
Total Knee Arthroplasty in Octogenarians: Should We Still Be so Restrictive?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patients characteristics
3.2. Comorbidities
3.3. Clinical Outcomes
3.4. Complications
3.4.1. Medical Complications
3.4.2. Surgical Complications
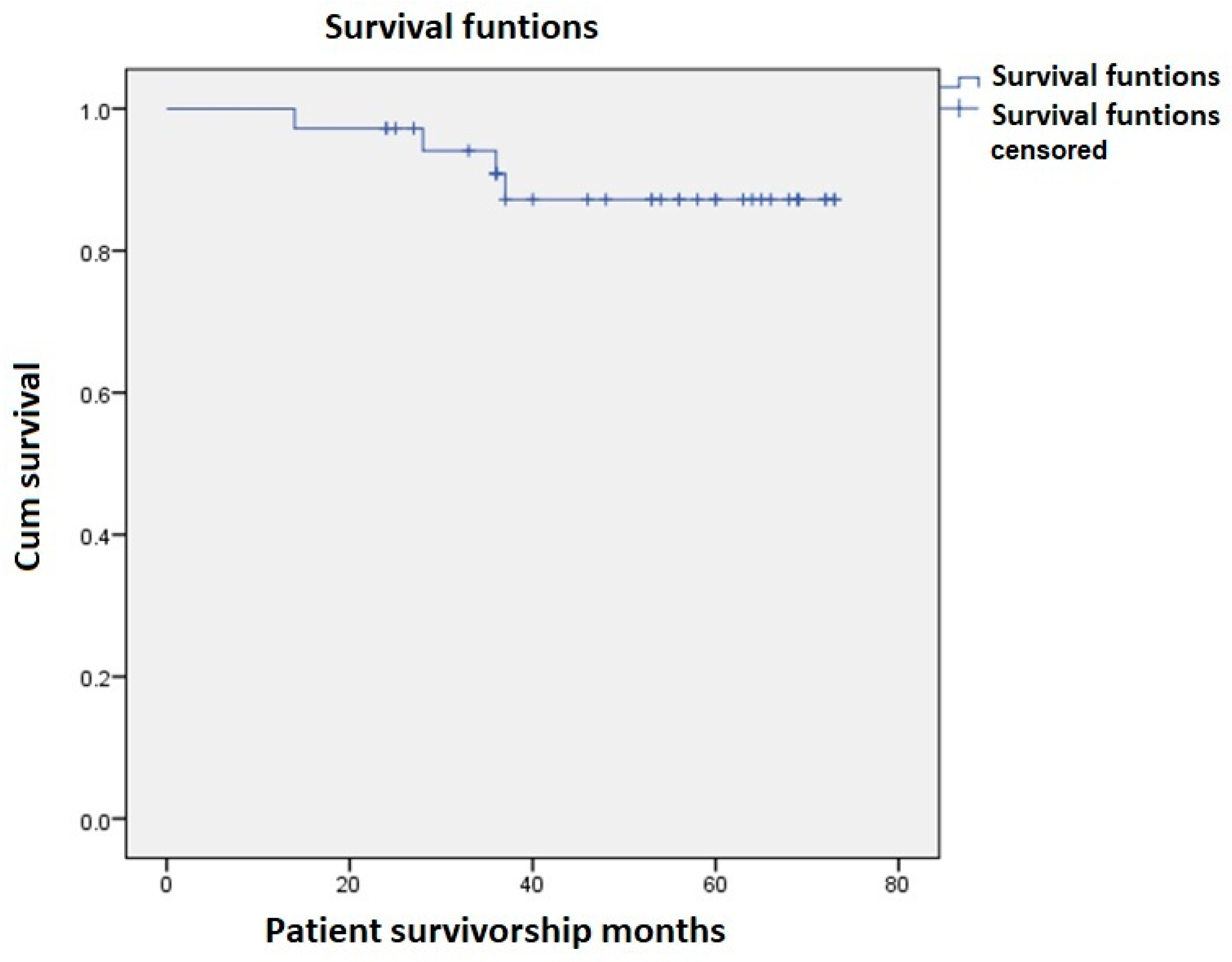
3.5. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Instituto Nacional de Estadística. Madrid, Indicadores de Mortalidad. Resultados Nacionales, Esperanza de Vida al Nacimiento. 2021. Available online: https://ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177004&menu=ultiDatos&idp=1254735573002 (accessed on 29 March 2021).
- Jones, C.A.; Beaupre, L.A.; Johnston, D.W.; Suarez-Almazor, M.E. Total joint arthroplasties: Current concepts of patient outcomes after surgery. Clin. Geriatr. Med. 2005, 21, 527–541. [Google Scholar] [CrossRef] [PubMed]
- Callahan, C.M.; Drake, B.G.; Heck, D.A.; Dittus, R.S. Patients outcomes following tricompartimental total knee replacement. A meta-analysis. JAMA 1994, 271, 1349–1357. [Google Scholar] [CrossRef]
- Sloan, M.; Premkumar, A.; Seht, N.P. Projected Volume of Primary Total Joint Arthroplasty in the U.S., 2014 to 2030. J. Bone Jt. Surg. Am. 2018, 100, 1455–1460. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, D.H.; Lee, Y.S. Is there an optimal age for total knee arthroplasty? A systematic review. Knee Surg. Relat. Res. 2020, 32, 60. [Google Scholar] [CrossRef]
- Hosick, W.B.; Lotke, P.A.; Baldwin, A. Total knee arthroplasty in patients 80 years of age and older. Clin. Orthop. Relat. Res. 1994, 299, 77–80. [Google Scholar] [CrossRef]
- Clement, N.D.; MacDonald, D.; Howie, C.R.; Biant, L.C. The outcome of primary total hip and knee arthroplasty in patients aged 80 years or more. J. Bone Jt. Surg. Br. 2011, 93, 1265–1270. [Google Scholar] [CrossRef] [Green Version]
- Lizaur-Utilla, A.; Martinez-Mendez, D.; Miralles-Muñoz, F.A.; Marco-Gómez, L.; Lopez-Prats, F.A. Risk-Benefit on Quality of Life After Total Knee Arthroplasty in Octogenarians. J. Arthroplast. 2017, 32, 2417–2420. [Google Scholar] [CrossRef]
- Murphy, B.P.D.; Dowsey, M.M.; Choong, P.F.M. The impact of advanced age on the outcomes of primary total hip and knee arthroplasty for osteoarthritis: A systematic review. Bone Jt. Surg. 2018, 32, 1463–1470. [Google Scholar] [CrossRef]
- Klasan, A.; Putnis, S.E.; Yeo, W.W.; Fritsch, B.A.; Coolican, M.R.; Parker, D.A. Advanced age is not a barrier to total knee arthroplasty: A detailed analysis of outcomes and complications in an elderly cohort compared with average age total knee arthroplasty patients. J. Arthroplast. 2019, 34, 1938–1945. [Google Scholar] [CrossRef] [PubMed]
- Belmar, C.J.; Barth, P.; Lonner, J.H.; Lotke, P.A. Total knee arthroplasty in patients 90 years of age and older. J. Arthroplast. 1999, 14, 911–914. [Google Scholar] [CrossRef]
- Joshi, A.B.; Gill, G. Total knee arthroplasty in nonagenarians. J. Arthroplast. 2002, 17, 681–684. [Google Scholar] [CrossRef]
- Berend, M.E.; Thong, A.E.; Faris, G.W.; Newbern, G.; Pierson, J.L.; Ritter, M.A. Total joint arthroplasty in the extremely elderly: Hip and knee arthroplasty after entering the 89th year of life. J. Arthroplast. 2003, 18, 817–821. [Google Scholar] [CrossRef]
- Starks, I.; Wainwright, T.W.; Lewis, J.; Lloyd, J.; Middleton, R.G. Older patients have the most to gain from orthopaedic enhanced recovery programes. Age Ageing 2014, 43, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Pitter, F.T.; Jørgensen, C.C.; Lindberg-Larsen, M.; Kehlet, H. Lundbeck Foundation Center for Fast-track Hip and Knee Replacement Collaborative Group. Postoperative Morbidity and Discharge Destinations After Fast-Track Hip and Knee Arthroplasty in Patients Older Than 85 Years. Anesth. Analg. 2016, 122, 1807–1815. [Google Scholar] [CrossRef]
- Kuperman, E.F.; Schweizer, M.; Joy, P.; Gu, X.; Fang, M.M. The effects of advanced age on primary total knee arthroplasty: A meta-analysis and systematic review. BMC Geriatr. 2016, 16, 41. [Google Scholar] [CrossRef] [Green Version]
- Andreozzi, V.; Conteduca, F.; Iorio, R.; Di Stasio, E.; Mazza, D.; Drogo, P.; Annibaldi, A.; Ferretti, A. Comorbidities rather than age affect medium-term outcome in octogenarian patients after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3142–3148. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar] [CrossRef]
- Jauregui, J.J.; Boylan, M.R.; Kapadia, B.H.; Naziri, Q.; Maheshwari, A.V.; Mont, M.A. Total Joint Arthroplasty in Nonagenarians: What Are the Risks? J. Arthroplast. 2015, 30, 2102–2105.e1. [Google Scholar] [CrossRef] [PubMed]
- Petruccelli, D.; Rahman, W.A.; de Beer, J.; Winemaker, M. Clinical outcomes of primary total joint arthroplasty among nonagenarian patients. J. Arthroplast. 2012, 27, 1599–1603. [Google Scholar] [CrossRef]
- Quintero, J.I.; Cardenas, L.L.; Navas, M.; Bautista, M.P.; Bonilla, G.A.; Llinas, A.M.; Adolfo, M. Primary joint arthroplasty surgery: Is the risk of major bleeding higher in elderly patients? A retrospective cohort study. J. Arthroplast. 2016, 31, 2264–2268. [Google Scholar] [CrossRef]
- Poeran, J.; Rasul, R.; Suzuki, S.; Danninger, T.; Mazumdar, M.; Opperer, M.; Boettner, F.; Memtsoudis, S.G. Tranexamic acid use and postoperative outcomes in patients undergoing total hip or knee arthroplasty in the United States: Retrospective analysis of effectiveness and safety. BMJ 2014, 349, g4829. [Google Scholar] [CrossRef] [Green Version]
- Han, S.B.; Kim, H.J.; Kim, T.K.; In, Y.; Oh, K.J.; Koh, I.J.; Lee, D.-H. Computer navigation is effective in reducing blood loss but has no effect on transfusion requirement following primary total knee arthroplasty: A meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3474–3481. [Google Scholar] [CrossRef]
- Bovonratwet, P.; Fu, M.C.; Tyagi, V.; Gu, A.; Sculco, P.K.; Grauer, J.N. Is discharge within a day total knee arthroplasty safe in the octogenarian population? J. Arthroplast. 2019, 34, 235–241. [Google Scholar] [CrossRef]
- Ode, Q.; Gaillard, R.; Batailler, C.; Herry, Y.; Neyret, P.; Servien, E.; Lustig, S. Fewer complications rate after UKA than TKA in patients over 85 years of age: A case-control study. Orthop. Traumatol. Surg. Res. 2018, 104, 955–959. [Google Scholar] [CrossRef]
- Gustke, K.A.; Gelbke, M.K. All-Polyethylene tibial component use for elderly, low-demand total knee arthroplasty patients. J. Arthroplast. 2017, 32, 2421–2426. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Count (n = 36)/Mean | Percent/SD |
|---|---|---|
| Age at surgery | 81.6 years (80–86) | ±1.5 years |
| Follow up (months) | 50 months (14–73) | |
| Sex (Male/Female) | 21/15 | 58.3%/41.7% |
| Side (Left/Female | 19/17 | 52.8%/47.2% |
| ASA Scale | II 24 (66.3%) III 12 (33.7%) | II 66.3% III 33.7% |
| Charlson | ||
| 0 | 16 (44.4%) | 44.40% |
| 1 | 14 (38.9%) | 38.90% |
| 2 | 2 (5.6%) | 5.60% |
| 3 | 4 (11.1%) | 11.10% |
| Comorbidities | ||
| Hypertension | 17 | 47.20% |
| Dyslipidemia | 14 (41.6%) | 41.60% |
| Benign Prostatic Hypertrophy | 6 (16.6%) | 16.60% |
| Cardiac disease | 5 (13.9%) | 13.90% |
| Obstructive Pulmonary disease | 4 (11.1%) | 11.10% |
| Cerebrovascular ischemic disease | 4 (11.1%) | 11.10% |
| Mental health disorders | 3 (8.3%) | 8.30% |
| Malignant tumor | 2 (5.3%) | 5.30% |
| Deep venous thrombosis | 2 (5.3%) | 5.30% |
| Chronic renal disease | 2 (5.3%) | 5.30% |
| Polymyalgia Rheumatica | 1 | 2.70% |
| Preoperative * | Postoperative * | p Value | |
|---|---|---|---|
| KSS | 34.6 ± 9 | 89.9 ± 6.9 | p < 0.001 |
| KSS function | 33.9 ± 10.2 | 86 ± 11.97 | p < 0.001 |
| Flexion | 101.5° ± 10.87° | 106.2°± 9.1° | p < 0.001 |
| Extension | −4.2° ± 4.2° | 0.97° ± 2° | p < 0.001 |
| Radiologic alignment | 6.75° ± 6.45° | 1.36° ± 1.4° | p < 0.001 |
| Count (n = 36)/Mean | |
|---|---|
| Length of stay in days | 5.8± 1.84 |
| Medical complications | 7 |
| Confusion | 2 |
| Atrial fibrillation | 1 |
| Urinary tract infection | 1 |
| Urinary incontinence | 1 |
| Hematuria | 1 |
| Congestive heart failure | 1 |
| Anemia requiring transfusions | 2 |
| Surgical complications | 2 |
| Persistent wound drainage | 1 |
| Fracture and mobilization | 1 |
| of the femoral component |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trigueros-Larrea, J.M.; Gonzalez-Bedia, M.A.; Lomo-Garrote, J.M.; Martin-de la Cal, O.; Martin-Ferrero, M.A. Total Knee Arthroplasty in Octogenarians: Should We Still Be so Restrictive? Geriatrics 2021, 6, 67. https://doi.org/10.3390/geriatrics6030067
Trigueros-Larrea JM, Gonzalez-Bedia MA, Lomo-Garrote JM, Martin-de la Cal O, Martin-Ferrero MA. Total Knee Arthroplasty in Octogenarians: Should We Still Be so Restrictive? Geriatrics. 2021; 6(3):67. https://doi.org/10.3390/geriatrics6030067
Chicago/Turabian StyleTrigueros-Larrea, Jose Maria, Maria Antonia Gonzalez-Bedia, Jose Maria Lomo-Garrote, Oscar Martin-de la Cal, and Miguel Angel Martin-Ferrero. 2021. "Total Knee Arthroplasty in Octogenarians: Should We Still Be so Restrictive?" Geriatrics 6, no. 3: 67. https://doi.org/10.3390/geriatrics6030067
APA StyleTrigueros-Larrea, J. M., Gonzalez-Bedia, M. A., Lomo-Garrote, J. M., Martin-de la Cal, O., & Martin-Ferrero, M. A. (2021). Total Knee Arthroplasty in Octogenarians: Should We Still Be so Restrictive? Geriatrics, 6(3), 67. https://doi.org/10.3390/geriatrics6030067