Comparison of Micro-Census Results for Magarya Ward, Wurno Local Government Area of Sokoto State, Nigeria, with Other Sources of Denominator Data

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Demographic Analysis
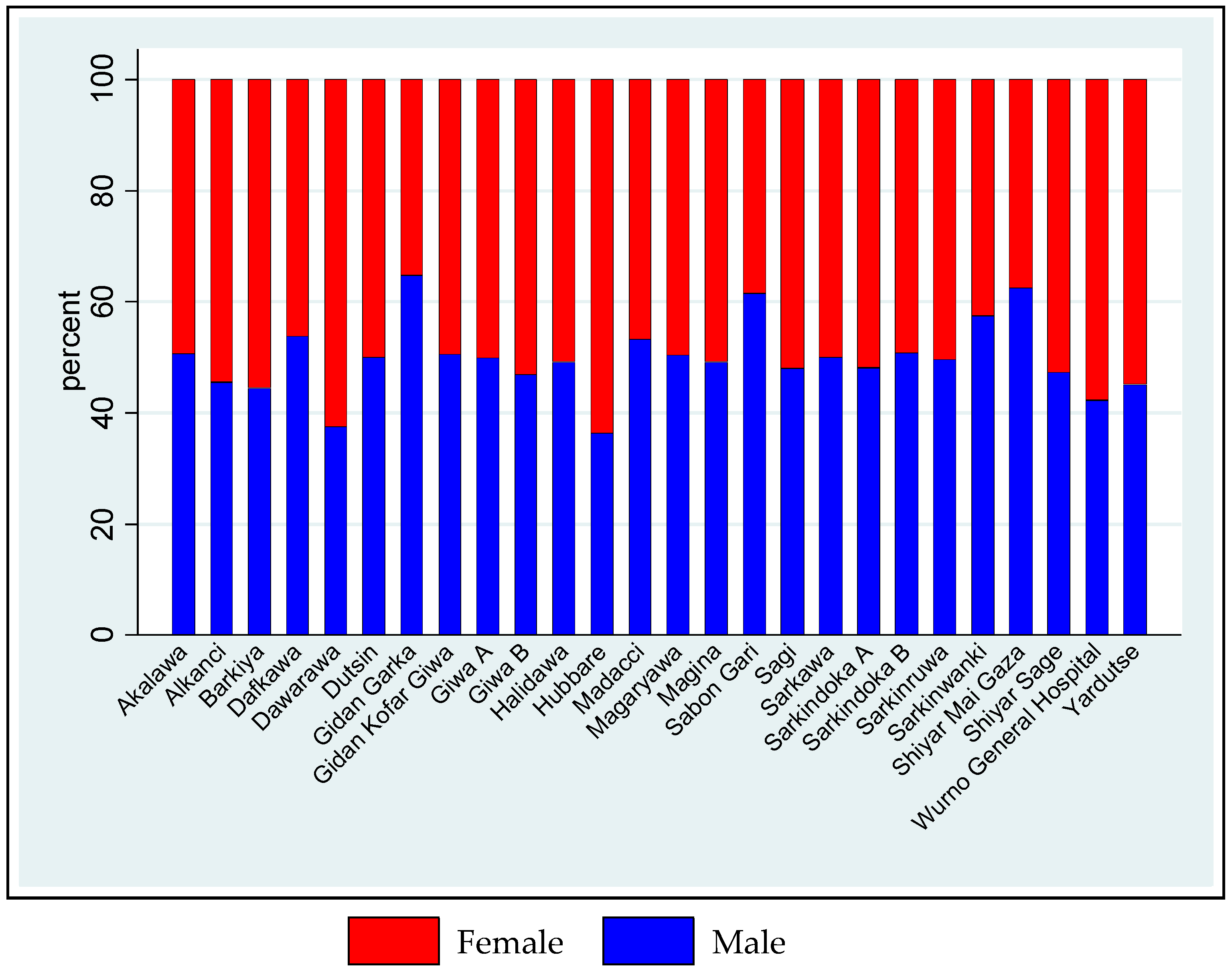
2.1.1. Settlement Characteristics
2.1.2. Household Characteristics
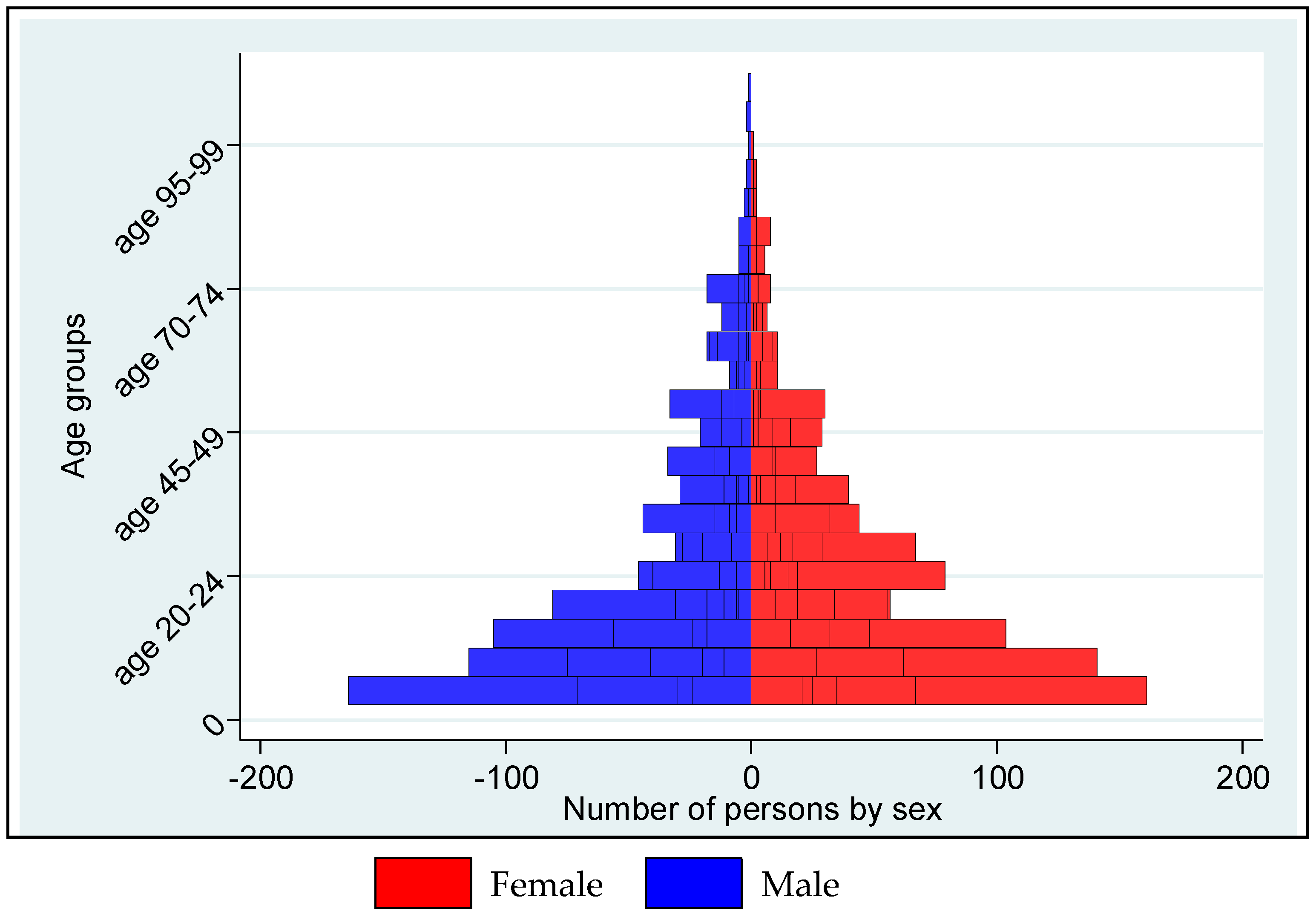
2.1.3. Personal Characteristics
2.2. Comparison with Other Sources of Demographic Data
2.2.1. Comparison with the 2018 projections from the 2006 Population and Housing Census
2.2.2. Comparison with the 2017 Polio Emergency Operations Centre (EOC) Walk-Through Enumeration
2.2.3. Comparison with the Count of Children Younger than 12 Months for 2018 Demand Generation Project (Franka, R.; Abad, N. CDC, Atlanta, GA, USA, personal communication, 15 May 2018)
2.2.4. Comparison with the 2018 Geographic, Population, and Demographic Estimates (GeoPoDe)
2.2.5. Comparison with the 2013 Nigeria Demographic and Health Survey
3. Materials and Methods
3.1. Ethical Considerations
3.2. Target Population
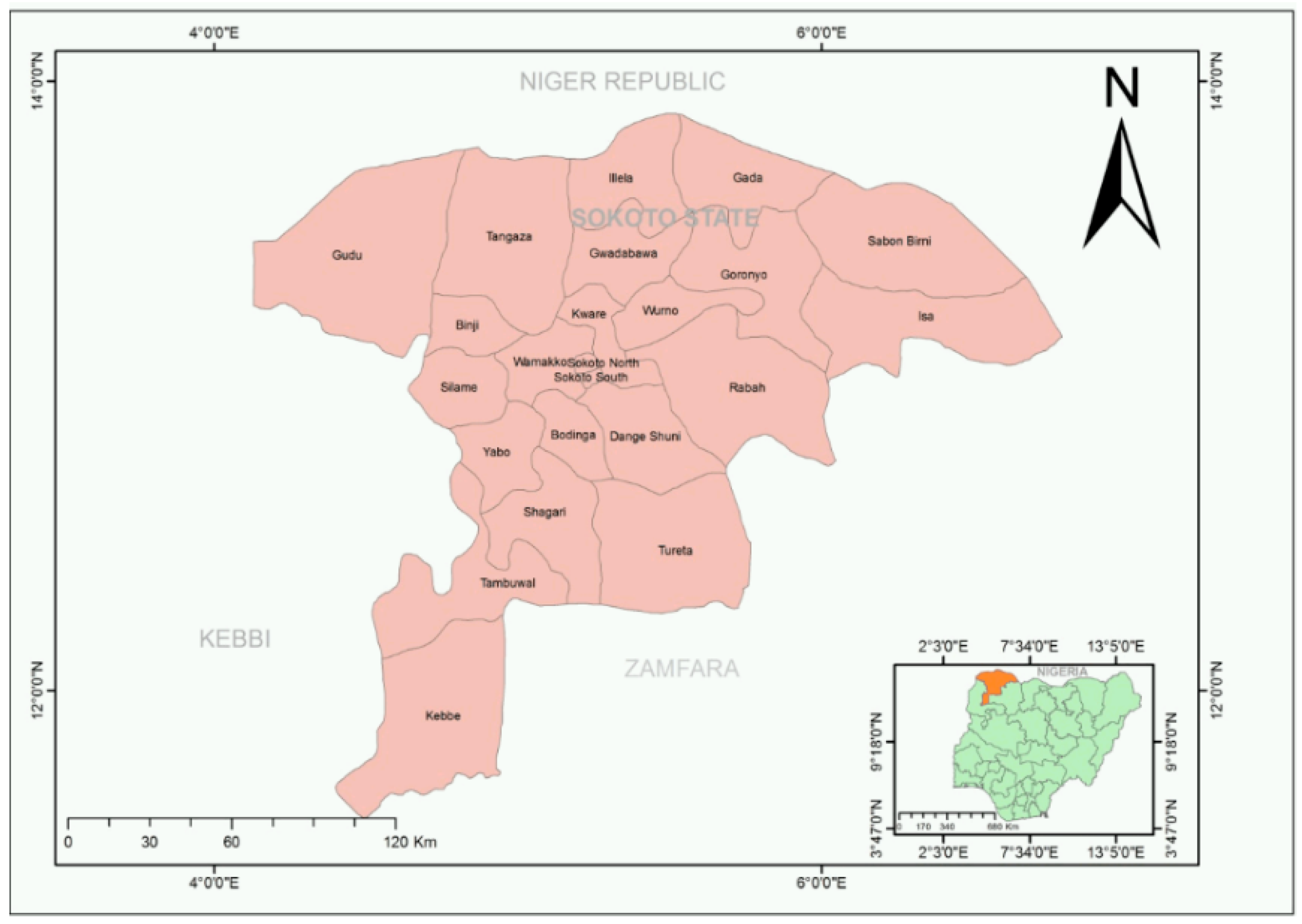
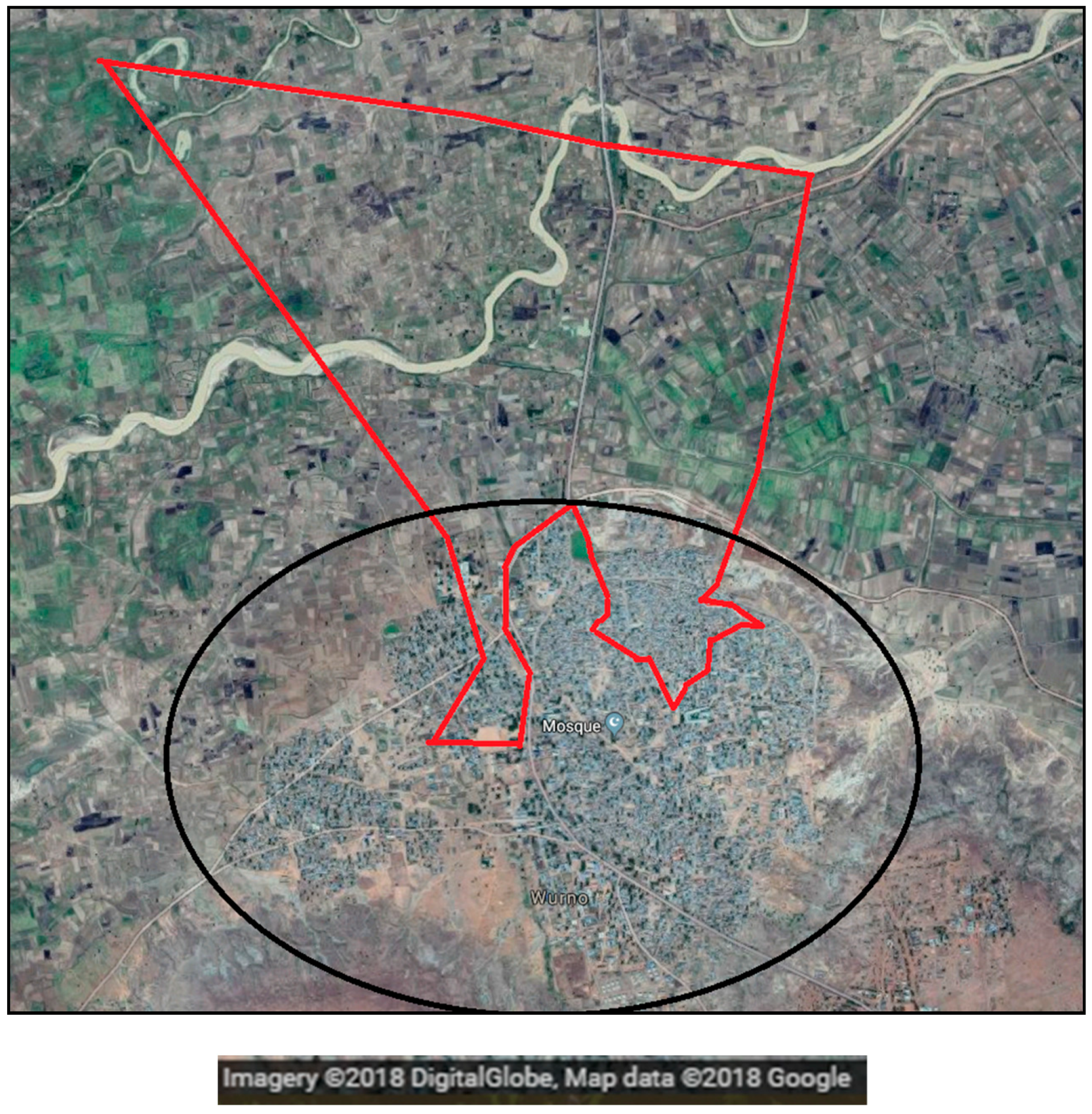
3.3. Location
3.4. Mapping
3.5. Enumeration Units
3.5.1. Building
3.5.2. Dwelling
3.5.3. Household
3.5.4. Household Member
3.6. Data Collection Tool
3.7. Enumeration Procedures
3.8. Data Quality Checks
3.8.1. Pre-Implementation Phase
3.8.2. Implementation Phase
3.8.3. Post-Implementation Phase
3.9. Data Analysis
4. Discussion
4.1. Summary of Findings
4.2. Comparisons
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A

References
- Demographic and Health Survey. Nigeria. 2013. Available online: https://www.dhsprogram.com/pubs/pdf/FR293/FR293.pdf (accessed on 6 August 2018).
- United Nations Children’s Fund. Nigeria: Multiple Indicator Cluster Survey 2016–17, Survey Findings Report. Available online: https://www.unicef.org/nigeria/resources_11701.html (accessed on 3 March 2018).
- WHO/UNICEF Estimated National Immunization Coverage. Data, Statistics and Graphics. Available online: http://www.who.int/immunization/monitoring_surveillance/data/en/ (accessed on 5 April 2018).
- National Health Management Information System, Nigeria. District Health Information System 2. Available online: https://dhis2nigeria.org.ng/dhis/dhis-web-commons/security/login.action (accessed on 6 April 2018).
- Integrated Public Use Micro-Data Series—International. Nigeria. 2006. Available online: https://international.ipums.org/international/enum_materials.shtml (accessed on 6 April 2018).
- Geo-Referenced Infrastructure & Demographic Data for Development. GRID3. Available online: www.grid3.org (accessed on 4 March 2018).
- Alegana, V.A.; Atkinson, P.M.; Pezzulo, C.; Sorichetta, A.; Weiss, D.; Bird, T.; Erbach-Schoenberg, E.; Tatem, A.J. Fine resolution mapping of population age-structures for health and development applications. J. R. Soc. Interface 2015, 12, 20150073. [Google Scholar] [CrossRef] [PubMed]
- Bill and Melinda Gates Foundation. GeoPoDe: Geographic, Population and Demographic Data. Available online: http://geopode.world/ (accessed on 17 March 2018).
- Maxar Company. DigitalGlobe. 2018. Available online: https://www.digitalglobe.com/ (accessed on 16 May 2018).
- Oleribe, O.; Kumar, V.; Awosika-Olumo, A.; Taylor-Robinson, S.D. Individual and socioeconomic factors associated with childhood immunization coverage in Nigeria. Pan Afr. Med. J. 2017, 26, 220. [Google Scholar] [CrossRef] [PubMed]
- Ezeh, O.K. Trends and population-attributable risk estimates for predictors of early neonatal mortality in Nigeria, 2003–2013: A cross-sectional analysis. BMJ Open 2017, 7, e013350. [Google Scholar] [CrossRef] [PubMed]
- Adewemimo, A.; Kalter, H.D.; Perin, J.; Koffi, A.K.; Quinley, J.; Black, R.E. Direct estimates of cause-specific mortality fractions and rates of under-five deaths in the northern and southern regions of Nigeria by verbal autopsy interview. PLoS ONE 2017, 12, e0178129. [Google Scholar] [CrossRef] [PubMed]
- Esri. ArcGIS. 2018. Available online: https://www.arcGeoPoDe.com/features/index.html (accessed on 16 April 2018).
- MACEPA Developer Products. EpiSample. 2018. Available online: https://play.google.com/store/apps/details?id=org.path.episample.android (accessed on 18 March 2018).
- World Health Organization. Handbook on Population and Housing—Census Editing Revision 1. Available online: https://unstats.un.org/unsd/publication/SeriesF/seriesf_82rev1e.pdf (accessed on 4 March 2018).
- 2019 ODK Community. Open Data Kit. 2019. Available online: https://opendatakit.org/software/ (accessed on 16 May 2018).
- Michael, C.A.; Waziri, N.E.; Gunnala, R.; Biya, O.; Kretsinger, K.; Wiesen, E.; Goodson, J.L.; Esapa, L.; Gidado, S.; Uba, B.; et al. Polio Legacy in Action: Using the Polio Eradication Infrastructure for Measles Elimination in Nigeria—The National Stop Transmission of Polio Program. J. Infect. Dis. 2017, 216, S373–S379. [Google Scholar] [CrossRef] [PubMed]
- Nigeria Centre for Disease Control. NFELTP. Available online: https://ncdc.gov.ng/training/nfeltp (accessed on 26 November 2018).
- Demographic and Health Survey. Evidence of Omission and Displacement in DHS Birth History. Available online: https://dhsprogram.com/pubs/pdf/MR11/MR11.pdf (accessed on 9 August 2018).
- World Health Organization. Principles and Recommendations for Population and Housing Censuses, Revision 3. 2014. Available online: https://unstats.un.org/unsd/demographic/meetings/egm/NewYork/2014/P&R_Revision3.pdf (accessed on 4 March 2018).
- Pardeshi, G.S. Age heaping and accuracy of age data collected during a community survey in the Yavatmal District, Maharashtra. Indian J. Community Med. 2010, 35, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, B.J.; Jedy-Agba, E.; Oga, E.; Adebamowo, C. Age Heaping and Cancer Rate Estimation in Nigeria; Working Paper 2013-03; Minnesota Population Centre: Minneapolis, MN, USA, 2013. [Google Scholar]
- Poy, A.; Masresha, B.; Shaba, K.; Katsande, R.; Weldegebriel, G.; Anya, B.; Okeibunor, J.; Mihigo, R.; Gasasira, A.; Nshimirimana, D. Immunization monitoring and vaccine-preventable diseases surveillance data management in the African Region. Afr. Health Monit. 2015, 1, 46–50. [Google Scholar]
- Gimbel, S.; Mwanza, M.; Nisingizwe, M.P.; Michel, C.; Hirschhorn, L. Improving data quality across 3 sub-Saharan African countries using the consolidated framework for implementation research (CFIR): Results from the African health initiative. BMC Health Serv. Res. 2017, 17, 828. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, J.; Argeseanu, C.S.; Eeckels, R.; Herbst, K. Data cleaning: Detecting, diagnosing, and editing data abnormalities. PLoS Med. 2005, 2, e267. [Google Scholar] [CrossRef] [PubMed]
- Kamadjeu, R. Tracking the polio virus down the Congo River: A case study on the use of Google Earth™ in public health planning and mapping. Int. J. Health Geogr. 2009, 8, 4. [Google Scholar] [CrossRef] [PubMed]
- Pindolia, D.; Garcia, A.; Huang, Z.; Smith, D.; Alegana, V.; Noor, A.M.; Snow, R.W.; Tatem, A.J. The demographics of human and malaria movement and migration patterns in East Africa. Malar. J. 2013, 12, 397. [Google Scholar] [CrossRef] [PubMed]
- Utazi, C.E.; Thorley, J.; Alegana, V.; Ferrari, M.J.; Takahashi, S.; Metcalf, C.J.; Lessles, J.; Tatem, A.J. High resolution age-structured mapping of childhood vaccination coverage in low and middle income countries. Vaccine 2018, 36, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Tatem, A.J.; Campbell, J.; Guerra-Arias, M.; de Bernis, L.; Moran, A.; Matthews, Z. Mapping for maternal and newborn health: The distributions of women of childbearing age, pregnancies and births. Int. J. Health Geogr. 2014, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Bailey, M.; Makannah, T.J. An evaluation of age and sex data of the population censuses of Sierra Leone: 1963–1985. Genus 1996, 52, 191–199. [Google Scholar] [PubMed]
- Mukherjee, B.N.; Mukhopadhyay, B.K. A study of digit preference and quality of age data in Turkish censuses. Genus 1988, 44, 201–227. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Settlement. | Total Population | Under 1 Year | Under5 Years | Under 15 Years | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Unknown | 142 | 1 | 0.7 | 25 | 1.6 | 66 | 1.6 |
| Akalawa | 994 | 28 | 1.8 | 183 | 11.4 | 487 | 11.4 |
| Alkanci | 143 | 3 | 2.1 | 33 | 2.1 | 77 | 1.8 |
| Barkiya | 135 | 4 | 3.0 | 19 | 1.2 | 64 | 1.5 |
| Dafkawa | 223 | 9 | 3.6 | 48 | 3.0 | 108 | 2.5 |
| Dawarawa | 72 | 4 | 5.6 | 15 | 1.0 | 35 | 0.8 |
| Dutsin | 226 | 5 | 2.2 | 52 | 3.3 | 113 | 2.7 |
| Gida Garka | 17 | 0 | 0.0 | 4 | 0.3 | 6 | 0.1 |
| Gida Kofar Giwa | 95 | 2 | 2.1 | 18 | 1.1 | 50 | 1.2 |
| Giwa A | 571 | 21 | 2.5 | 96 | 6.0 | 284 | 6.7 |
| Giwa B | 130 | 3 | 0.0 | 17 | 1.1 | 59 | 1.4 |
| Halidawa | 238 | 8 | 0.8 | 47 | 2.9 | 119 | 2.8 |
| Hubbare | 22 | 1 | 4.6 | 5 | 0.3 | 8 | 0.2 |
| Madacci | 60 | 1 | 1.7 | 7 | 0.4 | 23 | 0.5 |
| Magaryawa | 1,271 | 24 | 1.3 | 203 | 12.7 | 602 | 14.1 |
| Magina | 214 | 6 | 2.8 | 43 | 2.7 | 108 | 2.5 |
| Sabo Gari | 26 | 0 | 0.0 | 7 | 0.4 | 13 | 0.3 |
| Sagi | 146 | 3 | 1.4 | 19 | 1.2 | 80 | 1.9 |
| Sarkawa | 538 | 20 | 3.2 | 107 | 6.7 | 265 | 6.2 |
| Sarkindoka A | 1,563 | 52 | 2.3 | 326 | 20.4 | 791 | 18.5 |
| Sarkindoka B | 705 | 15 | 2.1 | 138 | 8.6 | 379 | 8.9 |
| Sarkinruwa | 363 | 12 | 3.3 | 65 | 4.1 | 188 | 4.4 |
| Sarkinwanki | 120 | 2 | 0.8 | 14 | 0.9 | 50 | 1.2 |
| Shiya Mai Gaza | 48 | 1 | 2.1 | 10 | 0.6 | 21 | 0.5 |
| Shiya Sage | 246 | 9 | 3.7 | 48 | 3.0 | 128 | 3.0 |
| Wurno General Hospital | 71 | 0 | 0.0 | 5 | 0.3 | 30 | 0.7 |
| Yardutse | 222 | 6 | 2.3 | 45 | 2.8 | 117 | 2.7 |
| Total | 8601 | 240 | 2.8 | 1599 | 18.6 | 4271 | 49.7 |
| Settlements | Micro-Census Count | EOC House-to-House Count | Demand Generation Count | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Unknown | 1 | 0.7 | ||||
| Akalawa | 28 | 1.8 | 84 | 2.6 | ||
| Alkanci | 3 | 2.1 | ||||
| Barkiya | 4 | 3.0 | 24 | 1.5 | ||
| Dafkawa | 9 | 3.6 | 19 | 0.9 | ||
| Dawarawa | 4 | 5.6 | 18 | 2.1 | ||
| Dutsin | 5 | 2.2 | 19 | 2.6 | ||
| Gida Garka | 0 | 0.0 | ||||
| Gida Kofar Giwa | 2 | 2.1 | ||||
| Giwa A | 21 | 2.5 | 20 | 3.8 | ||
| Giwa B | 3 | 0.1 | 10 | 0.6 | ||
| Halidawa | 8 | 0.8 | 55 | 2.5 | ||
| Hubbare | 1 | 4.6 | 3 | 1.1 | ||
| Madacci | 1 | 1.7 | ||||
| Magaryawa | 24 | 1.3 | 24 | 2.8 | ||
| Magina | 6 | 2.8 | 11 | 0.7 | ||
| Sabo Gari | 0 | 0.0 | ||||
| Sagi | 3 | 1.4 | ||||
| Sarkawa | 20 | 3.2 | 11 | 1.5 | ||
| Sarkindoka A | 52 | 2.3 | 55 | 1.1 | ||
| Sarkindoka B | 15 | 2.1 | 4 | 0.6 | ||
| Sarkinruwa | 12 | 3.3 | 1 | 0.1 | ||
| Sarkinwanki | 2 | 0.8 | 7 | 2.8 | ||
| Shiyar Mai Gaza | 1 | 2.1 | ||||
| Shiyar Sage | 9 | 3.7 | 25 | 2.0 | ||
| Wurno General Hospital | 0 | 0.0 | ||||
| Yardutse | 6 | 2.3 | 6 | 0.4 | ||
| Total | 240 | 2.8 | 396 | 1.5 | 238 | |
| Settlements | Micro-Census Count | EOC House-to-House Count | ||
|---|---|---|---|---|
| N | % | N | % | |
| Unknown | 25 | 1.6 | ||
| Akalawa | 183 | 11.4 | 261 | 7.9 |
| Alkanci | 33 | 2.1 | ||
| Barkiya | 19 | 1.2 | 187 | 11.3 |
| Dafkawa | 48 | 3.0 | 240 | 11.4 |
| Dawarawa | 15 | 1.0 | 153 | 17.5 |
| Dutsin | 52 | 3.3 | 85 | 11.8 |
| Gida Garka | 4 | 0.3 | ||
| Gida Kofar Giwa | 18 | 1.1 | ||
| Giwa A | 96 | 6.0 | 63 | 12.1 |
| Giwa B | 17 | 1.1 | 122 | 7.7 |
| Halidawa | 47 | 2.9 | 187 | 8.5 |
| Hubbare | 5 | 0.3 | 28 | 10.6 |
| Madacci | 7 | 0.4 | ||
| Magaryawa | 203 | 12.7 | 60 | 6.9 |
| Magina | 43 | 2.7 | 171 | 10.6 |
| Sabo Gari | 7 | 0.4 | ||
| Sagi | 19 | 1.2 | ||
| Sarkawa | 107 | 6.7 | 81 | 11.1 |
| Sarkindoka A | 326 | 20.4 | 491 | 9.9 |
| Sarkindoka B | 138 | 8.6 | 77 | 11.2 |
| Sarkinruwa | 65 | 4.1 | 80 | 7.3 |
| Sarkinwanki | 14 | 0.9 | 70 | 28.0 |
| Shiya Mai Gaza | 10 | 0.6 | ||
| Shiya Sage | 48 | 3.0 | 90 | 7.1 |
| Wurno General Hospital | 5 | 0.3 | ||
| Yardutse | 45 | 2.8 | 100 | 6.6 |
| Total | 1599 | 18.6 | 2546 | 9.7 |
| Settlements | Micro-Census Count | EOC House-to-House Count | ||
|---|---|---|---|---|
| N | % | N | % | |
| Unknown | 66 | 1.6 | ||
| Akalawa | 487 | 11.4 | 657 | 20.0 |
| Alkanci | 77 | 1.8 | ||
| Barkiya | 64 | 1.5 | 331 | 20.0 |
| Dafkawa | 108 | 2.5 | 421 | 20.0 |
| Dawarawa | 35 | 0.8 | 175 | 20.0 |
| Dutsin | 113 | 2.7 | 144 | 20.0 |
| Gida Garka | 6 | 0.1 | ||
| Gida Kofar Giwa | 50 | 1.2 | 255 | 20.0 |
| Giwa A | 284 | 6.7 | 104 | 20.0 |
| Giwa B | 59 | 1.4 | 317 | 20.0 |
| Halidawa | 119 | 2.8 | 441 | 20.0 |
| Hubbare | 8 | 0.2 | 53 | 20.0 |
| Madacci | 23 | 0.5 | ||
| Magaryawa | 602 | 14.1 | 174 | 20.0 |
| Magina | 108 | 2.5 | 322 | 20.0 |
| Sabo Gari | 13 | 0.3 | ||
| Sagi | 80 | 1.9 | ||
| Sarkawa | 265 | 6.2 | 146 | 20.0 |
| Sarkindoka A | 791 | 18.5 | 990 | 20.0 |
| Sarkindoka B | 379 | 8.9 | 138 | 20.0 |
| Sarkinruwa | 188 | 4.4 | 220 | 20.0 |
| Sarkinwanki | 50 | 1.2 | 50 | 20.0 |
| Shiyar Mai Gaza | 21 | 0.5 | ||
| Shiyar Sage | 128 | 3.0 | ||
| Wurno General Hospital | 30 | 0.7 | ||
| Yardutse | 117 | 2.7 | 303 | 20.0 |
| Total | 4271 | 49.7 | 5241 | 20.0 |
| Micro-Census Count | GeoPoDe Estimate | 2006 Census Projections | EOC House-to-House Estimate |
|---|---|---|---|
| 8601 | 8708 | 16,994 | 26,205 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghiselli, M.E.; Wilson, I.N.; Kaplan, B.; Waziri, N.E.; Sule, A.; Ayanleke, H.B.; Namalam, F.; Tambuwal, S.A.; Aliyu, N.; Kadi, U.; et al. Comparison of Micro-Census Results for Magarya Ward, Wurno Local Government Area of Sokoto State, Nigeria, with Other Sources of Denominator Data. Data 2019, 4, 20. https://doi.org/10.3390/data4010020
Ghiselli ME, Wilson IN, Kaplan B, Waziri NE, Sule A, Ayanleke HB, Namalam F, Tambuwal SA, Aliyu N, Kadi U, et al. Comparison of Micro-Census Results for Magarya Ward, Wurno Local Government Area of Sokoto State, Nigeria, with Other Sources of Denominator Data. Data. 2019; 4(1):20. https://doi.org/10.3390/data4010020
Chicago/Turabian StyleGhiselli, Margherita E., Idongesit Nta Wilson, Brian Kaplan, Ndadilnasiya Endie Waziri, Adamu Sule, Halimatu Bolatito Ayanleke, Faruk Namalam, Shehu Ahmad Tambuwal, Nuruddeen Aliyu, Umar Kadi, and et al. 2019. "Comparison of Micro-Census Results for Magarya Ward, Wurno Local Government Area of Sokoto State, Nigeria, with Other Sources of Denominator Data" Data 4, no. 1: 20. https://doi.org/10.3390/data4010020
APA StyleGhiselli, M. E., Wilson, I. N., Kaplan, B., Waziri, N. E., Sule, A., Ayanleke, H. B., Namalam, F., Tambuwal, S. A., Aliyu, N., Kadi, U., Bolu, O., Barau, N., Yahaya, M., Ugbenyo, G., Osigwe, U., Oguji, C., Usifoh, N., & Seaman, V. (2019). Comparison of Micro-Census Results for Magarya Ward, Wurno Local Government Area of Sokoto State, Nigeria, with Other Sources of Denominator Data. Data, 4(1), 20. https://doi.org/10.3390/data4010020