
The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
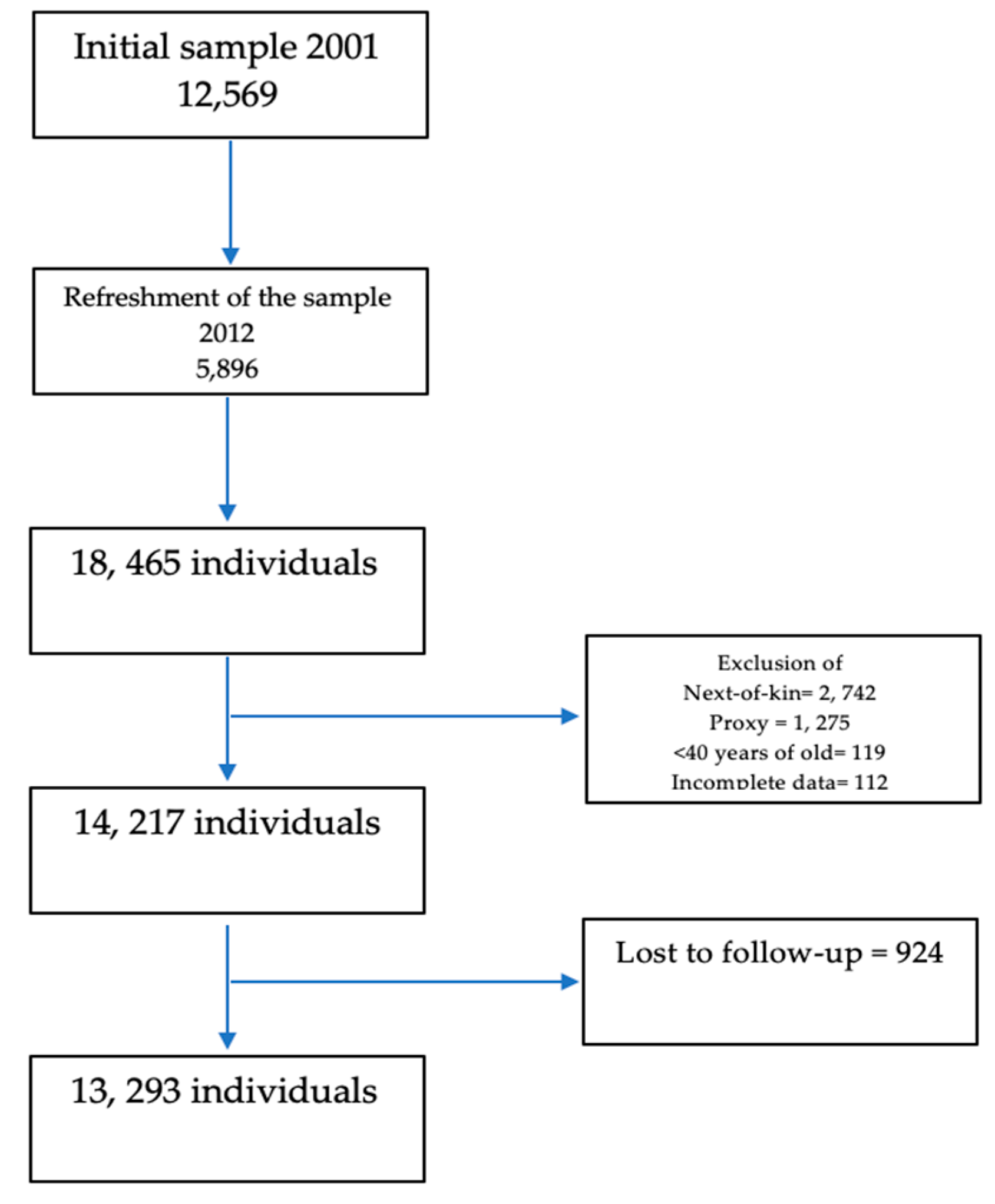
2.1. Study Population
2.2. Exposure Variable, Outcome Variables, and Covariables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bessa, B.; Ribeiro, O.; Coelho, T. Assessing the social dimension of frailty in old age: A systematic review. Arch. Gerontol. Geriatr. 2018, 78, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Northwood, M.; Ploeg, J.; Markle-Reid, M.; Sherifali, D. Integrative review of the social determinants of health in older adults with multimorbidity. J. Adv. Nurs. 2017, 74, 45–60. [Google Scholar] [CrossRef]
- Commission on Social Determinants of Health; World Health Organization; Marmot, M.G. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.-P.; Morley, J.E.; Ong, P.; et al. Frailty: An emerging public health priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Bulled, N.; Ostrach, B.; Mendenhall, E. Syndemics and the biosocial conception of health. Lancet 2017, 389, 941–950. [Google Scholar] [CrossRef]
- Andrew, M.K.; Keefe, J.M. Social vulnerability from a social ecology perspective: A cohort study of older adults from the National Population Health Survey of Canada. BMC Geriatr. 2014, 14, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogendijk, E.O.; van Hout, H.P.; Heymans, M.W.; van der Horst, H.E.; Frijters, D.H.; van Groenou, M.I.B.; Deeg, D.J.; Huisman, M. Explaining the association between educational level and frailty in older adults: Results from a 13-year longitudinal study in the Netherlands. Ann. Epidemiol. 2014, 24, 538–544.e2. [Google Scholar] [CrossRef] [PubMed]
- Grundy, E.M.; Tomassini, C. Marital history, health and mortality among older men and women in England and Wales. BMC Public Health 2010, 10, 554. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.P.; Jin, A.; Feng, L.; Nyunt, M.S.Z.; Chow, K.Y.; Feng, L.; Fong, N.P. Mortality of older persons living alone: Singapore Longitudinal Ageing Studies. BMC Geriatr. 2015, 15, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luanaigh, C.O.; Lawlor, B.A. Loneliness and the health of older people. Int. J. Geriatr. Psychiatry 2008, 23, 1213–1221. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social relationships and mortality risk: A meta-analytic review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef]
- Hill, T.D.; Saenz, J.; Rote, S.M. Religious participation and mortality risk in Mexico. J. Gerontol. B Psychol. Sci. Soc. Sci. 2018. [CrossRef]
- Hoogendijk, E.O.; Rijnhart, J.J.; Kowal, P.; Pérez-Zepeda, M.U.; Cesari, M.; Abizanda, P.; Ruano, T.F.; Schop-Etman, A.; Huisman, M.; Dent, E. Socioeconomic inequalities in frailty among older adults in six low- and middle-income countries: Results from the WHO Study on global AGEing and adult health (SAGE). Maturitas 2018, 115, 56–63. [Google Scholar] [CrossRef]
- Andrew, M.K.; Mitnitski, A.B.; Rockwood, K. Social vulnerability, frailty and mortality in elderly people. PLoS ONE 2008, 3, e2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitnitski, A.B.; E Graham, J.; Mogilner, A.J.; Rockwood, K. Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr. 2002, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrew, M.K.; Dupuis-Blanchard, S.; Maxwell, C.; Giguere, A.; Keefe, J.; Rockwood, K.; John, P.S. Social and societal implications of frailty, including impact on Canadian healthcare systems. J. Frailty Aging 2018, 7, 217–223. [Google Scholar]
- Armstrong, J.J.; Godin, J.; Launer, L.J.; White, L.R.; Mitnitski, A.; Rockwood, K.; Andrew, M.K. Changes in frailty predict changes in cognition in older men: The Honolulu-Asia Aging Study. J. Alzheimers Dis. 2016, 53, 1003–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, J.J.; Andrew, M.K.; Mitnitski, A.; Launer, L.J.; White, L.R.; Rockwood, K. Social vulnerability and survival across levels of frailty in the Honolulu-Asia Aging Study. Age Ageing 2015, 44, 709–712. [Google Scholar] [CrossRef] [Green Version]
- Ouvrard, C.; Avila-Funes, J.A.; Dartigues, J.; Amieva, H.; Tabue-Teguo, M. The social vulnerability index: Assessing replicability in predicting mortality over 27 years. J. Am. Geriatr. Soc. 2019, 67, 1305–1306. [Google Scholar] [CrossRef]
- Wallace, L.M.K.; Theou, O.; Pena, F.; Rockwood, K.; Andrew, M.K. Social vulnerability as a predictor of mortality and disability: Cross-country differences in the survey of health, aging, and retirement in Europe (SHARE). Aging Clin. Exp. Res. 2015, 27, 365–372. [Google Scholar] [CrossRef]
- Andrew, M.K.; Mitnitski, A.; Kirkland, S.A.; Rockwood, K. The impact of social vulnerability on the survival of the fittest older adults. Age Ageing 2012, 41, 161–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Zepeda, M.U.; Avila-Funes, J.A.; Gutierrez-Robledo, L.M. Frailty across age groups. J. Frailty Aging 2016, 5, 15–19. [Google Scholar]
- Wong, R.; Michaels-Obregon, A.; Palloni, A. Cohort profile: The Mexican Health and Aging Study (MHAS). Int. J. Epidemiol. 2017, 46, e2. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Palloni, A.; Gutierrez-Robledo, L.M. MHAS Mexican Health and Aging Study 2012. In Data Files and Documentation (PUBLIC use): Mexican Health and Aging Study, (Methodological Document); Branch, U.T.M., Ed.; MHAS: Galveston, TX, USA, 2014; Available online: www.MHASweb.org (accessed on 7 March 2021).
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, P.; Beirness, D.; Gliksman, L. Alcohol and Health in Canada: A Summary of Evidence and Guidelines for Low Risk Drinking. Canadian Centre on Substance Abuse. 2011. Available online: www.ccsa.ca/2011%20CCSA%20Documents/2011-Summary-of-Evidence-and-Guidelines-for-Low-Risk%20Drinking-en.pdf (accessed on 7 March 2021).
- Pérez-Zepeda, M.U.; Castrejón-Pérez, R.C.; Wynne-Bannister, E.; García-Peña, C. Frailty and food insecurity in older adults. Public Health Nutr. 2016, 19, 2844–2849. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Zepeda, M.U.; García-Peña, C.; Sánchez-Garrido, N.; Wynne-Bannister, E.G.; Moreno-Peniche, B. Collective violence and the health of the elderly: A cross-sectional analysis of a population-based national survey in Mexico. Rev. Panam. Salud Pública 2017, 41, e29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 14,217) | Men (n = 5959) | Women (n = 8379) | |
|---|---|---|---|
| Age, mean (SD) | 63.9 (10.1) | 65.2 (9.6) | 63 (10.2) |
| Physically active, n (%) | 5603 (39.4) | 2843 (48.1) | 2760 (33.2) |
| Tobacco use, n (%) | |||
| Never | 8931 (62.8) | 2352 (39.8) | 6579 (79.2) |
| Former user | 3553 (24.9) | 2427 (41) | 1126 (13.5) |
| Current user | 1733 (12.1) | 1134 (19.1) | 599 (7.2) |
| High-risk alcohol drinking, n (%) | 1330 (9.3) | 1019 (17.2) | 311 (3.7) |
| Social vulnerability index, mean (SD) | 0.42 (0.12) | 0.39 (0.11) | 0.43 (0.12) |
| Frailty index, mean (SD) | 0.23 (0.11) | 0.2 (0.1) | 0.25 (0.1) |
| Alive (n = 12,508) | Dead (n = 785) | p-Value * | |
|---|---|---|---|
| Age Categories, n (%) | |||
| 40–49 | 621 (4.9) | 4 (0.5) | <0.001 |
| 50–59 | 3987 (31.8) | 57 (7.2) | |
| 60–69 | 4616 (36.9) | 226 (28.8) | |
| 70–79 | 2488 (19.9) | 262 (33.4) | |
| ≥80 | 796 (6.4) | 236 (30.1) | |
| Sex, n (%) | |||
| Women | 7390 (59.1) | 388 (49.4) | <0.001 |
| Men | 5118 (40.9) | 397 (50.6) | |
| Physically active, n (%) | 5027 (40.2) | 177 (22.6) | <0.001 |
| Tobacco use, n (%) | |||
| Never | 7911 (63.2) | 474 (60.3) | 0.008 |
| Former user | 3076 (24.6) | 230 (29.3) | |
| Current user | 1521 (12.1) | 81 (10.3) | |
| High-risk alcohol drinking, n (%) | 1193 (9.5) | 39 (4.9) | <0.001 |
| Social vulnerability index, mean (SD) | 0.41 (0.12) | 0.48 (0.12) | <0.001 |
| Frailty index, mean (SD) | 0.22 (0.1) | 0.31 (0.13) | <0.001 |
| Social vulnerability index score tertiles, n (%) | |||
| <0.36 | 4233 (33.8) | 126 (16) | <0.001 |
| 0.36–0.47 | 4241 (33.9) | 233 (29.7) | |
| >0.47 | 4034 (32.2) | 426 (54.2) | |
| Frailty index categories, n (%) | |||
| <0.1 | 1079 (8.6) | 21 (2.7) | <0.001 |
| 0.11–0.2 | 4921 (39.3) | 168 (21.4) | |
| 0.21–0.3 | 3525 (28.2) | 196 (25) | |
| >0.3 | 2983 (23.9) | 400 (50.9) | |
| No Disability (n = 8950) | Disability (n = 1367) | p-Value * | |
|---|---|---|---|
| Age Categories, n (%) | |||
| 40–49 | 517 (5.8) | 34 (2.5) | <0.001 |
| 50–59 | 3310 (36.9) | 290 (21.2) | |
| 60–69 | 3306 (37) | 521 (38.1) | |
| 70–79 | 1485 (16.6) | 371 (27.1) | |
| ≥80 | 332 (3.7) | 151 (11.1) | |
| Sex, n (%) | |||
| Women | 5069 (56.6) | 828 (60.6) | 0.006 |
| Men | 3881 (43.4) | 539 (39.4) | |
| Physically active, n (%) | 3924 (43.8) | 455 (33.2) | <0.001 |
| Tobacco use, n (%) | |||
| Never | 5603 (62.6) | 902 (66) | 0.013 |
| Former user | 2178 (24.3) | 322 (23.6) | |
| Current user | 1169 (13.1) | 143 (10.4) | |
| High-risk alcohol drinking, n (%) | 962 (10.7) | 116 (8.5) | 0.011 |
| Social vulnerability index, mean (SD) | 0.2 (0.12) | 0.44 (0.12) | <0.001 |
| Frailty index, mean (SD) | 0.21 (0.09) | 0.28 (0.11) | <0.001 |
| Social vulnerability index score tertiles, n (%) | |||
| <0.36 | 3442 (38.4) | 340 (24.8) | <0.001 |
| 0.36–0.47 | 3033 (33.8) | 474 (34.6) | |
| >0.47 | 2475 (27.6) | 553 (40.4) | |
| Frailty index levels, n (%) | |||
| <0.1 | 681 (7.6) | 23 (1.7) | <0.001 |
| 0.11–0.2 | 3924 (43.9) | 299 (21.9) | |
| 0.21–0.3 | 2688 (30) | 462 (33.8) | |
| >0.31 | 1657 (18.5) | 583 (42.6) | |
| Mortality | Incident Disability | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Social vulnerability index tertiles | ||||||||||||
| <0.36 | Reference | |||||||||||
| 0.36–0.47 | 1.8 | 1.4–2.2 | <0.001 | 1.2 | 0.9–1.5 | 0.054 | 1.5 | 1.3–1.8 | <0.001 | 1.2 | 1.1–1.4 | 0.024 |
| >0.47 | 3.4 | 2.8–4.1 | <0.001 | 1.4 | 1.1–1.8 | <0.001 | 2.2 | 2.6 | <0.001 | 1.3 | 1.1–1.5 | 0.026 |
| Age categories | ||||||||||||
| 40–49 | Reference | |||||||||||
| 50–59 | 1.9 | 0.7–5.3 | 0.21 | 1.3 | 0.9–1.9 | 0.17 | ||||||
| 60–69 | 5.4 | 2–14.5 | 0.001 | 2.2 | 1.5–3.1 | <0.001 | ||||||
| 70–79 | 9.2 | 3.4–24.9 | <0.001 | 2.9 | 2–4.3 | <0.001 | ||||||
| ≥80 | 19.1 | 7.1–51.7 | <0.001 | 4.8 | 3.2–7.3 | <0.001 | ||||||
| Sex | ||||||||||||
| Women | Reference | |||||||||||
| Men | 1.7 | 1.5–2 | <0.001 | 1 | 0.8–1.1 | 0.7 | ||||||
| Physically active | 0.6 | 0.5–0.7 | <0.001 | 0.8 | 0.7–0.9 | <0.001 | ||||||
| Tobacco use | ||||||||||||
| Never | Reference | |||||||||||
| Former user | 0.99 | 0.83–1.18 | 0.84 | 0.9 | 0.8–1.1 | 0.42 | ||||||
| Current user | 1.04 | 0.81–1.3 | 0.81 | 0.9 | 0.7–1.1 | 0.29 | ||||||
| High-risk alcohol drinking | 0.7 | 0.5–1 | 0.11 | 1.1 | 0.9–1.4 | 0.27 | ||||||
| Frailty index levels | ||||||||||||
| <0.1 | Reference | |||||||||||
| 0.11–0.2 | 1.2 | 0.7–1.9 | 0.05 | 1.9 | 1.2–2.9 | <0.001 | ||||||
| 0.21–0.3 | 1.5 | 0.9–2.3 | 0.092 | 3.7 | 2.4–5.7 | <0.001 | ||||||
| >0.31 | 2.7 | 1.7–4.2 | <0.001 | 7.2 | 4.7–11.1 | <0.001 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Garrido, N.; Aguilar-Navarro, S.G.; Ávila-Funes, J.A.; Theou, O.; Andrew, M.; Pérez-Zepeda, M.U. The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults. Geriatrics 2021, 6, 24. https://doi.org/10.3390/geriatrics6010024
Sánchez-Garrido N, Aguilar-Navarro SG, Ávila-Funes JA, Theou O, Andrew M, Pérez-Zepeda MU. The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults. Geriatrics. 2021; 6(1):24. https://doi.org/10.3390/geriatrics6010024
Chicago/Turabian StyleSánchez-Garrido, Natalia, Sara G. Aguilar-Navarro, José Alberto Ávila-Funes, Olga Theou, Melissa Andrew, and Mario Ulises Pérez-Zepeda. 2021. "The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults" Geriatrics 6, no. 1: 24. https://doi.org/10.3390/geriatrics6010024
APA StyleSánchez-Garrido, N., Aguilar-Navarro, S. G., Ávila-Funes, J. A., Theou, O., Andrew, M., & Pérez-Zepeda, M. U. (2021). The Social Vulnerability Index, Mortality and Disability in Mexican Middle-Aged and Older Adults. Geriatrics, 6(1), 24. https://doi.org/10.3390/geriatrics6010024