
Evidence-Based Application of Acupuncture for Pain Management in Companion Animal Medicine


Abstract
:1. Introduction
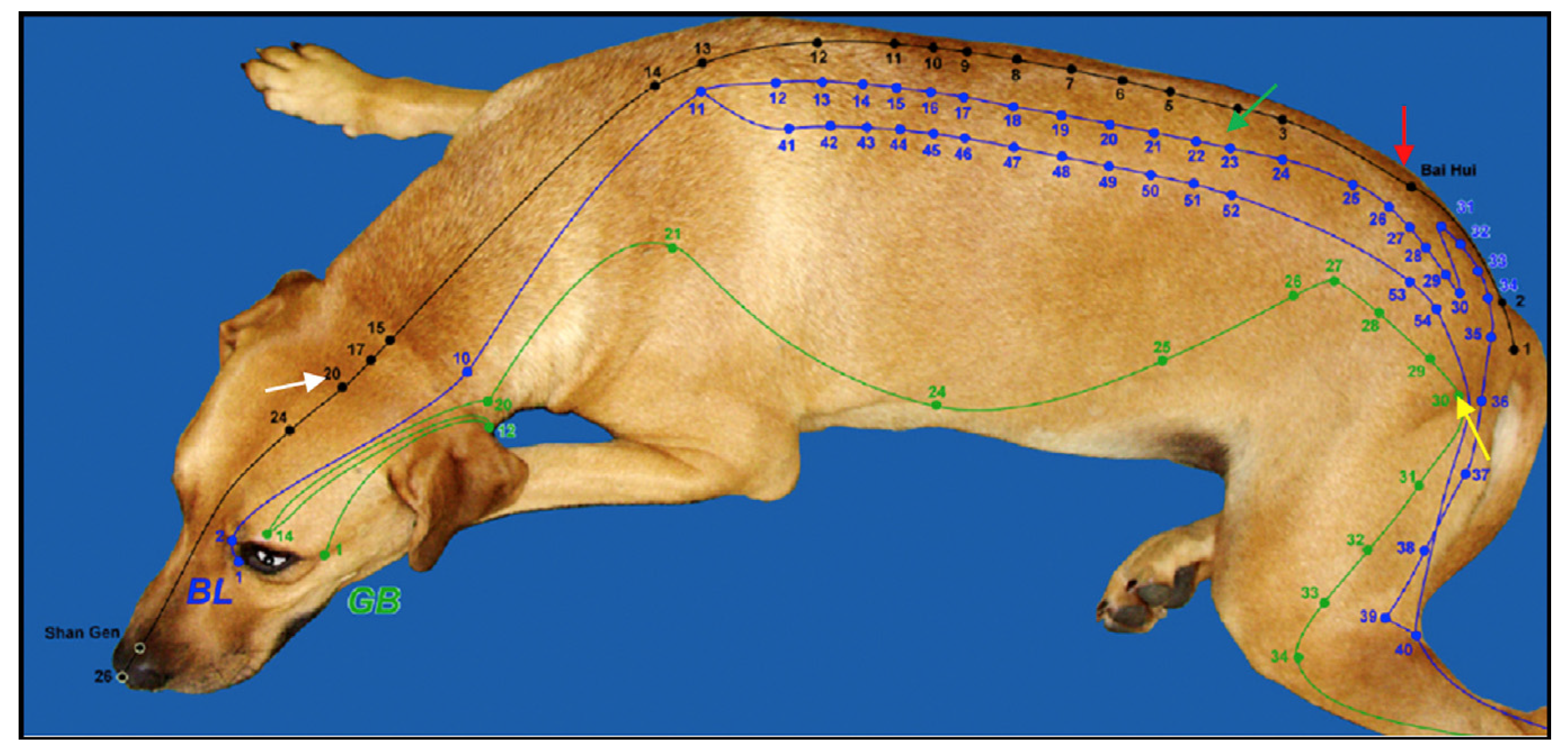
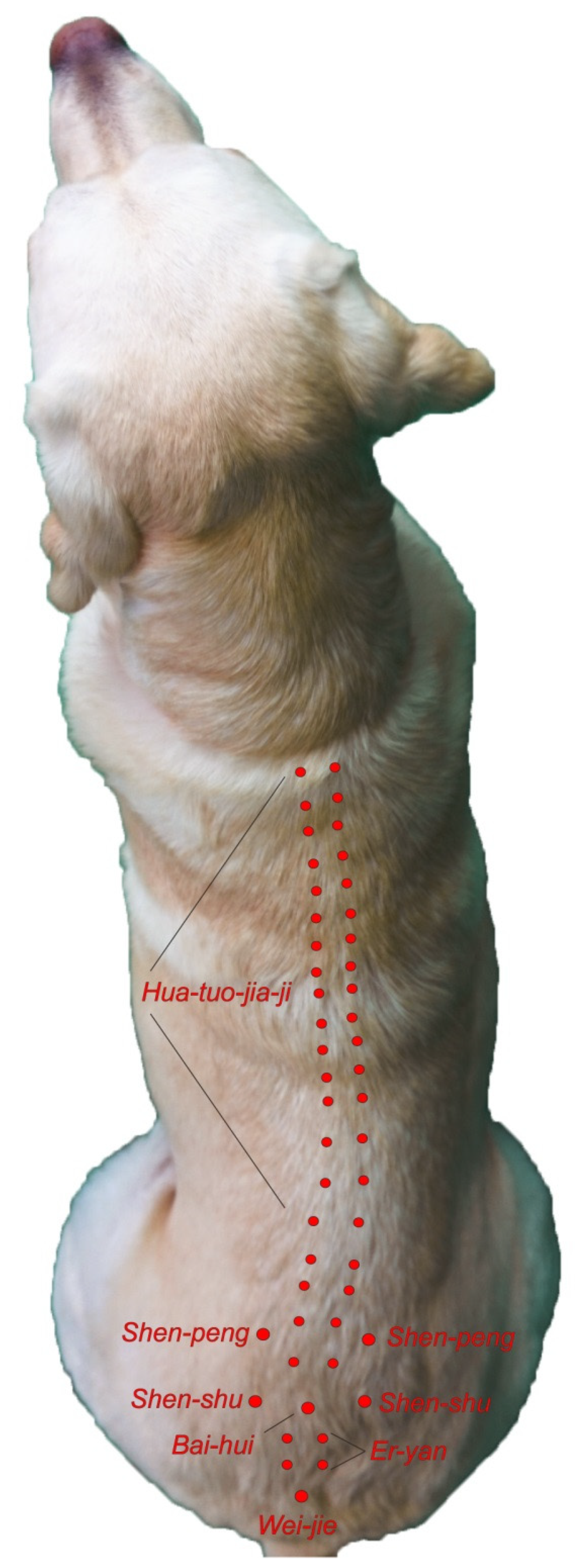
2. Acupuncture Points and Meridians

3. Analgesic Effects of Acupuncture
3.1. The Pain Pathway
3.2. Local Effects of Acupuncture
3.3. Spinal or Segmental Effects of Acupuncture
3.4. Suprasegmental (Brain) Effects of Acupuncture
4. Clinical Applications of Acupuncture for Pain Mitigation
5. Acupuncture Contraindications and Precautions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xie, H.; Wedemeyer, L. The Validity of Acupuncture in Veterinary Medicine. Am. J. Tradit. Chin. Vet. Med. 2012, 7, 35–43. [Google Scholar]
- Xie, H.; Preast, V. Xie’s Veterinary Acupuncture; Blackwell Publishing: Ames, IA, USA, 2007. [Google Scholar]
- Epstein, M.E.; Rodanm, I.; Griffenhagen, G.; Kadrlik, J.; Petty, M.; Robertson, S.; Simpson, W. 2015 AAHA/AAFP Pain Management Guidelines for Cats and Dogs. J. Am. Anim. Hosp. Assoc. 2015, 17, 251–272. [Google Scholar] [CrossRef]
- Cantwell, S.L. Traditional Chinese Veterinary Medicine: The Mechanism and Management of Acupuncture for Chronic Pain. Top. Companion Anim. Med. 2010, 25, 53–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shmalberg, J.; Memon, M.A. A Retrospective Analysis of 5195 Patient Treatment Sessions in an Integrative Veterinary Medicine Service: Patient Characteristics, Presenting Complaints, and Therapeutic Interventions. Vet. Med. Int. 2015, 2015, 983621. [Google Scholar] [CrossRef] [Green Version]
- Han, J.S. Acupuncture analgesia: Areas of consensus and controversy. Pain 2011, 152 (Suppl. 2), S41–S48. [Google Scholar] [CrossRef]
- Berman, B.M.; Langevin, H.M.; Witt, C.M.; Dubner, R. Clinical Therapeutics Acupuncture for Chronic Low Back Pain. N. Eng. J. Med. 2010, 363, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Kaptchuk, T.J.; Chen, K.J.; Song, J. Recent clinical trials of acupuncture in the West: Responses from the practitioners. Chin. J. Integr. Med. 2010, 16, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Selmer, M.; Shiau, D.S. Therapeutic Results of Integrative Medicine Treatments Combining Traditional Chinese with Western Medicine: A Systematic Review and Meta-Analysis. Am. J. Tradit. Chin. Vet. Med. 2019, 14, 41–47. [Google Scholar]
- Chen, S.; Wang, S.; Rong, P.; Wang, J.; Qiao, L.; Feng, X.; Liu, J.; Zhang, J. Acupuncture for visceral pain: Neural substrates and potential mechanisms. Evid.-Based Complementary Altern. Med. 2014, 2014, 609594. [Google Scholar] [CrossRef] [Green Version]
- Fan, A.Y.; Ouyang, H.; Qian, X.; Wei, H.; Wang, D.D.; He, D.; Tian, H.; Gong, C.; Matecki, A.; Alemi, S.F. Discussions on real-world acupuncture treatments for chronic low-back pain in older adults. J. Integr. Med. 2019, 17, 71–76. [Google Scholar] [CrossRef]
- Lane, D.M.; Hill, S.A. Effectiveness of combined acupuncture and manual therapy relative to no treatment for canine musculoskeletal pain. Can. Vet. J. 2016, 57, 407–414. [Google Scholar] [PubMed]
- Liu, C.M.; Chang, F.C.; Lin, C.T. Retrospective study of the clinical effects of acupuncture on cervical neurological diseases in dogs. J. Vet. Sci. 2016, 17, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, N.E.O.F.; Luna, S.P.L.; Joaquim, J.G.F.; Coutinho, H.D.; Possebon, F.S. Effect of acupuncture on pain and quality of life in canine neurological and musculoskeletal diseases. Can. Vet. J. 2017, 58, 941–951. [Google Scholar]
- Janssens, L.A.A. Observations on acupuncture therapy of chronic osteoarthritis in dogs: A review of sixty-one cases. J. Small Anim. Pract. 1986, 27, 825–837. [Google Scholar] [CrossRef]
- Chomsiriwat, P.; Ma, A. Comparison of the effects of electro-acupuncture and laser acupuncture on pain relief and joint range of motion in dogs with coxofemoral degenerative joint disease. Am. J. Tradit. Chin. Vet. Med. 2019, 14, 11–20. [Google Scholar]
- Shmalberg, J.; Burgess, J.; Davies, W. A randomized controlled blinded clinical trial of electro-acupuncture administered one month after cranial cruciate ligament repair in dogs. Am. J. Tradit. Chin. Vet. Med. 2014, 9, 41–43. [Google Scholar]
- Sousa, N.R.; Luna, S.P.; Cápua, M.L.; Lima, A.F.; Oliveira, F.A.; Viveiros, B.M.; Barbosa, L. Analgesia of preemptive pharmacopunc ture with meloxicam or aquapuncture in cats undergoing ovariohysterectomy. Ciência Rural. 2012, 42, 1231–1236. [Google Scholar] [CrossRef] [Green Version]
- Dewey, C.W.; Xie, H. The scientific basis of acupuncture for veterinary pain management: A review based on relevant literature from the last two decades. Open Vet. J. 2021, 11, 203–209. [Google Scholar] [CrossRef]
- Gong, C.; Liu, W. Advanced research validates classical principles-the neurobiological mechanisms involved in acupuncture for pain management. Longhua Chin. Med. 2019, 2, 16. [Google Scholar] [CrossRef]
- Schoen, A.M.; Janssens, L.; Rogers, P.A.M. Veterinary Acupuncture. In Seminars in Veterinary Medicine and Surgery (Small Animal); American Veterinary Publicationsl: New York, NY, USA, 1986; Volume 1, pp. 224–229. [Google Scholar]
- Zhang, Z.J.; Wang, X.M.; McAlonan, G.M. Neural acupuncture unit: A new concept for interpreting effects and mechanisms of acupuncture. Evid.-Based Complementary Altern. Med. 2012, 2012, 429412. [Google Scholar]
- Wright, B.D. Acupuncture for the treatment of animal pain. Vet. Clin. Small Anim. Pract. 2019, 49, 1029–1039. [Google Scholar] [CrossRef]
- Lu, D.P.; Lu, G.P. An Historical Review of Perspective on the impact of acupuncture on US Medicine and Society. Med. Acupunct. 2013, 25, 311–316. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.B.; Jia, D.X.; Li, H.Y.; Wei, Y.L.; Yan, H.; Zhao, P.N.; Gu, F.F.; Wang, G.J.; Wang, Y.P. Understanding qi running in the meridians as interstitial fluid flowing via interstitial space of low hydraulic resistance. Chin. J. Integr. Med. 2018, 24, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D. Acupuncture for the Treatment of Neuromuscular Conditions in Dogs and Cats, with Emphasis on Intervertebral Disc Disease. J. Am. Holist. Vet. Med. Assoc. 2021, 63, 23–33. [Google Scholar]
- Langevin, H.M. Acupuncture, connective tissue, and peripheral sensory modulation. Crit. Rev. Eukaryot. Gene Expr. 2014, 24, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Langevin, H.M.; Nedergaard, M.; Howe, A.K. Cellular control of connective tissue matrix tension. J. Cell. Biochem. 2013, 114, 1714–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, C.W.; Xie, H. Clinicians Guide to Canine Acupuncture; Chi Institute Press: Reddick, FL, USA, 2018. [Google Scholar]
- Weish, A.J.; Yaksh, T. Nociception and Pain Mechanisms. In The Handbook of Veterinary Pain Management; Gaynor, J., Muir, W.W., Eds.; Elsevier Mosley: Saint Louis, MO, USA, 2015; pp. 10–41. [Google Scholar]
- Zhang, J.H.; Cao, X.D.; Lie, J.; Tang, W.J.; Liu, H.Q.; Fenga, X.Y. Neuronal specificity of needling acupoints at same meridian: A control functional magnetic resonance imaging study with electroacupuncture. Acupunct. Electro-Ther. Res. 2007, 32, 179–193. [Google Scholar] [CrossRef]
- Fry, L.M.; Neary, S.M.; Sharrock, J.; Rychel, J.K. Acupuncture for analgesia in veterinary medicine. Top. Companion Anim. Med. 2014, 29, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Groppetti, D.; Pecile, A.M.; Sacerdote, P. Effectiveness of electroacupuncture analgesia compared with opioid administration in a dog model: A pilot study. Br. J. Anaesth. 2011, 107, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Lao, L.; Ren, K.; Berman, B.M. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology 2014, 120, 482–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.Q. Neural mechanism underlying acupuncture analgesia. Prog. Neurobiol. 2008, 85, 355–375. [Google Scholar] [CrossRef]
- Xie, H.; Sivula, N. Review of Veterinary Acupuncture Clinical Trials. Am. J. Tradit. Chin. Vet. Med. 2016, 11, 49–60. [Google Scholar]
- Watkin, H. Segmental dysfunction. Acupunct. Med. 1999, 17, 118–122. [Google Scholar] [CrossRef]
- de Lahunta, A.; Glass, E. Veterinary Neuroanatomy and Clinical Neurology, 3rd ed.; Saunders Elsevier: St. Louis, MO, USA, 2009; p. 540. [Google Scholar]
- Kong, J.; Kaptchuk, T.J.; Polich, G.; Kirsch, I.; Vangel, M.; Zyloney, C.; Rosen, B.; Gollub, R.L. An fMRI study on the interaction and dissociation between expectation of pain relief and acupuncture treatment. Neuroimage 2009, 47, 1066–1076. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Kaptchuk, T.J.; Polich, G.; Kirsch, I.; Vangel, M.; Zyloney, C.; Rosen, B.; Gollub, R.L. Expectancy and treatment interactions: A dissociation between acupuncture analgesia and expectancy evoked placebo analgesia. Neuroimage 2009, 45, 940–949. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; Gollub, R.L.; Rosman, I.S.; Webb, J.M.; Vangel, M.G.; Kirsch, I.; Kaptchuk, T.J. Brain activity associated with expectancy-enhanced placebo analgesia as measured by functional magnetic resonance imaging. J. Neurosci. 2006, 26, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Roynard, P.; Lauren, F.; Xie, H.; Fowler, M. Acupuncture for Small Animal Neurologic Disorders. Vet. Clin. Small Anim. Pract. 2018, 48, 201–219. [Google Scholar] [CrossRef]
- Hayashi, A.M.; Matera, J.M.; de Campos Fonseca Pinto, A.C. Evaluation of electroacupuncture treatment for thoracolumbar intervertebral disk disease in dogs. JAVMA 2007, 231, 913–918. [Google Scholar] [CrossRef]
- Lee, L. Non-Surgical Treatment for Cranial Cruciate Ligament Rupture in Senior Dogs: A Retrospective Case Series. Am. J. Tradit. Chin. Vet. Med. 2019, 14, 49–64. [Google Scholar]
- Ciolanescu, B. Comparison of the Efficacy of Traditional Chinese Veterinary Medicine Versus Conservative Management for Treatment of Cranial Cruciate Ligament Injury in 40 Companion Dogs. Am. J. Tradit. Chin. Vet. Med. 2020, 15, 23–34. [Google Scholar]
- Marx, C.; Silveira, M.D.; Selbach, I.; da Silva, A.S.; Braga, L.M.; Camassola, M.; Nardi, N.B. Acupoint injection of autologous stromal vascular fraction and allogeneic adipose-derived stem cells to treat hip dysplasia in dogs. Stem Cells Int. 2014, 2014, 391274. [Google Scholar] [CrossRef] [Green Version]
- Jaeger, G.T.; Larsen, S.; Søli, N.; Moe, L. Double blind, placebo-controlled trial of the pain-relieving effects of the implantation of gold beads into dogs with hip dysplasia. Vet. Rec. 2006, 158, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, G.T.; Larsen, S.; Søli, N.; Moe, L. Two years follow-up study of the pain-relieving effect of gold bead implantation in dogs with hip-joint arthritis. Acta Vet. Scand. 2007, 40, 9. [Google Scholar] [CrossRef] [Green Version]
- Bartholome, M.; Schulze, E. Efficacy of Gold Bead Acupuncture Treatment of Chronic Hip, Elbow and Spine Pain in 79 Dogs Following Unsuccessful Conventional Treatments. Am. J. Tradit. Chin. Vet. Med. 2020, 15, 17–30. [Google Scholar]
- Deisenroth, A.; Nolte, I.; Wefstaedt, P. Use of gold Implants as a treatment of pain related to canine hipdysplasia—a review. Part 2: Clinical trials and case reports. Tierarztl. Prax. Ausg. K Kleintiere/Heimtiere 2013, 41, 244–254. [Google Scholar] [CrossRef]
- Joaquim, J.G.; Luna, S.P.; Brondani, J.T.; Torelli, S.R.; Rahal, S.C.; de Paula Freitas, F. Comparison of decompressive surgery, electroacupuncture, and decompressive surgery followed by electroacupuncture for the treatment of dogs with intervertebral disk disease with long standing severe neurologic deficits. J. Am. Vet. Med. Assoc. 2011, 236, 1225–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, H.J.; Yoon, H.Y.; Kim, J.Y. Clinical Effect of additional electroacupuncture on thoracolumbar intervertebral disc herniation in 80 paraplegic dogs. Am. J. Chin. Med. 2010, 38, 1015–1025. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Type of Point | Location of Point |
|---|---|
| Type I | Motor points Located in areas where nerves enter muscles 67% of all acupoints are motor points |
| Type II | Located on superficial nerves in the sagittal plane on the dorsal and ventral midlines. |
| Type III | Located at high density loci of superficial nerves and nerve plexuses |
| Type IV | Located at musculotendinous junctions where the Golgi tendon organs are located. |
| Type of Nerve Fiber | Signal Carried | Myelin Sheath | Diameter (Micrometers) | Conduction Speed (m/s) |
|---|---|---|---|---|
| A-Beta | Touch | Yes | 6–12 | 35–90 |
| A-Delta | Pain—Mechanical and Thermal | Yes | 1–5 | 5–40 |
| C | Pain-Mechanical, thermal, chemical | No | 0.2–1.5 | 0.5–2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huntingford, J.L.; Petty, M.C. Evidence-Based Application of Acupuncture for Pain Management in Companion Animal Medicine. Vet. Sci. 2022, 9, 252. https://doi.org/10.3390/vetsci9060252
Huntingford JL, Petty MC. Evidence-Based Application of Acupuncture for Pain Management in Companion Animal Medicine. Veterinary Sciences. 2022; 9(6):252. https://doi.org/10.3390/vetsci9060252
Chicago/Turabian StyleHuntingford, Janice L., and Michael C. Petty. 2022. "Evidence-Based Application of Acupuncture for Pain Management in Companion Animal Medicine" Veterinary Sciences 9, no. 6: 252. https://doi.org/10.3390/vetsci9060252
APA StyleHuntingford, J. L., & Petty, M. C. (2022). Evidence-Based Application of Acupuncture for Pain Management in Companion Animal Medicine. Veterinary Sciences, 9(6), 252. https://doi.org/10.3390/vetsci9060252