
Hypoglycemia after Mitral Valve Repair in Dogs

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dogs
2.2. Mitral Valve Repair [10,12,13]
2.3. Cardiopulmonary Bypass [12,13]
2.4. Blood Sampling
2.5. Blood Biochemical Data
2.6. Statistical Analysis
3. Results
3.1. Dogs
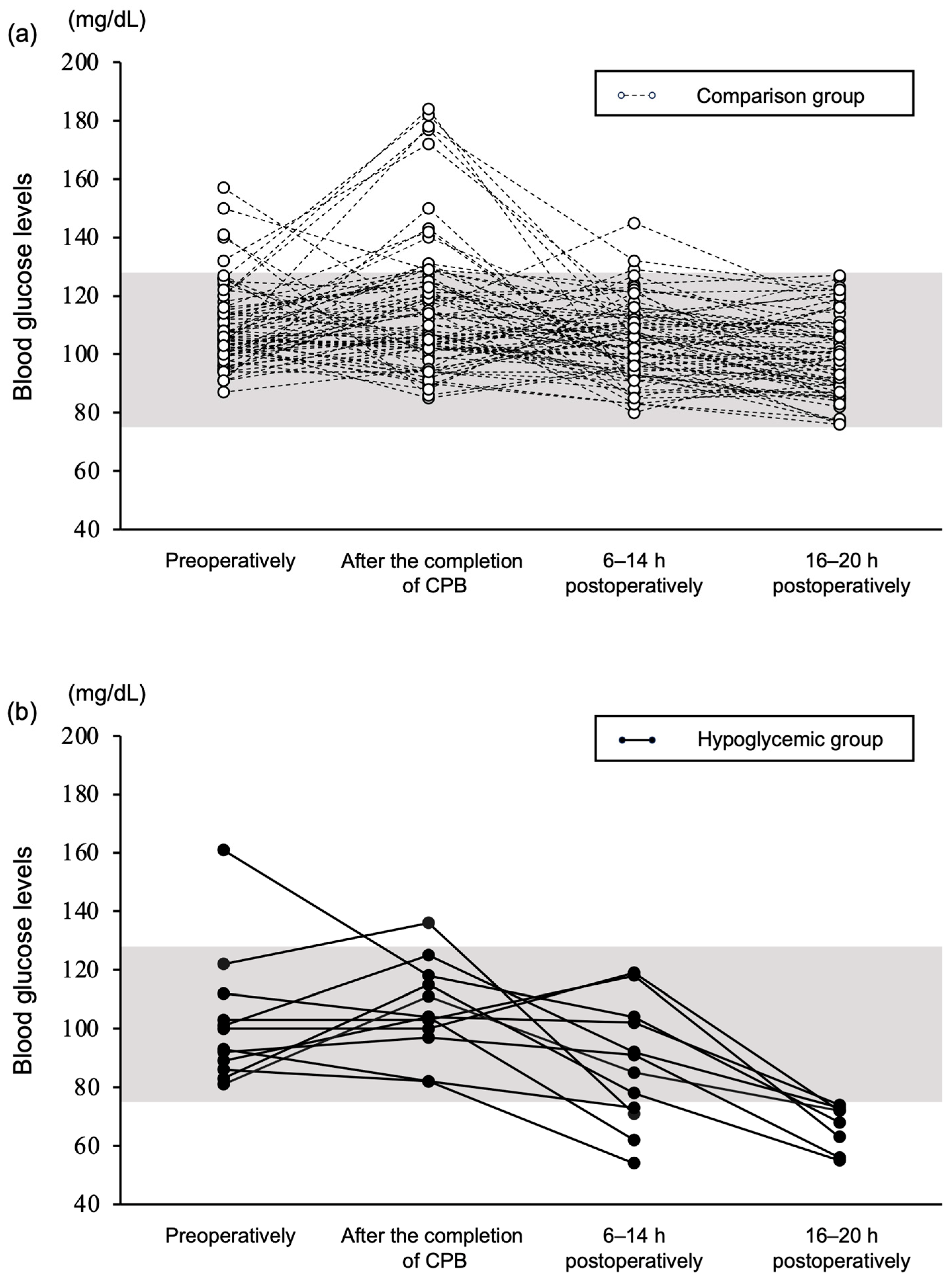
3.2. Blood Glucose Levels
3.3. Insulin, Glucagon, and Insulin/Glucagon Ratio
3.4. Risk Factors of Hypoglycemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McDonnell, M.E.; Guillermo, E.U. Insulin therapy for the management of hyperglycemia in hospitalized patients. Endocrinol. Metabol. Clin. 2012, 41, 175–201. [Google Scholar] [CrossRef] [PubMed]
- McCowen, K.C.; Malhotra, A.; Bruce, R. Stress-induced hyperglycemia. Crit. Care Clin. 2001, 17, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Ban, K.A.; Minei, J.P.; Laronga, C.; Harbrecht, B.G.; Jensen, E.H.; Fry, D.E.; Itani, K.M.; Dellinger, E.P.; Ko, C.Y.; Duane, T.M. American College of Surgeons and Surgical Infection Society: Surgical site infection guidelines, 2016 update. J. Am. Coll. Surg. 2017, 224, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Berríos-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for Disease Control and Prevention guideline for the prevention of surgical site infection. J. Am. Med. Assoc. Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef]
- Criado, A.; Dominguez, E.; Carmona, J.; Gomez-Arnau, J.; Avello, F. Hypoglycemic coma after cardiac surgery. Crit. Care Med. 1984, 12, 409–410. [Google Scholar] [CrossRef] [PubMed]
- Kurian, J.; Raul, V. Profound postoperative hypoglycemia in a malnourished patient. Can. J. Anesth. 2001, 48, 881–883. [Google Scholar] [CrossRef]
- Del Busto, I.; German, A.J.; Treggiari, E.; Romanelli, G.; O’Connell, E.M.; Batchelor, D.J.; Silvestrini, P.; Murtagh, K. Incidence of postoperative complications and outcome of 48 dogs undergoing surgical management of insulinoma. J. Vet. Intern. Med. 2020, 34, 1135–1143. [Google Scholar] [CrossRef]
- Veytsman, S.; Amsellem, P.; Husbands, B.D.; Rendahl, A.K.; Bergman, P.J.; Chanoit, G.; Hickey, C.; Cash, K.R.; Maritato, K.C.; Collivignarelli, F.; et al. Retrospective study of 20 cats surgically treated for insulinoma. Vet. Surg. 2023, 52, 42–50. [Google Scholar] [CrossRef]
- Holford, A.L.; Tobias, K.M.; Bartges, J.W.; Johnson, B.M. Adrenal response to adrenocorticotropic hormone in dogs before and after surgical attenuation of a single congenital portosystemic shunt. J. Vet. Intern. Med. 2008, 22, 832–838. [Google Scholar] [CrossRef]
- Mizuno, M.; Uechi, M. Mitral valve annuloplasty and chordal replacement in dogs. J. Vet. Cardiol. 2020, 4, 1–7. [Google Scholar] [CrossRef]
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Uechi, M.; Mizukoshi, T.; Mizuno, T.; Mizuno, M.; Harada, K.; Ebisawa, T.; Takeuchi, J.; Sawada, T.; Uchida, S.; Shinoda, A.; et al. Mitral valve repair under cardiopulmonary bypass in small-breed dogs: 48 cases (2006–2009). J. Am. Vet. Med. Assoc. 2012, 240, 1194–1201. [Google Scholar] [CrossRef] [PubMed]
- Uechi, M. Mitral valve repair in dogs. J. Vet. Cardiol. 2012, 14, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Suchowersky, N.D.; Carlson, E.A.; Lee, H.P.; Ellen, N.B. Comparison of glucose concentrations in canine whole blood, plasma, and serum measured with a veterinary point-of-care glucometer. J. Vet. Diag. Investig. 2021, 33, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Fracassi, F. Canine diabetes mellitus. In Textbook of Veterinary Internal Medicine, 8th ed.; Ettinger, S.J., Feldman, E.C., Côté, E., Eds.; Elsevier: St. Louis, MO, USA, 2017; pp. 1767–1781. [Google Scholar]
- Koenig, A. Hypoglycemia. In Small Animal Critical Care Medicine, 1st ed.; Hopper, K.H., Silverstein, D.C., Eds.; Saunders Elsevier: St. Louis, MO, USA, 2009; pp. 295–298. [Google Scholar]
- Ineson, D.L.; Freeman, L.M.; Rush, J.E. Clinical and laboratory findings and survival time associated with cardiac cachexia in dogs with congestive heart failure. J. Vet. Intern. Med. 2019, 33, 1902–1908. [Google Scholar] [CrossRef] [PubMed]
- Kongsayreepong, S.; Chaibundit, C.; Chadpaibool, J.; Komoltri, C.; Suraseranivongse, S.; Suwannanonda, P.; Raksamanee, E.O.; Noocharoen, P.; Silapadech, A.; Parakkamodom, S.; et al. Predictor of core hypothermia and the surgical intensive care unit. Anesth. Analg. 2003, 96, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Redondo, J.I.; Suesta, P.; Serra, C.I.; Soler, G.; Soler, L.G.; Gómez-Villamandos, R.J. Retrospective study of the prevalence of postanaesthetic hypothermia in dogs. Vet. Rec. 2012, 171, 374. [Google Scholar] [CrossRef] [PubMed]
- Kleiber, M. Body size and metabolic rate. Physiol. Rev. 1947, 27, 511–541. [Google Scholar] [CrossRef]
- Quesada-López, T.; Villarroya, F. Obesity and thermogenic adipose tissue plasticity in dogs. Vet. México OA 2023, 10. [Google Scholar] [CrossRef]
- Hamlin, R.L. Pathophysiology of heart failure. In Textbook of Canine and Feline Cardiology: Principles and Clinical Practice, 2nd ed.; Fox, P.R., Sisson, D., Moïse, N.S., Eds.; W. B. Saunders Company: Philadelphia, PA, USA, 1999; pp. 205–215. [Google Scholar]
- Marcondes, S.M.; Strunz, C.M.; Larsson, M.H. Correlation between activation of the sympathetic nervous system estimated by plasma concentrations of norepinephrine and Doppler echocardiographic variables in dogs with acquired heart disease. Am. J. Vet. Res. 2006, 67, 1163–1168. [Google Scholar] [CrossRef]
- Anand, I.S.; Ferrari, R.; Kalra, G.S.; Wahi, P.L.; Poole-Wilson, P.A.; Harris, P.C. Edema of cardiac origin. Studies of body water and sodium, renal function, hemodynamic indexes, and plasma hormones in untreated congestive cardiac failure. Circulation 1989, 80, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Aroor, A.R.; Mandavia, C.H.; Sowers, J.R. Insulin resistance and heart failure: Molecular mechanisms. Heart Fail. Clin. 2012, 8, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Prichard, B.N.; Owens, C.W.; Woolf, A.S. Adverse reactions to diuretics. Eur. Heart J. 1992, 13 (Suppl. G), 96–103. [Google Scholar] [CrossRef] [PubMed]
- Keller, N.; Jacobson, L.S.; Nel, M.; de Clerq, M.; Thompson, P.N.; Schoeman, J.P. Prevalence and risk factors of hypoglycemia in virulent canine babesiosis. J. Vet. Int. Med. 2004, 18, 265–270. [Google Scholar] [CrossRef]
- Fitton, A.; Brogden, R.N. Pimobendan. A review of its pharmacology and therapeutic potential in congestive heart failure. Drugs Aging. 1994, 4, 417–441. [Google Scholar] [CrossRef] [PubMed]
- Keck, F.S.; Foldenauer, A.; Zeller, G.; Wolf, C.; Loos, U.; Pfeiffer, E. Comparative effects of dopamine and dobutamine on glucoregulation in a rat model. Can. J. Physiol. Pharmacol. 1991, 69, 1178–1183. [Google Scholar] [CrossRef]
- Liang, C.S.; Hood, W.B. Dobutamine infusion in conscious dogs with and without autonomic nervous system inhibition: Effects on systemic hemodynamics, regional blood flows and cardiac metabolism. J. Pharmacol. Experimental Therap. 1979, 211, 698–705. [Google Scholar]
- Abs, R.; Verhelst, J.; Maeyaert, J.; Van Buyten, J.P.; Opsomer, F.; Adriaensen, H.; Verlooy, J.; Van Havenbergh, T.; Smet, M.; Van Acker, K. Endocrine consequences of long-term intrathecal administration of opioids. J. Clin. Endocrinol. Metab. 2000, 85, 2215–2222. [Google Scholar] [CrossRef]
- Nelson, R.W. Endocrine disorders. In Small Animal Internal Medicine, 5th ed.; Nelson, R.W., Couto, C.G., Eds.; Mosby Elsevier: St. Louis, MO, USA, 2013; pp. 777–823. [Google Scholar]
- Beaudry, D.; Knapp, D.W.; Montgomery, T.; Sandusky, G.S.; Morrison, W.B.; Nelson, R.W. Hypoglycemia in four dogs with smooth muscle tumors. J. Vet. Intern. Med. 1995, 9, 415–418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Hypoglycemic (n = 12) | Comparison (n = 72) |
|---|---|---|
| Age (years) | 10 (2) | 10 (2) |
| Body weight (kg) | 2.4 (2.2–2.7) | 4.1 (3.1–5.8) |
| Sex (F/FS/M/MC) | (0/6/1/5) | (3/27/11/31) |
| MMVD severity (asymptomatic/symptomatic) | (7/5) | (20/52) |
| BCS (1–9) | 5 (5–6) | 5 (4–6) |
| MCS (1–4) | 4 (4–4) | 4 (3–4) |
| Characteristics | Hypoglycemic (n = 12) | Comparison (n = 72) |
|---|---|---|
| Allogeneic blood transfusion (yes/no) | 9/3 | 20/52 |
| Blood collection for autologous blood transfusion (yes/no) | 6/6 | 61/11 |
| Autologous washed RBC transfusion (yes/no) | 3/9 | 16/56 |
| Postoperative opioid utilization (yes/no) | 11/1 | 58/14 |
| Hemodilution rate (%) | 36.7 (35.7–40.7) | 30.5 (7.3) |
| In–out fluid balance during CPB (mL/kg) | 49.6 (25.0) | 27.7 (19.1–42.3) |
| CPB time (min) | 78 (74–81) | 82 (75–92) |
| Cardiac arrest time (min) | 47 (43–53) | 51 (46–58) |
| Time under anesthesia (min) | 200 (31) | 210 (195–235) |
| Characteristics | p-Value | VIF | Adjusted VIF |
|---|---|---|---|
| Age | 0.488 | - | - |
| Body weight | 0.009 * | 6.835 | 2.229 |
| Sex | 0.333 | - | - |
| MMVD severity | 0.044 * | 1.110 | 1.098 |
| BCS | 0.570 | - | - |
| MCS | 0.109 * | 1.263 | 1.085 |
| Allogeneic blood transfusion | 0.004 * | 1.581 | 1.546 |
| Blood collection for autologous blood transfusion | 0.010 * | 1.624 | 1.621 |
| Autologous washed RBC transfusion | 0.831 | - | - |
| Postoperative opioids | 0.369 | - | - |
| Preoperative blood glucose levels | 0.135 * | 1.231 | 1.064 |
| Preoperative serum insulin concentrations | 0.099 * | 5.378 | 1.283 |
| Preoperative plasma glucagon concentrations | 0.592 | - | - |
| Preoperative I/G ratio | 0.158 * | 4.776 | - |
| Hemodilution rate | 0.012 * | 4.566 | - |
| In–out fluid balance during CPB | 0.058 * | 1.790 | 1.686 |
| CPB time | 0.208 | - | - |
| Cardiac arrest time | 0.084 * | 2.100 | 1.899 |
| Time under anesthesia | 0.122 * | 1.575 | 1.565 |
| Characteristics | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|
| Body weight | 0.288 | 0.115–0.720 | 0.008 * |
| MMVD severity, symptomatic (vs. asymptomatic) | 0.183 | 0.043–0.788 | 0.023 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nii, Y.; Takahashi, E.; Tabata, M.; Furusato, S.; Katsumata, M.; Uechi, M. Hypoglycemia after Mitral Valve Repair in Dogs. Vet. Sci. 2024, 11, 79. https://doi.org/10.3390/vetsci11020079
Nii Y, Takahashi E, Tabata M, Furusato S, Katsumata M, Uechi M. Hypoglycemia after Mitral Valve Repair in Dogs. Veterinary Sciences. 2024; 11(2):79. https://doi.org/10.3390/vetsci11020079
Chicago/Turabian StyleNii, Yasuyuki, Emi Takahashi, Miho Tabata, Shimon Furusato, Masaya Katsumata, and Masami Uechi. 2024. "Hypoglycemia after Mitral Valve Repair in Dogs" Veterinary Sciences 11, no. 2: 79. https://doi.org/10.3390/vetsci11020079
APA StyleNii, Y., Takahashi, E., Tabata, M., Furusato, S., Katsumata, M., & Uechi, M. (2024). Hypoglycemia after Mitral Valve Repair in Dogs. Veterinary Sciences, 11(2), 79. https://doi.org/10.3390/vetsci11020079