
Microfluidic-Based Novel Optical Quantification of Red Blood Cell Concentration in Blood Flow



Abstract
:1. Introduction
2. Materials and Methods
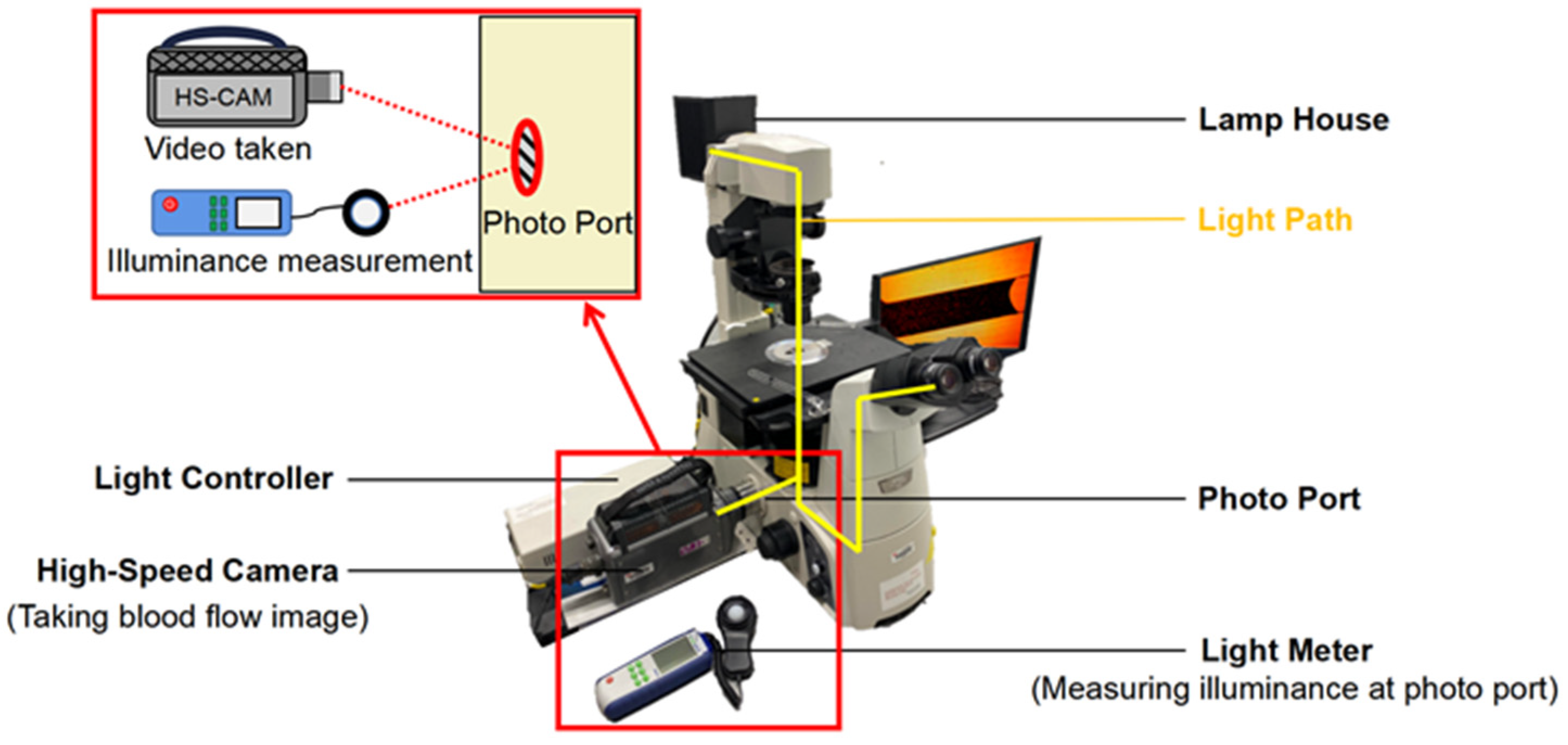
2.1. Optical Settings
2.2. Camera Settings
2.3. Blood Samples Preparation
2.4. PDMS Microchannel Fabrication
3. Experiment
3.1. Luminous Exposure Control
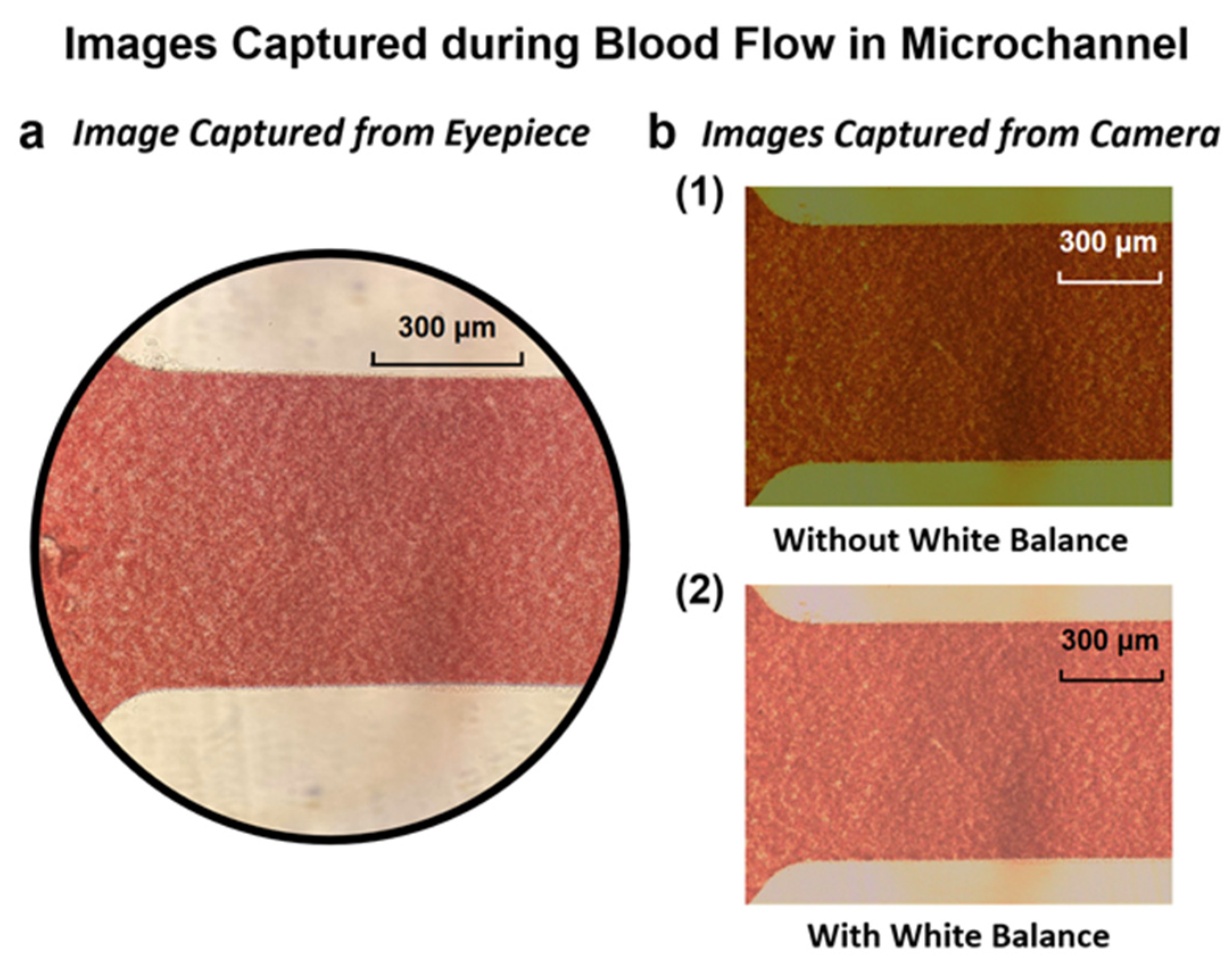
3.2. Capturing Blood Flow Images in the Microchannel
3.3. Conversion of RGB Image to Grayscale Image
4. Results and Discussions
4.1. Luminous Exposure Effect on the Grayscale for Different Hematocrit Values
4.2. Comparison of the Grayscale from the Samples of Different Donors
4.3. Results of Hematocrit and Grayscale at Different Ranges of Luminous Exposure
4.4. Determination of Hematocrit from Grayscale and Luminous Exposures
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giorno, R.; Clifford, J.H.; Beverly, S.; Rossing, R.G. Hematology reference values analysis by different statistical technics and variations with age and sex. Am. J. Clin. Pathol. 1980, 74, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Kosiborod, M.; Smith, G.L.; Radford, M.J.; Foody, J.M.; Krumholz, H.M. The prognostic importance of anemia in patients with heart failure. Am. J. Med. 2003, 114, 112–119. [Google Scholar] [CrossRef]
- Balestracci, A.; Martin, S.M.; Toledo, I.; Alvarado, C.; Wainsztein, R.E. Dehydration at admission increased the need for dialysis in hemolytic uremic syndrome children. Pediatric Nephrol. 2012, 27, 1407–1410. [Google Scholar] [CrossRef]
- Lipschitz, D.A.; Mitchell, C.O.; Thompson, C. The anemia of senescence. Am. J. Hematol. 1981, 11, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Wennecke, G. Hematocrit-A Review of Different Analytical Methods; Radiometer Medical ApS: Copenhagen, Denmark, 2004. [Google Scholar]
- Brown, J.; Theis, L.; Kerr, L.; Zakhidova, N.; O’Connor, K.; Uthman, M.; Oden, Z.M.; Richards-Kortum, R. A hand-powered, portable, low-cost centrifuge for diagnosing anemia in low-resource settings. Am. J. Trop. Med. Hyg. 2011, 85, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldenfarb, P.B.; Bowyer, F.P.; Hall, E.; Brosious, E. Reproducibility in the hematology laboratory: The microhematocrit determination. Am. J. Clin. Pathol. 1971, 56, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Chutipongtanate, A.; Yasaeng, C.; Virankabutra, T.; Chutipongtanate, S. Systematic comparison of four point-of-care methods versus the reference laboratory measurement of hemoglobin in the surgical ICU setting: A cross-sectional method comparison study. BMC Anesthesiol. 2020, 20, 1–6. [Google Scholar] [CrossRef]
- Koster, R.A.; Alffenaar, J.W.C.; Botma, R.; Greijdanus, B.; Touw, D.J.; Uges, D.R.; Kosterink, J.G. What is the right blood hematocrit preparation procedure for standards and quality control samples for dried blood spot analysis? Bioanalysis 2015, 7, 345–351. [Google Scholar] [CrossRef]
- George-Gay, B.; Parker, K. Understanding the complete blood count with differential. J. PeriAnesthesia Nurs. 2003, 18, 96–117. [Google Scholar] [CrossRef]
- Norr, L.C. Nutritional Consequences of Prehistoric Subsistence Strategies in Lower Central America. Ph.D. Dissertation, University of Illinois at Urbana-Champaign, Champaign, IL, USA, 1991. [Google Scholar]
- Berry, S.B.; Fernandes, S.C.; Rajaratnam, A.; De Chiara, N.S.; Mace, C.R. Measurement of the hematocrit using paper-based microfluidic devices. Lab Chip 2016, 16, 3689–3694. [Google Scholar] [CrossRef]
- Riegger, L.; Grumann, M.; Steigert, J.; Lutz, S.; Steinert, C.P.; Mueller, C.; Viertel, J.; Prucker, O.; Rühe, J.; Zengerle, R.; et al. Single-step centrifugal hematocrit determination on a 10-$ processing device. Biomed. Microdevices 2007, 9, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, A.; Kim, S.; Yang, S. Improvement of electrical blood hematocrit measurements under various plasma conditions using a novel hematocrit estimation parameter. Biosens. Bioelectron. 2012, 35, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Lee, Y.S.; Zhbanov, A.; Yang, S. A physiometer for simultaneous measurement of whole blood viscosity and its determinants: Hematocrit and red blood cell deformability. Analyst 2019, 144, 3144–3157. [Google Scholar] [CrossRef] [PubMed]
- Petersson, K.; Jakobsson, O.; Ohlsson, P.; Augustsson, P.; Scheding, S.; Malm, J.; Laurell, T. Acoustofluidic hematocrit determination. Anal. Chim. Acta 2018, 1000, 199–204. [Google Scholar] [CrossRef]
- Guan, G.; Wu, L.; Bhagat, A.A.; Li, Z.; Chen, P.C.; Chao, S.; Ong, C.J.; Han, J. Spiral microchannel with rectangular and trapezoidal cross-sections for size based particle separation. Sci. Rep. 2013, 3, 1475. [Google Scholar] [CrossRef] [Green Version]
- Nivedita, N.; Papautsky, I. Continuous separation of blood cells in spiral microfluidic devices. Biomicrofluidics 2013, 7, 054101. [Google Scholar] [CrossRef] [Green Version]
- Bhagat, A.A.S.; Kuntaegowdanahalli, S.S.; Papautsky, I. Continuous particle separation in spiral microchannels using dean flows and differential migration. Lab Chip 2008, 8, 1906–1914. [Google Scholar] [CrossRef]
- Ginsberg, B.H. Factors affecting blood glucose monitoring: Sources of errors in measurement. J. Diabetes Sci. Technol. 2009, 3, 903–913. [Google Scholar] [CrossRef] [Green Version]
- Nunna, B.B.; Mandal, D.; Lee, J.U.; Singh, H.; Zhuang, S.; Misra, D.; Bhuyian, M.N.U.; Lee, E.S. Detection of cancer antigens (CA-125) using gold nano particles on interdigitated electrode-based microfluidic biosensor. Nano Converg. 2019, 6, 3. [Google Scholar] [CrossRef]
- Nunna, B.B.; Mandal, D.; Zhuang, S.; Lee, E.S. A standalone micro biochip to monitor the cancer progression by measuring cancer antigens as a point-of-care (POC) device for enhanced cancer management. In Proceedings of the 2017 IEEE Healthcare Innovations and Point of Care Technologies (HI-POCT), Bethesda, MD, USA, 6–8 November 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 212–215. [Google Scholar]
- Nunna, B.B.; Lee, E.S. Point-of-care (POC) micro biochip for cancer diagnostics. In Proceedings of the 11th Annual TechConnect World Innovation Conference and Expo, Held Jointly with the 20th Annual Nanotech Conference and Expo, and the 2017 National SBIR/STTR Conference, Washington, MD, USA, 14–17 May 2017; TechConnect: Garching bei München, Germany, 2017; pp. 110–113. [Google Scholar]
- Lee, E.S.; Nunna, B.B. Biomarker Detection and Self-Separation of Serum during Capillary Flow. U.S. Patent 10,481,154, 19 November 2019. [Google Scholar]
- Etienne, E.E.; Nunna, B.B.; Talukder, N.; Wang, Y.; Lee, E.S. COVID-19 Biomarkers and Advanced Sensing Technologies for Point-of-Care (POC) Diagnosis. Bioengineering 2021, 8, 98. [Google Scholar] [CrossRef]
- Arif, T.M.; Ji, Z.; Rahim, M.A.; Nunna, B.B. Modeling Focused-Ultrasound Response for Non-Invasive Treatment Using Machine Learning. Bioengineering 2021, 8, 74. [Google Scholar] [CrossRef] [PubMed]
- Mandal, D.; Nunna, B.B.; Zhuang, S.; Rakshit, S.; Lee, E.S. Carbon nanotubes based biosensor for detection of cancer antigens (CA-125) under shear flow condition. Nano-Struct. Nano-Objects 2018, 15, 180–185. [Google Scholar] [CrossRef]
- Nunna, B.B.; Zhuang, S.; Javier, J.; Mandal, D.; Lee, E.S. Biomolecular Detection using Molecularly Imprinted Polymers (MIPs) at Point-of-Care (POC) Micro Biochip. In Proceedings of the 2016 IEEE-NIH 2016 Healthcare Innovation Point of Care Technologies Conference HI POCT16, (PCHT16-0099), Cancun, Mexico, 9–11 November 2016; pp. 9–11. [Google Scholar]
- Nunna, B.B.; Zhuang, S.; Malave, I.; Lee, E.S. Ovarian cancer diagnosis using micro biochip. In Proceedings of the NIH-IEEE 2015 Strategic Conference on Healthcare Innovations and Point-of-Care Technologies for Precision Medicine, (PCHT15-0056), North Bethesda, Maryland, 9–10 November 2015; pp. 9–10. [Google Scholar]
- Lee, E.S.; Nunna, B.B. Microfluidic Biochip with Enhanced Sensitivity. U.S. Patent 11,020,740, 1 June 2021. [Google Scholar]
- Lee, E.S.; Nunna, B.B.; Suh, K.S. Microfluidic Diagnostic Assembly. U.S. Patent 10,898,894, 26 January 2021. [Google Scholar]
- Eckmann, D.M.; Bowers, S.; Stecker, M.; Cheung, A.T. Hematocrit, volume expander, temperature, and shear rate effects on blood viscosity. Anesth. Analg. 2000, 91, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Pries, A.R.; Neuhaus, D.; Gaehtgens, P. Blood viscosity in tube flow: Dependence on diameter and hematocrit. Am. J. Physiol.-Heart Circ. Physiol. 1992, 263, H1770–H1778. [Google Scholar] [CrossRef]
- Baskurt, O.K.; Meiselman, H.J. Blood rheology and hemodynamics. In Seminars in Thrombosis and Hemostasis; Thieme Medical Publishers, Inc.: New York, NY, USA, 2003; Volume 29, pp. 423–450. [Google Scholar]
- Merrill, E.W.; Pelletier, G.A. Viscosity of human blood: Transition from Newtonian to non-Newtonian. J. Appl. Physiol. 1967, 23, 178–182. [Google Scholar] [CrossRef]
- Zilberman-Rudenko, J.; White, R.M.; Zilberman, D.A.; Lakshmanan, H.H.; Rigg, R.A.; Shatzel, J.J.; Maddala, J.; McCarty, O.J. Design and utility of a point-of-care microfluidic platform to assess hematocrit and blood coagulation. Cell. Mol. Bioeng. 2018, 11, 519–529. [Google Scholar] [CrossRef]
- Zeidan, A.; Golan, L.; Yelin, D. In vitro hematocrit measurement using spectrally encoded flow cytometry. Biomed. Opt. Express 2016, 7, 4327–4334. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Nunna, B.B.; Talukder, N.; Etienne, E.E.; Lee, E.S. Blood Plasma Self-Separation Technologies during the Self-Driven Flow in Microfluidic Platforms. Bioengineering 2021, 8, 94. [Google Scholar] [CrossRef]
- Pasini, E.M.; Lutz, H.U.; Mann, M.; Thomas, A.W. Red blood cell (RBC) membrane proteomics—Part I: Proteomics and RBC physiology. J. Proteom. 2021, 73, 403–420. [Google Scholar] [CrossRef]
- Kanias, T.; Acker, J.P. Biopreservation of red blood cells–the struggle with hemoglobin oxidation. FEBS J. 2010, 277, 343–356. [Google Scholar] [CrossRef]
- Collman, J.P.; Fu, L. Synthetic models for hemoglobin and myoglobin. Acc. Chem. Res. 1999, 32, 455–463. [Google Scholar] [CrossRef]
- Piña-Oviedo, S.; Ortiz-Hidalgo, C.; Ayala, A.G. Human colors—The rainbow garden of pathology: What gives normal and pathologic tissues their color? Arch. Pathol. Lab. Med. 2017, 141, 445–462. [Google Scholar] [CrossRef] [Green Version]
- D’Alessandro, B.; Dhawan, A.P. Multispectral transillumination imaging of skin lesions for oxygenated and deoxygenated hemoglobin measurement. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 6637–6640. [Google Scholar]
- Faber, D.J.; Aalders, M.C.; Mik, E.G.; Hooper, B.A.; van Gemert, M.J.; van Leeuwen, T.G. Oxygen saturation-dependent absorption and scattering of blood. Phys. Rev. Lett. 2004, 93, 028102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohri, M.; Sharifi, K.; Eidi, S. Hematology and serum biochemistry of Holstein dairy calves: Age related changes and comparison with blood composition in adults. Res. Vet. Sci. 2007, 83, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices (Auckl. NZ) 2014, 7, 231. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef]
- Saravanan, C. Color image to grayscale image conversion. In Proceedings of the 2010 Second International Conference on Computer Engineering and Applications, Bali, Indonesia, 19–21 March 2010; IEEE: Piscataway, NJ, USA, 2010; Volume 2, pp. 196–199. [Google Scholar]
- Shvartsman, L.D.; Fine, I. Optical transmission of blood: Effect of erythrocyte aggregation. IEEE Trans. Biomed. Eng. 2003, 50, 1026–1033. [Google Scholar] [CrossRef]
- Gester, K.; Jansen, S.V.; Stahl, M.; Steinseifer, U. A simple method for the investigation of cell separation effects of blood with physiological hematocrit values. Artif. Organs 2015, 39, 432–440. [Google Scholar] [CrossRef]
- Jalal, U.M.; Kim, S.C.; Shim, J.S. Histogram analysis for smartphone-based rapid hematocrit determination. Biomed. Opt. Express 2017, 8, 3317–3328. [Google Scholar] [CrossRef] [Green Version]
- Browne, A.W.; Ramasamy, L.; Cripe, T.P.; Ahn, C.H. A lab-on-a-chip for rapid blood separation and quantification of hematocrit and serum analytes. Lab Chip 2011, 11, 2440–2446. [Google Scholar] [CrossRef]
- Nunna, B.B.; Mandal, D.; Zhuang, S.; Lee, E.S. Innovative point-of-care (POC) micro biochip for early stage ovarian cancer diagnostics. Sens. Transducers 2017, 214, 12–20. [Google Scholar]
- Nunna, B.B.; Wang, Y.; Talukder, N.; Lee, E.S. Capillary Flow Dynamics of Blood with Varied Hematocrit in Microfluidic Platforms. In Proceedings of the 2022 IEEE Healthcare Innovations and Point of Care Technologies (HI-POCT), Houston, TX, USA, 10–11 March 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1–4. [Google Scholar]
- Pratt, W.K. Introduction to Digital Image Processing; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hv (lux·µs) | α (1/lux·µs) | β | γ (1/lux·µs) | δ |
|---|---|---|---|---|
| Less than 6000 | 0.084 | −83.1 | 0.0021 | 0.079 |
| 6000~15,000 | 0.10 | −189 | 0.00070 | 5.7 |
| Bigger than 15,000 | 0.15 | −842 | 0.0014 | −4.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Nunna, B.B.; Talukder, N.; Lee, E.S. Microfluidic-Based Novel Optical Quantification of Red Blood Cell Concentration in Blood Flow. Bioengineering 2022, 9, 247. https://doi.org/10.3390/bioengineering9060247
Wang Y, Nunna BB, Talukder N, Lee ES. Microfluidic-Based Novel Optical Quantification of Red Blood Cell Concentration in Blood Flow. Bioengineering. 2022; 9(6):247. https://doi.org/10.3390/bioengineering9060247
Chicago/Turabian StyleWang, Yudong, Bharath Babu Nunna, Niladri Talukder, and Eon Soo Lee. 2022. "Microfluidic-Based Novel Optical Quantification of Red Blood Cell Concentration in Blood Flow" Bioengineering 9, no. 6: 247. https://doi.org/10.3390/bioengineering9060247
APA StyleWang, Y., Nunna, B. B., Talukder, N., & Lee, E. S. (2022). Microfluidic-Based Novel Optical Quantification of Red Blood Cell Concentration in Blood Flow. Bioengineering, 9(6), 247. https://doi.org/10.3390/bioengineering9060247