Assessment of Longitudinal Left Ventricle Deformation by 2-Dimensional Speckle Tracking Echocardiography Obtained from Different Views in Cats

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Standard Echocardiography
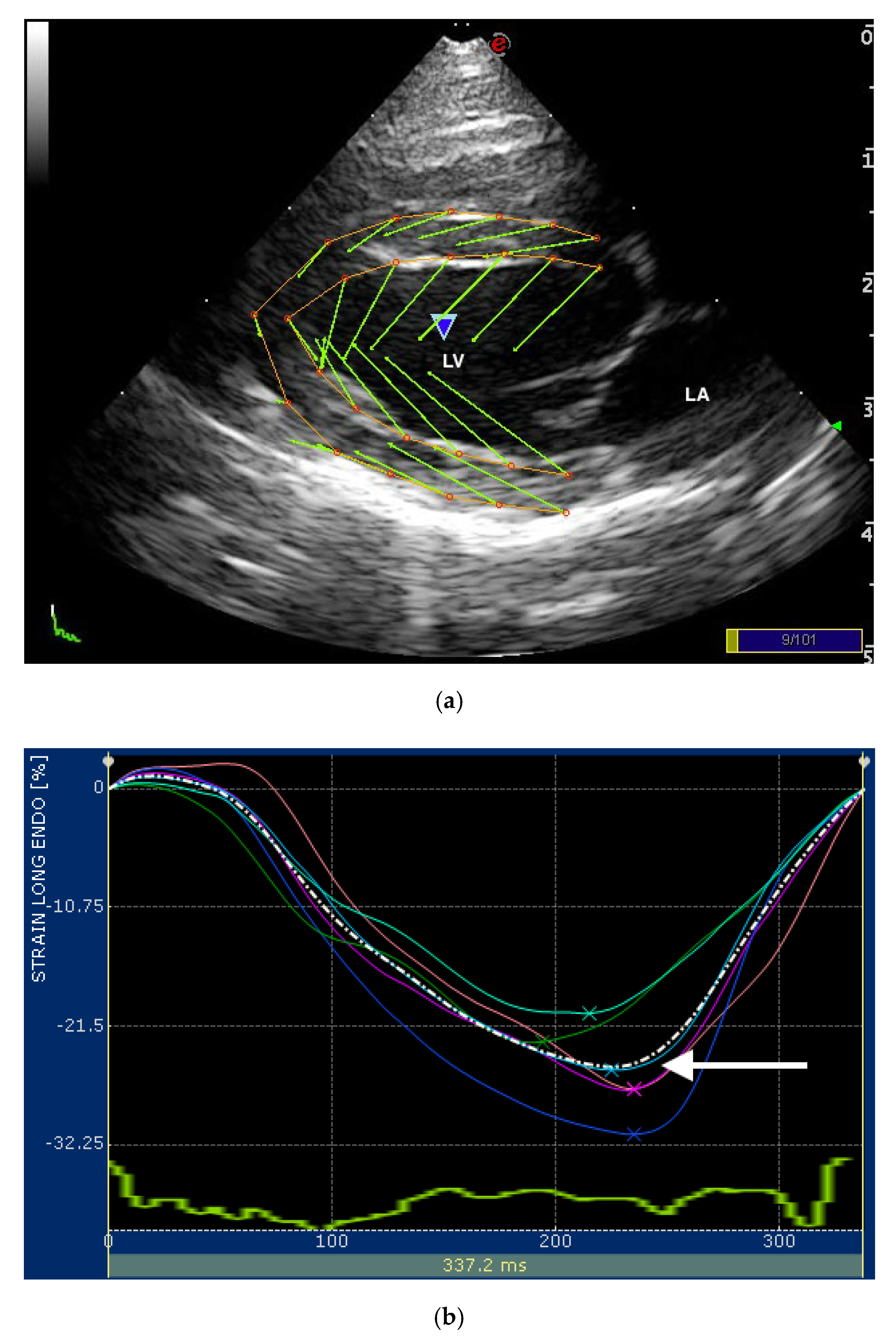
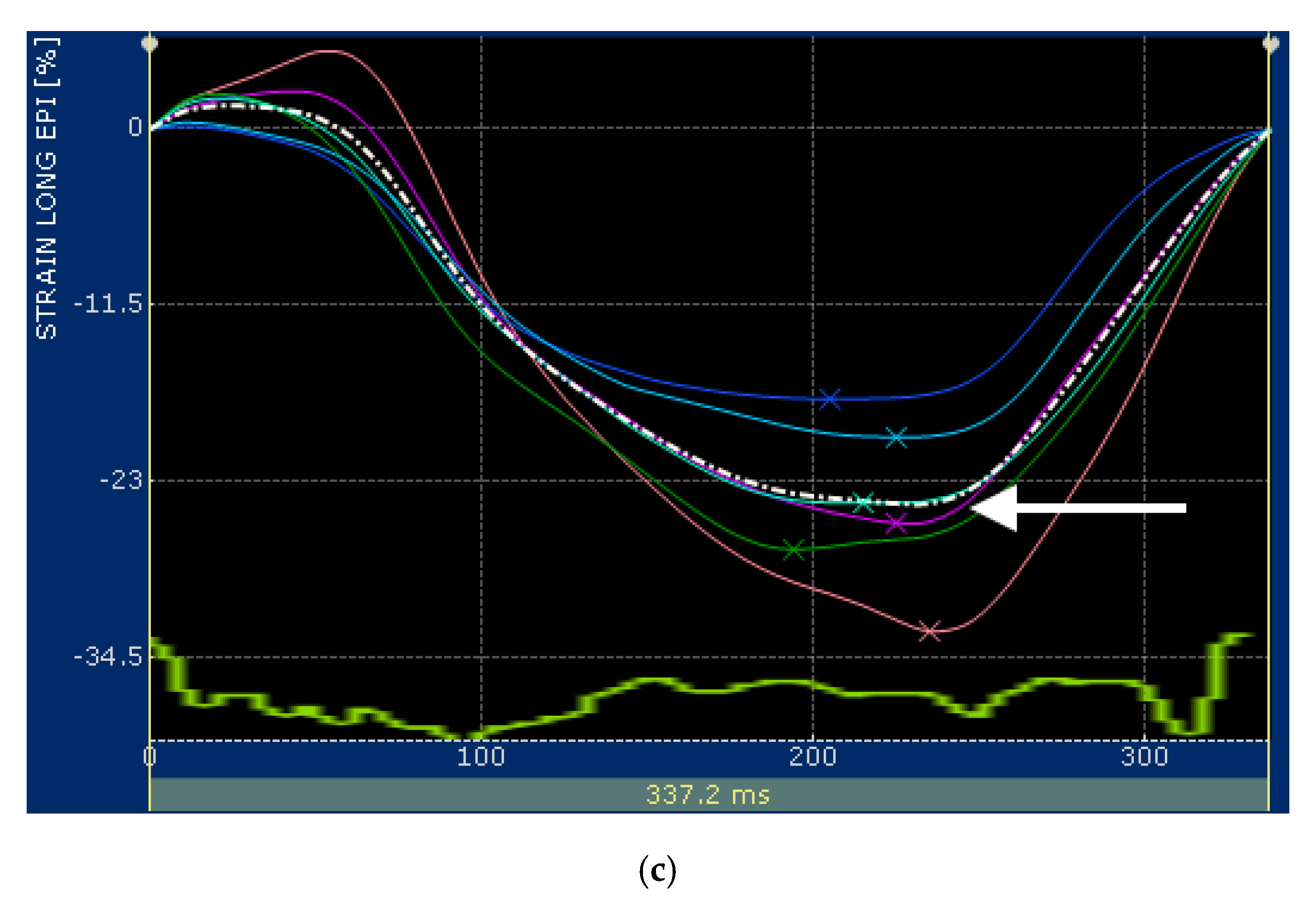
2.2. Speckle Tracking Echocardiography
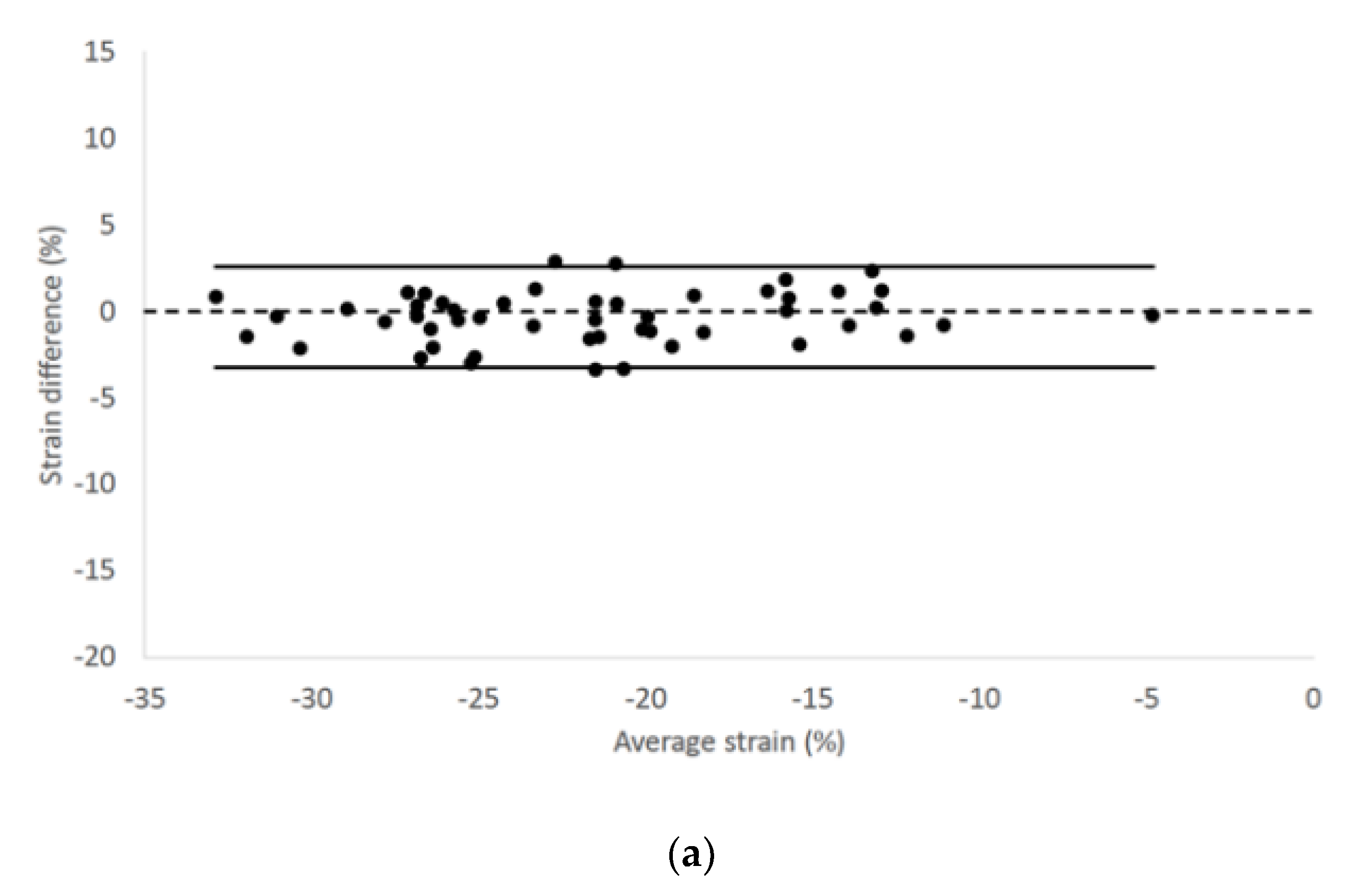
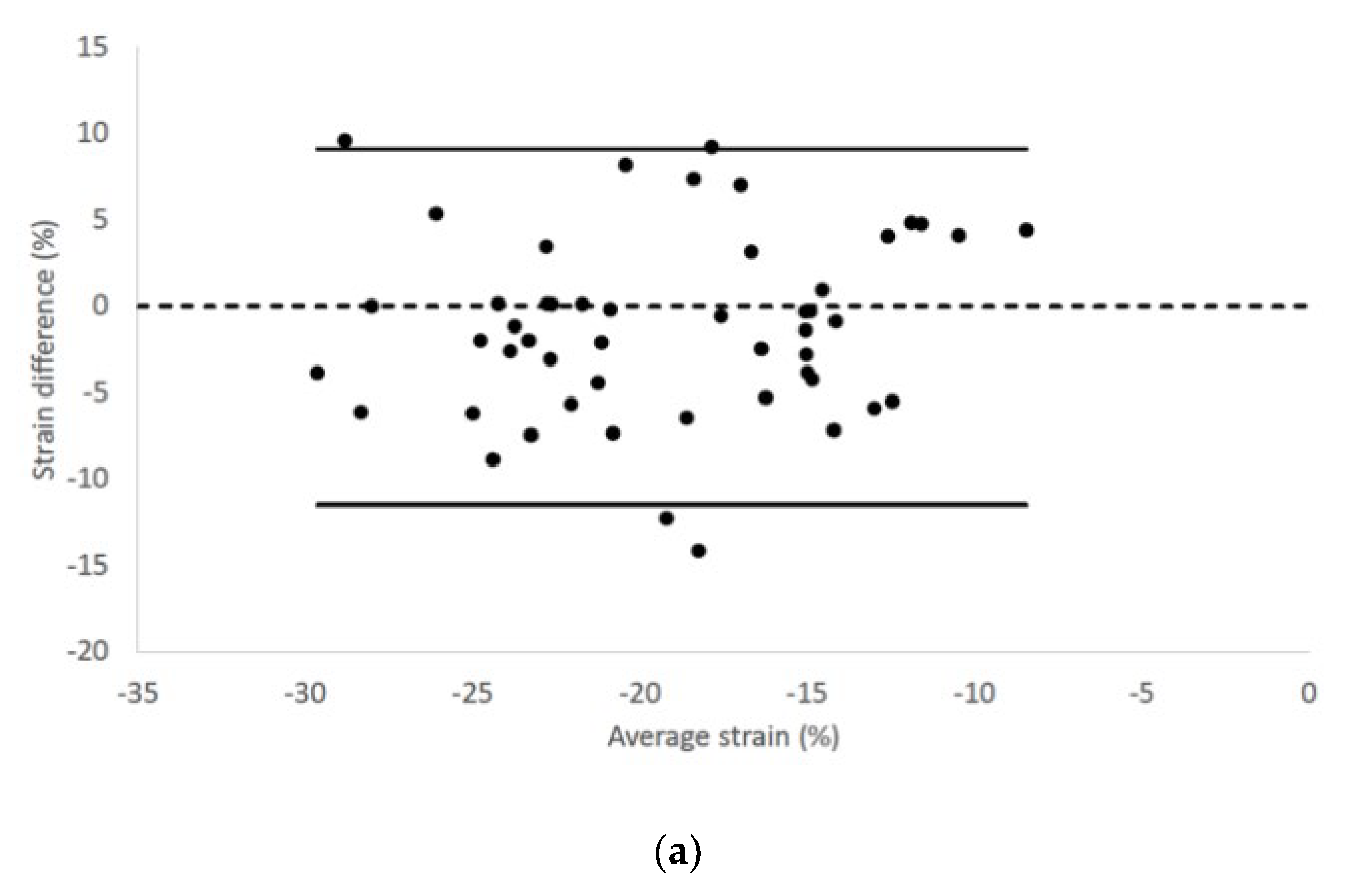
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mor-Avi, V.; Lang, R.M.; Badano, L.P.; Belohlavek, M.; Cardim, N.M.; Derumeaux, G.; Galderisi, M.; Marwick, T.; Nagueh, S.F.; Sengupta, P.P.; et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. Eur. J. Echocardiogr. 2011, 12, 167–205. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Phelan, D.; Klein, A. A test in context: Myocardial strain measured by speckle-tracking echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Fruganti, A.; Cerquetella, M.; Copponi, I.; Spaterna, A.; Tesei, B. Preliminary Evaluation of M-Mode, B-Mode, and X-Strain® Echocardiographic Indices Before and During Therapy in Dogs Affected by Dilated Cardiomyopathy. In Current Aspects in Biology, Animal Pathology, Clinic and Food Hygiene, 1st ed.; Pugliese, A., Gaiti, A., Boiti, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 1, pp. 97–102. [Google Scholar]
- Zois, N.E.; Tidholm, A.; Nägga, K.M.; Moesgaard, S.G.; Rasmussen, C.E.; Falk, T.; Häggström, J.; Pedersen, H.D.; Åblad, B.; Nilsen, H.Y.; et al. Radial and longitudinal strain and strain rate assessed by speckle-tracking echocardiography in dogs with myxomatous mitral valve disease. J. Vet. Intern. Med. 2012, 26, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Matsumoto, H.; Teshima, T.; Koyama, H. Clinical assessment of systolic myocardial deformations in dogs with chronic mitral valve insufficiency using two-dimensional speckle-tracking echocardiography. J. Vet. Cardiol. 2013, 15, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Pedro, B.; Stephenson, H.; Linney, C.; Cripps, P.; Dukes-McEwan, J. Assessment of left ventricular function in healthy Great Danes and in Great Danes with dilated cardiomyopathy using speckle tracking echocardiography. J. Vet. Cardiol. 2017, 19, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Spalla, I.; Locatelli, C.; Zanaboni, A.M.; Brambilla, P.; Bussadori, C. Echocardiographic assessment of cardiac function by conventional and speckle-tracking echocardiography in dogs with patent Ductus Arteriosus. J. Vet. Intern. Med. 2016, 30, 706–713. [Google Scholar] [CrossRef]
- Caivano, D.; Rishniw, M.; Birettoni, F.; Petrescu, V.F.; Porciello, F. Transverse Right Ventricle Strain and Strain Rate Assessed by 2-Dimensional Speckle Tracking Echocardiography in Dogs with Pulmonary Hypertension. Vet. Sci. 2020, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Caivano, D.; Rishniw, M.; Patata, V.; Giorgi, M.E.; Birettoni, F.; Porciello, F. Left atrial deformation and phasic function determined by 2-dimensional speckle tracking echocardiography in healthy dogs. J. Vet. Cardiol. 2016, 18, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Caivano, D.; Rishniw, M.; Birettoni, F.; Patata, V.; Giorgi, M.E.; Porciello, F. Left atrial deformation and phasic function determined by two-dimensional speckle-tracking echocardiography in dogs with myxomatous mitral valve disease. J. Vet. Cardiol. 2018, 20, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Corda, A.; Pinna Parpaglia, M.L.; Sotgiu, G.; Zobba, R.; Gomez Ochoa, P.; Prieto Ramos, J.; French, A. Use of 2-dimensional speckle-tracking echocardiography to assess left ventricular systolic function in dogs with systemic inflammatory response syndrome. J. Vet. Intern. Med. 2019, 33, 423–431. [Google Scholar] [CrossRef]
- Leitman, M.; Lysyansky, P.; Sidenko, S.; Shir, V.; Peleg, E.; Binenbaum, M.; Kaluski, E.; Krakover, R.; Vered, Z. Two-dimensional strain—A novel software for real-time quantitative echocardiographic assessment of myocardial function. J. Am. Soc. Echocardiogr. 2004, 17, 1021–1029. [Google Scholar] [CrossRef] [PubMed]
- Blessberger, H.; Binder, T. Two-dimensional speckle tracking echocardiography: Basic principles. Heart 2010, 96, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Fuji, Y.; Sunahara, H.; Aoki, T. Assessment of left ventricular longitudinal function in cats with subclinical hypertrophic cardiomyopathy using tissue Doppler imaging and speckle tracking echocardiography. J. Vet. Med. Sci. 2015, 77, 1101–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, R.; Mochizuki, Y.; Yoshimatsu, H. Determination of multidirectional myocardial deformations in cats with hypertrophic cardiomyopathy by using two-dimensional speckle tracking echocardiography. J. Fel. Med. Surg. 2017, 19, 1283–1289. [Google Scholar] [CrossRef]
- Suzuki, R.; Mochizuki, Y.; Yoshimatsu, H. Layer-specific myocardial function in asymptomatic cats with obstructive hypertrophic cardiomyopathy assessed using 2-dimensional speckle-tracking echocardiography. J. Vet. Intern. Med. 2019, 33, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wess, G.; Sarkar, R.; Hartmann, K. Assessment of left ventricular systolic function by strain imaging echocardiography in various stages of feline hypertrophic cardiomyopathy. J. Vet. Intern. Med. 2010, 24, 1375–1382. [Google Scholar] [CrossRef]
- Santarelli, G.; Talavera López, J.; Fernández Del Palacio, J. Evaluation of the right parasternal four-chamber view for the assessment of left ventricular longitudinal strain and strain rate by two-dimensional speckle tracking echocardiography in dogs. Res. Vet. Sci. 2018, 120, 78–85. [Google Scholar] [CrossRef]
- Thomas, W.P.; Gaber, C.E.; Jacobs, G.J.; Kaplan, P.M.; Lombard, C.W.; Moise, N.S.; Moses, B.L. Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat. Echocardiography committee of the specialty of cardiology, American college of veterinary internal medicine. J. Vet. Intern. Med. 1993, 7, 247–252. [Google Scholar] [CrossRef]
- Dickson, D.; Caivano, D.; Patteson, M.; Rishniw, M. The times they are a-changin’: Two-dimensional aortic valve measurements differ throughout diastole. J. Vet. Cardiol. 2016, 18, 15–25. [Google Scholar] [CrossRef]
- Vezzosi, T.; Schober, K.E. Doppler-derived echocardiographic evidence of pulmonary hypertension in cats with left-sided congestive heart failure. J. Vet. Cardiol. 2019, 23, 58–68. [Google Scholar] [CrossRef]
- Santilli, R.A.; Bussadori, C. Doppler echocardiographic study of left ventricular diastole in non-anaesthetized healthy cats. Vet. J. 1998, 156, 203–215. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Measurement in medicine: The analysis of method comparison studies. Statistician 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Patata, V.; Caivano, D.; Porciello, F.; Rishniw, M.; Domenech, O.; Marchesotti, F.; Giorgi, M.E.; Guglielmini, C.; Poser, H.; Spina, F.; et al. Pulmonary vein to pulmonary artery ratio in healthy and cardiomyopathic cats. J. Vet. Cardiol. 2020, 27, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Abduch, M.C.; Assad, R.S.; Mathias, W., Jr.; Aiello, V.D. The echocardiography in the cardiovascular laboratory: A guide to research with animals. Arq. Bras. Cardiol. 2014, 102, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Smets, P.; Daminet, S.; Wess, G. Simpson’s Method of Discs for Measurement of Echocardiographic End-Diastolic and End-Systolic Left Ventricular Volumes: Breed-Specific Reference Ranges in Boxer Dogs. J. Vet. Intern. Med. 2014, 28, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Wess, G.; Mäurer, J.; Simak, J.; Hartmann, K. Use of Simpson’s method of disc to detect early echocardiographic changes in Doberman Pinschers with dilated cardiomyopathy. J. Vet. Intern. Med. 2010, 24, 1069–1076. [Google Scholar] [CrossRef]
- Seckerdieck, M.; Holler, P.; Smets, P.; Wess, G. Simpson’s method of discs in Salukis and Whippets: Echocardiographic reference intervals for end-diastolic and end-systolic left ventricular volumes. J. Vet. Cardiol. 2015, 17, 271–281. [Google Scholar] [CrossRef]
- Kurosawa, T.A.; Sist, M.D.; Sanders, R.A. Echocardiographic variables in healthy North American Salukis. J. Vet. Cardiol. 2018, 20, 301–306. [Google Scholar] [CrossRef]
- Santarelli, G.; Baron Toaldo, M.; Bouvard, J.; Glaus, T.M.; Fernández Del Palacio, J. Variability among strain variables derived from two-dimensional speckle tracking echocardiography in dogs by use of various software. Am. J. Vet. Res. 2019, 80, 347–357. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STE Variables | RP4Ch View | LAP4Ch View |
|---|---|---|
| Endocardial LV longitudinal strain (%) | −21.71 ± 6.22 −22.23 (−32.68–−4.93) | −21.36 ± 5.98 −21.53 (−33.30–−4.70) |
| Epicardial LV longitudinal strain (%) | −19.83 ± 6.11 −21.02 (−31.56–−6.24) | −18.63 ± 5.55 −19.13 (−33.62–−9.68) |
| Endocardial LV longitudinal strain rate (Sec−1) | −3.19 ± 0.99 −2.88 (−6.23–−1.29) | −3.16 ± 0.96 −3.05 (−6.25–−1.32) |
| Epicardial LV longitudinal strain rate (Sec−1) | −3.08 ± 1.02 −2.92 (−5.92–−1.51) | −2.81 ± 0.90 −2.80 (−4.90–−1.36) |
| STE Variables | RP4Ch View | LAP4Ch View |
|---|---|---|
| Endocardial LV longitudinal strain | 5.4 | 7.3 |
| Epicardial LV longitudinal strain | 8.2 | 13 |
| Endocardial LV longitudinal strain rate | 18.7 | 15.3 |
| Epicardial LV longitudinal strain rate | 17.5 | 19.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caivano, D.; Rishniw, M.; Baiona, L.; Birettoni, F.; Nisini, N.; Porciello, F. Assessment of Longitudinal Left Ventricle Deformation by 2-Dimensional Speckle Tracking Echocardiography Obtained from Different Views in Cats. Vet. Sci. 2020, 7, 104. https://doi.org/10.3390/vetsci7030104
Caivano D, Rishniw M, Baiona L, Birettoni F, Nisini N, Porciello F. Assessment of Longitudinal Left Ventricle Deformation by 2-Dimensional Speckle Tracking Echocardiography Obtained from Different Views in Cats. Veterinary Sciences. 2020; 7(3):104. https://doi.org/10.3390/vetsci7030104
Chicago/Turabian StyleCaivano, Domenico, Mark Rishniw, Lucia Baiona, Francesco Birettoni, Noemi Nisini, and Francesco Porciello. 2020. "Assessment of Longitudinal Left Ventricle Deformation by 2-Dimensional Speckle Tracking Echocardiography Obtained from Different Views in Cats" Veterinary Sciences 7, no. 3: 104. https://doi.org/10.3390/vetsci7030104
APA StyleCaivano, D., Rishniw, M., Baiona, L., Birettoni, F., Nisini, N., & Porciello, F. (2020). Assessment of Longitudinal Left Ventricle Deformation by 2-Dimensional Speckle Tracking Echocardiography Obtained from Different Views in Cats. Veterinary Sciences, 7(3), 104. https://doi.org/10.3390/vetsci7030104