
Evaluation of Weight Gain, Clinicopathological and Radiographic Changes after Early Diagnosis and Treatment of Congenital Hypothyroidism in Cats

 ,
,  and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Sample Collection and Endocrine Tests
2.2. Statistical Analysis
3. Ethical Consideration
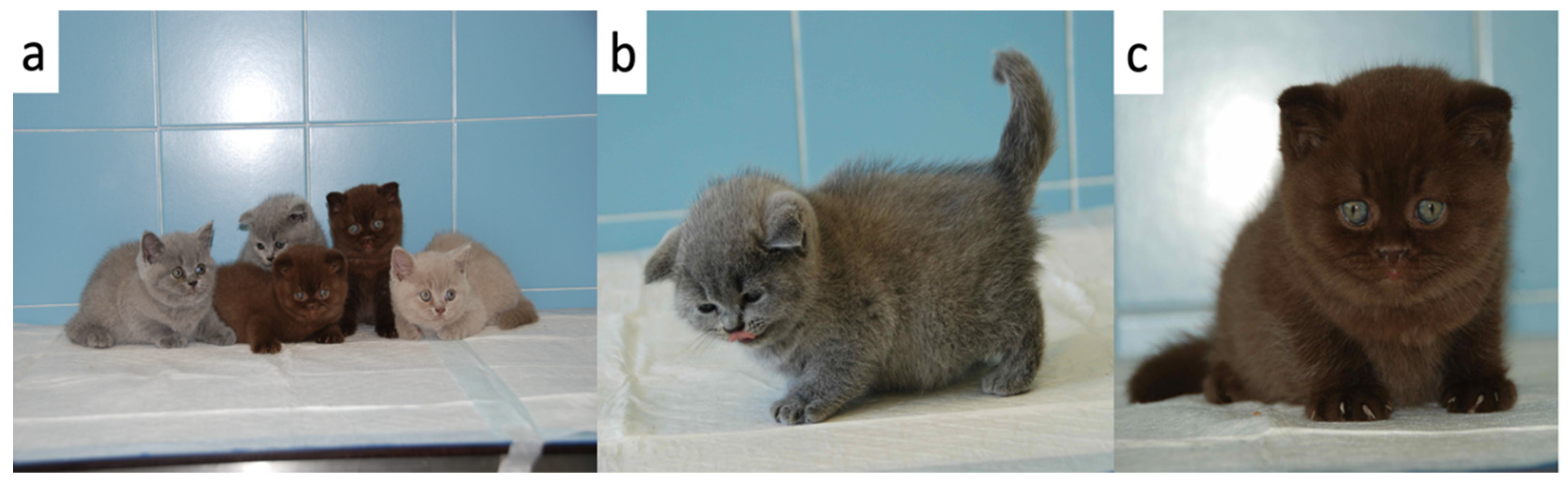
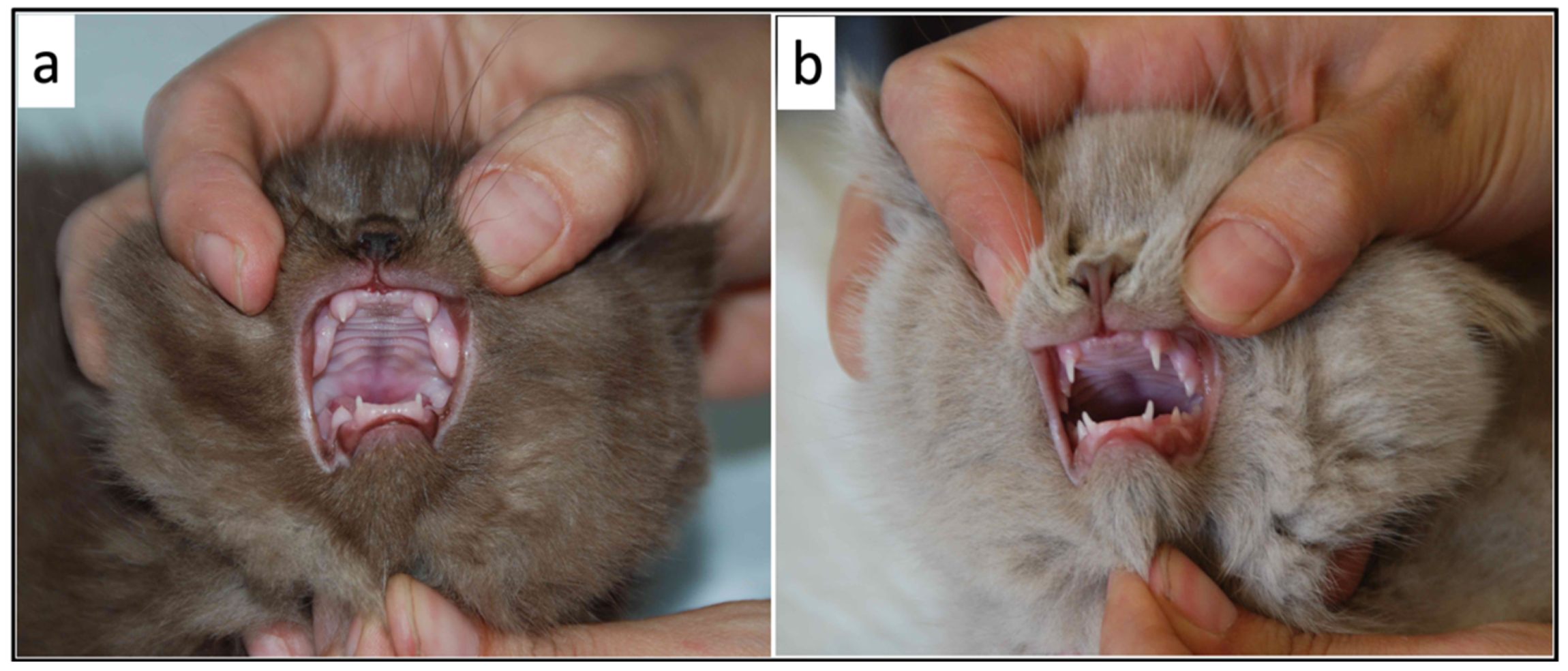
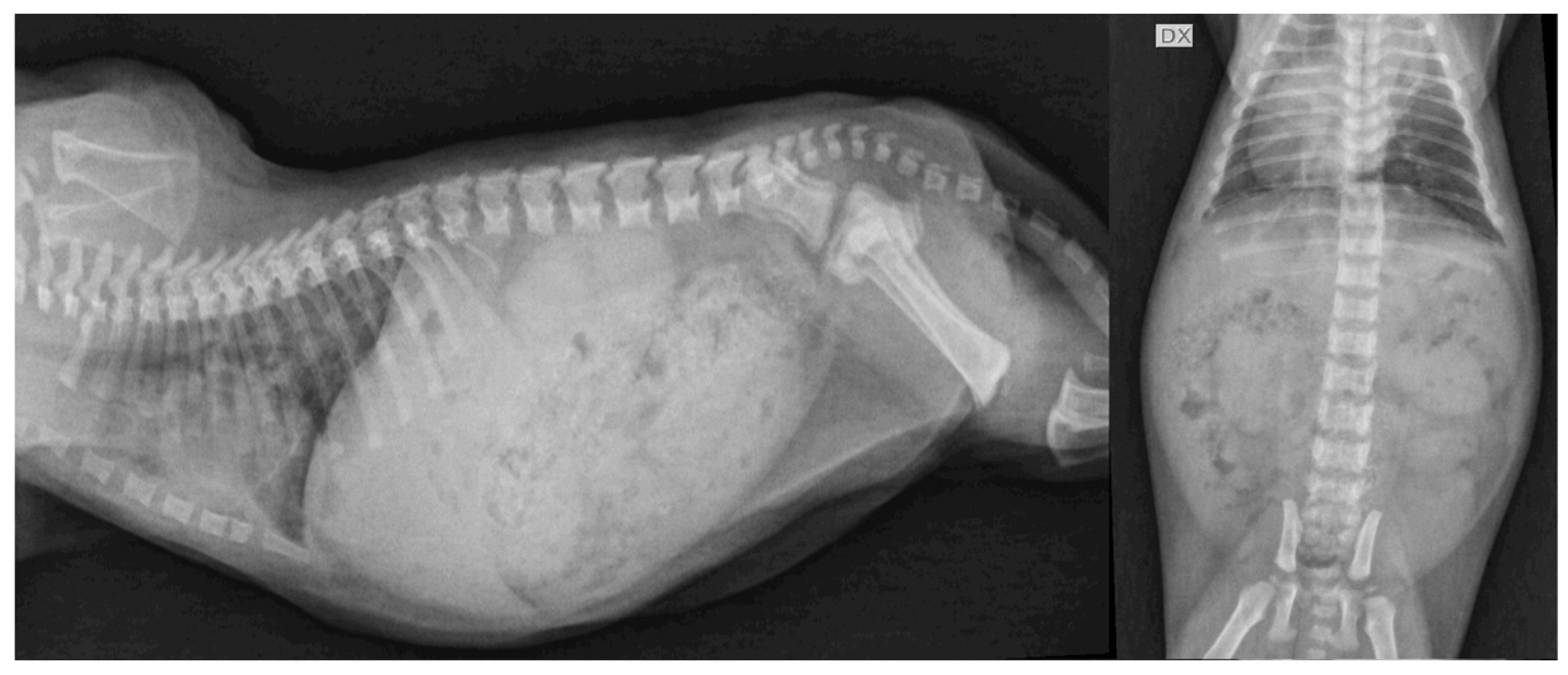
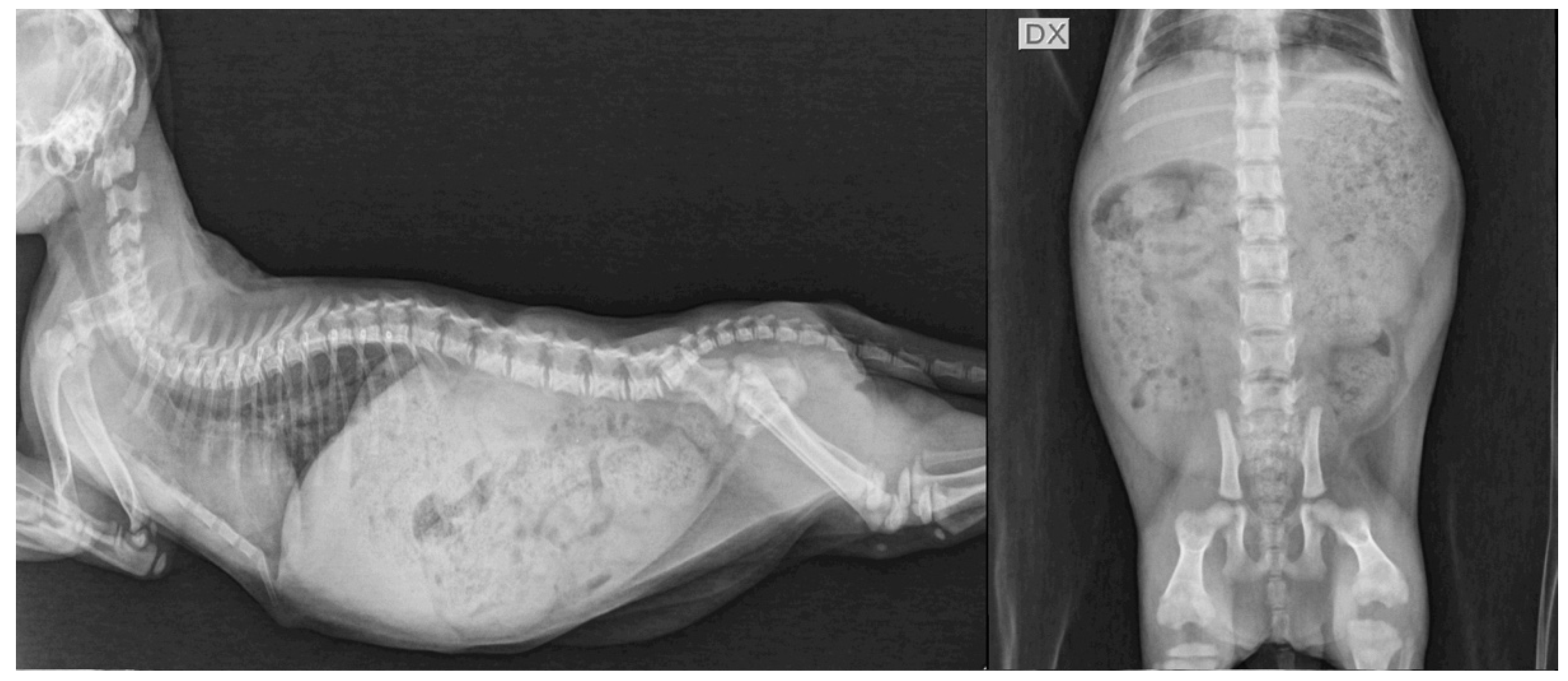
4. Clinical Cases
4.1. Case Description
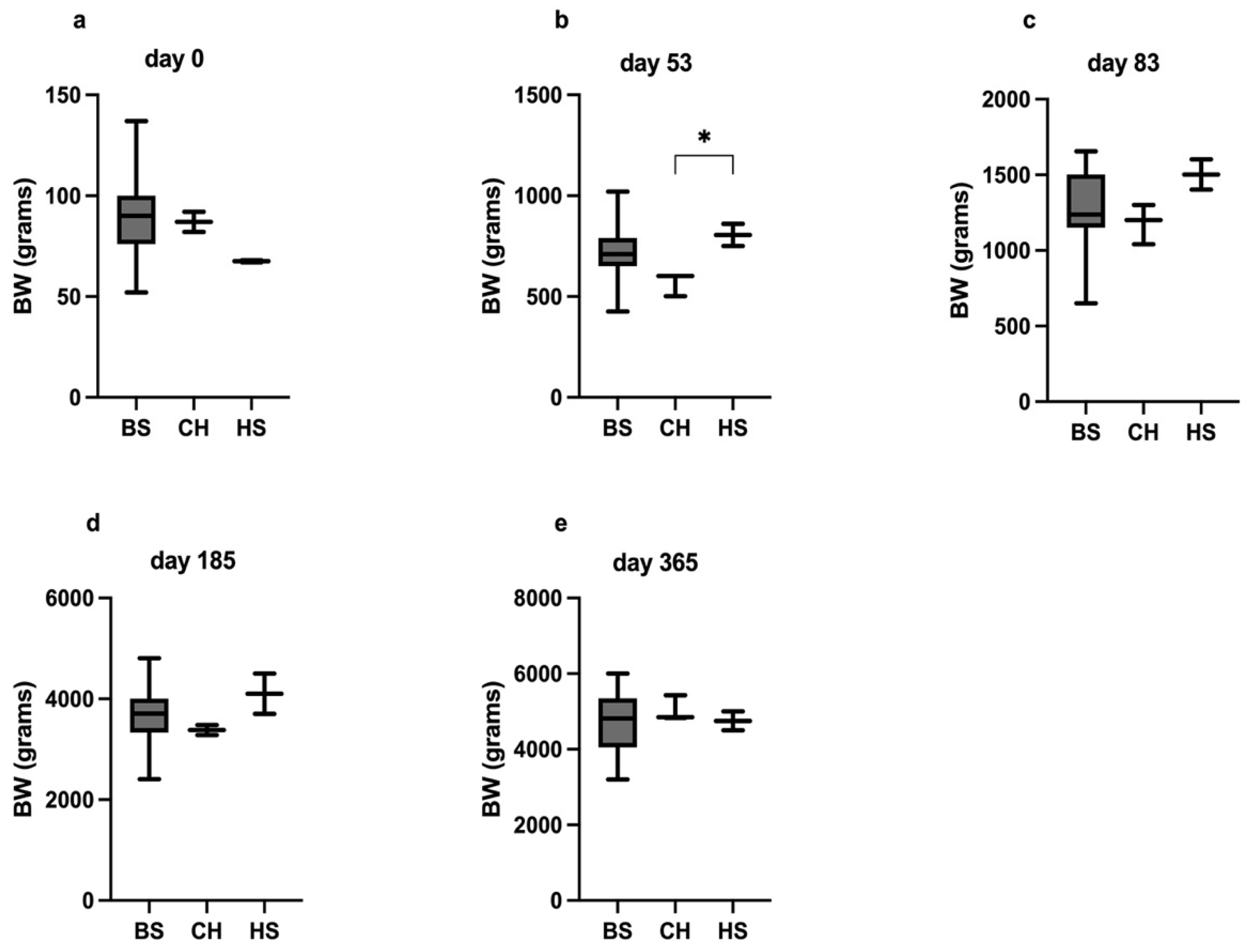
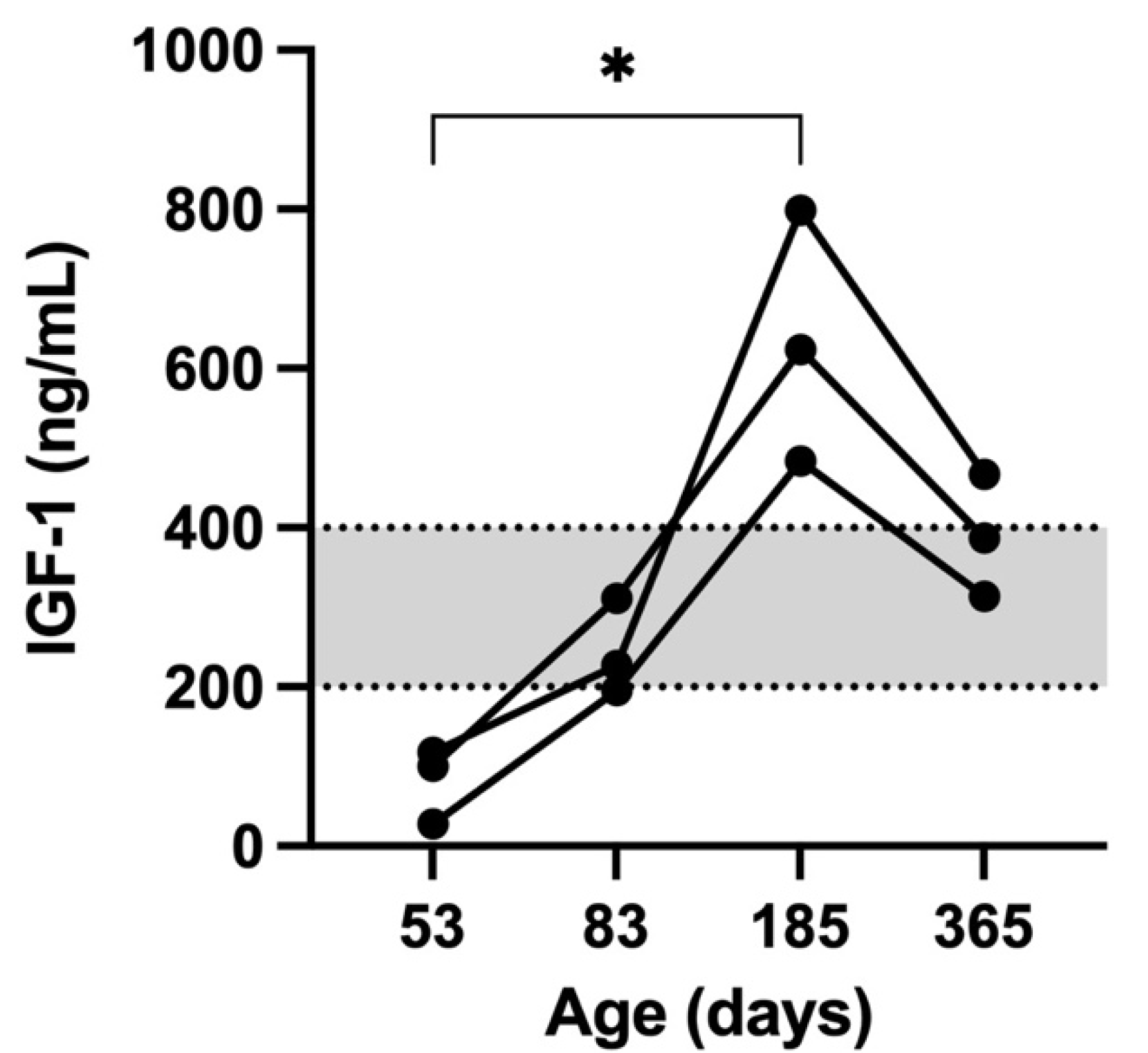
4.2. Body Weight Changes and IGF-1 Concentrations
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peterson, M.E. Hypothyroidism. In Feline Endocrinology; Feldman, E.C., Fracassi, F., Peterson, M.E., Eds.; EDRA: Milano, Italy, 2019; pp. 281–316. [Google Scholar]
- Reusch, C.E. Disorders of Growth Hormone. In Canine and Feline Endocrinology, 4th ed.; Feldman, E.C., Nelson, R.W., Reusch, C.E., Scott-Moncrieff, J.C.R., Eds.; Elsevier: St. Louis, MO, USA, 2015; pp. 37–76. [Google Scholar]
- Iturriaga, M.P.; Cocio, J.A.; Barrs, V.R. Cluster of cases of congenital feline goitrous hypothyroidism in a single hospital. J. Small Anim. Pract. 2020, 61, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Traas, A.M.; Abbott, B.L.; French, A.; Giger, U. Congenital thyroid hypoplasia and seizures in 2 littermate kittens. J. Vet. Intern. Med. 2008, 22, 1427–1431. [Google Scholar] [CrossRef] [PubMed]
- Bojanic, K.; Acke, E.; Jones, B.R. Congenital hypothyroidism of dogs and cats: A review. N. Z. Vet. J. 2011, 59, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.K.; Rosa, C.T.; De Witt, Y.; Schoeman, J.P. Congenital hypothyroidism and concurrent renal insufficiency in a kitten. J. S. Afr. Vet. Assoc. 2014, 85, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaldson, D.; Billson, F.M.; Scase, T.J.; Sparkes, A.H.; McConnel, F.; Mould, J.R.B.; Adams, V. Congenital hyposomatotropism in a domestic shorthair cat presenting with congenital corneal oedema. J. Small Anim. Pract. 2008, 49, 306–309. [Google Scholar] [CrossRef]
- Greco, D.S. Pituitary deficiencies. Top. Companion Anim. Med. 2012, 27, 2–7. [Google Scholar] [CrossRef]
- Peterson, M.E. Feline focus: Diagnostic testing for feline thyroid disease: Hypothyroidism. Compendium 2013, 35, E4. [Google Scholar]
- Quante, S.; Fracassi, F.; Gorgas, D.; Kircher, P.R.; Boretti, F.S.; Ohlerth, S.; Reusch, C.E. Congenital hypothyroidism in a kitten resulting in decreased IGF-I concentration and abnormal liver function tests. J. Feline Med. Surg. 2010, 12, 487–490. [Google Scholar] [CrossRef]
- Arnold, U.; Opitz, M.; Grosser, I.; Bader, R.; Eigenmann, J.E. Goitrous hypothyroidism and dwarfism in a kitten. J. Am. Anim. Hosp. Assoc. 1984, 20, 753–758. [Google Scholar]
- Peterson, M.E. Feline hypothyroidism. In Current Veterinary Therapy X; Kirk, R.W., Bonagura, J.D., Eds.; WB Saunders Co.: Philadelphia, PA, USA, 1989; pp. 1000–1001. [Google Scholar]
- Sjollema, B.E.; Den Hartog, M.T.; De Vijlder, J.J.M.; Van Dijk, J.E.; Rijnberk, A. Congenital hypothyroidism in two cats due to defective organification: Data suggesting loosely anchored thyroperoxidase. Eur. J. Endocrinol. 1991, 125, 435–440. [Google Scholar] [CrossRef]
- Tanase, H.; Kudo, K.; Horikoshi, H.; Mizushima, H.; Okazaki, T.; Ogata, E. Inherited primary hypothyroidism with thyrotrophin resistance in Japanese cats. J. Endocrinol. 1991, 129, 245-NP. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.R.; Gruffydd-Jones, T.J.; Sparkes, A.H.; Lucke, V.M. Preliminary studies on congenital hypothyroidism in a family of Abyssinian cats. Vet. Rec. 1992, 131, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.E.; Randolph, J.F.; Mooney, C.T. Endocrine diseases. In The Cat: Diagnosis and Clinical Management; Shereding, R.G., Ed.; Churchill Livingstone: New York, NY, USA, 1994; pp. 1404–1506. [Google Scholar]
- Firth, M.; Fodacaro, J.V.; Greco, D.S. Challenging cases in internal medicine: What’s your diagnosis? Vet. Med. 2000, 95, 606–614. [Google Scholar]
- Tobias, S.; Labato, M.A. Identifying and managing feline congenital hypothyroidism. Vet. Med. 2001, 96, 719–726. [Google Scholar]
- Mazrier, H.; French, A.; Ellinwood, N.M.; van Hoeven, M.; Zwiegle, J.; O’Donnell, P.; Jezyk, P.F.; Haskins, M.E.; Giger, U. Goitrous congenital hypothyroidism caused by thyroid peroxidase deficiency in a family of domestic shorthair cats. J. Vet. Intern. Med. 2003, 17, 395–396. [Google Scholar]
- Crowe, A. Congenital hypothyroidism in a cat. Can. Vet. J. 2004, 45, 168. [Google Scholar]
- Szabo, S.D.; Wells, K.L. What is your diagnosis? Congenital hypothyroidism. J. Am. Vet. Assoc. 2007, 230, 29–30. [Google Scholar] [CrossRef]
- McGhie, J.A.; Thompson, M.F. Intestinal intussusception in a 10-week-old kitten with congenital hypothyroidism. Aust. Vet Pract. 2011, 41, 122–125. [Google Scholar]
- Peterson, M.E. Primary goitrous hypothyroidism in a young adult domestic longhair cat: Diagnosis and treatment monitoring. J. Feline Med. Surg. Open Rep. 2015, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Van Bergen, L.; Bassez, I.; Junius, G.; Vandermeulen, E. Congenital primary hypothyroidism in a cat. Vlaams Diergeneeskundig Tijdschrift. 2016, 85, 349–354. [Google Scholar] [CrossRef]
- Jacobson, T.; Rochette, J. Congenital feline hypothyroidism with partially erupted adult dentition in a 10-month-old male neutered domestic shorthair cat: A case report. J. Vet. Dent. 2018, 35, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Tvarijonaviciute, A.; German, A.J.; Martínez-Subiela, S.; Tecles, F.; Ceron, J.J. Analytical performance of commercially-available assays for feline insulin-like growth factor 1 (IGF-1), adiponectin and ghrelin measurements. J. Feline Med. Surg. 2012, 14, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Stegeman, J.R.; Graham, P.A.; Hauptman, J.G. Use of recombinant human thyroid-stimulating hormone for thyrotropin-stimulation testing of euthyroid cats. Am. J. Vet. Res. 2003, 64, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Ghielmetti, V.; Wichert, B.; Rüegg, S.; Frey, D.; Liesegang, A. Food intake and energy expenditure in growing cats with and without a predisposition to overweight. J. Anim. Physiol. Anim. Nutr. 2018, 102, 1401–1410. [Google Scholar] [CrossRef]
- Laflamme, D. Development and validation of a body condition score system for cats: A clinical tool. Feline Pract. 1997, 25, 13–18. [Google Scholar]
- Valcavi, R.; Dieguez, C.; Preece, M.; Taylor, A.; Portioli, I.; Scanlon, M.F. Effect of thyroxine replacement therapy on plasma insulin-like growth factor 1 levels and growth hormone responses to growth hormone releasing factor in hypothyroid patients. Clin. Endocrinol. 1987, 27, 85–90. [Google Scholar] [CrossRef]
- Schmid, C.; Zwimpfer, C.; Brändle, M.; Krayenbühl, P.A.; Zapf, J.; Wiesli, P. Effect of thyroxine replacement on serum IGF-I, IGFBP-3 and the acid-labile subunit in patients with hypothyroidism and hypopituitarism. Clin. Endocrinol. 2006, 65, 706–711. [Google Scholar] [CrossRef]
- Peterson, M.E.; Guterl, J.N.; Nichols, R.; Rishniw, M. Evaluation of serum thyroid-stimulating hormone concentration as a diagnostic test for hyperthyroidism in cats. J. Vet. Intern. Med. 2015, 29, 1327–1334. [Google Scholar] [CrossRef] [Green Version]
- Stander, N.; Cassel, N. “Long bones-juvenile”. In BSAVA Manual of Canine and Feline Muscoloskeletal Imaging, 2nd ed.; Kirberger, M., McEvoy, F.J., Eds.; British Small Animal Veterinary Association: Gloucester, UK, 2016; pp. 87–107. [Google Scholar]
- Dennis, R. “Skull-general”. In BSAVA Manual of Canine and Feline Muscoloskeletal Imaging, 2nd ed.; Kirberger, M., McEvoy, F.J., Eds.; British Small Animal Veterinary Association: Gloucester, UK, 2016; pp. 275–300. [Google Scholar]
- Müller, E.E.; Locatelli, V.; Cocchi, D. Neuroendocrine control of growth hormone secretion. Physiol. Rev. 1999, 79, 511–607. [Google Scholar] [CrossRef]
- Kitiyanant, Y.; Saikhun, J.; Pavasuthipaisit, K. Somatic cell nuclear transfer in domestic cat oocytes treated with IGF-1 for in vitro maturation. Theriogenology 2003, 59, 1775–1786. [Google Scholar] [CrossRef]
- Guercio, G.; Rivarola, M.A.; Chaler, E.; Maceiras, M.; Belgorosky, A. Relationship between the GH/IGF-1 axis, insulin sensitivity, and adrenal androgens in normal prepubertal and pubertal boys. J. Clin. Endocrinol. Metab. 2002, 87, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Guercio, G.; Rivarola, M.A.; Chaler, E.; Maceiras, M.; Belgorosky, A. Relationship between the growth hormone/insulin-like growth factor-I axis, insulin sensitivity, and adrenal androgens in normal prepubertal and pubertal girls. J. Clin. Endocrinol. Metab. 2003, 88, 1389–1393. [Google Scholar] [CrossRef] [Green Version]
- Shia, W.Y.; Songkaew, A.; Singhanetr, S.; Chou, C.C.; Lee, W.M. The Investigation of the Relations between Insulin-liked Growth Factor-I and Body Weight and between Insulin-liked Growth Factor-I and Sex in Young Cats. Thai J. Vet. Med. 2011, 41, 105. [Google Scholar]
- Yüksel, B.; Özbek, M.N.; Mungan, N.Ö.; Darendeliler, F.; Budan, B.; Bideci, A.; Çetinkaya, E.; Berberoğlu, M.; Evliyaoğlu, O.; Yeşilkaya, E.; et al. Serum IGF-1 and IGFBP-3 levels in healthy children between 0 and 6 years of age. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.R.; Municchi, G.; Barnes, K.M.; Kamp, G.A.; Uriarte, M.M.; Ross, J.L.; Cassorla, F.; Cutler, G.B., Jr. Spontaneous growth hormone secretion increases during puberty in normal girls and boys. J. Clin. Endocrinol. Metab. 2011, 73, 428–435. [Google Scholar] [CrossRef]
- Juul, A.; Bang, P.; Hertel, N.T.; Main, K.; Dalgaard, P.; Jørgensen, K.; Jørn, M.; Kerstin, H.; Skakkebaek, N.E. Serum insulin-like growth factor-I in 1030 healthy children, adolescents, and adults: Relation to age, sex, stage of puberty, testicular size, and body mass index. J. Clin. Endocrinol. Metab. 1994, 78, 744–752. [Google Scholar] [PubMed]
- NRC (National Research Council). Energy. In Nutrient Requirements of Dogs and Cats; National Academies Press: Washington, DC, USA, 2006; pp. 28–48. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Kitten F1 | Kitten F2 | Kitten M1 | Reference Range |
|---|---|---|---|---|
| Baseline tT4 (nmol/L) | -- | 12.9 | 6.44 | 15–42 |
| tT4 after rhTSH (nmol/L) | -- | 12.9 | -- | 15–42 |
| TSH (ng/mL) | 5.44 | 6.20 | 12.00 | 0.03–0.30 |
| IGF-1 (ng/mL) | 53 Days | 83 Days | 185 Days | 365 Days | Reference Range |
|---|---|---|---|---|---|
| Kitten F1 | 100.60 | 311.50 | 623.40 | 387.30 | 200–400 |
| Kitten F2 | 27.51 | 195.50 | 483.70 | 313.80 | 200–400 |
| Kitten M1 | 117.50 | 227 | 798.50 | 467.10 | 200–400 |
| Kittens | Parameter | 83 Days | 185 Days | 365 Days | Reference Range |
|---|---|---|---|---|---|
| Kitten F1 | tT4 (nmol/L) | 63.40 | 45.40 | 31.8 | 15–42 |
| TSH (ng/mL) | 0.26 | 0.05 | 0.03 | 0.03–0.30 | |
| Kitten F2 | tT4 (nmol/L) | 34.40 | 15.20 | 21.6 | 15–42 |
| TSH (ng/mL) | 1.00 | 7.57 | 0.15 | 0.03–0.30 | |
| Kitten M1 | tT4 (nmol/L) | 45 | 28.20 | 46.2 | 15–42 |
| TSH (ng/mL) | 0.77 | 2.81 | 0.07 | 0.03–0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golinelli, S.; Tardo, A.M.; Vecchiato, C.G.; Guido, E.A.; Perfetti, S.; Diana, A.; Fracassi, F. Evaluation of Weight Gain, Clinicopathological and Radiographic Changes after Early Diagnosis and Treatment of Congenital Hypothyroidism in Cats. Vet. Sci. 2022, 9, 140. https://doi.org/10.3390/vetsci9030140
Golinelli S, Tardo AM, Vecchiato CG, Guido EA, Perfetti S, Diana A, Fracassi F. Evaluation of Weight Gain, Clinicopathological and Radiographic Changes after Early Diagnosis and Treatment of Congenital Hypothyroidism in Cats. Veterinary Sciences. 2022; 9(3):140. https://doi.org/10.3390/vetsci9030140
Chicago/Turabian StyleGolinelli, Stefania, Antonio Maria Tardo, Carla Giuditta Vecchiato, Eleonora Anicito Guido, Simone Perfetti, Alessia Diana, and Federico Fracassi. 2022. "Evaluation of Weight Gain, Clinicopathological and Radiographic Changes after Early Diagnosis and Treatment of Congenital Hypothyroidism in Cats" Veterinary Sciences 9, no. 3: 140. https://doi.org/10.3390/vetsci9030140
APA StyleGolinelli, S., Tardo, A. M., Vecchiato, C. G., Guido, E. A., Perfetti, S., Diana, A., & Fracassi, F. (2022). Evaluation of Weight Gain, Clinicopathological and Radiographic Changes after Early Diagnosis and Treatment of Congenital Hypothyroidism in Cats. Veterinary Sciences, 9(3), 140. https://doi.org/10.3390/vetsci9030140