
The Mini-Cog, Clock Drawing Test, and Three-Item Recall Test: Rapid Cognitive Screening Tools with Comparable Performance in Detecting Mild NCD in Older Patients


Abstracts
1. Background
2. Materials and Methods
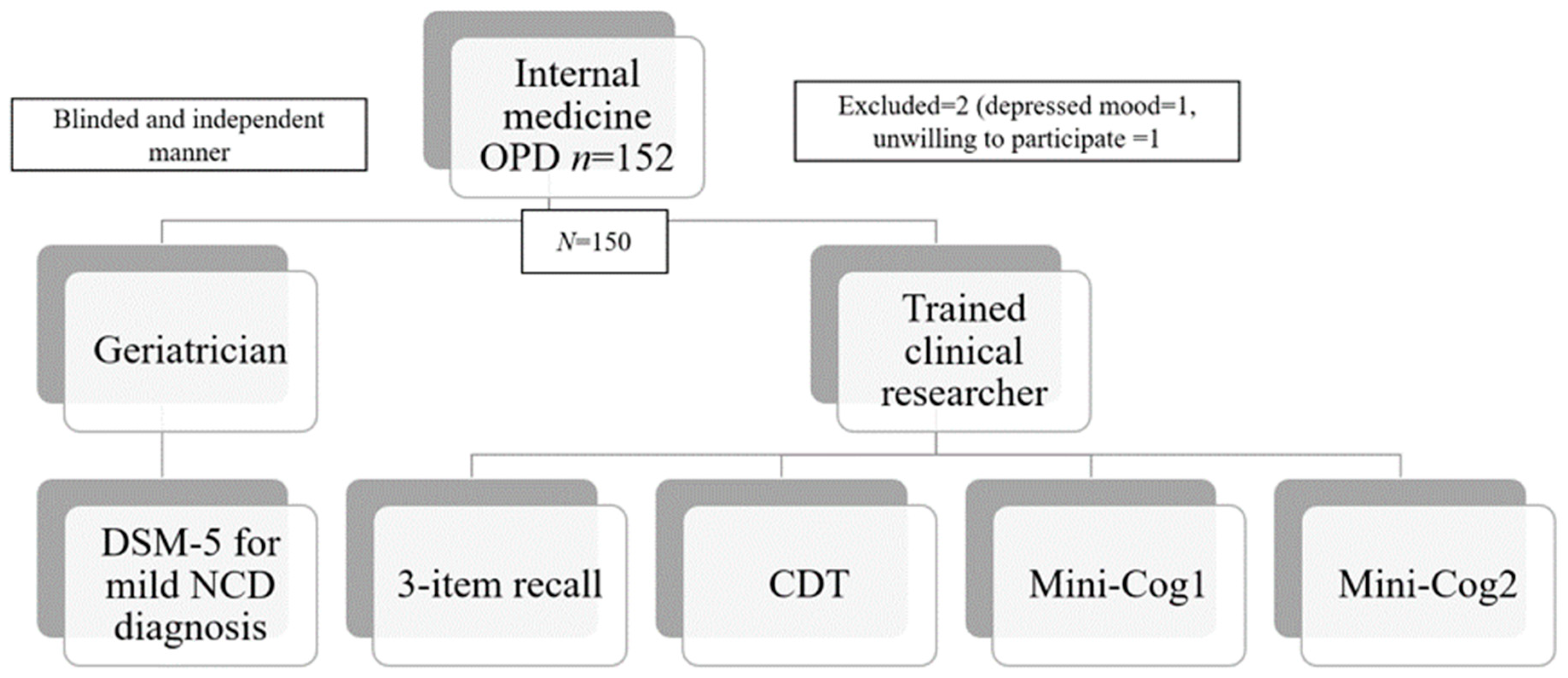
2.1. Participants and Setting
2.2. Operational Definition
Mild Neurocognitive Disorder (Mild NCD)
2.3. Instrument
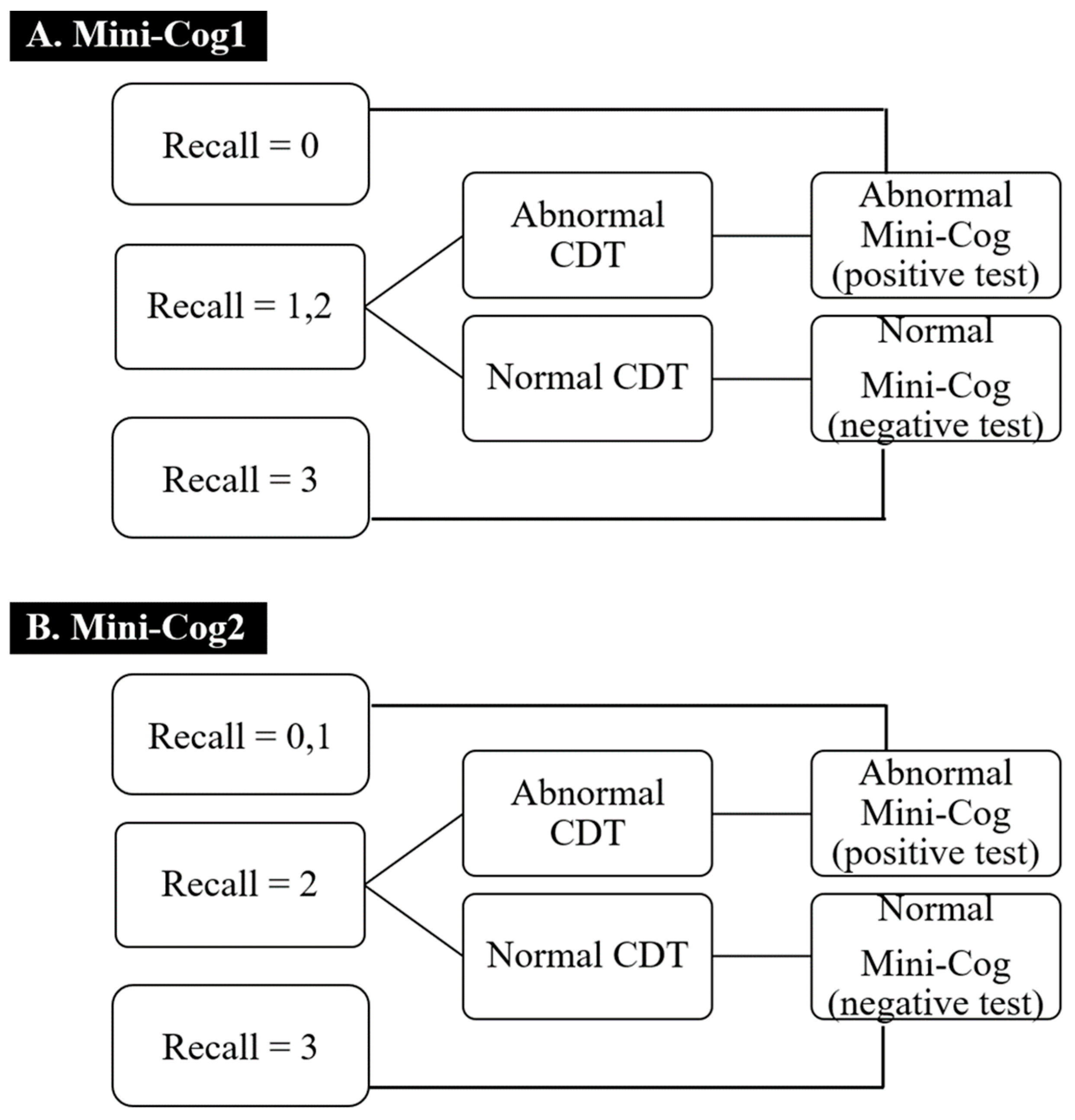
Mini-Cog1 and Mini-Cog2
2.4. Three-Item Recall Test
2.5. Clock Drawing Test
2.6. Procedure
2.7. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Mild NCD Screening Accuracy of the Three-Item Recall Test, CDT, Mini-Cog1, and Mini-Cog2
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boustani, M.; Schubert, C.; Sennour, Y. The challenge of supporting care for dementia in primary care. Clin. Interv. Aging 2007, 2, 631. [Google Scholar] [CrossRef] [Green Version]
- Roberts, R.O.; Knopman, D.S.; Mielke, M.M.; Cha, R.H.; Pankratz, V.S.; Christianson, T.J.; Geda, Y.E.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology 2014, 82, 317–325. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Morris, J.C.; Berg-Weger, M.; Borson, S.; Carpenter, B.D.; Del Campo, N.; Dubois, B.; Fargo, K.; Fitten, L.J.; Flaherty, J.H.; et al. Brain health: The importance of recognizing cognitive impairment: An IAGG consensus conference. J. Am. Med. Dir. Assoc. 2015, 16, 731–739. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, M.; Vibha, D. Reversible dementias. Indian J. Psychiatry 2009, 51, S52. [Google Scholar]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Singh, B.; Parsaik, A.K.; Mielke, M.M.; Erwin, P.J.; Knopman, D.S.; Petersen, R.C.; Roberts, R.O. Association of mediterranean diet with mild cognitive impairment and Alzheimer’s disease: A systematic review and meta-analysis. J. Alzheimers Dis. 2014, 39, 271–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangwongchai, S.; Phanasathit, M.; Charernboon, T.; Akkayagorn, L.; Hemrungrojn, S.; Phanthumchinda, K.; Nasreddine, Z. The validity of thai version of the montreal cognitive assessment (MoCA-T). Dement. Neuropsychol. 2009, 3, 172. [Google Scholar]
- Custodio, N.; Montesinos, R.; Lira, D.; Herrera-Perez, E.; Chavez, K.; Reynoso-Guzman, W.; Pintado-Caipa, M.; Cuenca, J.; Gamboa, C.; Metcalf, T.; et al. Validation of the RUDAS for the Identification of Dementia in Illiterate and Low-Educated Older Adults in Lima, Peru. Front. Neurol. 2020, 11, 374. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, L.; Yang, Y.; Gao, J. Cognitive assessment tools for mild cognitive impairment screening. J. Neurol. 2021, 268, 1615–1622. [Google Scholar] [CrossRef] [PubMed]
- Arevalo-Rodriguez, I.; Smailagic, N.; i Figuls, M.R.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Cosp, X.B.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Jia, X.F.; Jia, J. The Informant Questionnaire on Cognitive Decline in the Elderly individuals in screening mild cognitive impairment with or without functional impairment. J. Geriatr. Psychiatry Neurol. 2012, 25, 227–232. [Google Scholar] [CrossRef]
- Rossetti, H.; Lacritz, L.; Cullum, M.; Weiner, M. Normative data for the Montreal Cognitive Assessment (MoCA) in a population-based sample. Neurology 2011, 77, 1272–1275. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Older Population and Health System: A Profile of Thailand. Available online: https://www.who.int/ageing/projects/intra/phase_one/alc_intra1_cp_thailand.pdf (accessed on 1 January 2015).
- Borson, S.; Scanlan, J.; Brush, M.; Vitaliano, P.; Dokmak, A. The mini-cog: A cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int. J. Geriatr. Psychiatry 2000, 15, 1021–1027. [Google Scholar] [CrossRef]
- Trongsakul, S.; Lambert, R.; Clark, A.; Wongpakaran, N.; Cross, J. Development of the Thai version of Mini-Cog, a brief cognitive screening test. Geriatr. Gerontol. Int. 2015, 15, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Borson, S.; Scanlan, J.M.; Chen, P.; Ganguli, M. The Mini-Cog as a screen for dementia: Validation in a population-based sample. J. Am. Geriatr. Soc. 2003, 51, 1451–1454. [Google Scholar] [CrossRef]
- Ricci, M.; Pigliautile, M.; D’Ambrosio, V.; Ercolani, S.; Bianchini, C.; Ruggiero, C.; Vanacore, N.; Mecocci, P. The clock drawing test as a screening tool in mild cognitive impairment and very mild dementia: A new brief method of scoring and normative data in the elderly. Neurol. Sci. 2016, 37, 867–873. [Google Scholar] [CrossRef]
- Dudas, R.B.; Clague, F.; Thompson, S.A.; Graham, K.S.; Hodges, J.R. Episodic and semantic memory in mild cognitive impairment. Neuropsychologia 2005, 43, 1266–1276. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Hirai, H.W.; Wong, A.; Mok, V.C.; Lam, L.C.; Kwok, T.C.; Wong, S.Y. Recall Tests Are Effective to Detect Mild Cognitive Impairment: A Systematic Review and Meta-analysis of 108 Diagnostic Studies. J. Am. Med. Dir. Assoc. 2017, 18, 807.e17–807.e29. [Google Scholar] [CrossRef]
- Manjavong, M.; Limpawattana, P.; Sawanyawisuth, K. Performance of the Rowland Universal Dementia Assessment Scale in Screening Mild Cognitive Impairment at an Outpatient Setting. Dement. Geriatr. Cogn. Disord. Extra 2021, 11, 181–188. [Google Scholar] [CrossRef]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jitapunkul, S. Disability: The elderly problems. Chula. Med. J. 1994, 38, 68–75. [Google Scholar]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying neurocognitive disorders: The DSM-5 approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef]
- Kusalaruk, P.; Nakawiro, D. The validity study of the Mini-Cog test in Thai dementia patients. Rama. Med. J. 2012, 35, 264–271. [Google Scholar]
- Shengping, Y.; Gilbert, B. The receiver operating characteristic (ROC) curve. Southwest Respir. Crit. Care Chron. 2017, 5, 34–36. [Google Scholar]
- Seitz, D.P.; Chan, C.C.; Newton, H.T.; Gill, S.S.; Herrmann, N.; Smailagic, N.; Nikolaou, V.; Fage, B.A. Mini-Cog for the diagnosis of Alzheimer’s disease dementia and other dementias within a primary care setting. Cochrane Database Syst. Rev. 2018, 2, CD011415. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia--meta-analysis of 41 robust inception cohort studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef]
- Ferman, T.J.; Smith, G.E.; Kantarci, K.; Boeve, B.F.; Pankratz, V.S.; Dickson, D.W.; Graff-Radford, N.R.; Wszolek, Z.; Van Gerpen, J.; Uitti, R.; et al. Nonamnestic mild cognitive impairment progresses to dementia with Lewy bodies. Neurology 2013, 81, 2032–2038. [Google Scholar] [CrossRef] [Green Version]
- Kidd, P.M. Alzheimer’s disease, amnestic mild cognitive impairment, and age-associated memory impairment: Current understanding and progress toward integrative prevention. Altern Med. Rev. 2008, 13, 85–115. [Google Scholar] [PubMed]
- Borson, S.; Scanlan, J.M.; Watanabe, J.; Tu, S.P.; Lessig, M. Simplifying detection of cognitive impairment: Comparison of the Mini-Cog and Mini-Mental State Examination in a multiethnic sample. J. Am. Geriatr. Soc. 2005, 53, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Carnero-Pardo, C.; Cruz-Orduna, I.; Espejo-Martinez, B.; Martos-Aparicio, C.; Lopez-Alcalde, S.; Olazaran, J. Utility of the mini-cog for detection of cognitive impairment in primary care: Data from two spanish studies. Int J. Alzheimers Dis. 2013, 2013, 285462. [Google Scholar] [CrossRef] [Green Version]
- Milian, M.; Leiherr, A.M.; Straten, G.; Muller, S.; Leyhe, T.; Eschweiler, G.W. The Mini-Cog versus the Mini-Mental State Examination and the Clock Drawing Test in daily clinical practice: Screening value in a German Memory Clinic. Int. Psychogeriatr. 2012, 24, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro Filho, S.T.; Lourenco, R.A. The performance of the Mini-Cog in a sample of low educational level elderly. Dement. Neuropsychol. 2009, 3, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Dai, J.; Zhao, S.; Liu, W.; Li, H. Comparison of the value of Mini-Cog and MMSE screening in the rapid identification of Chinese outpatients with mild cognitive impairment. Medicine 2018, 97, e10966. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Non-Mild NCD N = 108 (72%) | Mild NCD N = 42 (28%) | ||
|---|---|---|---|---|
| Age, median (IQR1,3) | 67 | (62.5, 73.5) | 72 | (66, 75) |
| Women, n (%) | 53 | (49.1) | 25 | (59.5%) |
| Years of education, n (%) | ||||
| 0 | 0 | (0) | 3 | (7.1) |
| ≤6 years | 34 | (31.5) | 25 | (59.5) |
| 6 to 12 years | 28 | (25.9) | 7 | (16.7) |
| >12 years | 46 | (42.6) | 7 | (16.7) |
| Marital status, n (%) | ||||
| Single | 3 | (2.8) | 2 | (4.8) |
| Married | 82 | (75.9) | 26 | (61.9) |
| Divorced | 8 | (7.4) | 1 | (2.4) |
| Widow | 15 | (13.9) | 13 | (30.9) |
| Comorbid disease(s) *, n (%) | ||||
| DM | 43 | (39.8) | 23 | (54.8) |
| HT | 81 | (75) | 33 | (78.6) |
| DLD | 72 | (66.6) | 15 | (35.7) |
| CKD | 27 | (25) | 4 | (9.5) |
| AF | 7 | (6.5) | 4 | (9.5) |
| IHD | 2 | (1.9) | 2 | (4.8) |
| CVA | 5 | (4.6) | 4 | (9.5) |
| OSA | 7 | (6.5) | 2 | (4.8) |
| Number of items recall, median (IQR1,3) | 3 | (2, 3) | 2 | (1, 2) |
| Abnormal CDT, n (%) | 36 | (33.3) | 28 | (66.7) |
| Positive Mini-Cog1, n (%) | 20 | (18.5) | 27 | (65.3) |
| Positive Mini-Cog2, n (%) | 29 | (26.9) | 29 | (69.1) |
| Tests | Sensitivity | Specificity | AUC of ROC Curve | 95%CI | p-Value |
|---|---|---|---|---|---|
| 3-item recall | 85.7% | 56.5% | 0.71 | 0.63–0.78 | p = 0.36 |
| CDT | 66.7% | 66.7% | 0.67 | 0.58–0.75 | |
| Mini-Cog1 | 57.4% | 85.4% | 0.73 | 0.65–0.81 | |
| Mini-Cog2 | 69% | 73.1% | 0.71 | 0.63–0.79 |
| Tests | AUC (95%CI) | |
|---|---|---|
| ≤6 Years N = 62 * | >6 Years N = 88 ** | |
| 3-item recall | 0.71 (0.60–0.82) | 0.71 (0.60,0.82) |
| CDT | 0.57 (0.46–0.68) | 0.59 (0.45,0.73) |
| Mini-Cog1 | 0.68 (0.57–0.80) | 0.67 (0.53–0.81) |
| Mini-Cog2 | 0.69 (0.57–0.80) | 0.65 (0.51–0.79) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limpawattana, P.; Manjavong, M. The Mini-Cog, Clock Drawing Test, and Three-Item Recall Test: Rapid Cognitive Screening Tools with Comparable Performance in Detecting Mild NCD in Older Patients. Geriatrics 2021, 6, 91. https://doi.org/10.3390/geriatrics6030091
Limpawattana P, Manjavong M. The Mini-Cog, Clock Drawing Test, and Three-Item Recall Test: Rapid Cognitive Screening Tools with Comparable Performance in Detecting Mild NCD in Older Patients. Geriatrics. 2021; 6(3):91. https://doi.org/10.3390/geriatrics6030091
Chicago/Turabian StyleLimpawattana, Panita, and Manchumad Manjavong. 2021. "The Mini-Cog, Clock Drawing Test, and Three-Item Recall Test: Rapid Cognitive Screening Tools with Comparable Performance in Detecting Mild NCD in Older Patients" Geriatrics 6, no. 3: 91. https://doi.org/10.3390/geriatrics6030091
APA StyleLimpawattana, P., & Manjavong, M. (2021). The Mini-Cog, Clock Drawing Test, and Three-Item Recall Test: Rapid Cognitive Screening Tools with Comparable Performance in Detecting Mild NCD in Older Patients. Geriatrics, 6(3), 91. https://doi.org/10.3390/geriatrics6030091