
Reproducibility and Feasibility of Classification and National Guidelines for Histological Diagnosis of Canine Mammary Gland Tumours: A Multi-Institutional Ring Study

 ,
,  , ,
, ,  , , , ,
, , , , 
 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Guidelines and WP Composition
- Histological subtypes—To precisely apply the histological diagnosis reported in the DTF classification, as proposed by the authors. For example, the term “carcinoma in situ” was not applied and instead used atypical hyperplasia or atypical epitheliosis, depending on specific morphological aspects. As another example, it was agreed that the tumour histotype was defined based on the prevalent morphological pattern where more than one pattern was observed (e.g., tubular and solid).
- Criteria for malignancy—To employ the following parameter as criteria for malignancy: (I) tumour architecture with reduced tubular organisation (with no objective measurement and no specific cut off); (II) marked cellular and nuclear pleomorphism (with no objective measurement and no specific cut off); and (III) high mitotic count. A cut off ≥6 mitoses per 2.37 mm2 was proposed and applied exclusively when other criteria for malignancy were borderline/unclear. This was to indicate the possibility of a lesion with clear evidence of malignancy (e.g., anaplastic carcinoma) and a mitotic count below 6, or of a clearly benign lesion (e.g., ductal adenoma) with a number of mitoses higher or equal to 6. Regarding the mitotic count, it was performed digitally by the WP following these criteria: total area of observation of 2.37 mm2 [70] taking into consideration that the digital fields to obtain this total area had to be highly cellular and avoid cystic/necrotic fields. If the expected area (2.37 mm2) could not be obtained, the mitotic count was proportionally determined; most mitotically active areas (usually at the periphery of the tumour) were chosen to start, moving to consecutive fields. After two fields with no mitoses, the third new field was chosen as the next new mitotically active field to then proceed again consecutively, and so on until ten counted fields in total. In order to do so, each participant calculated the number of fields to be examined on their screen to cover the standardised 2.37 mm2 area. This was done by dividing 2.37 mm2 by the total area of a 40“×” U+00D7 image field, which was measured with a ruler tool on the screen [70]. Additional criteria for malignancy were (IV) presence of small areas of random necrosis (groups of neoplastic cells with karyolysis and karyorrhexis), keeping in mind that central wide necrosis can be present both in benign and malignant lesions; (V) peripheral infiltration, determined as an irregular contour of the tumour showing a desmoplastic reaction, often associated with a mixed inflammatory infiltrate; (VI) pluristratification of neoplastic cells with loss of polarity, atypia, and dysplasia; and (VII) lymphatic vessel invasion by neoplastic cells.
3.2. Outcomes Expressed in Terms of Hyperplasia-Dysplasia/Benign/Malignant (H, B, M) Showed a Substantial Agreement
3.3. Outcomes Expressed in Terms of ICD-O Morphological Code/Diagnosis Had a Moderate Agreement
3.4. Outcomes Expressed in Terms of Grading
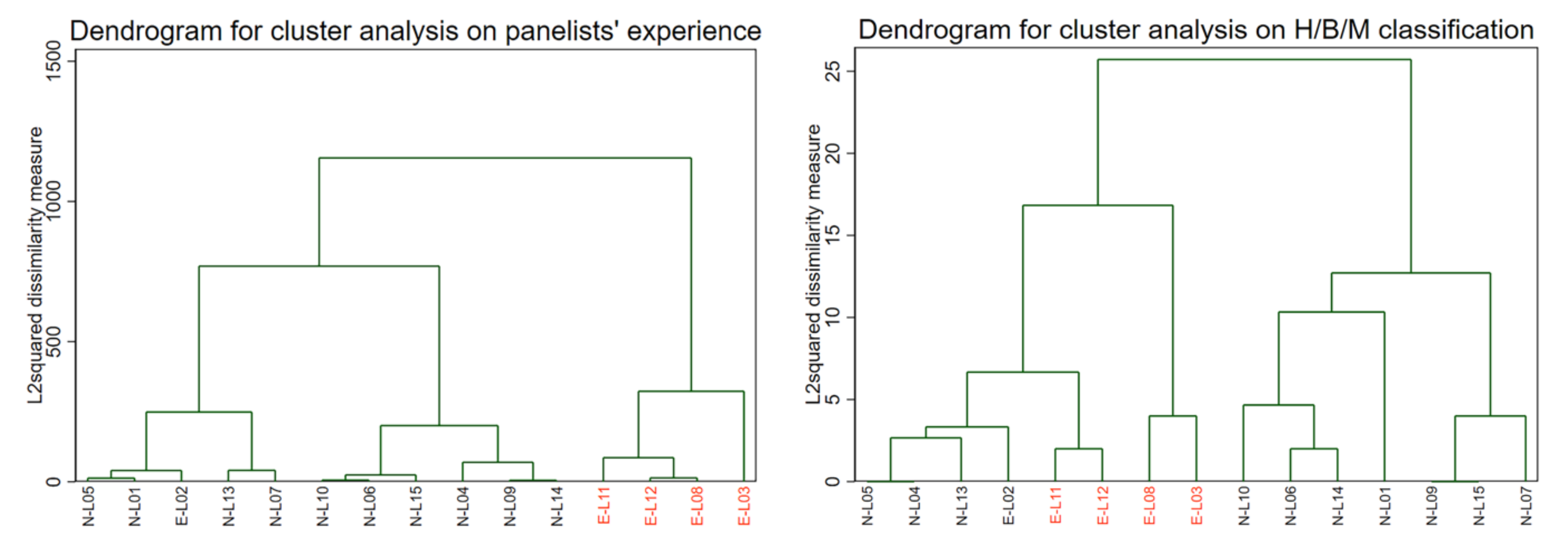
3.5. Outcomes Expressed Considering Panellist Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, F.; Peña, L.; Ibisch, C.; Loussouarn, D.; Gama, A.; Rieder, N.; Belousov, A.; Campone, M.; Abadie, J. Canine invasive mammary carcinomas as models of human breast cancer. Part 1: Natural history and prognostic factors. Breast Cancer Res. Treat. 2018, 167, 635–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peña, L.; De Andrés, P.J.; Clemente, M.; Cuesta, P.; Pérez-Alenza, M.D. Prognostic value of histological grading in noninflammatory canine mammary carcinomas in a prospective study with two-year follow-up: Relationship with clinical and histological characteristics. Vet. Pathol. 2013, 50, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Rasotto, R.; Berlato, D.; Goldschmidt, M.H.; Zappulli, V. Prognostic Significance of Canine Mammary Tumor Histologic Subtypes: An Observational Cohort Study of 229 Cases. Vet. Pathol. 2017, 54, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, G.; Alonso-Diez, A.; Perez-Alenza, D.; Pena, L. From Conventional to Precision Therapy in Canine Mammary Cancer: A Comprehensive Review. Front. Vet. Sci. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Hampe, J.F.; Misdorp, W. Tumours and dysplasias of the mammary gland. Bull. World Health Organ. 1974, 50, 111–133. [Google Scholar] [PubMed]
- Misdorp, W.; Else, R.W.; Hellmen, E.; Lipscomb, T.P. Histological Classification of Mammary Tumors of the Dog and the Cat; Armed Forces Institute of Pathology: Washington, DC, USA, 1999. [Google Scholar]
- Zapulli, V.; Peña, L.; Rasotto, R.; Goldschmidt, M.H.; Gama, A.; Scruggs, J.L. Surgical Pathology of Tumors of Domestic Animals Volume 2: Volume 2: Mammary Tumors: Mammary Tumors; Kiupel, M., Ed.; Davis-Thompson DVM Foundation: Washington, DC, USA, 2019; Volume 2. [Google Scholar]
- Santos, M.; Correia-Gomes, C.; Santos, A.; de Matos, A.; Dias-Pereira, P.; Lopes, C. Interobserver Reproducibility of Histological Grading of Canine Simple Mammary Carcinomas. J. Comp. Pathol. 2015, 153, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.Y.; Liao, A.T.; Liu, C.H. Interobserver Variation in the Morphopathological Diagnosis of Canine Mammary Gland Tumor Among Veterinary Pathologists. Int. J. Appl. Res. Vet. Med. 2011, 9, 388–391. [Google Scholar]
- Adams, A.L.; Chhieng, D.C.; Bell, W.C.; Winokur, T.; Hameed, O. Histologic grading of invasive lobular carcinoma: Does use of a 2-tiered nuclear grading system improve interobserver variability? Ann. Diagn. Pathol. 2009, 13, 223–225. [Google Scholar] [CrossRef]
- Denkert, C.; Wienert, S.; Poterie, A.; Loibl, S.; Budczies, J.; Badve, S.; Bago-Horvath, Z.; Bane, A.; Bedri, S.; Brock, J.; et al. Standardized evaluation of tumor-infiltrating lymphocytes in breast cancer: Results of the ring studies of the international immuno-oncology biomarker working group. Mod. Pathol. 2016, 29, 1155–1164. [Google Scholar] [CrossRef]
- van Dam, P.J.; van der Stok, E.P.; Teuwen, L.A.; Van den Eynden, G.G.; Illemann, M.; Frentzas, S.; Majeed, A.W.; Eefsen, R.L.; Coebergh van den Braak, R.R.J.; Lazaris, A.; et al. International consensus guidelines for scoring the histopathological growth patterns of liver metastasis. Br. J. Cancer 2017, 117, 1427–1441. [Google Scholar] [CrossRef] [Green Version]
- Lohse, A.W.; Sebode, M.; Bhathal, P.S.; Clouston, A.D.; Dienes, H.P.; Jain, D.; Gouw, A.S.H.; Guindi, M.; Kakar, S.; Kleiner, D.E.; et al. Consensus recommendations for histological criteria of autoimmune hepatitis from the International AIH Pathology Group: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology: Results of a workshop on AIH histology hosted by the European Reference Network on Hepatological Diseases and the European Society of Pathology. Liver. Int. 2022, 42, 1058–1069. [Google Scholar] [CrossRef]
- Willmann, M.; Yuzbasiyan-Gurkan, V.; Marconato, L.; Dacasto, M.; Hadzijusufovic, E.; Hermine, O.; Sadovnik, I.; Gamperl, S.; Schneeweiss-Gleixner, M.; Gleixner, K.V.; et al. Proposed Diagnostic Criteria and Classification of Canine Mast Cell Neoplasms: A Consensus Proposal. Front. Vet. Sci. 2021, 8, 10. [Google Scholar] [CrossRef]
- Gilles, F.H.; Tavare, C.J.; Becker, L.E.; Burger, P.C.; Yates, A.J.; Pollack, I.F.; Finlay, J.L. Pathologist interobserver variability of histologic features in childhood brain tumors: Results from the CCG-945 study. Pediatr. Dev. Pathol. 2008, 11, 108–117. [Google Scholar] [CrossRef]
- Eefting, D.; Schrage, Y.M.; Geirnaerdt, M.J.; Le Cessie, S.; Taminiau, A.H.; Bovée, J.V.; Hogendoorn, P.C.; Consortium, E. Assessment of interobserver variability and histologic parameters to improve reliability in classification and grading of central cartilaginous tumors. Am. J. Surg. Pathol. 2009, 33, 50–57. [Google Scholar] [CrossRef]
- Evans, H.L.; Ayala, A.G.; Romsdahl, M.M. Prognostic factors in chondrosarcoma of bone: A clinicopathologic analysis with emphasis on histologic grading. Cancer 1977, 40, 818–831. [Google Scholar] [CrossRef]
- Corazza, G.R.; Villanacci, V.; Zambelli, C.; Milione, M.; Luinetti, O.; Vindigni, C.; Chioda, C.; Albarello, L.; Bartolini, D.; Donato, F. Comparison of the interobserver reproducibility with different histologic criteria used in celiac disease. Clin. Gastroenterol. Hepatol. 2007, 5, 838–843. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef]
- Corazza, G.R.; Villanacci, V. Coeliac disease. J. Clin. Pathol. 2005, 58, 573–574. [Google Scholar] [CrossRef] [Green Version]
- Rugge, M.; Sacchi, D.; Genta, R.M.; Zanco, F.; Guzzinati, S.; Pizzi, M.; Fassan, M.; Di Sabatino, A.; El-Serag, H. Histological assessment of gastric pseudopyloric metaplasia: Intra- and inter-observer consistency. Dig. Liver Dis. 2021, 53, 61–65. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, S.H.B.; Lázaro, G.C.; Franco, L.M.; Valença, J.T.; Nobre E Souza, M.; Souza, M.H.L.P. Agreement between different pathologists in histopathologic diagnosis od 128 gastric polyps. Arq. Gastroenterol. 2017, 54, 263–266. [Google Scholar] [CrossRef] [Green Version]
- Park, H.R.; Min, K.; Kim, H.S.; Jung, W.W.; Park, Y.K. Expression of vascular endothelial growth factor-C and its receptor in osteosarcomas. Pathol. Res. Pract. 2008, 204, 575–582. [Google Scholar] [CrossRef]
- Meyer, J.S.; Alvarez, C.; Milikowski, C.; Olson, N.; Russo, I.; Russo, J.; Glass, A.; Zehnbauer, B.A.; Lister, K.; Parwaresch, R.; et al. Breast carcinoma malignancy grading by Bloom-Richardson system vs proliferation index: Reproducibility of grade and advantages of proliferation index. Mod. Pathol. 2005, 18, 1067–1078. [Google Scholar] [CrossRef]
- Elston, C.; Ellis, I. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Longacre, T.A.; Ennis, M.; Quenneville, L.A.; Bane, A.L.; Bleiweiss, I.J.; Carter, B.A.; Catelano, E.; Hendrickson, M.R.; Hibshoosh, H.; Layfield, L.J.; et al. Interobserver agreement and reproducibility in classification of invasive breast carcinoma: An NCI breast cancer family registry study. Mod. Pathol. 2006, 19, 195–207. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Guideline Update. Arch. Pathol Lab. Med. 2020, 144, 545–563. [Google Scholar] [CrossRef] [Green Version]
- Gomes, D.S.; Porto, S.S.; Balabram, D.; Gobbi, H. Inter-observer variability between general pathologists and a specialist in breast pathology in the diagnosis of lobular neoplasia, columnar cell lesions, atypical ductal hyperplasia and ductal carcinoma in situ of the breast. Diagn. Pathol. 2014, 9, 121. [Google Scholar] [CrossRef] [Green Version]
- Lakhani, S.R.; Ellis, I.O.; Schnitt, S.; Tan, P.H.; van de Vijver, M. WHO Classification of Tumours of the Breast, IV ed.; World Health Organization, International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- Elmore, J.G.; Longton, G.M.; Carney, P.A.; Geller, B.M.; Onega, T.; Tosteson, A.N.; Nelson, H.D.; Pepe, M.S.; Allison, K.H.; Schnitt, S.J.; et al. Diagnostic concordance among pathologists interpreting breast biopsy specimens. JAMA 2015, 313, 1122–1132. [Google Scholar] [CrossRef]
- Makela, K.; Hodgson, U.; Piilonen, A.; Kelloniemi, K.; Bloigu, R.; Sutinen, E.; Salmenkivi, K.; Ronty, M.; Lappi-Blanco, E.; Myllarniemi, M.; et al. Analysis of the Histologic Features Associated With Interobserver Variation in Idiopathic Pulmonary Fibrosis. Am. J. Surg. Pathol. 2018, 42, 672–678. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An Official ATS/ERSARS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-based Guidelines for Diagnosis and Management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef] [Green Version]
- Hashisako, M.; Tanaka, T.; Terasaki, Y.; Uekusa, T.; Achcar, R.D.; Aswad, B.I.; Bamefleh, H.S.; Capelozzi, V.L.; English, J.C.; Fabro, A.T.; et al. Interobserver Agreement of Usual Interstitial Pneumonia Diagnosis Correlated With Patient Outcome. Arch. Pathol. Lab. Med. 2016, 140, 1375–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grilley-Olson, J.E.; Hayes, D.N.; Moore, D.T.; Leslie, K.O.; Wilkerson, M.D.; Qaqish, B.F.; Hayward, M.C.; Cabanski, C.R.; Yin, X.Y.; Socinski, M.A.; et al. Validation of Interobserver Agreement in Lung Cancer Assessment: Hematoxylin-Eosin Diagnostic Reproducibility for Non-Small Cell Lung Cancer The 2004 World Health Organization Classification and Therapeutically Relevant Subsets. Arch. Pathol. Lab. Med. 2013, 137, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D.; Brambilla, E.; Muller-Hermelink, H.K.; Harris, C.C. World Health Organization classification of tumours. Am. J. Surg. Pathol. 2004, 10, 179–184. [Google Scholar]
- Thunnissen, E.; Beasley, M.B.; Borczuk, A.C.; Brambilla, E.; Chirieac, L.R.; Dacic, S.; Flieder, D.; Gazdar, A.; Geisinger, K.; Hasleton, P.; et al. Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study. Mod. Pathol. 2012, 25, 1574–1583. [Google Scholar] [CrossRef]
- Yoshizawa, A.; Motoi, N.; Riely, G.J.; Sima, C.S.; Gerald, W.L.; Kris, M.G.; Park, B.J.; Rusch, V.W.; Travis, W.D. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: Prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod. Pathol. 2011, 24, 653–664. [Google Scholar] [CrossRef]
- Nicholson, A.G.; Torkko, K.; Viola, P.; Duhig, E.; Geisinger, K.; Borczuk, A.C.; Hiroshima, K.; Tsao, M.S.; Warth, A.; Lantuejoul, S.; et al. Interobserver Variation among Pathologists and Refinement of Criteria in Distinguishing Separate Primary Tumors from Intrapulmonary Metastases in Lung. J. Thorac. Oncol. 2018, 13, 205–217. [Google Scholar] [CrossRef]
- Girard, N.; Deshpande, C.; Lau, C.; Finley, D.; Rusch, V.; Pao, W.; Travis, W.D. Comprehensive Histologic Assessment Helps to Differentiate Multiple Lung Primary Nonsmall Cell Carcinomas From Metastases. Am. J. Surg. Pathol. 2009, 33, 1752–1764. [Google Scholar] [CrossRef] [Green Version]
- Shi, K.H.; Compres, E.; Walton, K.E.; Mohan, L.S.; Zhang, B.; Panah, E.; Quan, V.T.L.; Garfield, E.M.; Khan, A.U.; Kim, D.; et al. Incorporation of dermoscopy improves inter-observer agreement among dermatopathologists in histologic assessment of melanocytic neoplasms. Arch. Dermatol. Res. 2021, 313, 101–108. [Google Scholar] [CrossRef]
- Furness, P.N.; Taub, N.; Assmann, K.J.M.; Banfi, G.; Cosyns, J.P.; Dorman, A.M.; Hill, C.M.; Kapper, S.K.; Waldherr, R.; Laurinavicius, A.; et al. International variation in histologic grading is large, and persistent feedback does not improve reproducibility. Am. J. Surg. Pathol. 2003, 27, 805–810. [Google Scholar] [CrossRef] [Green Version]
- Racusen, L.C.; Solez, K.; Colvin, R.B.; Bonsib, S.M.; Castro, M.C.; Cavallo, T.; Croker, B.P.; Demetris, A.J.; Drachenberg, C.B.; Fogo, A.B.; et al. The Banff 97 working classification of renal allograft pathology. Kidney Int. 1999, 55, 713–723. [Google Scholar] [CrossRef] [Green Version]
- Ganti, A.; Brown, H.J.; Gattuso, P.; Ghai, R.; Papagiannopoulos, P.; Batra, P.S.; Tajudeen, B.A. Inter-pathologist Agreement on Structured Histopathology Reporting in Chronic Rhinosinusitis. Ann. Otol. Rhinol. Laryngol. 2021, 130, 899–903. [Google Scholar] [CrossRef]
- Hasegawa, T.; Yamamoto, S.; Nojima, T.; Hirose, T.; Nikaido, T.; Yamashiro, K.; Matsuno, Y. Validity and reproducibility of histologic diagnosis and grading for adult soft-tissue sarcomas. Hum. Pathol. 2002, 33, 111–115. [Google Scholar] [CrossRef]
- Hasegawa, T.; Yokoyama, R.; Lee, Y.H.; Shimoda, T.; Beppu, Y.; Hirohashi, S. Prognostic relevance of a histological grading system using MIB-1 for adult soft-tissue sarcoma. Oncology 2000, 58, 66–74. [Google Scholar] [CrossRef]
- Tramm, T.; Di Caterino, T.; Jylling, A.M.B.; Lelkaitis, G.; Laenkholm, A.V.; Rago, P.; Tabor, T.P.; Talman, M.L.M.; Vouza, E.; Sci Comm, P.; et al. Standardized assessment of tumor-infiltrating lymphocytes in breast cancer: An evaluation of inter-observer agreement between pathologists. Acta Oncol. 2018, 57, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Salgado, R.; Denkert, C.; Campbell, C.; Savas, P.; Nuciforo, P.; Aura, C.; de Azambuja, E.; Eidtmann, H.; Ellis, C.E.; Baselga, J.; et al. Tumor-Infiltrating Lymphocytes and Associations With Pathological Complete Response and Event-Free Survival in HER2-Positive Early-Stage Breast Cancer Treated With Lapatinib and Trastuzumab A Secondary Analysis of the NeoALTTO Trial. JAMA Oncol. 2015, 1, 448–455. [Google Scholar] [CrossRef]
- Kilmartin, D.; O’Loughlin, M.; Andreu, X.; Bago-Horvath, Z.; Bianchi, S.; Chmielik, E.; Cserni, G.; Figueiredo, P.; Floris, G.; Foschini, M.P.; et al. Intra-Tumour Heterogeneity Is One of the Main Sources of Inter-Observer Variation in Scoring Stromal Tumour Infiltrating Lymphocytes in Triple Negative Breast Cancer. Cancers 2021, 13, 4410. [Google Scholar] [CrossRef]
- Phythian, C.J.; Cripps, P.J.; Grove-White, D.; Michalopoulou, E.; Duncan, J.S. Inter-observer agreement for clinical examinations of foot lesions of sheep. Vet. J. 2016, 216, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Hodgkinson, O. The importance of feet examination in sheep health management. Small Rumin. Res. 2010, 92, 67–71. [Google Scholar] [CrossRef]
- Winter, A. Lameness in sheep 1. Diagnosis. In Practice 2004, 26, 58–63. [Google Scholar] [CrossRef]
- Lidbury, J.A.; Hoffmann, A.R.; Ivanek, R.; Cullen, J.M.; Porter, B.F.; Oliveira, F.; Van Winkle, T.J.; Grinwis, G.C.; Sucholdolski, J.S.; Steiner, J.M. Interobserver Agreement Using Histological Scoring of the Canine. J. Vet. Intern. Med. 2017, 31, 778–783. [Google Scholar] [CrossRef]
- Ingh, T.S.G.A.M.v.d.; Winkle, T.J.V.; Cullen, J.M.; Charles, J.A.; Desmet, V.J. Chapter 7 Morphological classification of parenchymal disorders of the canine and feline liver: 2. Hepatocellular death, hepatitis and cirrhosis. In WSAVA Standards for Clinical and Histological Diagnosis of Canine and Feline Liver Disease; Saunders: Philadelphia, PA, USA, 2006; pp. 85–101. [Google Scholar]
- Goldschmidt, M.; Pena, L.; Rasotto, R.; Zappulli, V. Classification and Grading of Canine Mammary Tumors. Vet. Path. 2011, 48, 117–131. [Google Scholar] [CrossRef]
- Karayannopoulou, M.; Kaldrymidou, E.; Constantinidis, T.C.; Dessiris, A. Histological grading and prognosis in dogs with mammary carcinomas: Application of a human grading method. J. Comp. Pathol. 2005, 133, 246–252. [Google Scholar] [CrossRef]
- Northrup, N.C.; Howerth, E.W.; Harmon, B.G.; Brown, C.A.; Carmicheal, K.P.; Garcia, A.P.; Latimer, K.S.; Munday, J.S.; Rakich, P.M.; Richey, L.J.; et al. Variation among pathologists in the histologic grading of canine cutaneous mast cell tumors with uniform use of a single grading reference. J. Vet. Diagn. Investig. 2005, 17, 561–564. [Google Scholar] [CrossRef] [Green Version]
- Patnaik, A.K.; Ehler, W.J.; MacEwen, E.G. Canine cutaneous mast cell tumor: Morphologic grading and survival time in 83 dogs. Vet. Pathol. 1984, 21, 469–474. [Google Scholar] [CrossRef]
- Belluco, S.; Avallone, G.; Di Palma, S.; Rasotto, R.; Oevermann, A. Inter- and Intraobserver Agreement of Canine and Feline Nervous System Tumors. Vet. Pathol. 2019, 56, 342–349. [Google Scholar] [CrossRef]
- Higgins, R.J.; Bollen, A.W.; Dickinson, P.G.; Sisò-Llonch, S. Tumours of the nervous system. In Tumors in Domestic Animals, 5th ed.; Wiley, J., Ed.; 2017; Volume 98, pp. 891–934. [Google Scholar]
- Yap, F.W.; Rasotto, R.; Priestnall, S.L.; Parsons, K.J.; Stewart, J. Intra- and inter-observer agreement in histological assessment of canine soft tissue sarcoma. Vet. Comp. Oncol. 2017, 15, 1553–1557. [Google Scholar] [CrossRef] [Green Version]
- Dennis, M.M.; Reddacliff, L.A.; Whittington, R.J. Longitudinal study of clinicopathological features of Johne’s disease in sheep naturally exposed to Mycobacterium avium subspecies paratuberculosis. Vet. Pathol. 2011, 48, 565–575. [Google Scholar] [CrossRef]
- Zappulli, V.; Baldassarre, V.; Brunetti, B.; Burrai, G.P.; Cocumelli, C.; Grieco, V.; Iussich, S.; Maniscalco, V.; Mariotti, F.; Millanta, F.; et al. Linee Guida per la Diagnosi dei Processi Iperplastici/Displasici e Neoplastici della Mammella del Cane e del Gatto; AIPVet: Dolenjske Toplice, Slovenia, 2021. [Google Scholar]
- Fritz, A.G. International Classification of Diseases for Oncology: ICD-O, 3rd ed.; first revision; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research, 2nd ed.; Chapman & Hall/CRC: London, UK, 1991. [Google Scholar]
- Shoukri, M.M. Measures of Interobserver Agreement and Reliability; Chapman & Hall/CRC: London, UK, 2004. [Google Scholar]
- Szklo, M.a.N.F.J. Quality assurance and control. In Epidemiology: Beyond the Basis, 2nd ed.; Jones and Barlett: Sudbury, ON, Canada, 2006; pp. 297–350. [Google Scholar]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions; John Wiley and Sons: New York, USA, 2003. [Google Scholar]
- Joe, H.W. Hierarchical Grouping to Optimize an Objective Function, urldate = 2022-04-21. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar]
- Meuten, D.J.; Moore, F.M.; George, J.W. Mitotic Count and the Field of View Area: Time to Standardize. Vet. Pathol. 2016, 53, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Allison, K.H.; Reisch, L.M.; Carney, P.A.; Weaver, D.L.; Schnitt, S.J.; O’Malley, F.P.; Geller, B.M.; Elmore, J.G. Understanding diagnostic variability in breast pathology: Lessons learned from an expert consensus review panel. Histopathology 2014, 65, 240–251. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Lester, S.C.; Bose, S.; Chen, Y.Y.; Connolly, J.L.; de Baca, M.E.; Fitzgibbons, P.L.; Hayes, D.F.; Kleer, C.; O’Malley, F.P.; Page, D.L.; et al. Protocol for the examination of specimens from patients with invasive carcinoma of the breast. Arch. Pathol. Lab. Med. 2009, 133, 1515–1538. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; Hughes, M.T.; Fitzgerald, P.; Thompson, J.F.; Scolyer, R.A. Interobserver variation in the histopathologic reporting of key prognostic parameters, particularly clark level, affects pathologic staging of primary cutaneous melanoma. Ann. Surg. 2009, 249, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Scolyer, R.A.; Judge, M.J.; Evans, A.; Frishberg, D.P.P.; Prieto, V.G.; Thompson, J.F.; Trotter, M.J.; Walsh, M.Y.; Walsh, N.M.; Ellis, D.W. Data set for pathology reporting of cutaneous invasive melanoma: Recommendations from the international collaboration on cancer reporting (ICCR). Am. J. Surg. Pathol. 2013, 37, 1797–1814. [Google Scholar] [CrossRef]
- Reagan, J.K.; Selmic, L.E.; Fallon, C.; Driskell, E.A.; Garrett, L.D. Evaluation of information presented within mast cell tumour histopathology reports in the United States: 2012–2015. Vet. Med. Sci. 2018, 4, 252–262. [Google Scholar] [CrossRef]
- Taylor, L.A.; Eguchi, M.M.; Reisch, L.M.; Radick, A.C.; Shucard, H.; Kerr, K.F.; Piepkorn, M.W.; Knezevich, S.R.; Elder, D.E.; Barnhill, R.L.; et al. Histopathologic synoptic reporting of invasive melanoma: How reliable are the data? Cancer 2021, 127, 3125–3136. [Google Scholar] [CrossRef]
- Nurdjaja, V.; Yozu, M.; Mathy, J.A. Essential Components of Melanoma Histopathological Reporting: The Surgical Oncologist’s Perspective. J. Skin Cancer 2018, 2018, 9838410. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.H.; Kim, J.M.; Kang, G.H.; Chang, H.J.; Kang, D.W.; Kim, J.H.; Bae, J.M.; Seo, A.N.; Park, H.S.; Kang, Y.K.; et al. Standardized Pathology Report for Colorectal Cancer, 2nd Edition. J. Pathol. Transl. Med. 2020, 54, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.Y.; Park, S.Y.; Bae, Y.K.; Kim, J.Y.; Kim, E.K.; Kim, W.G.; Kwon, Y.; Lee, A.; Lee, H.J.; Lee, J.S.; et al. Standardized Pathology Report for Breast Cancer. J. Breast Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef]
- Santos, M.; Correia-Gomes, C.; Santos, A.; de Matos, A.; Rocha, E.; Lopes, C.; Pereira, P.D. Nuclear pleomorphism: Role in grading and prognosis of canine mammary carcinomas. Vet. J. 2014, 200, 426–433. [Google Scholar] [CrossRef]
- Gandomkar, Z.; Brennan, P.C.; Mello-Thoms, C. Computer-Assisted Nuclear Atypia Scoring of Breast Cancer: A Preliminary Study. J. Digit. Imaging 2019, 32, 702–712. [Google Scholar] [CrossRef]
- Mousavikhamene, Z.; Sykora, D.J.; Mrksich, M.; Bagheri, N. Morphological features of single cells enable accurate automated classification of cancer from non-cancer cell lines. Sci. Rep. 2021, 11, 24375. [Google Scholar] [CrossRef]
- Dimitriou, N.M.; Flores-Torres, S.; Kinsella, J.M.; Mitsis, G.D. Quantifying the Morphology and Mechanisms of Cancer Progression in 3D in-vitro environments: Integrating Experiments and Multiscale Models. bioRxiv 2022. [Google Scholar] [CrossRef]
- Sorenmo, K.U.; Kristiansen, V.M.; Cofone, M.A.; Shofer, F.S.; Breen, A.M.; Langeland, M.; Mongil, C.M.; Grondahl, A.M.; Teige, J.; Goldschmidt, M.H. Canine mammary gland tumours; a histological continuum from benign to malignant; clinical and histopathological evidence. Vet. Comp. Oncol. 2009, 7, 162–172. [Google Scholar] [CrossRef]
- Tan, P.H.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Webster, J.D.; Dennis, M.M.; Dervisis, N.; Heller, J.; Bacon, N.J.; Bergman, P.J.; Bienzle, D.; Cassali, G.; Castagnaro, M.; Cullen, J.; et al. Recommended guidelines for the conduct and evaluation of prognostic studies in veterinary oncology. Vet. Pathol. 2011, 48, 7–18. [Google Scholar] [CrossRef]
- Tanaka, Y.; Koyama, K.; Horiuchi, N.; Watanabe, K.; Kobayashi, Y. Relationship between Histological Grade and Histopathological Appearance in Canine Mammary Carcinomas. J. Comp. Pathol. 2020, 179, 59–64. [Google Scholar] [CrossRef]
- Nawaz, M.A.; Sewissy, A.A.; Soliman, T.H.A. Automated Classification of Breast Cancer Histology Images Using Deep Learning Based Convolutional Neural Networks. Int. J. Comput. Sci. Netw. Secur. 2018, 18, 152–160. [Google Scholar]
- Pantanowitz, L.; Hartman, D.; Qi, Y.; Cho, E.Y.; Suh, B.; Paeng, K.; Dhir, R.; Michelow, P.; Hazelhurst, S.; Song, S.Y.; et al. Accuracy and efficiency of an artificial intelligence tool when counting breast mitoses. Diagn. Pathol. 2020, 15, 80. [Google Scholar] [CrossRef]
- Lashen, A.; Ibrahim, A.; Katayama, A.; Ball, G.; Mihai, R.; Toss, M.; Rakha, E. Visual assessment of mitotic figures in breast cancer: A comparative study between light microscopy and whole slide images. Histopathology 2021, 79, 913–925. [Google Scholar] [CrossRef]
- Ginter, P.S.; Idress, R.; D’Alfonso, T.M.; Fineberg, S.; Jaffer, S.; Sattar, A.K.; Chagpar, A.; Wilson, P.; Harigopal, M. Histologic grading of breast carcinoma: A multi-institution study of interobserver variation using virtual microscopy. Mod. Pathol. 2021, 34, 701–709. [Google Scholar] [CrossRef]
- Rasotto, R.; Goldschmidt, M.H.; Castagnaro, M.; Carnier, P.; Caliari, D.; Zappulli, V. The dog as a natural animal model for study of the mammary myoepithelial basal cell lineage and its role in mammary carcinogenesis. J. Comp. Pathol. 2014, 151, 166–180. [Google Scholar] [CrossRef]
- Sánchez-Céspedes, R.; Millán, Y.; Guil-Luna, S.; Reymundo, C.; Espinosa de Los Monteros, A.; Martín de Las Mulas, J. Myoepithelial cells in canine mammary tumours. Vet. J. 2016, 207, 45–52. [Google Scholar] [CrossRef]
- Klaver, E.; van der Wel, M.; Duits, L.; Pouw, R.; Seldenrijk, K.; Offerhaus, J.; Visser, M.; Ten Kate, F.; Biermann, K.; Brosens, L.; et al. Performance of gastrointestinal pathologists within a national digital review panel for Barrett’s oesophagus in the Netherlands: Results of 80 prospective biopsy reviews. J. Clin. Pathol. 2021, 74, 48–52. [Google Scholar] [CrossRef]
- Oberbauer, A.M.; Belanger, J.M.; Famula, T.R. A Review of the Impact of Neuter Status on Expression of Inherited Conditions in Dogs. Front. Vet. Sci. 2019, 6, 397. [Google Scholar] [CrossRef]
- Fausak, E.D. A Mapping Study of Veterinary Literature on Perceptions and Attitudes of Female Canine Spaying. Front. Vet. Sci. 2020, 7, 559659. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Topic | Species | No. Pat | No. Cases | RD | Lesion Classification | Classification System | Grading System | Outcome | InterO Agreement | IntraO Agreement |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gilles et al., 2008 [15] | brain tumours | H | 5 | 229 | NA | histological criteria | NA | NA | weighted k | 0.65 | NA |
| Eefting et al., 2009 [16] | cartilagino-us tumours | H | 18 | 16 | NA | histological grade | NA | Evans (1977) [17] | weighted k | 0.58–0.78 | NA |
| Corazza et al., 2007 [18] | celiac disease | H | 6 | 60 | NA | histological criteria | Oberhuber (1999) [19] & Corazza (2005) [20] | NA | weighted k | 0.35–0.55 | NA |
| Rugge et al., 2021 [21] | gastric metaplasia | H | 3 | 74 | NA | histological criteria & IHC | Nagtegaal (2020) [22] | NA | weighted k | 0.7–0.9 | 0.7 k |
| Barbosa et al., 2017 [23] | gastric polyps | H | 3 | 128 | majority diagnosis | standard diagnosis | Park (2008) [24] | NA | unweighted k | 0.40–0.79 | NA |
| Meyer et al., 2005 [25] | HBC | H | 7 | 9000 | NA | histological grade & IHC | NA | Elston and Ellis (1991) [26] | unweighted k | 0.5–0.59 | NA |
| Longacre et al., 2006 [27] | HBC | H | 13 | 35 | NA | standard diagnosis & grade | structured report | Elston and Ellis (1991) [26] | unweighted k | 0.3–1 | NA |
| Adams et al., 2009 [10] | HBC | H | 5 | 38 | NA | histological grade | NA | Elston and Ellis (1991) [26] vs 2-tiered system | unweighted k | 0.32 vs. 0.47 | NA |
| Allison et al., 2014 [28] | HBC | H | 3 | 201 | NA | standard diagnosis | NR | NA | % agreement | 62.70% | NA |
| Gomes et al., 2014 [29] | HBC | H | 1 | 610 | original report | histological subtypes | Lakhani (2012) [30] | NA | unweighted k | 0.22–0.68 | NA |
| Elmore et al., 2015 [31] | HBC | H | 115 | 240 | 3 panel members | 4 categories | NR | NA | % agreement | 75.30% | NA |
| Mäkelä et al., 2018 [32]. | lung fibrosis | H | 4 | 60 | NA | 4 categories | Raghu (2011) [33] | NA | unweighted k | 0.4–0.77 | NA |
| Hashisako et al., 2016 [34] | lung (interstitial pneumonia) | H | 11 | 20 | NA | histological criteria | Raghu (2011) [33] | NA | unweighted k | 0.23 | NA |
| Grilley-Olson et al., 2012 [35] | lung tumours | H | 24 | 96 | majority diagnosis | standard diagnosis & categories | Travis (2004) [36] | NA | weighted k, bootstrap for IC | 0.25–0.48 | NA |
| Thunnissen et al., 2012 [37] | lung tumours | H | 26 (28) | 115 (64) | NA | standard diagnosis (invasion) | Yoshizawa (2011) [38] | NA | unweighted k | 0.38–0.77 (0.08–0.55) | NA |
| Nicholson et al., 2018 [39] | lung tumours | H | 16 | 126 | NA | histological criteria | Girard (2009) [40] | NA | unweighted k | 0.6 | NA |
| Shi et al., 2021 [41] | melanocytic neoplasms | H | 3 | 136 | NA | 3 categories | NR | NR | unweighted k | 0.496 | NA |
| Furness et al., 2003 [42]. | renal allografts | H | 21 | 85 | NA | histological criteria | Racusen (1999) [43] | NA | unweighted k | 0.2–0.4 | NA |
| Ganti et al., 2021 [44] | rhinosinusitis (chronic) | H | 2 | 92 | NA | histological criteria | Structured report | NA | unweighted k | 0.22–0.64 | NA |
| Hasegawa et al., 2002 [45] | soft tissue sarcomas | H | 4 | 130 | expert panel | standard diagnosis, grade & IHC | NR | Hasegawa (2000) [46] | % agreement, unweighted k | 75-100%, 0.34–0.86 | NA |
| Denkert et al., 2016 [11] | TILs in HBC | H | 32 & 28 | 120 | NA | semiquantitative percentage | web-based & software system | NA | ICC, unweighted k | 0.7 & 0.89, 0.45 & 0.63 | NA |
| Tramm et al., 2018 [47] | TILs in HBC | H | 9 | 124 | NA | cutoff categories | Salgado (2015) [48] | NA | ICC, unweighted k | 0.71, 0.38–0.46 | NA |
| Kilmartin et al., 2021 [49] | TILs in HBC | H | 23 | 49 | NA | absolute n. & cutoff categories | scoring digital tool (https://www.tilsinbreastcancer.org) | NA | ICC | 0.63 & 0.57 | NA |
| Phytian et al., 2016 [50] | foot lesions | O | 8 | 1158 | test standard observer | macroscopic criteria | Hodginkson (2010) [51] & Winter (2004) [52] | NA | unweighted k | 0.47–0.72 | NA |
| Lidbury et al., 2017 [53] | liver lesions | C | 6 | 50 | NA | scoring system | van den Ingh (2016) [54] | NA | unweighted k | 0.16–0.35 | NA |
| Chu et al., 2011 [9] | mammary tumours | C | 10 | 15 | NA | benign vs. malignant | NR | NA | unweighted k | 0.43 | NA |
| Santos et al., 2015 [8] | mammary tumours | C | 3 | 46 | 2 panel vet members | histological grade | Goldschmidt (2011) [55] | Karayannopoulou (2005) [56] | weighted & unweighted k | 0.5–0.7 | NA |
| Northrup et al., 2005 [57] | mast cell tumours | C | 10 | 60 | previous report | histological grade | NA | Patnaik (1984) [58] | % agreement, weighted k | 62.1%, 0.62 | NA |
| Belluco et al., 2019 [59] | nervous system tumours | C & F | 4 | 46 | neuropathologist | standard diagnosis & IHC | Higgins (2017) [60] | NA | unweighted k | 0.66–0.76 | NA |
| Yap et al., 2016 [61] | soft tissue sarcomas | C | 3 | 70 | NA | histological criteria & grade | Dennis (2011) [62] | Dennis (2011) [62] | ICC, unweighted k | 0.6 & 0.43k | 0.78–1 ICC |
| Lesions | ICD-O-3.2 Codes | Category |
|---|---|---|
| 1. Hyperplasia/Dysplasia | ||
| 1.1 Duct ectasia (DE) | NA | H |
| 1.2 Lobular hyperplasia (LH) (adenosis) | ||
| 1.2.1 regular (LH-R) | NA | H |
| 1.2.2 with secretory activity (LH-S) | NA | H |
| 1.2.3 with fibrosis (LH-F) | NA | H |
| 1.2.4 with atypia (LH-A) | NA | H |
| 1.3 Epitheliosis (EP) | NA | H |
| 1.4 Papillomatosis (PAP) | 8060/0 | H |
| 2. Benign epithelial neoplasms | ||
| 2.1 Simple benign tumours | ||
| 2.1.1 Adenoma—simple (SAD) | 8211/0 | B |
| 2.1.2 Myoepithelioma (MEP) | 8982/0 | B |
| 2.2 Non-simple benign tumours | ||
| 2.2.1 Complex adenoma (CAD) | 8983/0 | B |
| 2.2.2 Benign mixed tumour (BMT) | 8940/0 | B |
| 2.2.3 Fibroadenoma (FAD) | 9010/0 | B |
| 2.3 Ductal-associated benign tumours | ||
| 2.3.1 Ductal adenoma (DAD) | 8147/0 * | B |
| 2.3.2 Intraductal papillary adenoma (IDPA) | 8503/0 | B |
| 3. Malignant neoplasms | ||
| 3.1 Carcinoma–in situ | not applied | |
| 3.2 Simple carcinomas | ||
| 3.2.1 Tubular (including cribriform) carcinoma (STC) | 8211/3 | M |
| 3.2.2 Tubulopapillary carcinoma (STPC) | 8263/3 | M |
| 3.2.3 Solid carcinoma (SoC) | 8230/3 | M |
| 3.2.4 Invasive micropapillary carcinoma (IMPC) | 8507/3 | M |
| 3.2.5 Comedocarcinoma (CoC) | 8501/3 | M |
| 3.2.6 Anaplastic carcinoma (AC) | 8021/3 | M |
| 3.3 Non-simple carcinoma | ||
| 3.3.1 Carcinoma arising in complex adenoma/benign mixed tumour (C in B) | 8941/3 * | M |
| 3.3.2 Complex carcinoma (CC) | 8983/3 | M |
| 3.3.3 Carcinoma and malignant myoepithelioma (C&MM) | 8562/3 | M |
| 3.3.4 Mixed carcinoma (MC) | 8940/3 | M |
| 3.4 Ductal-associated carcinoma | ||
| 3.4.1 Ductal carcinoma (DC) | 8147/3 * | M |
| 3.4.2 Intraductal papillary carcinoma (including papillary-cystic) (IDPC) | 8503/3 | M |
| 4. Malignant epithelial neoplasms-special types | ||
| 4.1 Squamous cell carcinoma (SCC) | 8070/3 * | M |
| 4.2 Adenosquamous carcinoma (ASC) | 8560/3 * | M |
| 4.3 Mucinous carcinoma (MuC) | 8480/3 | M |
| 4.4 Lipid-rich carcinoma (LRC) | 8314/3 | M |
| 4.5 Spindle cell carcinoma (SPC) | 8572/3 * | M |
| 4.6 Malignant myoepithelioma (MM) | 8982/3 * | M |
| 5. Malignant mesenchymal neoplasms | ||
| 5.1 Osteosarcoma (OC) | 9180/3 * | M |
| 5.2 Chondrosarcoma (CS) | 9220/3 * | M |
| 5.3 Fibrosarcoma (FS) | 8810/3 * | M |
| 5.4 Hemangiosarcoma (HS) | 9120/3 * | M |
| 5.5 Other sarcomas (other S) | 8800/3 * | M |
| 6. Carcinosarcoma (CS) | 8980/3 * | M |
| 7. Hyperplasia/dysplasia of the Teat | ||
| 7.1 Melanosis of the skin of the teat (Skin M) | ND | H |
| 7.2 Hyperplasia of the teat (TH) | ND | H |
| 8. Neoplasms of the teat | ||
| 8.1 Benign ductal-associated neoplasms | ||
| 8.1.1 Ductal adenoma | 8147/0 * | B |
| 8.1.2 Intraductal papillary adenoma | 8503/0 | B |
| 8.2 Malignant ductal-associated neoplasms | ||
| 8.2.1 Ductal carcinoma | 8147/3 * | M |
| 8.2.2 Intraductal papillary carcinoma | 8503/3 | M |
| 8.3 Carcinoma with epidermal infiltration (Paget-like disease) (C-EI) | 8540/3 | M |
| Feature | Points |
|---|---|
| A. Tubules formation (a) | |
| Tubules comprise >75% of the tumour | 1 |
| Tubules comprise 10–75% of the tumour (moderate formation of tubules admixed with non-tubular areas) | 2 |
| Tubules comprise <10% (minimal or no tubule formation) | 3 |
| B. Nuclear pleomorphism (b) | |
| Uniform, regular, small nuclei with occasional small nucleoli | 1 |
| Moderate degree of variation in nuclear size and shape, hyperchromatic nucleus, presence of nucleoli (some of which can be prominent) | 2 |
| Marked variation in nuclear size, hyperchromatic nucleus, often with more than 1 prominent nucleoli | 3 |
| C. Mitoses per 10 hpf (c) | |
| 0–9/10 hpf | 1 |
| 10–19/10 hpf | 2 |
| 20 or more/10 hpf | 3 |
| Histological malignant grading | Totale score (A + B + C) |
| I (low, well differentiated) | 3–5 |
| II (intermediate, moderately differentiated) | 6–7 |
| III (high, poorly differentiated) | 8–9 |
| Age | Sex | Affiliation | Years of Experience * | Position, Titles (In Addition to DVM) | CMTs Biopsies (per Week) | Self-Assessment of Level of Confidence in CMTs (High/Medium/Low) | Considered an Expert by Colleagues on CMTs | Published Papers on MTs° |
|---|---|---|---|---|---|---|---|---|
| 34 | F | Private and University | 6 | Histopathology Consultant, PhD, ECVP | 15 | medium | NO | 0 |
| 46 | F | University | 15 | AP, PhD, ECVP | 5 | high | YES | 14 |
| 40 | M | University | 7 | AsP, PhD, ECVP | 2 | high | YES | 8 |
| 40 | M | IZS° | 10 | Senior Scientist | 10 | medium | NO | 0 |
| 57 | F | University | 25 | PhD | 3 | medium | NO | 2 |
| 48 | F | University | 20 | AP, MSc^ | 4 | medium | NO | 6 |
| 38 | F | IZS° | 10 | Senior Scientist, PhD | 7 | medium | NO | 6 |
| 54 | F | University | 10 | AsP | 4 | medium | NO | 4 |
| 49 | F | University | 20 | AP | 20 | high | YES | 16 |
| 45 | M | University | 14 | FP, PhD | 5 | medium | NO | 0 |
| 62 | F | University | 25 | FP, PhD | 2 | medium | NO | 0 |
| 38 | F | Private | 14 | Senior Consultant, PhD ECVP | 8 | high | YES | 12 |
| 42 | F | University | 15 | AsP | 2 | medium | NO | 1 |
| 48 | F | University | 17 | AP, PhD | 1 | medium | NO | 2 |
| 46 | F | University | 15 | FP, MSc, PhD, ECVP | 6 | high | YES | 21 |
| S-ID | P01 | P02 | P03 | P04 | P05 | P06 | P07 | P08 | P09 | P10 | P11 | P12 | P13 | P14 | P15 | GM |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | IDPA | IDPA | DC | DC | DC | IDPC | DC | IDPC | IDPC | DC | IDPC | IDPA | IDPC | DC | IDPC | |
| 2 | IMPC | IMPC | STC | IMPC | IMPC | IMPC | IMPC | IMPC | IMPC | IMPC | IMPC | STC | IMPC | IMPC | IMPC | IMPC |
| 3 | CAD | CAD | CC | CC | CC | CAD | CAD | CAD | CAD | CAD | CAD | CAD | CC | CAD | CAD | CAD |
| 4 | MC | C in B | MC | MC | MC | MC | MC | C in B | MC | MC | C in B | C in B | MC | C in B | MC | MC |
| 5 | DC | STPC | STPC | STPC | STPC | DC | IDPC | STPC | IDPC | IDPC | STPC | STPC | STPC | IDPC | IDPC | STPC |
| 6 | C-EI | STC | STC | STC | STC | IC | STPC | IMPC | STC | STPC | STC | IC | STC | CC | STC | STC |
| 7 | STPC | IDPA | IDPC | IDPA | IDPA | STPC | IDPC | DC | IDPA | IDPA | IDPA | IDPC | IDPA | DAD | IDPA | IDPA |
| 8 | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M | Skin M |
| 9 | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE | DE |
| 10 | STC | LH-A | SAD | LH-A | LH-A | STC | STC | SAD | DC | SAD | SAD | SAD | DAD | STC | DC | SAD |
| 11 | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC | CoC |
| 12 | EP | EP | LH-F | EP | EP | EP | EP | EP | LH-R | EP | EP | EP | EP | EP | LH-R | EP |
| 13 | IDPA | TH | C-EI | TH | TH | TH | TH | C-EI | TH | TH | TH | TH | PAP | TH | TH | TH |
| 14 | LRC | MM | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC | LRC |
| 15 | DAD | DAD | DAD | DAD | DAD | DAD | DAD | STC | DAD | DAD | DAD | DAD | SAD | SAD | DAD | DAD |
| 16 | TH | ASC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC | SCC |
| 17 | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC | MuC |
| 18 | FAD | LH-F | LH-A | LH-F | LH-F | FAD | V | LH-A | LH-A | LH-F | LH-F | LH-F | LH-F | FAD | LH-A | LH-F |
| 19 | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP | MEP |
| 20 | SPC | SPC | Other S | SPC | SPC | Other S | Other S | Other S | MM | Other S | Other S | Other S | FS | SoC | MM | Other S |
| 21 | AC | AC | IC | AC | AC | AC | AC | AC | AC | IC | AC | AC | AC | IC | AC | AC |
| 22 | LH-R | LH-R | LH-R | LH-R | LH-R | LH-R | LH-S | LH-F | LH-S | LH-R | LH-R | LH-R | LH-R | LH-R | LH-S | LH-R |
| 23 | PAP | PAP | PAP | PAP | PAP | PAP | PAP | PAP | PAP | PAP | PAP | PAP | LH-S | PAP | PAP | PAP |
| 24 | C in B | MC | MC | C in B | C in B | C in B | C in B | MC | MC | C in B | MC | MC | C in B | MC | MC | MC |
| 25 | ChS | OS | OS | OS | OS | ChS | OS | OS | OS | OS | OS | OS | Other S | OS | OS | OS |
| 26 | LH-F | FAD | FAD | FAD | FAD | LH-F | FAD | FAD | LH-F | LH-A | FAD | FAD | C&MM | LH-A | LH-F | FAD |
| 27 | SoC | LRC | LRC | LRC | LRC | LRC | LRC | SoC | LRC | SoC | LRC | LRC | Other S | LRC | LRC | LRC |
| 28 | SoC | DC | MM | SoC | SoC | SoC | DC | MM | DC | STC | DC | DC | DC | DC | DC | DC |
| 29 | SAD | SAD | CAD | CAD | CAD | SAD | LH-A | LH-A | LH-A | CC | LH-A | LH-A | CAD | LH-F | LH-A | LH-A |
| 30 | IDPC | IDPC | SoC | IDPC | IDPC | C&MM | C&MM | C&MM | SoC | ASC | C&MM | C&MM | SoC | STPC | SoC | C&MM |
| 31 | MM | C&MM | C&MM | C&MM | C&MM | MM | CC | SPC | CC | C&MM | CC | CC | MM | C&MM | CC | C&MM |
| 32 | BMT | BMT | C in B | BMT | BMT | BMT | BMT | BMT | CAD | BMT | BMT | BMT | BMT | BMT | CAD | BMT |
| 33 | ASC | IDPC | ASC | ASC | ASC | ASC | IDPA | ASC | ASC | C-EI | ASC | ASC | ASC | IDPA | ASC | ASC |
| 34 | CS | CS | CS | CS | CS | CS | CS | CS | CS | CS | CS | CS | OS | CS | CS | CS |
| 35 | LH-S | LH-S | LH-S | LH-S | LH-S | LH-S | SAD | LH-S | SAD | LH-S | LH-S | LH-S | LH-A | LH-S | SAD | LH-S |
| 36 | SCC | SoC | AC | HS | HS | HS | SoC | SoC | AC | HS | SoC | SoC | HS | AC | AC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papparella, S.; Crescio, M.I.; Baldassarre, V.; Brunetti, B.; Burrai, G.P.; Cocumelli, C.; Grieco, V.; Iussich, S.; Maniscalco, L.; Mariotti, F.; et al. Reproducibility and Feasibility of Classification and National Guidelines for Histological Diagnosis of Canine Mammary Gland Tumours: A Multi-Institutional Ring Study. Vet. Sci. 2022, 9, 357. https://doi.org/10.3390/vetsci9070357
Papparella S, Crescio MI, Baldassarre V, Brunetti B, Burrai GP, Cocumelli C, Grieco V, Iussich S, Maniscalco L, Mariotti F, et al. Reproducibility and Feasibility of Classification and National Guidelines for Histological Diagnosis of Canine Mammary Gland Tumours: A Multi-Institutional Ring Study. Veterinary Sciences. 2022; 9(7):357. https://doi.org/10.3390/vetsci9070357
Chicago/Turabian StylePapparella, Serenella, Maria Ines Crescio, Valeria Baldassarre, Barbara Brunetti, Giovanni P. Burrai, Cristiano Cocumelli, Valeria Grieco, Selina Iussich, Lorella Maniscalco, Francesca Mariotti, and et al. 2022. "Reproducibility and Feasibility of Classification and National Guidelines for Histological Diagnosis of Canine Mammary Gland Tumours: A Multi-Institutional Ring Study" Veterinary Sciences 9, no. 7: 357. https://doi.org/10.3390/vetsci9070357
APA StylePapparella, S., Crescio, M. I., Baldassarre, V., Brunetti, B., Burrai, G. P., Cocumelli, C., Grieco, V., Iussich, S., Maniscalco, L., Mariotti, F., Millanta, F., Paciello, O., Rasotto, R., Romanucci, M., Sfacteria, A., & Zappulli, V. (2022). Reproducibility and Feasibility of Classification and National Guidelines for Histological Diagnosis of Canine Mammary Gland Tumours: A Multi-Institutional Ring Study. Veterinary Sciences, 9(7), 357. https://doi.org/10.3390/vetsci9070357