
Two-Axis Continuous Distractor for Mandibular Reconstruction

 ,
,  ,
, 
Abstract
:1. Introduction
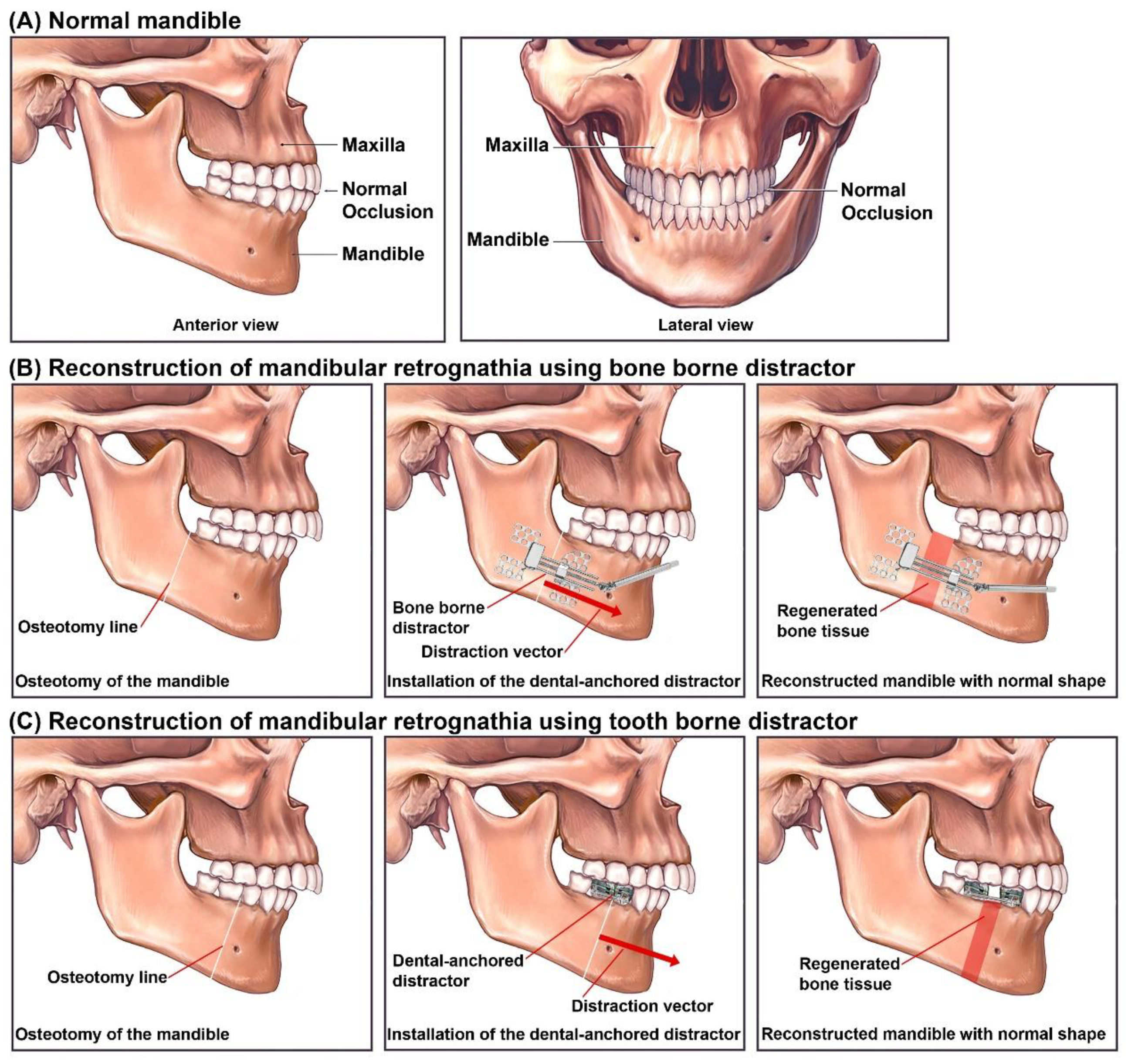
Distraction Osteogenesis for Mandibular Reconstruction
2. Materials and Methods
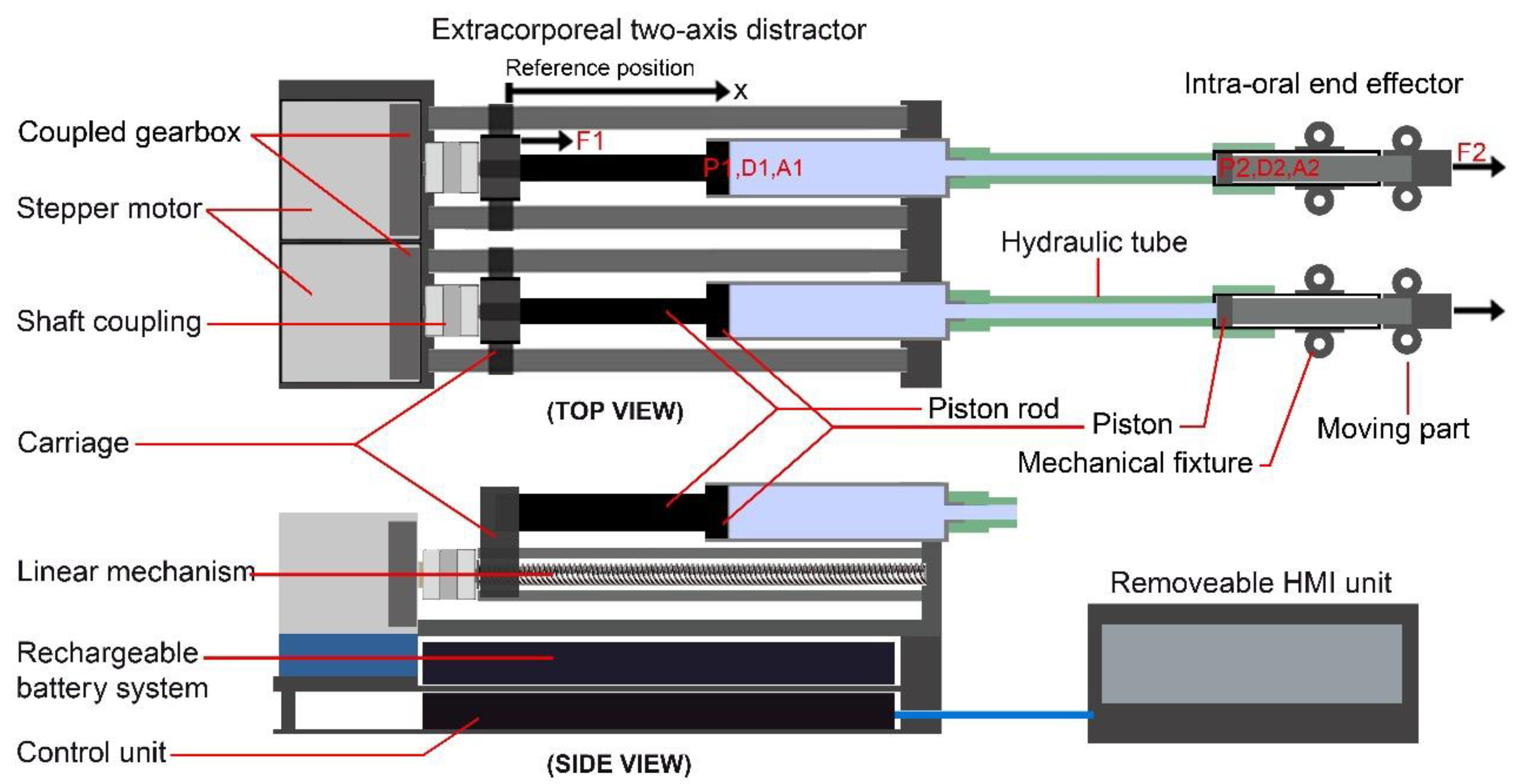
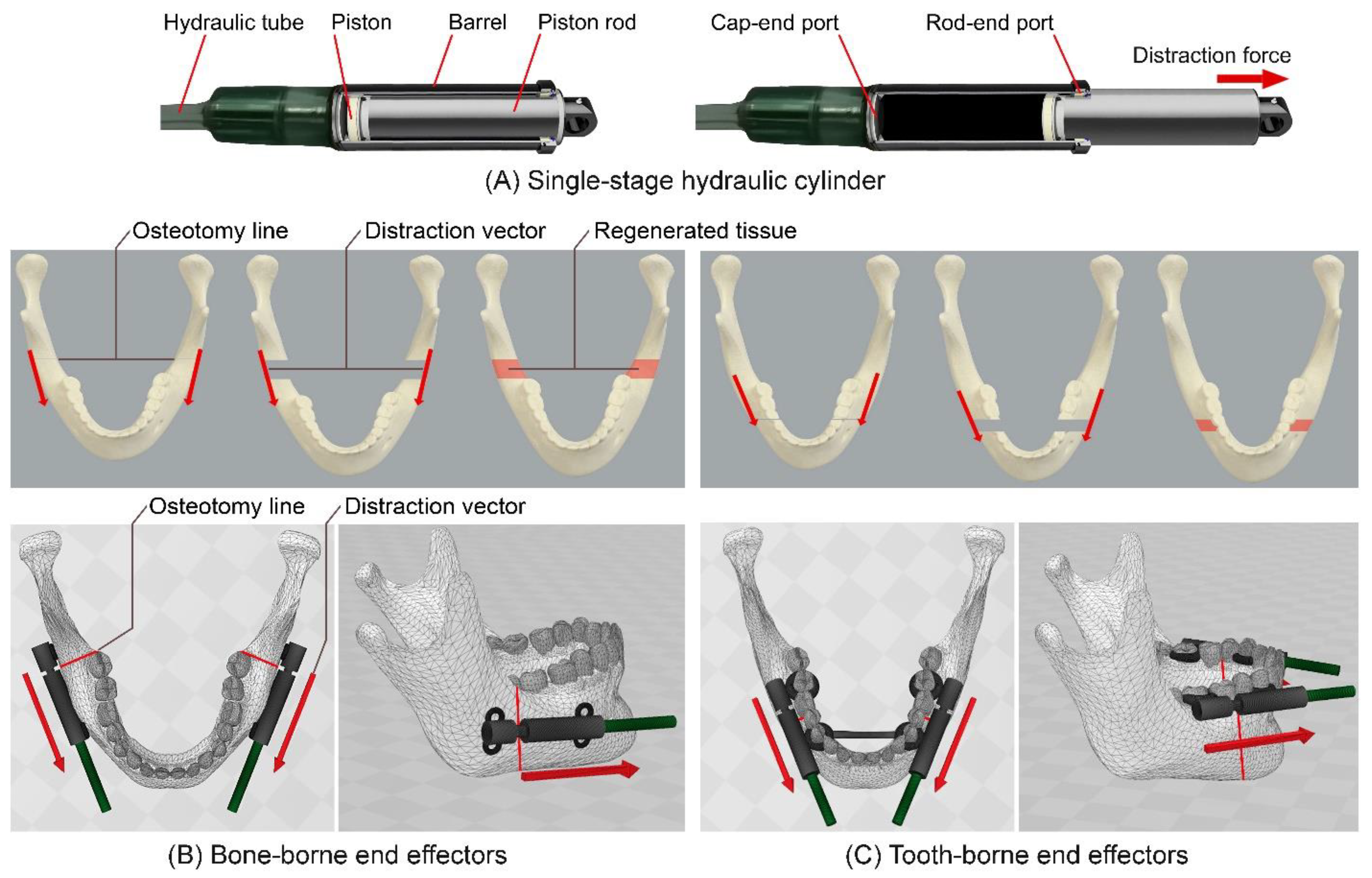
2.1. Design and Principles
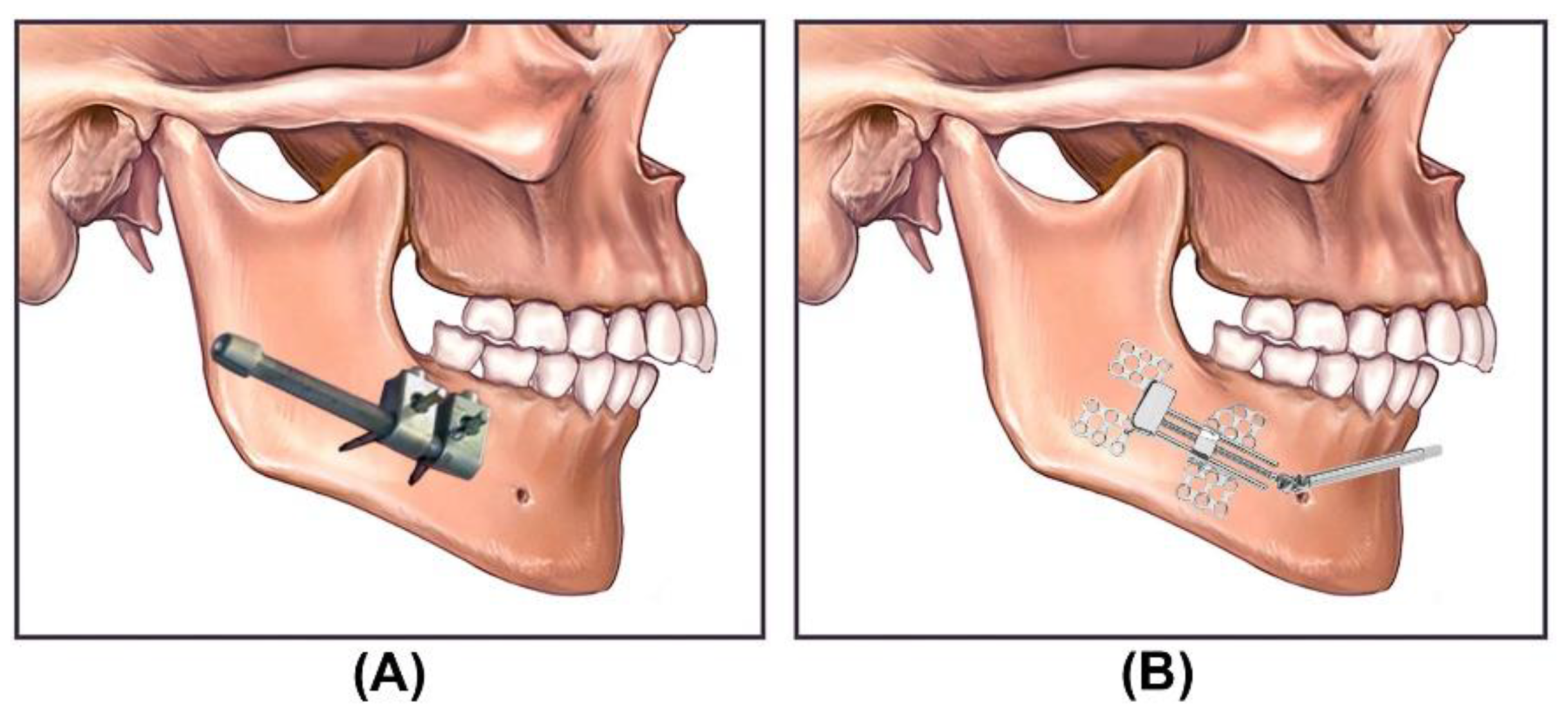
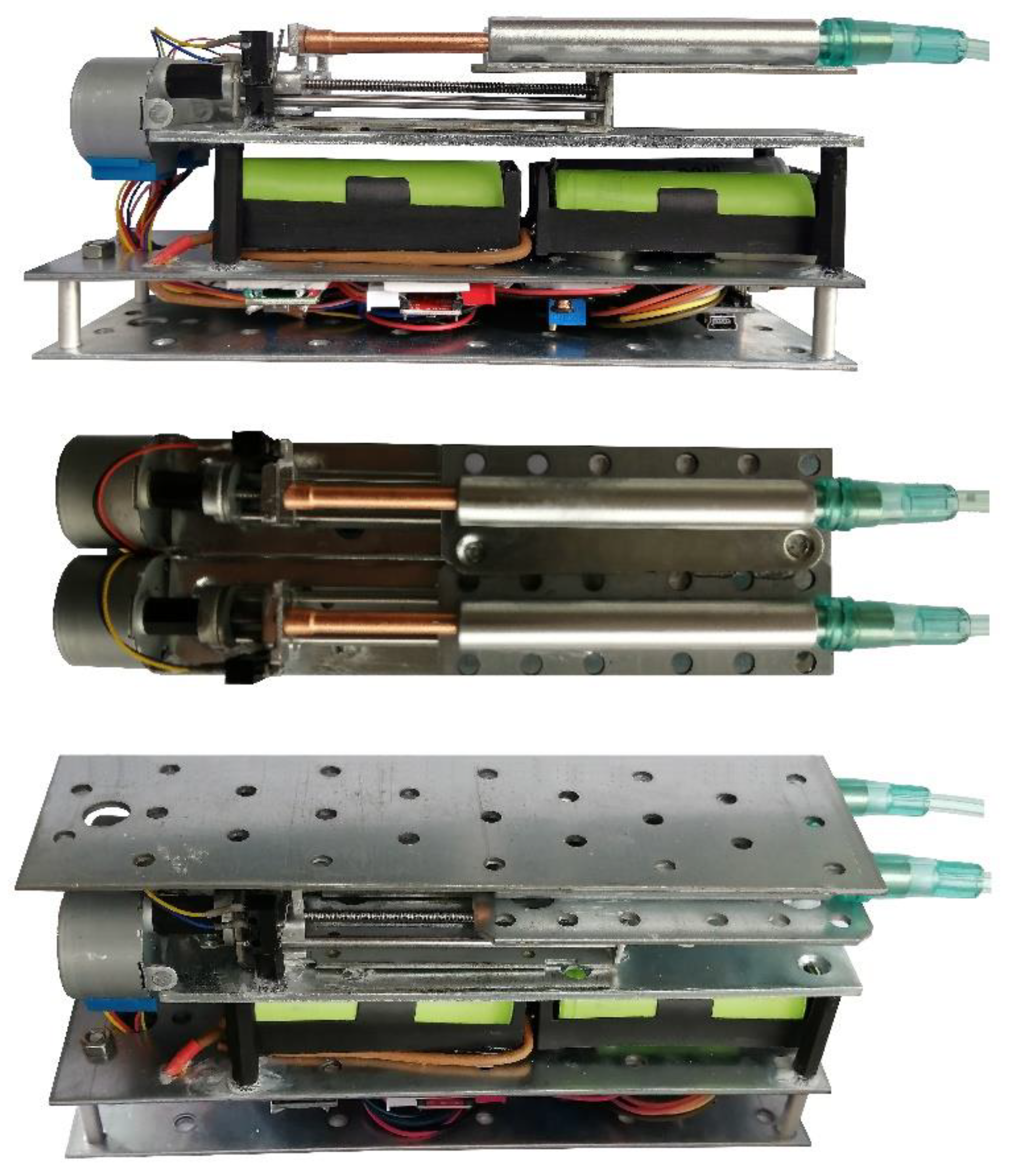
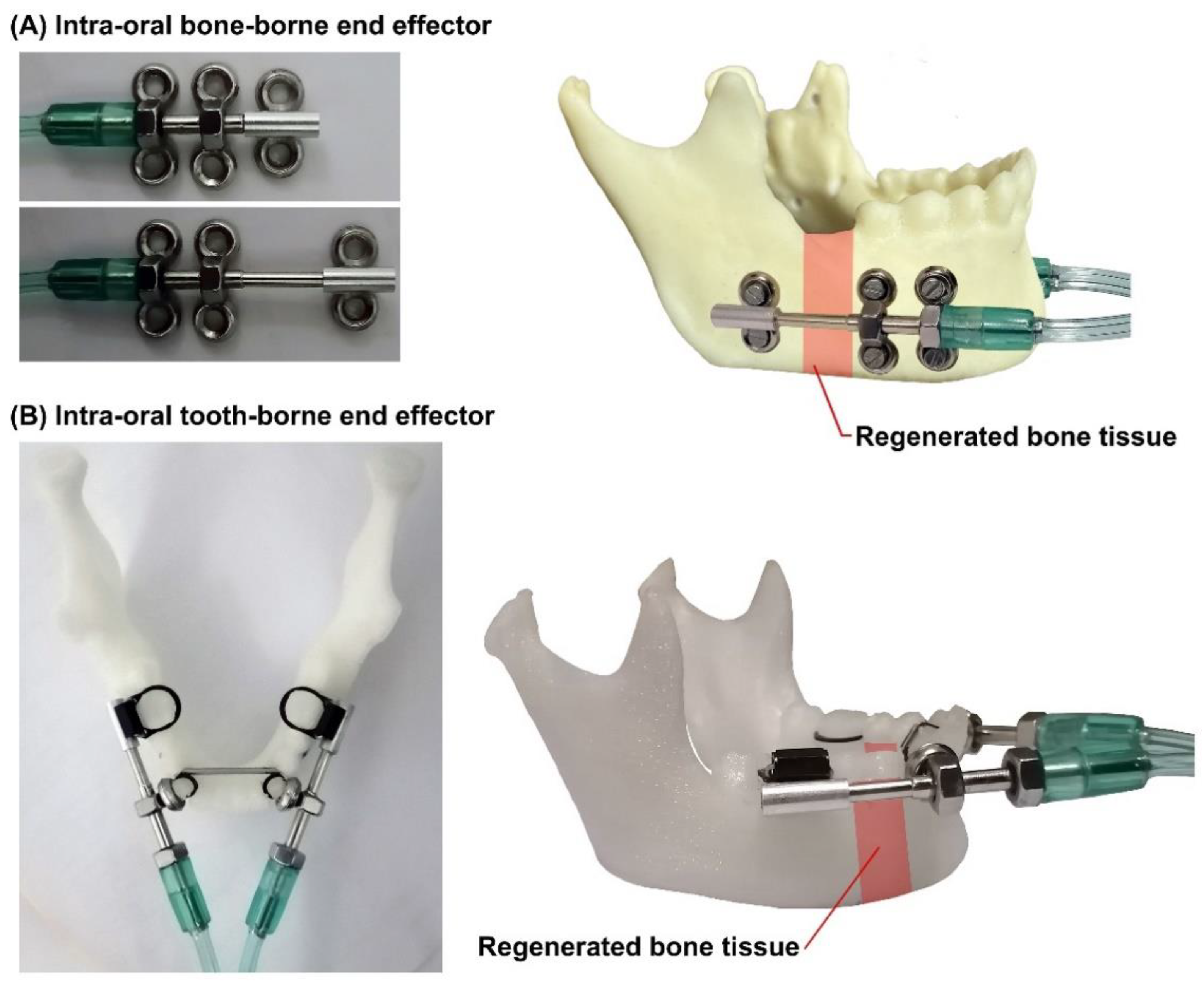
2.2. Intra-Oral BB and TB End Effectors
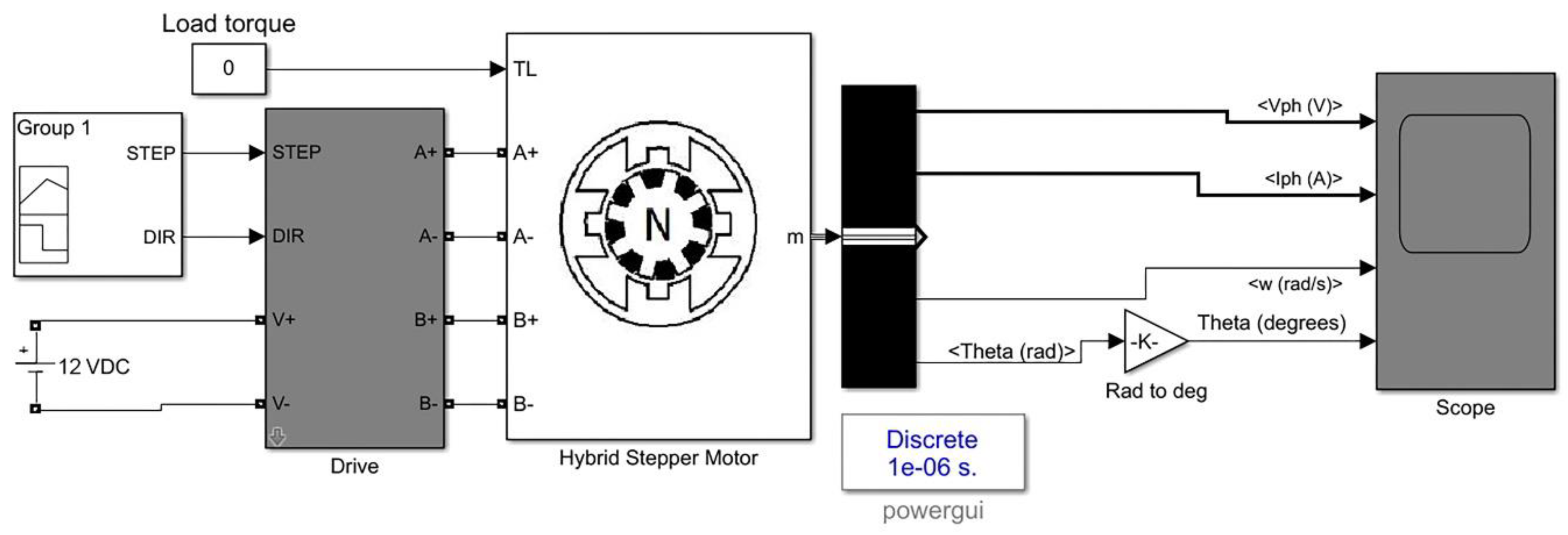
2.3. Mathematical Modeling
2.4. Experimental Study
3. Results
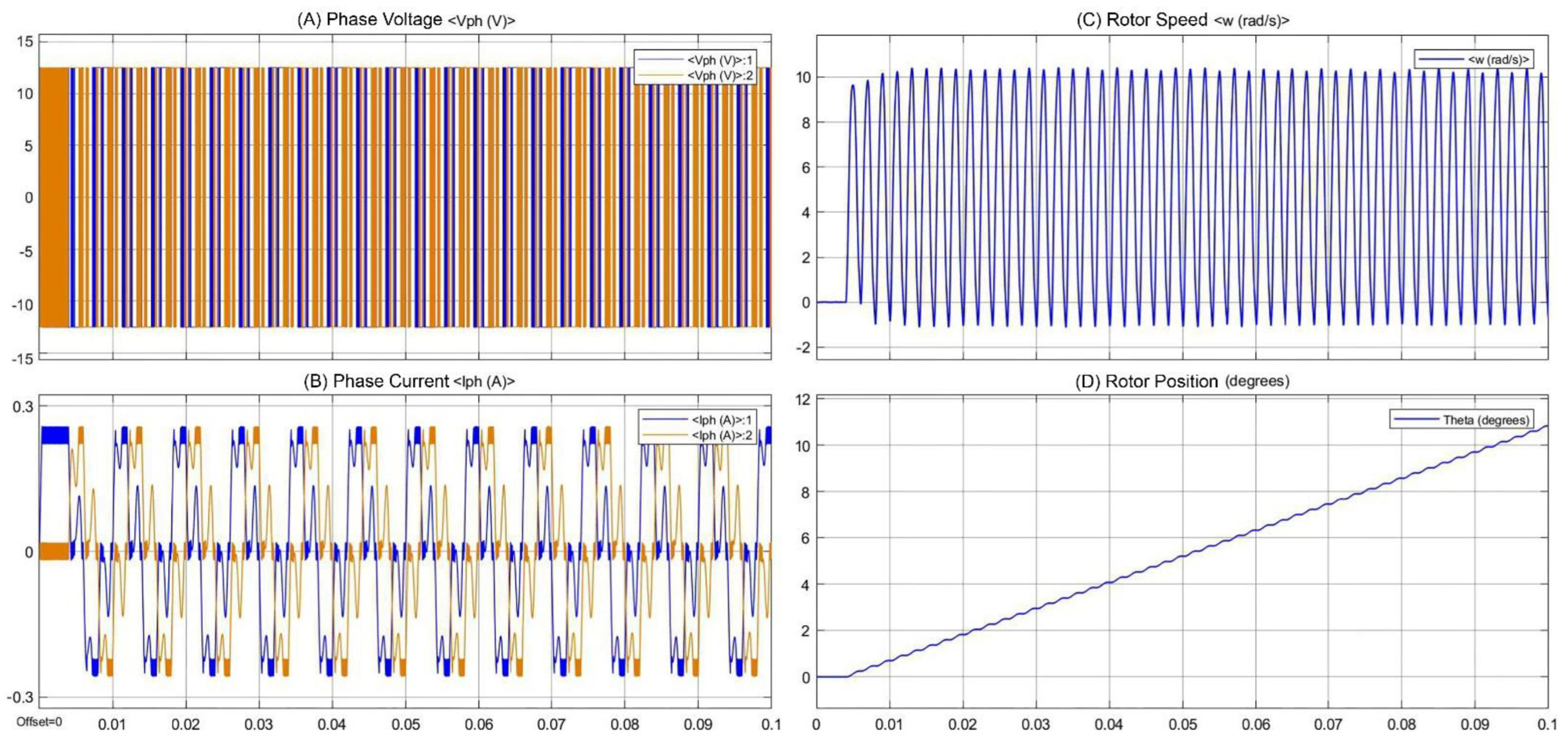
3.1. Simulation Results
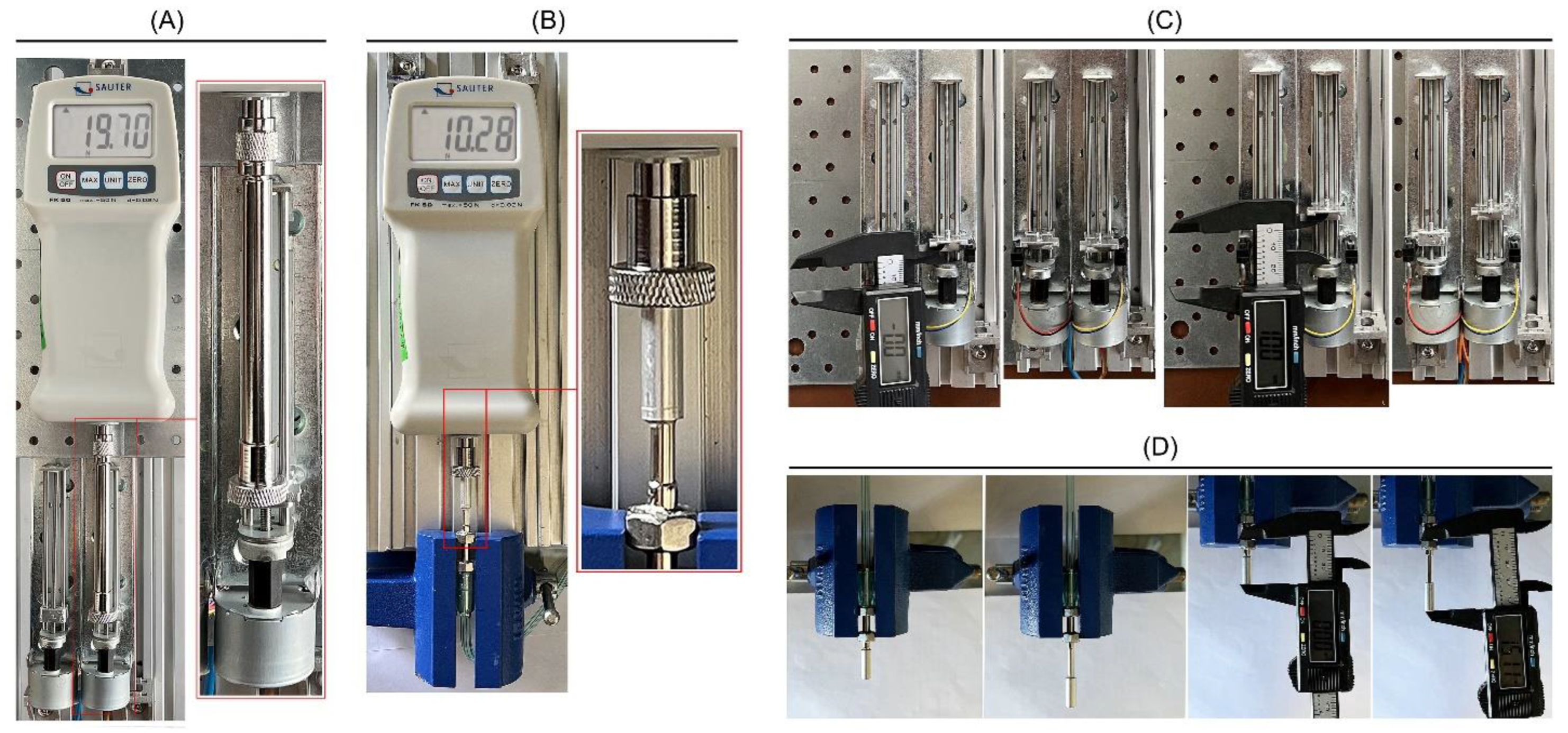
3.2. Measurement of the Generated Force and Linear Positioning of the Mechanism
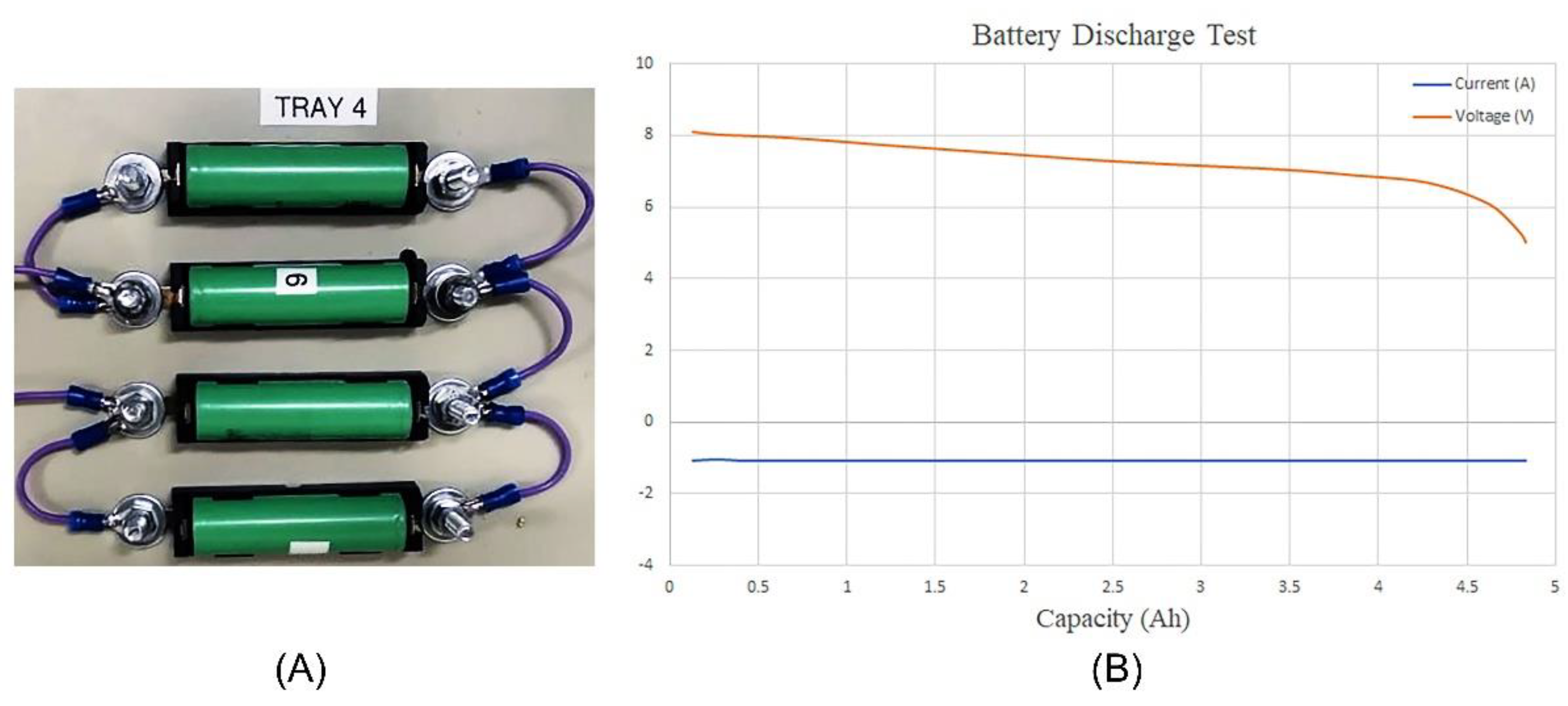
3.3. Evaluation of the Battery System
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Troulis, M.J.; Padwa, B.; Kaban, L.B. Distraction Osteogenesis. In Management of Complications in Oral and Maxillofacial Surgery; John Wiley & Sons: Hoboken, NJ, USA, 2022; pp. 209–220. [Google Scholar]
- Proffit, W.R.; Jackson, T.H.; Turvey, T.A. Changes in the pattern of patients receiving surgical-orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; McGrath, C.; Hägg, U. The impact of malocclusion and its treatment on quality of life: A literature review. Int. J. Paediatr. Dent. 2006, 16, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Hatefi, S.; Alizargar, J.; Le Roux, F.; Hatefi, K.; Sh, M.E.; Davids, H.; Hsieh, N.C.; Smith, F.; Abou-El-Hossein, K. Review of physical stimulation techniques for assisting distraction osteogenesis in maxillofacial reconstruction applications. Med. Eng. Phys. 2021, 91, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Hatefi, S.; Hatefi, K.; Le Roux, F.; Alizargar, J.; Behdadipour, Z.; Yihun, Y.; Abou-El-Hossein, K. Review of automatic continuous distraction osteogenesis devices for mandibular reconstruction applications. BioMed. Eng. OnLine 2020, 19, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.; Vashistha, A.; Chaudhary, M.; Kaur, G. Biological basis of distraction osteogenesis—A review. J. Oral Maxillofac. Surg. Med. Pathol. 2016, 28, 1–7. [Google Scholar] [CrossRef]
- Resnick, M.C.; Padwa, B.L. Use of distraction osteogenesis in orthognathic surgery. Semin. Orthod. 2019, 25, 205–217. [Google Scholar] [CrossRef]
- Swennen, G.; Dempf, R.; Schliephake, H. Cranio-facial distraction osteogenesis: A review of the literature. Part II: Experimental studies. Int. J. Oral Maxillofac. Surg. 2002, 31, 123–135. [Google Scholar] [CrossRef]
- Mofid, M.M.; Manson, P.N.; Robertson, B.C.; Tufaro, A.P.; Elias, J.J.; Vander Kolk, C.A. Craniofacial distraction osteogenesis: A review of 3278 cases. Plast. Reconstr. Surg. 2001, 108, 1103–1114. [Google Scholar] [CrossRef]
- Molina, F. Mandibular distraction osteogenesis: A clinical experience of the last 17 years. J. Craniofacial Surg. 2009, 20, 1794–1800. [Google Scholar] [CrossRef]
- Amir, R.L.; Everts, V.; Bronckers, A.L. Bone regeneration during distraction osteogenesis. Odontology 2009, 97, 63–75. [Google Scholar] [CrossRef]
- Karp, N.S.; Thorne, C.H.M.; McCarthy, J.G.; Sissons, H.A. Bone lengthening in the craniofacial skeleton. Ann. Plast. Surg. 1990, 24, 231–237. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.G.; Schreiber, J.; Karp, N.; Thorne, C.H.; Grayson, B.H. Lengthening the human mandible by gradual distraction. Plast. Reconstr. Surg. 1992, 89, 1–8. [Google Scholar] [CrossRef] [PubMed]
- El-Ghannam, A. Bone reconstruction: From bioceramics to tissue engineering. Expert Rev. Med. Devices 2005, 2, 87–101. [Google Scholar] [CrossRef]
- Goldwaser, B.R.; Papadaki, M.E.; Kaban, L.B.; Troulis, M.J. Automated continuous mandibular distraction osteogenesis: Review of the literature. J. Oral Maxillofac. Surg. 2012, 70, 407–416. [Google Scholar] [CrossRef]
- Ilizarov, G.A. The principles of the Ilizarov method. Bull. Hosp. Jt. Dis. Orthop. Inst. 1987, 48, 1–11. [Google Scholar]
- Ilizarov, G.A. The tension-stress effect on the genesis and growth of tissues: Part I. The influence of stability of fixation and soft-tissue preservation. Clin. Orthop. Relat. Res. 1989, 238, 249–281. [Google Scholar] [CrossRef]
- Ilizarov, G.A. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin. Orthop. Relat. Res. 1989, 239, 263–285. [Google Scholar] [CrossRef]
- Cano, J.; Campo, J.; Moreno, L.A.; Bascones, A. Osteogenic alveolar distraction: A review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, 11–28. [Google Scholar] [CrossRef]
- Gubin, A.; Borzunov, D.; Marchenkova, L.O.; Malkova, T.A.; Smirnova, I.L. Contribution of GA Ilizarov to bone reconstruction: Historical achievements and state of the art. Strateg. Trauma Limb Reconstr. 2016, 11, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Hariri, F.; Chin, S.Y.; Rengarajoo, J.; Foo, Q.C.; Abidin, S.N.N.Z.; Badruddin, A.F.A. Distraction Osteogenesis in Oral and Craniomaxillofacial Reconstructive Surgery. In Osteogenesis and Bone Regeneration; IntechOpen: London, UK, 2018. [Google Scholar]
- Uckan, S.; Veziroglu, F.; Dayangac, E. Alveolar distraction osteogenesis versus autogenous onlay bone grafting for alveolar ridge augmentation: Technique, complications, and implant survival rates. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 106, 511–515. [Google Scholar] [CrossRef]
- Van Strijen, P.J.; Breuning, K.H.; Becking, A.G.; Perdijk, F.B.T.; Tuinzing, D.B. Complications in bilateral mandibular distraction osteogenesis using internal devices. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Saulačić, N.; Martín, M.S.; Camacho, M.D.L.A.L.; García, A.G. Complications in alveolar distraction osteogenesis: A clinical investigation. J. Oral Maxillofac. Surg. 2007, 65, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Mazzonetto, R.; Allais, M.; Maurette, P.E.; Moreira, R.W.F. A retrospective study of the potential complications during alveolar distraction osteogenesis in 55 patients. Int. J. Oral Maxillofac. Surg. 2007, 36, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Dasukil, S.; Verma, S.; Boyina, K.; Jena, A. Unpredicted bilateral device breakage during active phase of mandibular distraction: A case report and literature review. J. Stomatol. Oral Maxillofac. Surg. 2020, 122, 319–324. [Google Scholar] [CrossRef]
- Rubio-Bueno, P.; Villa, E.; Carreno, A.; Naval, L.; Sastre, J.; Manzanares, R.; Dıaz-Gonzalez, F.J. Intraoral mandibular distraction osteogenesis: Special attention to treatment planning. J. Cranio-Maxillofac. Surg. 2001, 29, 254–262. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.D.; Rivera, R.D.; E Feinberg, S.; Sastry, A.M. An Implantable Battery System for a Continuous Automatic Distraction Device for Mandibular Distraction Osteogenesis. J. Med. Devices 2010, 4, 045005. [Google Scholar] [CrossRef]
- Guerrero, C.A.; Bell, W.H.; Contasti, G.I.; Rodriguez, A.M. Mandibular widening by intraoral distraction osteogenesis. Br. J. Oral Maxillofac. Surg. 1997, 35, 383–392. [Google Scholar] [CrossRef]
- Carls, R.F.; Sailer, H.F. Seven years clinical experience with mandibular distraction in children. J. Cranio-Maxillofac. Surg. 1998, 26, 197–208. [Google Scholar] [CrossRef]
- Andrade, N.; Gandhewar, T.; Kalra, R. Development and evolution of distraction devices: Use of indigenous appliances for Distraction Osteogenesis—An overview. Ann. Maxillofac. Surg. 2011, 1, 58. [Google Scholar] [CrossRef] [Green Version]
- Tucker, M.R. Part one: Management of severe mandibular retrognathia in the adult patient using traditional orthognathic surgery. J. Oral Maxillofac. Surg. 2002, 60, 1334–1340. [Google Scholar] [CrossRef]
- Li, Y.; Pan, Q.; Xu, J.; He, X.; Li, H.A.; Oldridge, D.A.; Li, G.; Qin, L. Overview of methods for enhancing bone regeneration in distraction osteogenesis: Potential roles of biometals. J. Orthop. Transl. 2021, 27, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Guastaldi, F.P.; Takusagawa, T.; McCain, J.P.; Monteiro, J.L.; Troulis, M.J. Maxillofacial Reconstruction: From Autogenous Bone Grafts to Bone Tissue Engineering. In Advances in Dental Implantology using Nanomaterials and Allied Technology Applications; Chaughule, R.S., Dashaputra, R., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 353–364. [Google Scholar]
- Diner, P.A.; Kollar, E.M.; Martinez, H.; Vazquez, M.P. Intraoral distraction for mandibular lengthening: A technical innovation. J. Cranio-Maxillofac. Surg. 1996, 24, 92–95. [Google Scholar] [CrossRef]
- Huang, C.-S.; Ko, W.-C.; Lin, W.-Y.; Liou, E.J.-W.; Hong, K.-F.; Chen, Y.-R. Mandibular Lengthening by Distraction Osteogenesis in Children—A One-Year Follow-Up Study. Cleft Palate-Craniofacial J. 1999, 36, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Havlik, J.R.; Bartlett, S.P. Mandibular Distraction Lengthening in the Severely Hypoplastic Mandible: A Problematic Case with Tongue Aplasia. J. Craniofacial Surg. 1994, 5, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Codivilla, A. The classic: On the means of lengthening, in the lower limbs, the muscles and tissues which are shortened through deformity. Clin. Orthop. Relat. Res. 2008, 466, 2903–2909. [Google Scholar] [CrossRef] [Green Version]
- Cohen, R.S.; Rutrick, R.E.; Burstein, F.D. Distraction Osteogenesis of the Human Craniofacial Skeleton: Initial Experience with a New Distraction System. J. Craniofacial Surg. 1995, 6, 368–374. [Google Scholar] [CrossRef]
- Brevi, B.C.; Toma, L.; Magri, A.S.; Sesenna, E. Use of the mandibular distraction technique to treat obstructive sleep apnea syndrome. J. Oral Maxillofac. Surg. 2011, 69, 566–571. [Google Scholar] [CrossRef]
- Botzenhart, U.U.; Végh, A.; Jianu, R.; Gedrange, T. Mandibular midline distraction osteogenesis. Oral Health Dental. Manag. 2013, 12, 305–312. [Google Scholar]
- Al-Moraissi, E.A.; Ellis, E., III. Bilateral sagittal split ramus osteotomy versus distraction osteogenesis for advancement of the retrognathic mandible. J. Oral Maxillofac. Surg. 2015, 73, 1564–1574. [Google Scholar] [CrossRef]
- Akkerman, V.; Ho, J.; de Lange, E.B.J.; van de Onderkaak, V. Bilaterale sagittale splijtingsosteotomie versus distractieosteogenese. Ned. Tijdschr. Tandheelkd. 2015, 122, 603–608. [Google Scholar] [CrossRef] [Green Version]
- Kloukos, D.; Fudalej, P.; Sequeira-Byron, P.; Katsaros, C. Maxillary distraction osteogenesis versus orthognathic surgery for cleft lip and palate patients. Cochrane Database Syst. Rev. 2016, 9, CD010403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vale, F.; Queiroga, J.; Pereira, F.; Ribeiro, M.; Marques, F.; Travassos, R.; Nunes, C.; Paula, A.B.; Francisco, I. A New Orthodontic-Surgical Approach to Mandibular Retrognathia. Bioengineering 2021, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Fernandes do Vale, F.J. Distração Osteogénica Mandibular Dento-Ancorada: Estudo Experimental. Ph.D. Thesis, University of Coimbra, Coimbra, Portugal, 2014. [Google Scholar]
- Razdolsky, Y.; Pensler, J.; Dessner, S. Skeletal distraction for mandibular lengthening with a completely intraoral toothborne distractor. Craniofacial Growth Ser. 1998, 34, 117–140. [Google Scholar]
- El-Bialy, T.; Razdolsky, Y.; Kravitz, N.; Dessner, S.; Elgazzar, R. Long-term results of bilateral mandibular distraction osteogenesis using an intraoral tooth-borne device in adult Class II patients. Int. J. Oral Maxillofac. Surg. 2013, 42, 1446–1453. [Google Scholar] [CrossRef] [PubMed]
- Hatefi, S.; Ghahraei, O.; Bahraminejad, B. Design and Development of a Novel Multi-Axis Automatic Controller for Improving Accuracy in CNC Applications. Majlesi J. Electr. Eng. 2017, 11, 19. [Google Scholar]
- Hatefi, S.; Ghahraei, O.; Bahraminejad, B. Design and Development of a Novel CNC Controller for Improving Machining Speed. Majlesi J. Electr. Eng. 2016, 10, 7. [Google Scholar]
- Ruilope, R.P. Modelling and Control of Stepper Motors for High Accuracy Positioning Systems Used in Radioactive Environments; Universidad Politecnica de Madrid: Madrid, Spain, 2014. [Google Scholar]
- Karadeniz, M.A.; Alkayyali, M.; Szemes, P.T. Modelling and Simulation of Stepper Motor For Position Control Using LabVIEW. Recent Innov. Mechatron. 2018, 5, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Djasim, U.M.; Wolvius, E.B.; Bos, J.A.; van Neck, H.W.; van der Wal, K.G. Continuous versus discontinuous distraction: Evaluation of bone regenerate following various rhythms of distraction. J. Oral Maxillofac. Surg. 2009, 67, 818–826. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase 1: Extracorporeal Linear Mechanism | |||||
|---|---|---|---|---|---|
| Test | Repeat Cycle | Carriage Movement Rate (mm/day) | Desired Carriage Travel (mm) | Mean Measured Carriage Travel (mm) | Mean Carriage Positioning Error Rate (%) |
| 1 | 5 | 3 | 5 | 5.01 | 0.20 |
| 2 | 5 | 3 | 10 | 10.04 | 0.40 |
| 3 | 5 | 5 | 10 | 10.03 | 0.30 |
| 4 | 5 | 3 | 15 | 15.03 | 0.2 |
| 5 | 5 | 5 | 15 | 15.02 | 0.13 |
| Phase 2: Intra-Oral End Effector | |||||
| Test | Repeat Cycle | DR (mm/day) | Desired DL (mm) | Mean Measured DL (mm) | Mean DL Error Rate (%) |
| 1 | 5 | 3 | 5 | 5.23 | 4.6 |
| 2 | 5 | 3 | 10 | 10.26 | 2.6 |
| 3 | 5 | 5 | 10 | 10.18 | 1.8 |
| 4 | 5 | 3 | 15 | 15.23 | 1.5 |
| 5 | 5 | 5 | 15 | 15.46 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatefi, S.; Etemadi Sh, M.; Alizargar, J.; Behdadipour, V.; Abou-El-Hossein, K. Two-Axis Continuous Distractor for Mandibular Reconstruction. Bioengineering 2022, 9, 371. https://doi.org/10.3390/bioengineering9080371
Hatefi S, Etemadi Sh M, Alizargar J, Behdadipour V, Abou-El-Hossein K. Two-Axis Continuous Distractor for Mandibular Reconstruction. Bioengineering. 2022; 9(8):371. https://doi.org/10.3390/bioengineering9080371
Chicago/Turabian StyleHatefi, Shahrokh, Milad Etemadi Sh, Javad Alizargar, Venous Behdadipour, and Khaled Abou-El-Hossein. 2022. "Two-Axis Continuous Distractor for Mandibular Reconstruction" Bioengineering 9, no. 8: 371. https://doi.org/10.3390/bioengineering9080371
APA StyleHatefi, S., Etemadi Sh, M., Alizargar, J., Behdadipour, V., & Abou-El-Hossein, K. (2022). Two-Axis Continuous Distractor for Mandibular Reconstruction. Bioengineering, 9(8), 371. https://doi.org/10.3390/bioengineering9080371