
Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
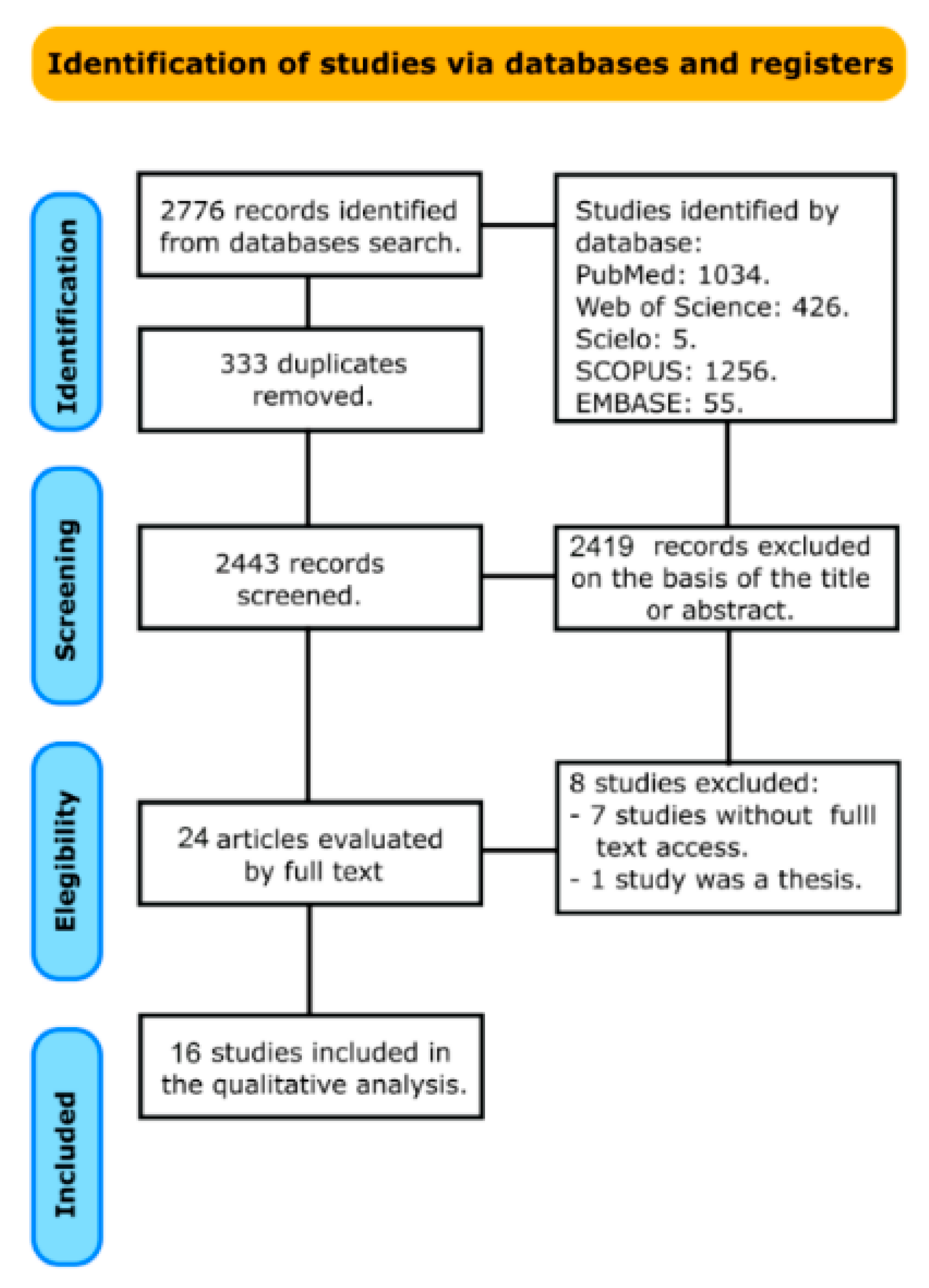
3. Results

{kind=link}
| Author and Year | Type of Clinical Trial | Number of Participants | Reason for Tooth Wear | Restoration Techniques Used | Follow-Up | Clinical Criteria for Evaluation | Main Conclusion |
|---|---|---|---|---|---|---|---|
| Bartlett 2006 [16] | Randomized clinical study | 16 patients with severe tooth wear 13 controls without evidence of tooth wear | Mixture of bruxism and erosion | Direct or indirect microfilled resin composite restorations | 3-year period | United States Public Health Service Evaluation System (USPHS) criteria | Using direct and indirect resin composites for fixing worn posterior teeth is contraindicated |
| Burian 2021 [49] | In-vivo study | Complex rehabilitations with deviations in vertical dimension of occlusion (VDO) 12 patients with severe tooth wear underwent prosthetic rehabilitation, restoring the VDO | Not described | Lithium disilicate ceramic (LS2) Experimental CAD/CAM polymer (COMP) | 3-year period | Geomagic Qualify software (2 January 2012, Geomagic Inc., Morrisville, NC, USA) was used to compare resulting baseline and follow-up STL datasets. | LS2 presented less wear, yet tooth preparation was needed. Clinicians should balance well between required preparation invasiveness and long-term occlusal stability in patients with worn dentitions |
| Crins 2021 [48] | Randomized controlled trial | 49 patients | Grinding/clenching and Gastro-Oesophageal Reflux Disease | Direct composite restorations (DRC) with micro-hybrid composite restorations (Clearfil AP-X, Kuraray) and nano-hybrid composite restorations (IPS Empress Direct, Ivoclar Vivadent) for buccal veneers indirect composite restorations with indirect palatal veneer restorations (Clearfil Estenia C&B, cemented with Panavia F, Kuraray) | 3-year period | Functional (debond, fracture, adaptation, anatomy), Biological (caries, endodontic treatment) Esthetic conditions | Composite restorations showed superior behavior compared to the indirect composite restorations, when used in the molar region |
| Gresnigt 2019 [47] | Randomized split-mouth clinical trial | 11 patients | Not described | 48 indirect resin composite (Estenia) and ceramic laminate veneers (IPS Empress Esthetic) | 10 years | USPHS criteria | Anterior ceramic laminate veneers might be favored over indirect composite laminate veneers |
| Hammoudi 2020 [46] | Randomized clinical trial | 62 participants with extensive tooth wear | Mechanical (bruxism or engaged in vigorous labor or exercise), and chemical factors | 713 lithium disilicate (LD) and translucent zirconia (TZ) crowns | 65 months | USPHS criteria | The use of high-strength ceramic materials, as well as consistent adhesive bonding, are probably the key factors in the long-term success of ceramic crowns in participants with extensive tooth wear independent of the specific etiology |
| Hemmings 2000 [23] | Clinical study | 16 patients | Not described | 52 restorations composed of Durafill composite and Scotchbond Multipurpose dentine adhesive system 52 Herculite XRV composite and Optibond dentine bonding agent | 30 months | Loss Fracture Marginal discoloration Loss of marginal integrity Noticeable wear Pain or sensitivity Endodontic failure Esthetic failure | Direct composite restorations may be a treatment option for localized anterior tooth wear |
| Katsoulis 2011 [45] | Observational study | 42 patients | High daily consumption of tough and acidic food, reflux problems, bulimia combined with clenching and grinding | 48 full prosthodontic rehabilitation | 3 years | Complete oral examination Photos Functional and cast analysis General health conditions and behavioral aspects | The rehabilitation of partially edentulous patients with severe tooth wear is a complex task, and more information regarding treatment protocols, prosthetic indications and treatment outcome is needed |
| da Rocha Scalzer Lopes 2021 [50] | Retrospective study with cross-sectional design | 43 individuals | Not described | 112 single crowns | 120 months | Analysis parameters of morphological variations in tooth wear are indicated | Ceramic systems can be considered as alternatives of restorative material, even in individuals with clinical features evocative of chronic tooth wear |
| Mehta 2021 [52] | Prospective trial | 34 participants | Chemical (erosion) and mechanical wear (bruxism) signs | Direct restorations using a micro-hybrid (Clearfil AP-X; Kuraray, Japan) and a nanohybrid (IPS Empress Direct; Ivoclar Vivadent, Schaan, Liechtenstein) composite | 1 month and 1-, 3-, and 5-years, post-treatment | Presence or absence of any symptoms of pain, difficulty with phonetics and/ or mastication, challenges with the adaption to the new VDO, or any TMJ-related concerns | Premolar restorations exposed lesser risks of failure compared to the molar restorations |
| Mehta 2021 (b) [51] | Prospective trial | 34 participants | Chemical (erosion) and mechanical wear (bruxism) signs | Direct restorations using a micro-hybrid (Clearfil AP-X; Kuraray, Japan) and a nanohybrid (IPS Empress Direct; Ivoclar Vivadent, Schaan, Liechtenstein) composite | 5.5 years | Presence or absence of any symptoms of pain, difficulty with phonetics and/ or mastication, challenges with the adaption to the new VDO, or any TMJ-related concerns | Molar restorations, posterior mandibular restorations and the anterior restorations requiring two further sessions for completion, were associated with significantly higher risks for failure |
| Milosevic 2016 [13] | Prospective trial | 164 patients | Not described | Nano-particle hybrid composite material (Spectrum®®; Dentsply, Weybridge, UK) | 8 years | Failure of the restoration | The assessed failure rate in the first year was 5.4%. Time to failure was significantly greater in older subjects and when a deficiency of posterior support was present. Bruxism and an increase in the Occlusal Vertical Dimension were not associated with failure |
| Oudkerk 2020 [18] | Prospective trial | 7 patients | Chemical (erosion) and mechanical wear (bruxism) | PICN blocks (Vita Enamic HT, Vita Zahnfabrik, Germany; Ceramill Motion 2, Amann Girrbach) | One month, six months, 1 year and 2 years | World Dental Federation | PICN restorations displayed elevated survival and success rates after two years |
| Redman 2003 [20] | Retrospective | 31 subjects | Primarily erosion, Primarily attrition, Combined erosion/attrition | Microfilled (Durafill), hybrid (Herculite—97 direct and 18 indirect) composites, and 73 indirect ‘ceromer’ (Artglass) | 5 years | Modified United States Public Health Services criteria | Placement of resin-based composite restorations to treat localised anterior tooth wear has worthy short to medium term survival |
| Smales 2007 [3] | Retrospective | 25 patients | Tooth grinding, gastric and dietary acids, and abrasive restorative materials | Resin-based composites (RBC), indirect ceramo-metal crowns (CMCs), and full gold crowns | Survival rate | RBCs usually failed from fractures, and CMCs from complete losses. RBC failures were usually replaced or repaired, while CMC failures often required root canal therapies or extractions | |
| Taubóck 2021 [53] | Prospective trial | 13 patients | Erosion-induced tooth wear and no signs of temporomandibular disorders | Microhybrid (first cohort; n = 59) or nanofilled (second cohort; n = 105) composite restorations | 11 years | USPHS criteria | Direct composite restorations employed at an amplified vertical dimension of occlusion display suitable clinical long-term performance in patients presenting severe tooth wear |
| Vailati 2013 [21] | Prospective | 12 patients | Presence of gastroesophageal reflux, excessive ingestion of acidic beverages | Direct and Indirect composite restorations (Miris, Coltène/Whaledent) and feldspathic ceramic veneers (Creation CC, Willi Geller International) | 6 years | Modified United States Public Health Services criteria | Restoring compromised maxillary anterior teeth by means of veneers prevents excessive tooth structure removal and loss of tooth vitality |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salas, M.; Nascimento, G.; Huysmans, M.; Demarco, F. Estimated Prevalence of Erosive Tooth Wear in Permanent Teeth of Children and Adolescents: An Epidemiological Systematic Review and Meta-Regression Analysis. J. Dent. 2015, 43, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Van’t Spijker, A.; Rodriguez, J.M.; Kreulen, C.M.; Bronkhorst, E.M.; Bartlett, D.W.; Creugers, N. Prevalence of Tooth Wear in Adults. Int. J. Prosthodont. 2009, 22, 35–42. [Google Scholar] [PubMed]
- Smales, R.J.; Berekally, T.L. Long-Term Survival of Direct and Indirect Restorations Placed for the Treatment of Advanced Tooth Wear. Eur. J. Prosthodont. Restor. Dent. 2007, 15, 2–6. [Google Scholar] [PubMed]
- Shellis, R.P.; Addy, M. The Interactions between Attrition, Abrasion and Erosion in Tooth Wear. Erosive Tooth Wear 2014, 25, 32–45. [Google Scholar]
- Addy, M.; Shellis, R. Interaction between Attrition, Abrasion and Erosion in Tooth Wear. Dent. Eros. 2006, 20, 17–31. [Google Scholar]
- Wetselaar, P.; Wetselaar-Glas, M.J.; Katzer, L.D.; Ahlers, M.O. Diagnosing Tooth Wear, a New Taxonomy Based on the Revised Version of the Tooth Wear Evaluation System (TWES 2.0). J. Oral Rehabil. 2020, 47, 703–712. [Google Scholar] [CrossRef]
- Li, M.H.; Bernabé, E. Tooth Wear and Quality of Life among Adults in the United Kingdom. J. Dent. 2016, 55, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Muts, E.-J.; van Pelt, H.; Edelhoff, D.; Krejci, I.; Cune, M. Tooth Wear: A Systematic Review of Treatment Options. J. Prosthet. Dent. 2014, 112, 752–759. [Google Scholar] [CrossRef]
- Al-Khayatt, A.; Ray-Chaudhuri, A.; Poyser, N.; Briggs, P.; Porter, R.; Kelleher, M.; Eliyas, S. Direct Composite Restorations for the Worn Mandibular Anterior Dentition: A 7-year Follow-up of a Prospective Randomised Controlled Split-mouth Clinical Trial. J. Oral Rehabil. 2013, 40, 389–401. [Google Scholar] [CrossRef]
- Attin, T.; Filli, T.; Imfeld, C.; Schmidlin, P.R. Composite Vertical Bite Reconstructions in Eroded Dentitions after 5·5 Years: A Case Series. J. Oral Rehabil. 2012, 39, 73–79. [Google Scholar] [CrossRef]
- Hamburger, J.T.; Opdam, N.J.; Bronkhorst, E.M.; Kreulen, C.M.; Roeters, J.J.; Huysmans, M.-C. Clinical Performance of Direct Composite Restorations for Treatment of Severe Tooth Wear. J. Adhes. Dent. 2011, 13, 585–593. [Google Scholar] [PubMed]
- Loomans, B.; Kreulen, C.; Huijs-Visser, H.; Sterenborg, B.; Bronkhorst, E.; Huysmans, M.; Opdam, N. Clinical Performance of Full Rehabilitations with Direct Composite in Severe Tooth Wear Patients: 3.5 Years Results. J. Dent. 2018, 70, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, A.; Burnside, G. The Survival of Direct Composite Restorations in the Management of Severe Tooth Wear Including Attrition and Erosion: A Prospective 8-Year Study. J. Dent. 2016, 44, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Poyser, N.; Briggs, P.; Chana, H.; Kelleher, M.; Porter, R.; Patel, M. The Evaluation of Direct Composite Restorations for the Worn Mandibular Anterior Dentition–Clinical Performance and Patient Satisfaction. J. Oral Rehabil. 2007, 34, 361–376. [Google Scholar] [CrossRef] [PubMed]
- Edelhoff, D.; Güth, J.; Erdelt, K.; Brix, O.; Liebermann, A. Clinical Performance of Occlusal Onlays Made of Lithium Disilicate Ceramic in Patients with Severe Tooth Wear up to 11 Years. Dent. Mater. 2019, 35, 1319–1330. [Google Scholar] [CrossRef]
- Bartlett, D.; Sundaram, G. An up to 3-Year Randomized Clinical Study Comparing Indirect and Direct Resin Composites Used to Restore Worn Posterior Teeth. Int. J. Prosthodont. 2006, 19, 613–617. [Google Scholar]
- Mainjot, A.K.J. The One Step-No Prep Technique: A Straightforward and Minimally Invasive Approach for Full-mouth Rehabilitation of Worn Dentition Using Polymer-infiltrated Ceramic Network (PICN) CAD-CAM Prostheses. J. Esthet. Restor. Dent. 2020, 32, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Oudkerk, J.; Eldafrawy, M.; Bekaert, S.; Grenade, C.; Vanheusden, A.; Mainjot, A. The One-Step No-Prep Approach for Full-Mouth Rehabilitation of Worn Dentition Using PICN CAD-CAM Restorations: 2-Yr Results of a Prospective Clinical Study. J. Dent. 2020, 92, 103245. [Google Scholar] [CrossRef]
- Mainjot, A.K.J.; Charavet, C. Orthodontic-assisted One Step-no Prep Technique: A Straightforward and Minimally-invasive Approach for Localized Tooth Wear Treatment Using Polymer-infiltrated Ceramic Network CAD-CAM Prostheses. J. Esthet. Restor. Dent. 2020, 32, 645–661. [Google Scholar] [CrossRef]
- Redman, C.; Hemmings, K.; Good, J. The Survival and Clinical Performance of Resin–Based Composite Restorations Used to Treat Localised Anterior Tooth Wear. Br. Dent. J. 2003, 194, 566–572. [Google Scholar] [CrossRef]
- Vailati, F.; Gruetter, L.; Belser, U.C. Adhesively Restored Anterior Maxillary Dentitions Affected by Severe Erosion: Up to 6-Year Results of a Prospective Clinical Study. Eur. J. Esthet. Dent. 2013, 8, 506–530. [Google Scholar] [PubMed]
- Mesko, M.E.; Sarkis-Onofre, R.; Cenci, M.S.; Opdam, N.J.; Loomans, B.; Pereira-Cenci, T. Rehabilitation of Severely Worn Teeth: A Systematic Review. J. Dent. 2016, 48, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Hemmings, K.W.; Darbar, U.R.; Vaughan, S. Tooth Wear Treated with Direct Composite Restorations at an Increased Vertical Dimension: Results at 30 Months. J. Prosthet. Dent. 2000, 83, 287–293. [Google Scholar] [CrossRef]
- Gow, A.M.; Hemmings, K.W. The Treatment of Localised Anterior Tooth Wear with Indirect Artglass Restorations at an Increased Occlusal Vertical Dimension. Results after Two Years. Eur. J. Prosthodont. Restor. Dent. 2002, 10, 101–105. [Google Scholar]
- Elderton, R. Clinical Studies Concerning Re-Restoration of Teeth. Adv. Dent. Res. 1990, 4, 4–9. [Google Scholar] [CrossRef]
- Mehta, S.; Banerji, S.; Millar, B.; Suarez-Feito, J.-M. Current Concepts on the Management of Tooth Wear: Part 2. Active Restorative Care 1: The Management of Localised Tooth Wear. Br. Dent. J. 2012, 212, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Lussi, A.; Hellwig, E.; Zero, D.; Jaeggi, T. Erosive Tooth Wear: Diagnosis, Risk Factors and Prevention. Am. J. Dent. 2006, 19, 319. [Google Scholar]
- Loomans, B.; Opdam, N.; Attin, T.; Bartlett, D.; Edelhoff, D.; Frankenberger, R.; Benic, G.; Ramseyer, S.; Wetselaar, P.; Sterenborg, B. Severe Tooth Wear: European Consensus Statement on Management Guidelines. J. Adhes. Dent. 2017, 19, 111–119. [Google Scholar]
- Van de Sande, F.; Opdam, N.; Da Rosa Rodolpho, P.; Correa, M.; Demarco, F.; Cenci, M. Patient Risk Factors’ Influence on Survival of Posterior Composites. J. Dent. Res. 2013, 92, S78–S83. [Google Scholar] [CrossRef]
- Mehta, S.B.; Banerji, S.; Millar, B.J.; Suarez-Feito, J.-M. Current Concepts on the Management of Tooth Wear: Part 4. An Overview of the Restorative Techniques and Dental Materials Commonly Applied for the Management of Tooth Wear. Br. Dent. J. 2012, 212, 169–177. [Google Scholar] [CrossRef]
- Varma, S.; Preiskel, A.; Bartlett, D. The Management of Tooth Wear with Crowns and Indirect Restorations. Br. Dent. J. 2018, 224, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K.J. Standardizing Failure, Success, and Survival Decisions in Clinical Studies of Ceramic and Metal–Ceramic Fixed Dental Prostheses. Dent. Mater. 2012, 28, 102–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denry, I.; Kelly, J.R. State of the Art of Zirconia for Dental Applications. Dent. Mater. 2008, 24, 299–307. [Google Scholar] [CrossRef]
- Warreth, A.; Elkareimi, Y. All-Ceramic Restorations: A Review of the Literature. Saudi Dent. J. 2020, 32, 365–372. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B. Novel Zirconia Materials in Dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Weigl, P.; Sander, A.; Wu, Y.; Felber, R.; Lauer, H.-C.; Rosentritt, M. In-Vitro Performance and Fracture Strength of Thin Monolithic Zirconia Crowns. J. Adv. Prosthodont. 2018, 10, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Aljawad, A.; Rees, J.S. Retrospective Study of the Survival and Patient Satisfaction with Composite Dahl Restorations in the Management of Localised Anterior Tooth Wear. Eur. J. Prosthodont. Restor. Dent. 2016, 24, 222–229. [Google Scholar]
- Bartlett, D.; Sundaram, G.; Moazzez, R. Trial of protective effect of fissure sealants, in vivo, on the palatal surfaces of anterior teeth, in patients suffering from erosion. J. Dent. 2011, 39, 26–29. [Google Scholar] [CrossRef]
- Hamburger, J.T. Treatment of Severe Tooth Wear: A Minimally Invasive Approach; [Sl: Sn]; Radboud University: Nijmegen, The Netherlands, 2015; ISBN 90-90-28731-0. [Google Scholar]
- Walls, A. The Use of Adhesively Retained All-Porcelain Veneers during the Management of Fractured and Worn Anterior Teeth: Part 2. Clinical Results after 5 Years of Follow-Up. Br. Dent. J. 1995, 178, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Walls, A. The Use of Adhesively Retained All-Porcelain Veneers during the Management of Fractured and Worn Anterior Teeth: Part 1. Clinical Technique. Br. Dent. J. 1995, 178, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Woodley, N.; Griffiths, B.; Hemmings, K. Retrospective Audit of Patients with Advanced Toothwear Restored with Removable Partial Dentures. Eur. J. Prosthodont. Restor. Dent. 1996, 4, 185–191. [Google Scholar] [PubMed]
- Katsoulis, J.; Nikitovic, S.G.; Spreng, S.; Neuhaus, K.; Mericske-Stern, R. Prosthetic Rehabilitation and Treatment Outcome of Partially Edentulous Patients with Severe Tooth Wear: 3-Years Results. J. Dent. 2011, 39, 662–671. [Google Scholar] [CrossRef]
- Hammoudi, W.; Trulsson, M.; Svensson, P.; Smedberg, J.-I. Long-Term Results of a Randomized Clinical Trial of 2 Types of Ceramic Crowns in Participants with Extensive Tooth Wear. J. Prosthet. Dent. 2020, 127, 248–257. [Google Scholar] [CrossRef]
- Gresnigt, M.; Cune, M.; Jansen, K.; Van der Made, S.; Özcan, M. Randomized Clinical Trial on Indirect Resin Composite and Ceramic Laminate Veneers: Up to 10-Year Findings. J. Dent. 2019, 86, 102–109. [Google Scholar] [CrossRef]
- Crins, L.; Opdam, N.; Kreulen, C.; Bronkhorst, E.; Sterenborg, B.; Huysmans, M.; Loomans, B. Randomized Controlled Trial on the Performance of Direct and Indirect Composite Restorations in Patients with Severe Tooth Wear. Dent. Mater. 2021, 37, 1645–1654. [Google Scholar] [CrossRef]
- Burian, G.; Erdelt, K.; Schweiger, J.; Keul, C.; Edelhoff, D.; Güth, J.-F. In-Vivo-Wear in Composite and Ceramic Full Mouth Rehabilitations over 3 Years. Sci. Rep. 2021, 11, 14056. [Google Scholar] [CrossRef]
- da Rocha Scalzer Lopes, G.; de Faria Viana, A.A.; Diniz, V.; de Matos, J.D.; Andrade, V.C.; Bottino, M.A.; Nishioka, R.S.; Chiarelli, F.M.; Feitosa, A.C.R.; Guerra, S.M.G. Incidence of Fracture in Single Ceramic Crowns in Patients with Chronic Tooth Wear: A Clinical Follow-up. Int. J. Odontostomatol. 2021, 15, 102–110. [Google Scholar] [CrossRef]
- Mehta, S.B.; Lima, V.P.; Bronkhorst, E.M.; Crins, L.; Bronkhorst, H.; Opdam, N.J.; Huysmans, M.-C.D.; Loomans, B.A. Clinical Performance of Direct Composite Resin Restorations in a Full Mouth Rehabilitation for Patients with Severe Tooth Wear: 5.5-Year Results. J. Dent. 2021, 112, 103743. [Google Scholar] [CrossRef]
- Mehta, S.B.; Bronkhorst, E.M.; Lima, V.P.; Crins, L.; Bronkhorst, H.; Opdam, N.J.; Huysmans, M.-C.D.; Loomans, B.A. The Effect of Pre-Treatment Levels of Tooth Wear and the Applied Increase in the Vertical Dimension of Occlusion (VDO) on the Survival of Direct Resin Composite Restorations. J. Dent. 2021, 111, 103712. [Google Scholar] [CrossRef]
- Tauböck, T.T.; Schmidlin, P.R.; Attin, T. Vertical Bite Rehabilitation of Severely Worn Dentitions with Direct Composite Restorations: Clinical Performance up to 11 Years. J. Clin. Med. 2021, 10, 1732. [Google Scholar] [CrossRef]
- Alhadainy, H.A.; Abdalla, A.I. 2-Year Clinical Evaluation of Dentin Bonding Systems. Am. J. Dent. 1996, 9, 77–79. [Google Scholar]
- Clelland, N.L.; Villarroel, S.C.; Knobloch, L.A.; Seghi, R.R. Simulated Oral Wear of Packable Composites. Oper. Dent. 2003, 28, 830–837. [Google Scholar]
- Knobloch, L.A.; Kerby, R.E.; Seghi, R.; Berlin, J.S.; Clelland, N. Fracture Toughness of Packable and Conventional Composite Materials. J. Prosthet. Dent. 2002, 88, 307–313. [Google Scholar] [CrossRef]
- Lima, V.P.; Machado, J.B.; Zhang, Y.; Loomans, B.A.; Moraes, R.R. Laboratory methods to simulate the mechanical degradation of resin composite restorations. Dent. Mater. 2022, 38, 214–229. [Google Scholar] [CrossRef]
- Raposo, L.H.A.; Neiva, N.A.; da Silva, G.R.; Carlo, H.L.; da Mota, A.S.; do Prado, C.J.; Soares, C.J. Ceramic Restoration Repair: Report of Two Cases. J. Appl. Oral Sci. 2009, 17, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Campos, T.; Ramos, N.; Machado, J.; Bottino, M.; Souza, R.; Melo, R. A New Silica-Infiltrated Y-TZP Obtained by the Sol-Gel Method. J. Dent. 2016, 48, 55–61. [Google Scholar] [CrossRef] [Green Version]
- de Matos, J.D.M.; Nakano, L.J.N.; Bottino, M.A.; de Jesus, R.H.; Maciel, L.C. Current Considerations for Dental Ceramics and Their Respective Union Systems. Rev. Bras. Odontol. 2020, 77, e1768. [Google Scholar] [CrossRef]
- Erpenstein, H.; Borchard, R.; Kerschbaum, T. Long-Term Clinical Results of Galvano-Ceramic and Glass-Ceramic Individual Crowns. J. Prosthet. Dent. 2000, 83, 530–534. [Google Scholar] [CrossRef]
- Cehreli, M.C.; Kökat, A.M.; Ozpay, C.; Karasoy, D.; Akca, K. A Randomized Controlled Clinical Trial of Feldspathic versus Glass-Infiltrated Alumina All-Ceramic Crowns: A 3-Year Follow-Up. Int. J. Prosthodont. 2011, 24, 77–84. [Google Scholar] [PubMed]
- Wall, J.G.; Cipra, D.L. Alternative Crown Systems: Is the Metal-Ceramic Crown Always the Restoration of Choice? Dent. Clin. N. Am. 1992, 36, 765–782. [Google Scholar] [CrossRef]
- Mainjot, A.K.; Dupont, N.M.; Oudkerk, J.C.; Dewael, T.Y.; Sadoun, M.J. From Artisanal to CAD-CAM Blocks: State of the Art of Indirect Composites. J. Dent. Res. 2016, 95, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Alt, V.; Hannig, M.; Wöstmann, B.; Balkenhol, M. Fracture Strength of Temporary Fixed Partial Dentures: CAD/CAM versus Directly Fabricated Restorations. Dent. Mater. 2011, 27, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Stawarczyk, B.; Liebermann, A.; Eichberger, M.; Güth, J.-F. Evaluation of Mechanical and Optical Behavior of Current Esthetic Dental Restorative CAD/CAM Composites. J. Mech. Behav. Biomed. Mater. 2016, 55, 1–11. [Google Scholar] [CrossRef]
- Magne, P.; Schlichting, L.H.; Maia, H.P.; Baratieri, L.N. In Vitro Fatigue Resistance of CAD/CAM Composite Resin and Ceramic Posterior Occlusal Veneers. J. Prosthet. Dent. 2010, 104, 149–157. [Google Scholar] [CrossRef]
- Güth, J.; Edelhoff, D.; Goldberg, J.; Magne, P. CAD/CAM Polymer vs Direct Composite Resin Core Buildups for Endodontically Treated Molars without Ferrule. Oper. Dent. 2016, 41, 53–63. [Google Scholar] [CrossRef]
- Yilmaz, B. CAD-CAM High-Density Polymer Implant-Supported Fixed Diagnostic Prostheses. J. Prosthet. Dent. 2018, 119, 688–692. [Google Scholar] [CrossRef]
- Wassell, R.; Walls, A.; McCabe, J. Direct Composite Inlays versus Conventional Composite Restorations: 5-Year Follow-Up. J. Dent. 2000, 28, 375–382. [Google Scholar] [CrossRef]

| #1 | Tooth Wear OR Tooth erosion OR Tooth attrition OR Dental Wear |
| #2 | Restoration OR Direct Restoration OR Composite OR Resin Composite OR Composite Resin OR Dental Composite OR Resin Based Composite OR Composite Dental Resin OR Fillings OR Indirect Restoration OR Partial Restorations OR Posterior Partial Crowns OR Full-Coverage Restoration OR Ceramic OR Bonded OR Partial Preparations OR Indirect Bonded Restorations OR Porcelain OR Ceramic Veneer OR Overlay OR Inlay OR Onlay |
| #3 | Clinical Trials OR Controlled Clinical Trial OR Retrospective Studies OR Randomized Controlled Trial OR Randomized Controlled Trials OR Prospective Clinical Trial OR Retrospective Study OR Prospective Studies OR Prospective Study OR Clinical Trial OR Randomized Clinical Trial OR Random Allocation OR Double-Blind Method OR Single-Blind Method OR Clinical Trial OR Clinical Trials OR Follow-up Studies OR Prospective Studies OR Cross-over Studies |
| #4 | #1 and #2 and #3 |
| Study and Year | Selection Bias | Performance and Detection Bias | Bias Due to Incomplete Data | Reporting Bias | Other Bias |
|---|---|---|---|---|---|
| Bartlett 2006 [16] | Low risk | High risk | Low risk | High risk | High risk |
| Burian 2021 [49] | Low risk | High risk | High risk | High risk | High risk |
| Crins 2021 [48] | Low risk | Low risk | Low risk | High risk | High risk |
| Gresnigt 2019 [47] | Low risk | Low risk | Low risk | High risk | High risk |
| Hammoudi 2020 [46] | Low risk | Low risk | Low risk | Low risk | High risk |
| Hemmings 2000 [23] | Low risk | High risk | High risk | High risk | Low risk |
| Katsoulis 2011 [45] | High risk | High risk | High risk | High risk | Low risk |
| da Rocha Scalzer Lopes 2021 [50] | High risk | High risk | High risk | High risk | Low risk |
| Mehta 2021 [52] | Low risk | Low risk | High risk | High risk | Low risk |
| Mehta 2021 (b) [51] | Low risk | High risk | High risk | High risk | Low risk |
| Milosevic 2016 [13] | High risk | High risk | High risk | High risk | Low risk |
| Oudkerk 2020 [18] | High risk | High risk | Low risk | High risk | Low risk |
| Redman 2003 [20] | High risk | High risk | Low risk | High risk | Low risk |
| Smales 2007 [3] | High risk | High risk | High risk | High risk | High risk |
| Taubóck 2021 [53] | High risk | High risk | Low risk | High risk | High risk |
| Vailati 2013 [21] | High risk | High risk | Low risk | Low risk | High risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hardan, L.; Mancino, D.; Bourgi, R.; Cuevas-Suárez, C.E.; Lukomska-Szymanska, M.; Zarow, M.; Jakubowicz, N.; Zamarripa-Calderón, J.E.; Kafa, L.; Etienne, O.; et al. Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies. Bioengineering 2022, 9, 346. https://doi.org/10.3390/bioengineering9080346
Hardan L, Mancino D, Bourgi R, Cuevas-Suárez CE, Lukomska-Szymanska M, Zarow M, Jakubowicz N, Zamarripa-Calderón JE, Kafa L, Etienne O, et al. Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies. Bioengineering. 2022; 9(8):346. https://doi.org/10.3390/bioengineering9080346
Chicago/Turabian StyleHardan, Louis, Davide Mancino, Rim Bourgi, Carlos Enrique Cuevas-Suárez, Monika Lukomska-Szymanska, Maciej Zarow, Natalia Jakubowicz, Juan Eliezer Zamarripa-Calderón, Laura Kafa, Olivier Etienne, and et al. 2022. "Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies" Bioengineering 9, no. 8: 346. https://doi.org/10.3390/bioengineering9080346
APA StyleHardan, L., Mancino, D., Bourgi, R., Cuevas-Suárez, C. E., Lukomska-Szymanska, M., Zarow, M., Jakubowicz, N., Zamarripa-Calderón, J. E., Kafa, L., Etienne, O., Reitzer, F., Kharouf, N., & Haïkel, Y. (2022). Treatment of Tooth Wear Using Direct or Indirect Restorations: A Systematic Review of Clinical Studies. Bioengineering, 9(8), 346. https://doi.org/10.3390/bioengineering9080346