42.44 | 45.09 | 43.77 | 3.21 | 0.64 | 42.44 | 45.09 | N/A | N/A | |
| UI—Sag Plane | mm | 1.69 | 1.66 | 0.33 | 1.01 | 2.38 | 1.69 | 1.66 | 0.33 | 1.01 | 2.38 | N/A | N/A | |
| LI—Sag Plane | mm | 1.94 | 1.86 | 0.37 | 1.17 | 2.71 | 1.94 | 1.86 | 0.37 | 1.17 | 2.71 | N/A | N/A | |
| Variables | Pre-Peak | Peak | Post-Peak | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Orientation | Measurement | Units | Normality | Normality | Normality | ||||||
| Antero-posterior | S—N | mm | 63.66 | ± | 3.38 | 64.87 | ± | 3.54 | 66.92 | ± | 4.74 |
| PNS—A | mm | 42.71 | ± | 3.07 | 44.29 | ± | 3.18 | 45.98 | ± | 3.28 | |
| GoL—Me | mm | 74.83 | ± | 4.94 | 76.96 | ± | 5.54 | 81.81 | ± | 4.24 | |
| GoR—Me | mm | 75.00 | ± | 4.71 | 77.58 | ± | 5.16 | 82.48 | ± | 4.86 | |
| Sagittal angular | SNA | deg | 80.35 | ± | 2.86 | 80.84 | ± | 4.12 | 80.20 | ± | 2.77 |
| SNB | deg | 77.84 | ± | 2.65 | 80.84 | ± | 4.13 | 78.40 | ± | 2.90 | |
| ANB | deg | 2.60 | ± | 1.02 | 2.58 | ± | 1.23 | 2.30 | ± | 0.88 | |
| Vertical linear | N—Me | mm | 101.47 | ± | 7.46 | 106.27 | ± | 7.45 | 114.27 | ± | 7.40 |
| N—ANS | mm | 45.94 | ± | 3.64 | 48.56 | ± | 3.65 | 51.59 | ± | 2.99 | |
| ANS—Me | mm | 56.72 | ± | 5.18 | 58.83 | ± | 4.95 | 63.61 | ± | 5.45 | |
| CdL—GoL | mm | 55.77 | ± | 3.94 | 52.15 | ± | 12.84 | 55.05 | ± | 7.33 | |
| CdR—GoR | mm | 55.87 | ± | 3.96 | 51.80 | ± | 11.92 | 55.16 | ± | 6.99 | |
| S—GoL | mm | 75.10 | ± | 5.92 | 79.84 | ± | 6.30 | 85.16 | ± | 9.04 | |
| S—GoR | mm | 75.23 | ± | 5.50 | 79.74 | ± | 6.11 | 85.44 | ± | 8.25 | |
| Vertical angular | Ba—S—N | deg | 130.13 | ± | 4.94 | 129.62 | ± | 6.07 | 129.70 | ± | 6.18 |
| S-N—ANS-PNS | deg | 7.94 | ± | 2.84 | 8.59 | ± | 3.57 | 8.61 | ± | 3.02 | |
| S-N—GoL-Me | deg | 46.90 | ± | 3.53 | 46.06 | ± | 3.72 | 46.78 | ± | 4.25 | |
| S-N—GoR-Me | deg | 46.84 | ± | 3.81 | 46.11 | ± | 4.28 | 46.91 | ± | 4.53 | |
| CdL—GoL—Me | deg | 120.85 | ± | 4.77 | 119.48 | ± | 9.51 | 118.84 | ± | 4.74 | |
| CdR—GoR—Me | deg | 120.66 | ± | 5.00 | 119.47 | ± | 8.93 | 118.22 | ± | 5.21 | |
| CdL—GoL—N | deg | 46.19 | ± | 4.58 | 54.62 | ± | 3.95 | 51.72 | ± | 4.45 | |
| CdR—GoR—N | deg | 46.46 | ± | 4.72 | 54.82 | ± | 3.38 | 51.56 | ± | 4.04 | |
| N—GoL—Me | deg | 65.20 | ± | 3.74 | 66.24 | ± | 4.70 | 67.35 | ± | 3.75 | |
| N—GoR—Me | deg | 65.07 | ± | 3.72 | 65.75 | ± | 4.22 | 67.06 | ± | 4.18 | |
| ANS-PNS—GoL-Me | deg | 27.54 | ± | 4.49 | 40.87 | ± | 2.76 | 41.60 | ± | 3.44 | |
| ANS-PNS—GoR-Me | deg | 41.89 | ± | 3.61 | 40.94 | ± | 2.91 | 41.54 | ± | 4.40 | |
| Transverse | SorL—Sag Plane | mm | 23.31 | ± | 3.17 | 24.17 | ± | 2.74 | 24.93 | ± | 3.36 |
| SorR—Sag Plane | mm | 23.35 | ± | 2.82 | 24.66 | ± | 3.35 | 25.71 | ± | 4.07 | |
| MxL—Sag Plane | mm | 28.24 | ± | 2.14 | 29.34 | ± | 2.53 | 29.32 | ± | 2.50 | |
| MxR—Sag Plane | mm | 28.25 | ± | 3.19 | 29.74 | ± | 3.55 | 28.94 | ± | 3.20 | |
| CdL—Sag Plane | mm | 45.15 | ± | 2.92 | 46.97 | ± | 2.48 | 47.28 | ± | 2.98 | |
| CdR—Sag Plane | mm | 44.81 | ± | 2.91 | 46.45 | ± | 2.72 | 47.09 | ± | 2.59 | |
| GoL—Sag Plane | mm | 40.69 | ± | 3.48 | 41.02 | ± | 2.97 | 44.10 | ± | 3.53 | |
| GoR—Sag Plane | mm | 40.44 | ± | 3.76 | 41.81 | ± | 2.78 | 43.77 | ± | 3.21 | |
| UI—Sag Plane | mm | 2.37 | ± | 2.06 | 2.54 | ± | 1.82 | 1.69 | ± | 1.66 | |
| LI—Sag Plane | mm | 2.49 | ± | 2.23 | 2.47 | ± | 1.64 | 1.94 | ± | 1.86 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farronato, M.; Baselli, G.; Baldini, B.; Favia, G.; Tartaglia, G.M. 3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups. Bioengineering 2022, 9, 216. https://doi.org/10.3390/bioengineering9050216
Farronato M, Baselli G, Baldini B, Favia G, Tartaglia GM. 3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups. Bioengineering. 2022; 9(5):216. https://doi.org/10.3390/bioengineering9050216
Chicago/Turabian StyleFarronato, Marco, Giuseppe Baselli, Benedetta Baldini, Gianfranco Favia, and Gianluca Martino Tartaglia. 2022. "3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups" Bioengineering 9, no. 5: 216. https://doi.org/10.3390/bioengineering9050216
APA StyleFarronato, M., Baselli, G., Baldini, B., Favia, G., & Tartaglia, G. M. (2022). 3D Cephalometric Normality Range: Auto Contractive Maps (ACM) Analysis in Selected Caucasian Skeletal Class I Age Groups. Bioengineering, 9(5), 216. https://doi.org/10.3390/bioengineering9050216