A Comprehensive Overview of Polypharmacy in Elderly Patients in Saudi Arabia


Abstract
:1. Introduction
- Increased healthcare costs for elderly patients, prescribing inappropriate medications will contribute in extra cost for the patients as well as the healthcare system [9].
- Attributing the risk of adverse drug reaction, the risk of adverse drug reaction (ADR) is increased as the number of medications increases; therefore, it is expected that ADR is higher in geriatric patients [9].
- Prescription cascade, addition of medications due to misinterpreted ADRs will continue adding medication with being misdiagnosed [7].
- Drug–drug interaction, elderly patients are predisposed to drug–drug interactions, the probability of drug–drug interactions is increased as the utilization of a number of medications is increased [9].
- Patient compliance, elderly patients are more commonly not adherent to their medications because of its different and frequent regimens [9].
Age-Related Pharmacokinetics, Pharmacodynamics
2. Aims & Objectives
- To develop a full-framed picture about the utilization of medications for geriatric patients
- To review the percentage of older adults with five medications or more.
- To investigate the association between polypharmacy and comorbidities in elderly patients.
3. Methodology
3.1. Study Sitting and Area
3.2. Study Design
3.3. Study Population
3.4. Sample Size
3.4.1. Population Characteristics
3.4.2. Inclusion Criteria
- Male and female patients aged 65 and older.
- Patients received appropriate medications.
3.4.3. Exclusion Criteria
- Patients who are receiving non-systemic or short-duration medications.
- Male and female patients who are younger than 65 years old.
- People aged 65 who did not take any medication.
- Healthy people.
3.5. Data Collection Tools and Techniques
3.5.1. Database Collection
3.5.2. Medication(s) Count
3.6. Statistical Analysis Consideration
3.7. Ethical Consideration/Approval
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations. Global Issues (Ageing). Available online: http://www.un.org/en/sections/issues-depth/ageing/ (accessed on 29 March 2018).
- Kim, L.D.; Koncilja, K.; Nielsen, C. Medication management in older adults. Clevel. Clin. J. Med. 2018, 85, 129–135. [Google Scholar] [CrossRef]
- Whitson, H.E.; Boyd, C.M. Managing Multiple Comorbidities. UpToDate. (Updated May 2018). Available online: https://www.uptodate.com/contents/managing-multiple-comorbidities (accessed on 29 March 2018).
- World Bank. World Databank: World Development Indicators (1960–2014). Available online: https://data.worldbank.org/country/saudi-arabia (accessed on 3 April 2018).
- Khoja, A.T.; Aljawadi, M.H.; Al-Shammari, S.A.; Mohamed, A.G.; Al-Manaa, H.A.; Morlock, L.; Ahmed, S.; Khoja, T.A.M. The health of Saudi older adults; results from the Saudi National Survey for Elderly Health (SNSEH) 2006–2015. Saudi Pharm. J. 2018, 26, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.S.; Shati, M.; Keshtkar, A.; Malakouti, S.K.; Bazargan, M.; Assari, S. Defining polypharmacy in the elderly: A systematic review protocol. BMJ Open 2016, 6, e010989. [Google Scholar] [CrossRef]
- Rochon, P.A. Drug Prescribing for Older Adults. UpToDate. (Updated November 2018). Available online: https://www.uptodate.com/contents/drug-prescribing-for-older-adults (accessed on 29 March 2018).
- Payne, R.A. The epidemiology of polypharmacy. Clin. Med. (London). 2016, 16, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salazar, J.A.; Poon, I.; Nair, M. Clinical consequences of polypharmacy in elderly: Expect the unexpected, think the unthinkable. Expert Opin. Drug Saf. 2007, 6, 695–704. [Google Scholar] [CrossRef]
- Jansen, P.A.; Brouwers, J.R. Clinical pharmacology in old persons. Sci. (Cairo) 2012, 2012, 723678. [Google Scholar] [CrossRef]
- Wells, B.; DiPiro, J.; Schwinghammer, T.; DiPiro, C. Pharmacotherapy Handbook, 9th ed.; McGraw-Hill: New York, NY, USA, 2015; p. 879. [Google Scholar]
- Alvis, B.D.; Hughes, C.G. Physiology Considerations in Geriatric Patients. Anesthesiol Clin. 2015, 33, 447–456. [Google Scholar] [CrossRef]
- Lai, S.W.; Liao, K.F.; Liao, C.C. Polypharmacy correlates with increased risk for hip fracture in the elderly: A population-based study. Med. (Baltim.) 2010, 89, 5. [Google Scholar] [CrossRef]
- Rawle, M.J.; Cooper, R.; Kuh, D.; Richards, M. Associations Between Polypharmacy and Cognitive and Physical Capability: A British Birth Cohort Study. J. Am. Geriatr. Soc. 2018, 66, 916–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangoni, A.A.; Jackson, S.H.D. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2004, 57, 6–14. [Google Scholar] [CrossRef]
- Davies, E.A.; O’Mahony, M.S. Adverse drug reactions in special populations—The elderly. Br. J. Clin. Pharmacol. 2015, 80, 796–807. [Google Scholar] [CrossRef] [PubMed]
- General Authority of Statistics in Kingdom of Saudi Arabia-Elderly Survey (2017). Available online: https://www.stats.gov.sa/sites/default/files/elderly_survey2017ar.pdf (accessed on 29 March 2018).
- Linjakumpu, T.; Hartikainen, S.; Klaukka, T.; Veijola, J.; Sirkka-LiisaKivelä, R. Use of medications and polypharmacy are increasing among the elderly. Epidemiology 2002, 55, 809–817. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. Bmc Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef]
- Maher, R.L.; Hanlon, J.T.; Hajjar, E.R. Clinical Consequences of Polypharmacy in Elderly. Expert Opin. Drug Saf. 2014, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, J.; Michaud, V.; Steffen, L. The Dangers of Polypharmacy in Elderly Patients. JAMA Intern. Med. 2017, 177, 1544. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashar, A.; Al Sinawi, H.; Al Mahrizi, A.; Al-Hatrushi, M. Prevalence and Covariates of Polypharmacy in Elderly Patients on Discharge from a Tertiary Care Hospital in Oman. Oman. Med. J. 2016, 31, 421–425. [Google Scholar] [CrossRef]
- Qato, D.M.; Alexander, G.C.; Conti, R.; Johnson, M.; Schumm, P.; Lindau, S.T. Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA 2008, 300, 2867–2878. [Google Scholar]
- Charlson, M.E.; Pomcpei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Evans, D.C.; Cook, C.H.; Christy, J.M. Comorbidity–polypharmacy scoring facilitates outcome prediction in older trauma patients. J. Am. Geriatr. Soc. 2012, 60, 1465–1470. [Google Scholar] [CrossRef]
- Rozzini, R.; Frisoni, G.B.; Ferrucci, L.; Barbisoni, P.; Sabatini, T.; Ranieri, P.; Guralnik, J.M.; Trabucchi, M. Geriatric Index of Comorbidity: Validation and comparison with other measures of comorbidity. Age Ageing 2002, 31, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Molokhia, M.; Majeed, A. Current and future perspectives on the management of polypharmacy. BMC Fam. Pract. 2017, 18, 70. [Google Scholar] [CrossRef] [PubMed]
- Mair, A.; Fernandez-Llimos, F.; Alonso, A.; Harrison, C.; Hurding, S.; Kempen, T.G.H.; Kinnear, M.; Michael, N.; McIntosh, J.; Wilson, M.; et al. The Simpathy Consortium. Polypharmacy Management by 2030: A Patient Safety Challenge. Available online: https://openair.rgu.ac.uk/handle/10059/2493 (accessed on 29 March 2018).
- Gurwitz, J.H.; Field, T.S.; Harrold, L.R.; Rothschild, J.; Debellis, K.; Seger, A.C.; Cadoret, C.; Fish, L.S.; Garber, L.; Kelleher, M.; et al. Incidence and Preventability of Adverse Drug Events Among Older Persons in the Ambulatory Setting. JAMA 2003, 289, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Guharoy, R. Polypharmacy: America’s other drug problem. Am. J. Health-Syst. Pharm. 2017, 74, 1305–1306. [Google Scholar] [CrossRef] [PubMed]
- Mubarak, N.; Makramalla, E.; Albur, U.; Kumar, A. Prevalence of poly-pharmacy in the elderly: Implications of age, gender, comorbidities and drug interactions. J. Pharm. Pharm. Sci. 2014, 1, 1–7. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
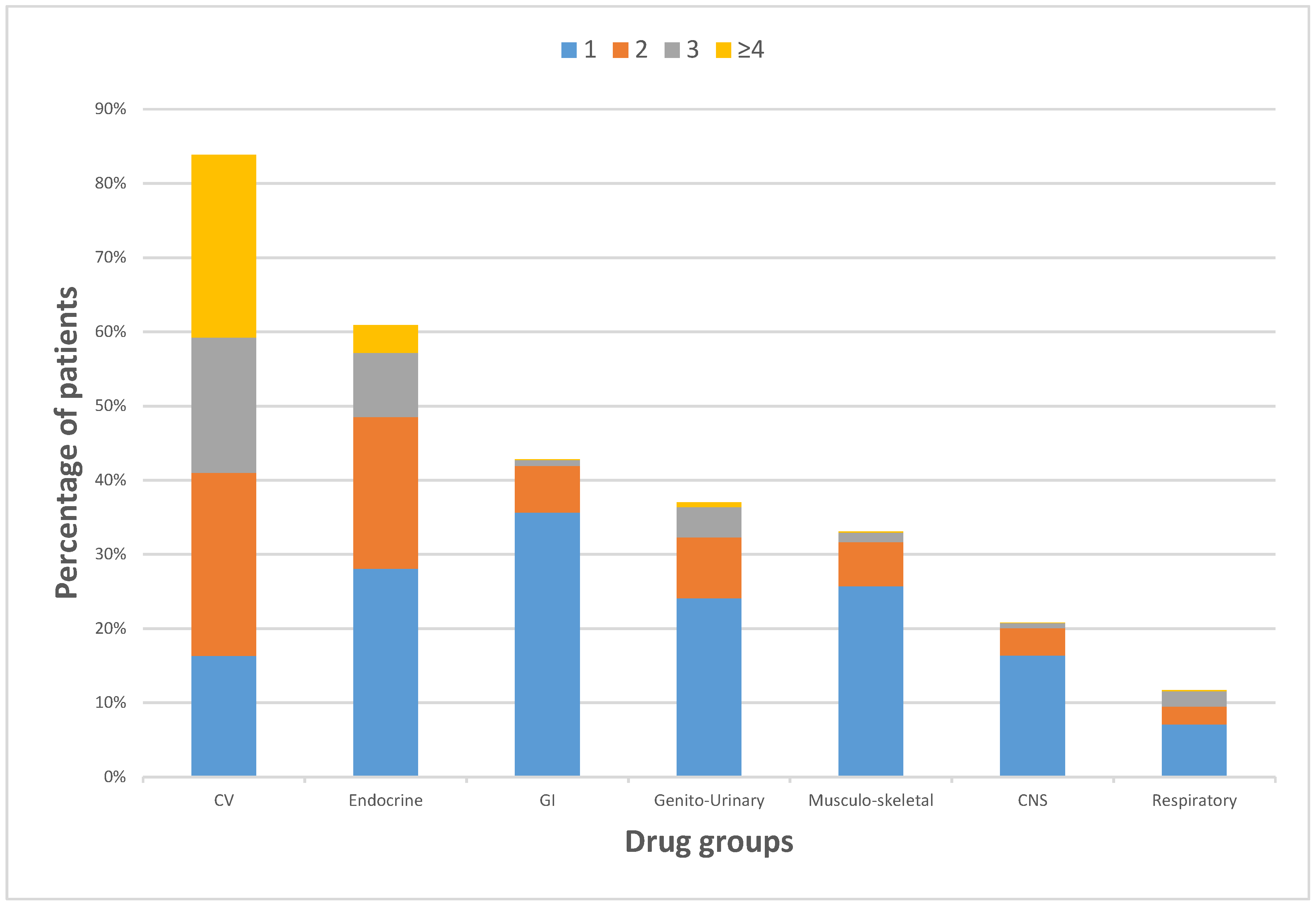
| Drugs by Body System: (% of All Patients) | Number of Patients Per Drug Quantity | ||||
|---|---|---|---|---|---|
| 0 Drugs | 1 Drug | 2 Drugs | 3 Drugs | 4 Drugs | |
| Cardiovascular System Drug(s) (83.88%) | 485 patients | 491 patients | 742 patients | 549 patients | 742 patients |
| Endocrine System Drug(s) (60.91%) | 1176 patients | 845 patients | 615 patients | 260 patients | 113 patients |
| Gastro-intestinal System Drug(s) (42.83%) | 1720 patients | 1073 patients | 189 patients | 24 patients | 3 patients |
| Genito-urinary System Drug(s) (37.02%) | 1895 patients | 725 patients | 247 patients | 123 patients | 19 patients |
| Musculoskeletal System Drug(s) (33.06%) | 2014 patients | 774 patients | 178 patients | 39 patients | 4 patients |
| Nervous System Drug(s) (20.80%) patients | 2383 patients | 493 patients | 111 patients | 20 patients | 2 patients |
| Respiratory System Drug(s) (11.69%) | 2657 patients | 213 patients | 72 patients | 63 patients | 4 patients |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsuwaidan, A.; Almedlej, N.; Alsabti, S.; Daftardar, O.; Al Deaji, F.; Al Amri, A.; Alsuwaidan, S. A Comprehensive Overview of Polypharmacy in Elderly Patients in Saudi Arabia. Geriatrics 2019, 4, 36. https://doi.org/10.3390/geriatrics4020036
Alsuwaidan A, Almedlej N, Alsabti S, Daftardar O, Al Deaji F, Al Amri A, Alsuwaidan S. A Comprehensive Overview of Polypharmacy in Elderly Patients in Saudi Arabia. Geriatrics. 2019; 4(2):36. https://doi.org/10.3390/geriatrics4020036
Chicago/Turabian StyleAlsuwaidan, Aseel, Norah Almedlej, Sawsan Alsabti, Omamah Daftardar, Fawzi Al Deaji, Ali Al Amri, and Salem Alsuwaidan. 2019. "A Comprehensive Overview of Polypharmacy in Elderly Patients in Saudi Arabia" Geriatrics 4, no. 2: 36. https://doi.org/10.3390/geriatrics4020036
APA StyleAlsuwaidan, A., Almedlej, N., Alsabti, S., Daftardar, O., Al Deaji, F., Al Amri, A., & Alsuwaidan, S. (2019). A Comprehensive Overview of Polypharmacy in Elderly Patients in Saudi Arabia. Geriatrics, 4(2), 36. https://doi.org/10.3390/geriatrics4020036