Cognitive Flexibility and Inhibition in Individuals with Age-Related Hearing Loss

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Audiological Evaluation
2.3. Cognitive Flexibility and Inhibition Evaluation
2.3.1. Verbal Fluency
2.3.2. TMT-B
2.3.3. D-KEFS Stroop
2.3.4. Go/NoGo Tasks
2.4. Statistical Analysis
3. Results
3.1. Group Differences
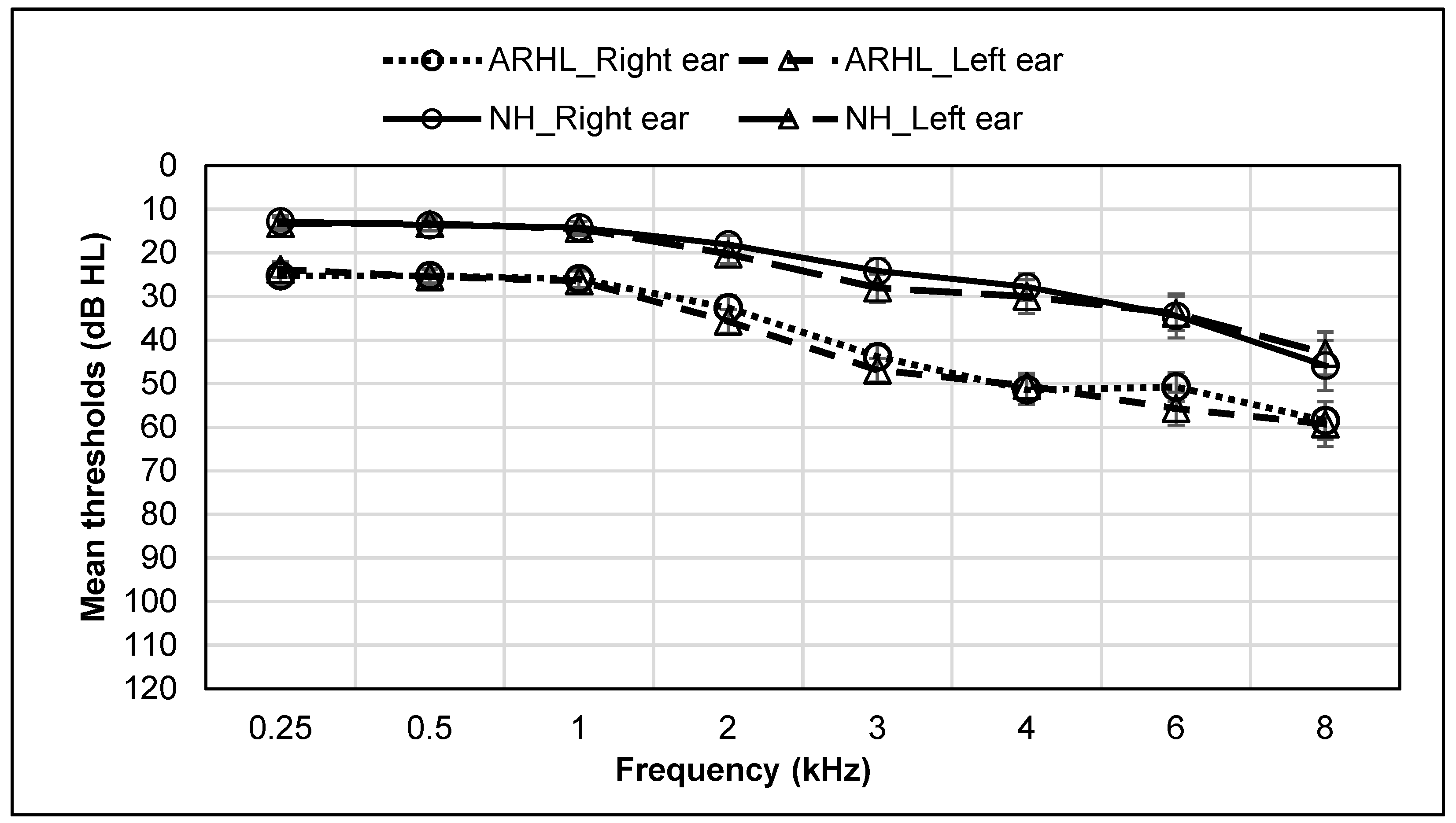
3.1.1. Audiological Measures
3.1.2. Cognitive Flexibility and Inhibition Measures
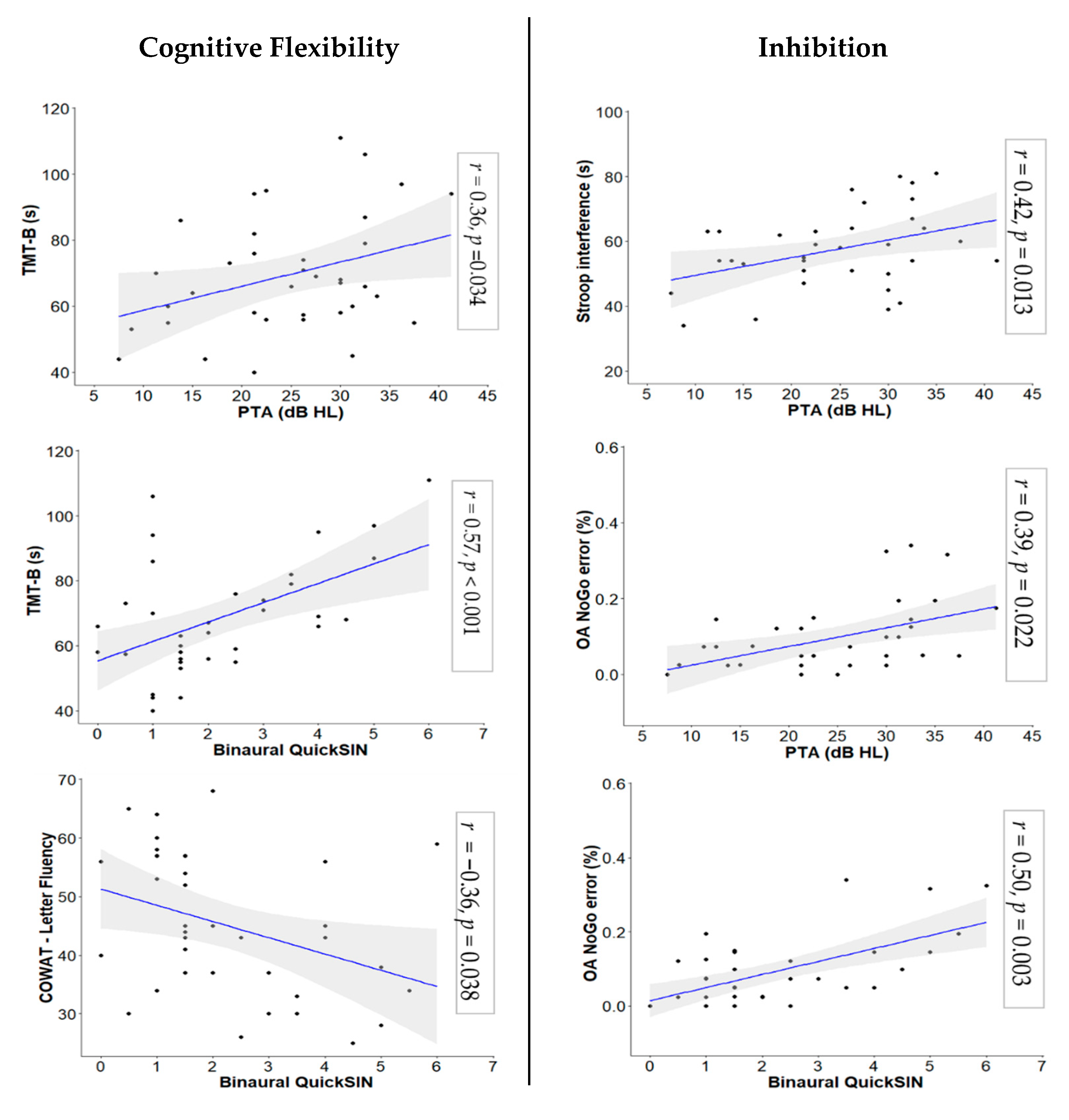
3.2. Correlations
4. Discussion
4.1. Inhibition
4.2. Cognitive Flexibility
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruickshanks, K.J.; Tweed, T.S.; Wiley, T.L.; Klein, B.E.K.; Klein, R.; Chappell, R.; Nondahl, D.M.; Dalton, D.S. The 5-Year Incidence and Progression of Hearing Loss. Arch. Otolaryngol. Neck Surg. 2003, 129, 1041. [Google Scholar] [CrossRef] [Green Version]
- Quaranta, N.; Coppola, F.; Casulli, M.; Barulli, O.; Lanza, F.; Tortelli, R.; Capozzo, R.; Leo, A.; Tursi, M.; Grasso, A.; et al. The prevalence of peripheral and central hearing impairment and its relation to cognition in older adults. Audiol. Neurotol. 2015, 19, 10–14. [Google Scholar] [CrossRef]
- National Institute on Deafness and Other Communication Disorders. Age-related hearing loss (presbyacusis). In NIDCD Fact Sheet; National Institute on Deafness and Other Communication Disorders: Bethesda, MD, USA, 2016; pp. 1–6. [Google Scholar]
- Chmiel, R.; Jerger, J. Hearing aid use, central auditory disorder, and hearing handicap in elderly persons. J. Am. Acad. Audiol. 1996, 7, 190–202. [Google Scholar] [PubMed]
- Humes, L.E.; Dubno, J.R.; Gordon-salant, S.; Lister, J.J.; Anthony, T.; Cruickshanks, K.J.; Gates, G.A.; Wilson, R.H.; Sciences, H.; Surgery, N.; et al. Central Presbycusis: A Review and Evaluation of the Evidence. J. Am. Acad. Audiol. 2012, 23, 635–666. [Google Scholar] [CrossRef] [PubMed]
- Arlinger, S. Negative consequences of uncorrected hearing loss—A review. Int. J. Audiol. 2003, 42 (Suppl. 2), 2S17–2S20. [Google Scholar] [CrossRef]
- Huang, Q.; Tang, J. Age-related hearing loss or presbycusis. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 1179–1191. [Google Scholar] [CrossRef]
- Jerger, J.; Jerger, S.; Oliver, T.; Pirozzolo, F. Speech understanding in the elderly. Ear Hear. 1989, 10, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Divenyi, P.L.; Stark, P.B.; Haupt, K.M. Decline of speech understanding and auditory thresholds in the elderly. J. Acoust. Soc. Am. 2005, 118, 1089–1100. [Google Scholar] [CrossRef]
- Frisina, R.D.; Walton, J.P. Age-related structural and functional changes in the cochlear nucleus. Hear. Res. 2006, 216–217, 216–223. [Google Scholar] [CrossRef]
- Atcherson, S.R.; Nagaraj, N.K.; Kennett, S.E.W.; Levisee, M. Overview of Central Auditory Processing Deficits in Older Adults. Semin. Hear. 2015, 36, 150–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humes, L.E.; Young, L.A. Sensory-cognitive interactions in older adults. Ear Hear. 2016, 37, 52S–61S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, K.; Ross, B. Effects of age and age-related hearing loss on the brain. J. Commun. Disord. 2007, 40, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Li-Korotky, H.S. Age-related hearing loss: Quality of care for quality of life. Gerontologist 2012, 52, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Liljas, A.E.M.; Walters, K.; de Oliveira, C.; Wannamethee, S.G.; Ramsay, S.E.; Carvalho, L.A. Self-Reported Sensory Impairments and Changes in Cognitive Performance: A Longitudinal 6-Year Follow-Up Study of English Community-Dwelling Adults Aged ≥50 Years. J. Aging Health 2018, 1–19. [Google Scholar] [CrossRef]
- Hällgren, M.; Larsby, B.; Lyxell, B.; Arlinger, S. Evaluation of a cognitive test battery in young and elderly normal-hearing and hearing-impaired persons. J. Am. Acad. Audiol. 2001, 12, 357–370. [Google Scholar]
- Humes, L.E. Factors underlying the speech-recognition performance of elderly hearing-aid wearers. J. Acoust. Soc. Am. 2002, 112, 1112–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentler, R.A. Effectiveness of directional microphones and noise reduction schemes in hearing aids: A systematic review of the evidence. J. Am. Acad. Audiol. 2005, 16, 473–484. [Google Scholar] [CrossRef]
- Kochkin, S. Increasing hearing aid adoption through multiple environmental listening utility. Hear. J. 2007, 60, 28–31. [Google Scholar] [CrossRef] [Green Version]
- Boxtel, M.V.; Beijsterveldt, V.C.; Jolles, V.P. Mild Hearing Impairment Can Reduce Verbal Memory Performance in a Healthy Adult Population. J. Clin. Exp. Neuropsychol. 2003, 22, 147–154. [Google Scholar] [CrossRef]
- Bucks, R.S.; Dunlop, P.D.; Taljaard, D.S.; Brennan-Jones, C.G.; Hunter, M.; Wesnes, K.; Eikelboom, R.H. Hearing loss and cognition in the Busselton Baby Boomer cohort: An epidemiological study. Laryngoscope 2016, 126, 2367–2375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, A.; Shah, K.; Hough, O.; Hynynen, K. Focused ultrasound-mediated drug delivery through the blood–brain barrier. Expert Rev. Neurother. 2016, 15, 477–491. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.R. Hearing loss and cognition among older adults in the United States. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66 A, 1131–1136. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.R.; Ferrucci, L.; Metter, E.J.; An, Y.; Zonderman, A.B.; Resnick, S.M. Hearing Loss and Cognition in the Baltimore Longitudinal Study of Aging. Neuropsychology 2011, 25, 763–770. [Google Scholar] [CrossRef] [Green Version]
- Rönnberg, J.; Lunner, T.; Zekveld, A.; Sörqvist, P.; Danielsson, H.; Lyxell, B.; Dahlström, Ö.; Signoret, C.; Stenfelt, S.; Pichora-Fuller, M.K.; et al. The Ease of Language Understanding (ELU) model: Theoretical, empirical, and clinical advances. Front. Syst. Neurosci. 2013, 7, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humes, L.E. Understanding the speech-understanding problems of older adults. Am. J. Audiol. 2013, 22, 303–305. [Google Scholar] [CrossRef]
- Humes, L.E.; Kidd, G.R.; Lentz, J.J. Auditory and cognitive factors underlying individual differences in aided speech-understanding among older adults. Front. Syst. Neurosci. 2013, 7, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Janse, E. A non-auditory measure of interference predicts distraction by competing speech in older adults. Aging Neuropsychol. Cogn. 2012, 19, 741–758. [Google Scholar] [CrossRef] [Green Version]
- Van Rooij, J.C.G.M.; Plomp, R. Auditive and cognitive factors in speech perception by elderly listeners. II: Multivariate analyses. J. Acoust. Soc. Am. 1990, 88, 2611–2624. [Google Scholar] [CrossRef] [PubMed]
- Mackie, M.A.; Van Dam, N.T.; Fan, J. Cognitive control and attentional functions. Brain Cogn. 2013, 82, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [Green Version]
- Kane, M.J.; Hasher, L.; Stoltzfus, E.R.; Zacks, R.T.; Connelly, S.L. Inhibitory attentional mechanisms and aging. Psychol. Aging 1994, 9, 103–112. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervera, T.C.; Soler, M.J.; Dasi, C.; Ruiz, J.C. Speech recognition and working memory capacity in young-elderly listeners: Effects of hearing sensitivity. Can. J. Exp. Psychol. 2009, 63, 216–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foo, C.; Rudner, M.; Rönnberg, J.; Lunner, T. Recognition of Speech in Noise with New Hearing Instrument Compression Release Settings Requires Explicit Cognitive Storage and Processing Capacity. J. Am. Acad. Audiol. 2008, 18, 618–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granick, S.; Kleban, M.H.; Weiss, A.D. Relationships between hearing loss and cognition in normally hearing aged persons. J. Gerontol. 1976, 31, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, M.J.S.; Van Gerven, P.W.M. Disregarding hearing loss leads to overestimation of age-related cognitive decline. Neurobiol. Aging 2017, 56, 180–189. [Google Scholar] [CrossRef]
- Harrison Bush, A.; Lister, J.; Lin, F.; Betz, J.; Edwards, J. Peripheral Hearing and Cognition: Evidence from the Staying Keen in Later Life (SKILL) Study. Ear Hear. 2015, 36, 395–407. [Google Scholar] [CrossRef] [Green Version]
- Ren, F.; Luo, J.; Ma, W.; Xin, Q.; Xu, L.; Fan, Z.; Ai, Y.; Zhao, B.; Gao, F.; Wang, H. Hearing loss and cognition among older adults in a Han Chinese cohort. Front. Neurosci. 2019, 13, 1–11. [Google Scholar] [CrossRef]
- Souza, P.E.; Arehart, K.H.; Shen, J.; Anderson, M.; Kates, J.M. Working memory and intelligibility of hearing-aid processed speech. Front. Psychol. 2015, 6, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, R.J.; Munro, K.J. Predictors of aided speech recognition, with and without frequency compression, in older adults. Int. J. Audiol. 2015, 54, 467–475. [Google Scholar] [CrossRef] [Green Version]
- Ellis, R.J.; Molander, P.; Rönnberg, J.; Lyxell, B.; Andersson, G.; Lunner, T. Predicting speech-in-noise recognition from performance on the trail making test: Results from a large-scale internet study. Ear Hear. 2016, 37, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Knight, S.; Heinrich, A. Different measures of auditory and visual stroop interference and their relationship to speech intelligibility in noise. Front. Psychol. 2017, 8, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Knight, S.; Heinrich, A. Visual inhibition measures predict speech-in-noise perception only in people with low levels of education. Front. Psychol. 2019, 9. [Google Scholar] [CrossRef]
- Lunner, T. Cognitive function in relation to hearing aid use. Int. J. Audiol. 2003, 42, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Lunner, T.; Sundewall-Thorén, E. Interactions between Cognition, Compression, and Listening Conditions: Effects on Speech-in-Noise Performance in a Two-Channel Hearing Aid. J. Am. Acad. Audiol. 2008, 18, 604–617. [Google Scholar] [CrossRef] [Green Version]
- Nagaraj, N.K. Working Memory and Speech Comprehension in Older Adults With Hearing Impairment. J. Speech Lang. Hear. Res. 2017, 60, 2949. [Google Scholar] [CrossRef]
- Moore, D.R.; Edmondson-Jones, M.; Dawes, P.; Fortnum, H.; McCormack, A.; Pierzycki, R.H.; Munro, K.J. Relation between speech-in-noise threshold, hearing loss and cognition from 40–69 years of age. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Ng, E.H.N.; Rudner, M.; Lunner, T.; Rönnberg, J. Relationships between self-report and cognitive measures of hearing aid outcome. SpeechLang. Hear. 2013, 16, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Jayakody, D.M.P.; Friedland, P.L.; Eikelboom, R.H.; Martins, R.N.; Sohrabi, H.R. A novel study on association between untreated hearing loss and cognitive functions of older adults: Baseline non-verbal cognitive assessment results. Clin. Otolaryngol. 2018, 43, 182–191. [Google Scholar] [CrossRef]
- Na, W.; Kim, G.; Kim, G.; Han, W.; Kim, J. Clinical Interventions in Aging Dovepress effects of hearing loss on speech recognition under distracting conditions and working memory in the elderly. Clin. Interv. Aging 2017, 2017, 1175–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zekveld, A.A.; Deijen, J.B.; Goverts, S.T.; Kramer, S.E. The Relationship Between Nonverbal Cognitive Functions and Hearing Loss. J. SpeechLang. Hear. Res. 2007, 50, 74–82. [Google Scholar] [CrossRef]
- Arehart, K.; Souza, P.; Baca, R.; Kates, J. Working Memory, Age, and Hearing Loss: Susceptibility to Hearing Aid Distortion. Ear Hear. 2013, 34. [Google Scholar] [CrossRef] [Green Version]
- Rudner, M.; Lunner, T.; Behrens, T.; Thorén, E.S.; Rönnberg, J. Working Memory Capacity May Influence Perceived Effort during Aided Speech Recognition in Noise. J. Am. Acad. Audiol. 2012, 23, 577–589. [Google Scholar] [CrossRef]
- Somnath, A.; Gundmi, A.; Bhargavi, P.; Rai, S. Comparison of cognitive functions in elderly population with and without hearing loss. Indian J. Otol. 2020, 26, 163–167. [Google Scholar] [CrossRef]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Si-monsick, E.M.; et al. Hearing Loss and Cognitive Decline in Older Adults. JAMA Intern. Med. 2013, 173, 293. [Google Scholar] [CrossRef]
- Deal, J.A.; Sharrett, A.R.; Albert, M.S.; Coresh, J.; Mosley, T.H.; Knopman, D.; Wruck, L.M.; Lin, F.R. Hearing impairment and cognitive decline: A pilot study conducted within the atherosclerosis risk in communities Neurocognitive Study. Am. J. Epidemiol. 2015, 181, 680–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croll, P.H.; Vinke, E.J.; Armstrong, N.M.; Licher, S.; Vernooij, M.W.; Baatenburg de Jong, R.J.; Goedegebure, A.; Ikram, M.A. Hearing loss and cognitive decline in the general population: A prospective cohort study. J. Neurol. 2020, 268, 860–871. [Google Scholar] [CrossRef]
- Huber, M.; Roesch, S.; Pletzer, B.; Lukaschyk, J.; Lesinski-Schiedat, A.; Illg, A. Cognition in older adults with severe to profound sensorineural hearing loss compared to peers with normal hearing for age. Int. J. Audiol. 2020, 59, 254–262. [Google Scholar] [CrossRef]
- Valentijn, S.; Boxtel, M.; Hooren, S.; Bosma, H.; Beckers, H.; Ponds, R.; Jolles, J. Change in Sensory Functioning Predicts Change in Cognitive Functioning: Results from a 6-Year Follow-Up in the Maastricht Aging Study. J. Am. Geriatr. Soc. 2005, 53, 374–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, W.S.; Kalluri, S.; Pentony, S.; Nooraei, N. Predicting the effect of hearing loss and audibility on amplified speech reception in a multi-talker listening scenario. J. Acoust. Soc. Am. 2013, 133, 4268–4278. [Google Scholar] [CrossRef]
- Van Knijff, E.C.; Coene, M.; Govaerts, P.J. Speech understanding in noise in elderly adults: The effect of inhibitory control and syntactic complexity. Int. J. Lang. Commun. Disord. 2018, 53, 628–642. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.; Phillips, N.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Almeida, S.A. Short versions of the geriatric depression scale: A study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int. J. Geriatr. Psychiatry 1999, 14, 858–865. [Google Scholar] [CrossRef]
- ANSI Specification for Audiometers; American National Standards Institute: New York, NY, USA, 2010.
- Carhart, R.; Jerger, J. Preferred method for clinical determination of pure-tone thresholds. J. Speech Hear. Disord. 1959, 24, 330–345. [Google Scholar] [CrossRef]
- Tillman, T.; Carhart, R. An expanded test for speech discrimination utilizing CNC monosyllabic words. Northwestern University Auditory Test No. 6. SAM-TR-66-55. Tech. Rep. Sam-Tr. 1966, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Killion, M.C.; Niquette, P.A.; Gudmundsen, G.I.; Revit, L.J.; Banerjee, S.; Killion, M.C.; Niquette, P.A.; Gudmundsen, G.I. Development of a quick speech-in-noise test for measuring signal-to-noise ratio loss in normal-hearing and hearing-impaired listeners. J. Acoust. Soc. Am. 2004, 116, 2395–2405. [Google Scholar] [CrossRef]
- Goodglass, H.; Kaplan, E.; Weintraub, S.; Barresi, B. Boston Diagnostic Aphasia Examination 2001, 1 Box (1 Book, 1 Video, 3 Books of Picture Cards); Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Benton, A.; Hamsher, K. Multilingual Aphasia Examination, 2nd ed.; AJA Associates: Iowa City, IA, USA, 1976. [Google Scholar]
- Reitan, R.M. Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Holdnack, J. Reliability and validity of the Delis-Kaplan Executive Function System: An update. J. Int. Neuropsychol. Soc. 2004, 10, 301–303. [Google Scholar] [CrossRef]
- Maguire, M.J.; Brier, M.R.; Moore, P.S.; Ferree, T.C.; Ray, D.; Mostofsky, S.; Hart, J.; Kraut, M.A. The influence of perceptual and semantic categorization on inhibitory processing as measured by the N2-P3 response. Brain Cogn. 2009, 71, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Mudar, R.; Chiang, H.-S.; Eroh, J.; Nguyen, L.; Maguire, M.; Spence, J.; Kung, F.; Kraut, M.; Hart, J. The Effects of Amnestic Mild Cognitive Impairment on Go/NoGo Semantic Categorization Task Performance and Event-Related Potentials. J. Alzheimer’s Dis. 2016, 50, 577–590. [Google Scholar] [CrossRef] [Green Version]
- Mudar, R.; Chiang, H.-S.; Maguire, M.; Spence, J.; Eroh, J.; Kraut, M.; Heart, J., Jr. Effects of Age on Cognitive Control during Semantic Categorization. Behav. Brain Res. 2015. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.T.; Mudar, R.A.; Chiang, H.-S.; Schneider, J.M.; Maguire, M.J.; Kraut, M.A.; Hart, J. Theta and Alpha Alterations in Amnestic Mild Cognitive Impairment in Semantic Go/NoGo Tasks. Front. Aging Neurosci. 2017, 9, 160. [Google Scholar] [CrossRef] [Green Version]
- Littman, R.; Takács, Á. Do all inhibitions act alike? A study of go/no-go and stop-signal paradigms. PLoS ONE 2017, 12, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Akeroyd, M.A. Are individual differences in speech reception related to individual differences in cognitive ability? A survey of twenty experimental studies with normal and hearing-impaired adults. Int. J. Audiol. 2008, 47. [Google Scholar] [CrossRef] [PubMed]
- Brännström, K.J.; Karlsson, E.; Waechter, S.; Kastberg, T. Extended high-frequency pure tone hearing thresholds and core executive functions. Int. J. Audiol. 2018, 57, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Eckert, M.A.; Cute, S.L.; Vaden, K.I.; Kuchinsky, S.E.; Dubno, J.R. Auditory cortex signs of age-related hearing loss. JARO J. Assoc. Res. Otolaryngol. 2012, 13, 703–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, M.A.; Vaden, K.I.; Dubno, J.R. Age-Related Hearing Loss Associations With Changes in Brain Morphology. Trends Hear. 2019, 23, 1–14. [Google Scholar] [CrossRef]
- Dubno, J.R.; Lee, F.-S.; Matthews, L.J.; Ahlstrom, J.B.; Horwitz, A.R.; Mills, J.H. Longitudinal changes in speech recognition in older persons. J. Acoust. Soc. Am. 2008, 123, 462–475. [Google Scholar] [CrossRef]
- Lee, F.-S.; Matthews, L.J.; Dubno, J.R.; Mills, J.H. Longitudinal study of pure-tone thresholds in older persons. Ear Hear. 2005, 26, 1–11. [Google Scholar] [CrossRef]
- Vallesi, A. Targets and non-targets in the aging brain: A go/nogo event-related potential study. Neurosci. Lett. 2011, 487, 313–317. [Google Scholar] [CrossRef]
- Kuchinsky, S.E.; Vaden, K.I.; Ahlstrom, J.B.; Cute, S.L.; Humes, L.E.; Dubno, J.R.; Eckert, M.A. Task-Related Vigilance during Word Recognition in Noise for Older Adults with Hearing Loss. Exp. Aging Res. 2016, 42, 64–85. [Google Scholar] [CrossRef] [Green Version]
- McDowd, J.M. Inhibition in attention and aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1997, 52, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Lustig, C.; Hasher, L.; Zacks, R.T. Inhibitory deficit theory: Recent developments in a “new view.”. Inhib. Cogn. 2008, 145–162. [Google Scholar] [CrossRef]
- Hu, S.; Ide, J.S.; Chao, H.H.; Castagna, B.; Fischer, K.A.; Zhang, S.; Li, C.S. Structural and functional cerebral bases of diminished inhibitory control during healthy aging. Hum. Brain Mapp. 2018, 39, 5085–5096. [Google Scholar] [CrossRef]
- Hasher, L.; Stoltzfus, E.R.; Zacks, R.T.; Rypma, B. Age and Inhibition. J. Exp. Psychol. Learn. Mem. Cogn. 1991, 17, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Hasher, L.; Lustig, C.; Zacks, R. Inhibitory mechanisms and the control of attention. In Variation in Working Memory; Oxford University Press: New York, NY, USA, 2007; pp. 227–249. ISBN1 0-19-516863-1. ISBN2 978-0-19-516863-1. [Google Scholar]
- Hartmann, L.; Wachtl, L.; de Lucia, M.; Spierer, L. Practice-induced functional plasticity in inhibitory control interacts with aging. Brain Cogn. 2019, 132, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.D.; Craik, F.I.M. 50 Years of Cognitive Aging Theory. J. Gerontol. Ser. B 2017, 72, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Stenbäck, V.; Hällgren, M.; Lyxell, B.; Larsby, B. The Swedish Hayling task, and its relation to working memory, verbal ability, and speech-recognition-in-noise. Scand. J. Psychol. 2015, 56, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Sommers, M.S.; Danielson, S.M. Inhibitory processes and spoken word recognition in young and older adults: The interaction of lexical competition and semantic context. Psychol. Aging 1999, 14, 458–472. [Google Scholar] [CrossRef]
- Brännström, K.J.; Kastberg, T.; Waechter, S.; Karlsson, E. Hearing thresholds and cognitive flexibility in young healthy individuals with normal hearing. Int. J. Audiol. 2020, 59, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Ellis, R.J.; Munro, K.J. Does cognitive function predict frequency compressed speech recognition in listeners with normal hearing and normal cognition? Int. J. Audiol. 2013, 52, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Classon, E.; Löfkvist, U.; Rudner, M.; Rönnberg, J. Verbal fluency in adults with postlingually acquired hearing impairment. SpeechLang. Hear. 2014, 17, 88–100. [Google Scholar] [CrossRef]
- Whitson, H.E.; Cronin-Golomb, A.; Cruickshanks, K.J.; Gilmore, G.C.; Owsley, C.; Peelle, J.E.; Recanzone, G.; Sharma, A.; Swenor, B.; Yaffe, K.; et al. American Geriatrics Society and National Institute on Aging Bench-to-Bedside Conference: Sensory Impairment and Cognitive Decline in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 2052–2058. [Google Scholar] [CrossRef] [PubMed]
- Van Rooij, J.C.G.M.; Plomp, R. Auditive and cognitive factors in speech perception by elderly listeners. III. Additional data and final discussion. J. Acoust. Soc. Am. 1992, 91, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Pichora-Fuller, M.K. Cognitive Decline and Hearing Health Care for Older Adults. Am. J. Audiol. 2015, 24, 108–111. [Google Scholar] [CrossRef] [Green Version]
- Pichora-Fuller, M.K. Cognitive aging and auditory information processing. Int. J. Audiol. 2003, 42, 26–32. [Google Scholar] [CrossRef]
- Lindenberger, U.; Baltes, P. Sensory Functioning and Intelligence in Old Age: A Strong Connection. Psychol. Aging 1994, 9, 339–355. [Google Scholar] [CrossRef] [PubMed]
- Cohen, G. Review article: Speech comprehension in the elderly: The effects of cognitive changes. Br. J. Audiol. 1987, 21, 221–226. [Google Scholar] [CrossRef]
- CHABA. Committee on Hearing, Bioacoustics, and Biomechanics, Commission on Behavioral and Social Sciences and Education, National Research Council. J. Acoust. Soc. Am. 1988, 83, 859–895. [Google Scholar]
- Baltes, P.B.; Lindenberger, U. Emergence of a powerful connection between sensory and cognitive functions across the adult life span: A new window to the study of cognitive aging? Psychol. Aging 1997, 12, 12–21. [Google Scholar] [CrossRef]
- Humes, L.E. Associations Between Measures of Auditory Function and Brief Assessments of Cognition. Am. J. Audiol. 2020, 1–13. [Google Scholar] [CrossRef]
- Kurylo, D.D.; Corkin, S.; Allard, T.; Zatorre, R.J.; Growdon, J.H. Auditory function in Alzheimer’s disease. Neurology 1993, 43, 1893–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swords, G.M.; Nguyen, L.T.; Mudar, R.A.; Llano, D.A. Auditory system dysfunction in Alzheimer disease and its prodromal states: A review. Ageing Res. Rev. 2018, 44, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Tuwaig, M.; Savard, M.; Jutras, B.; Poirier, J.; Collins, D.L.; Rosa-Neto, P.; Fontaine, D.; Breitner, J.C.S. Deficit in Central Auditory Processing as a Biomarker of Pre-Clinical Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 60, 1589–1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates, G.A.; Anderson, M.L.; McCurry, S.M.; Feeney, M.P.; Larson, E.B. Central auditory dysfunction as a harbinger of Alzheimer dementia. Arch. Otolaryngol. Head. Neck Surg. 2011, 137, 390–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, J.D.; Lister, J.J.; Elias, M.N.; Tetlow, A.M.; Sardina, A.L.; Sadeq, N.A.; Brandino, A.D.; Harrison Bush, A.L. Auditory Processing of Older Adults With Probable Mild Cognitive Impairment. J. Speech. Lang. Hear. Res. 2017, 60, 1427–1435. [Google Scholar] [CrossRef] [PubMed]
- Sardone, R.; Battista, P.; Donghia, R.; Lozupone, M.; Tortelli, R.; Guerra, V.; Grasso, A.; Griseta, C.; Castellana, F.; Zupo, R.; et al. Age-Related Central Auditory Processing Disorder, MCI, and Dementia in an Older Population of Southern Italy. Otolaryngol. Neck Surg. 2020, 163, 348–355. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| ARHL Group | NH Group | |
|---|---|---|
| Total N | 21 | 18 |
| Age (years) | 71.29 (7.90) | 67.11 (5.46) |
| Education (years) | 17.76 (3.43) | 17.83 (1.65) |
| Sex | 12F/9M | 12F/6M |
| ARHL Group | NH Group | p-Value | |
|---|---|---|---|
| Better ear PTA (dB HL) | 32.61 (6.69) | 16.59 (5.82) | 0.000 * |
| Right SRT (dB HL) | 31.19 (9.60) | 19.72 (5.80) | 0.000 * |
| Left SRT (dB HL) | 31.67 (6.58) | 19.44 (5.91) | 0.000 * |
| Right WRS (%) | 94.29 (10.62) | 98.44 (2.79) | 0.116 |
| Left WRS (%) | 94.67 (8.61) | 98.22 (4.79) | 0.128 |
| Right QuickSIN | 6.00 (3.15) | 2.80 (1.79) | 0.001 * |
| Left QuickSIN | 5.69 (3.26) | 3.02 (2.02) | 0.005 * |
| Binaural QuickSIN | 3.69 (2.86) | 1.58 (1.08) | 0.006 * |
| ARHL Group | NH Group | p-Value | |
|---|---|---|---|
| Category Fluency | 20.38 (4.96) | 22.72 (4.95) | 0.150 |
| COWAT-Letter Fluency | 43.29 (12.38) | 48.28 (12.80) | 0.224 |
| TMT-B (s) | 77.11 (25.28) | 65.27 (16.49) | 0.098 |
| Stroop mixing cost | 5.90 (17.50) | 8.89 (17.54) | 0.599 |
| Stroop color-word interference (s) | 62.62 (13.41) | 53.39 (8.99) | 0.018 * |
| SC RT a (ms) | 350.25 (51.58) | 343.51 (35.85) | 0.647 |
| SC Go error a (%) | 0.04 (0.10) | 0.96 (0.16) | 0.306 |
| SC NoGo error a (%) | 0.14 (0.10) | 0.08 (0.05) | 0.030 * |
| OA RT a (ms) | 420.85 (40.65) | 438.10 (36.74) | 0.180 |
| OA Go error a (%) | 0.05 (0.06) | 0.04 (0.07) | 0.618 |
| OA NoGo error a (%) | 0.18 (0.21) | 0.05 (0.05) | 0.016 * |
| PTA (dB HL) a | Binaural QuickSIN Score b | |
|---|---|---|
| Cognitive Flexibility | ||
| Category Fluency | −0.25 | −0.26 |
| COWAT-Letter Fluency | −0.21 | −0.36 * |
| TMT-B (s) | 0.36 * | 0.57 * |
| Stroop mixing cost | −0.10 | 0.05 |
| Inhibition | ||
| Stroop color-word interference (s) | 0.42 * | 0.20 |
| SC NoGo error (%) | 0.33 | 0.41 |
| OA NoGo error (%) | 0.39 * | 0.50 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shende, S.A.; Nguyen, L.T.; Lydon, E.A.; Husain, F.T.; Mudar, R.A. Cognitive Flexibility and Inhibition in Individuals with Age-Related Hearing Loss. Geriatrics 2021, 6, 22. https://doi.org/10.3390/geriatrics6010022
Shende SA, Nguyen LT, Lydon EA, Husain FT, Mudar RA. Cognitive Flexibility and Inhibition in Individuals with Age-Related Hearing Loss. Geriatrics. 2021; 6(1):22. https://doi.org/10.3390/geriatrics6010022
Chicago/Turabian StyleShende, Shraddha A., Lydia T. Nguyen, Elizabeth A. Lydon, Fatima T. Husain, and Raksha A. Mudar. 2021. "Cognitive Flexibility and Inhibition in Individuals with Age-Related Hearing Loss" Geriatrics 6, no. 1: 22. https://doi.org/10.3390/geriatrics6010022
APA StyleShende, S. A., Nguyen, L. T., Lydon, E. A., Husain, F. T., & Mudar, R. A. (2021). Cognitive Flexibility and Inhibition in Individuals with Age-Related Hearing Loss. Geriatrics, 6(1), 22. https://doi.org/10.3390/geriatrics6010022