
Influence of Sociodemographic, Health-Related, and Behavioral Factors on Food Guidelines Compliance in Older Adults: A Hierarchical Approach from the Chilean National Health Survey 2016–17 Data

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Variables
2.2.1. Dependent Variable
- Daily water intake: <6 glasses; ≥6 glasses.
- Weekly frequency of legumes (beans, lentils, peas, chickpeas) consumption: <2 times; ≥2 times.
- Daily frequency of non-fat dairy intake: <3 servings; ≥3 servings.
- Weekly frequency of fish and seafood: <2 times; ≥2 times.
- Daily portions of fruits and vegetables: <5 portions; ≥5 portions.
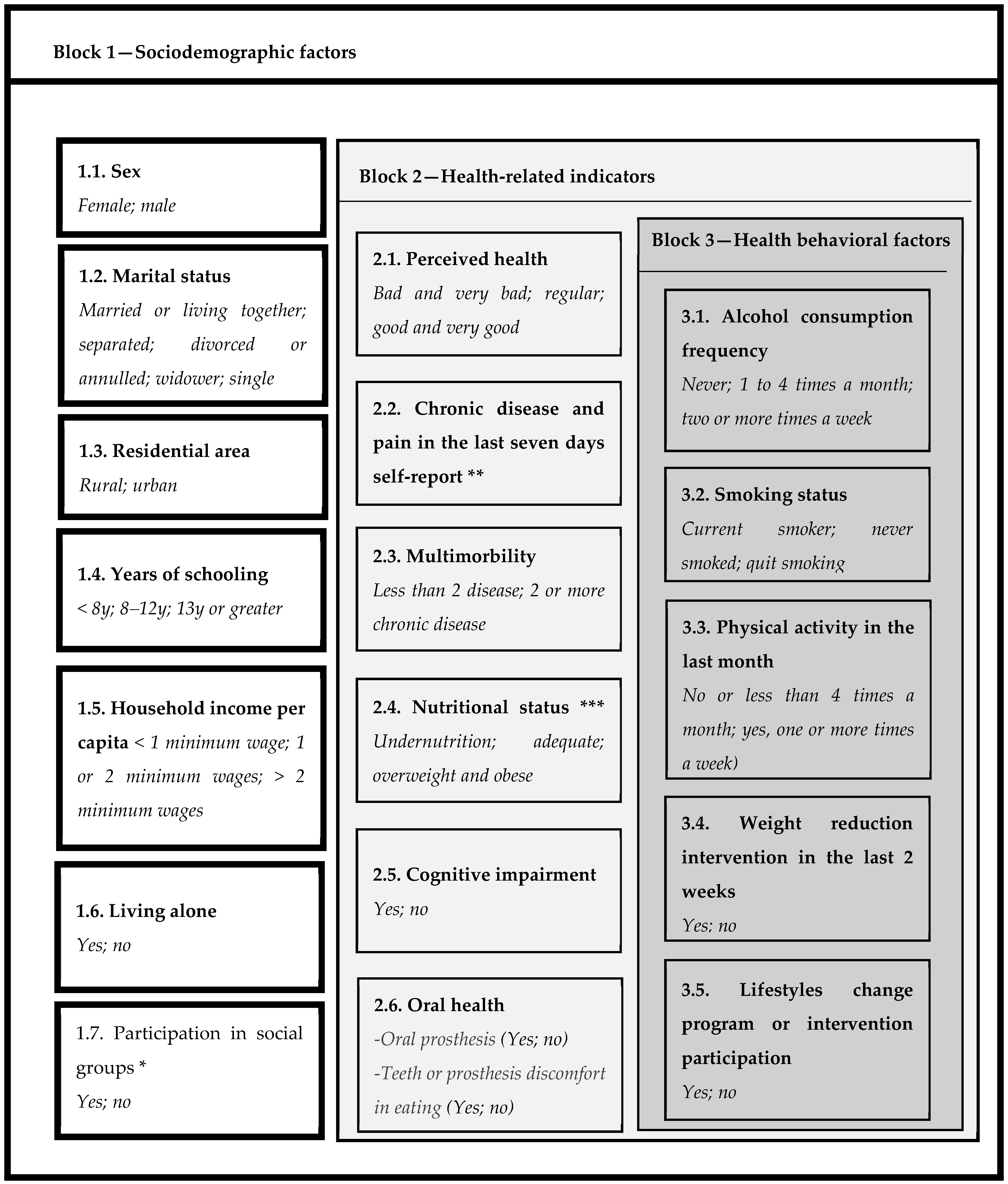
2.2.2. Independent Variables
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sadana, R.; Blas, E.; Budhwani, S.; Koller, T.; Paraje, G. Healthy Ageing: Raising Awareness of Inequalities, Determinants, and What Could Be Done to Improve Health Equity. Gerontologist 2016, 56, S178–S193. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Life Expectancy and Healthy Life Expectancy—Data by WHO Region; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Pac, A.; Tobiasz-Adamczyk, B.; Błędowski, P.; Skalska, A.; Szybalska, A.; Zdrojewski, T.; Więcek, A.; Chudek, J.; Michel, J.P.; Grodzicki, T. Influence of Sociodemographic, Behavioral and Other Health-Related Factors on Healthy Ageing Based on Three Operative Definitions. J. Nutr. Health Aging 2019, 23, 862–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thumala, D.; Kennedy, B.K.; Calvo, E.; Gonzalez-Billault, C.; Zitko, P.; Lillo, P.; Villagra, R.; Ibáñez, A.; Assar, R.; Andrade, M.; et al. Aging and Health Policies in Chile: New Agendas for Research. Health Syst. Reform 2017, 3, 253–260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Consortium on Metrics and Evidence for Healthy Ageing-Peer Review Meeting of Contributors to the Global Baseline Report for Decade of Healthy Ageing Meeting Report (Unedited); WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Beard, J.; Officer, A.; IA, D.C.; Sadana, R.; Pot, A.; Michel, J.; Al, E. The World Report on Ageing and Health: A Policy Framework for Healthy Ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Gordon, S.J.; Grimmer, K.A.; Baker, N.; Bell, E.; Coveney, J.; Jordaan, J.H.; Lind, C.; Marin, T.; Murray, J.; Norton, L.H.; et al. Feasibility of Population Screening Tests to Establish a Healthy Ageing Trajectory. SAGE Open Med. 2019, 7, 205031211882244. [Google Scholar] [CrossRef]
- Milte, C.M.; McNaughton, S.A. Dietary Patterns and Successful Ageing: A Systematic Review. Eur. J. Nutr. 2016, 55, 423–450. [Google Scholar] [CrossRef] [Green Version]
- Govindaraju, T.; Sahle, B.W.; McCaffrey, T.A.; McNeil, J.J.; Owen, A.J. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients 2018, 10, 971. [Google Scholar] [CrossRef] [Green Version]
- Yannakoulia, M.; Mamalaki, E.; Anastasiou, C.A.; Mourtzi, N.; Lambrinoudaki, I.; Scarmeas, N. Eating Habits and Behaviors of Older People: Where Are We Now and Where Should We Go? Maturitas 2018, 114, 14–21. [Google Scholar] [CrossRef]
- Whitelock, E.; Ensaff, H. On Your Own: Older Adults’ Food Choice and Dietary Habits. Nutrients 2018, 10, 413. [Google Scholar] [CrossRef] [Green Version]
- Gille, D.; Bütikofer, U.; Chollet, M.; Schmid, A.; Altintzoglou, T.; Honkanen, P.; Stoffers, H.; Walther, B.; Piccinali, P. Nutrition Behavior of the Middle-Aged and Elderly: Compliance with Dietary Recommendations of the Food Pyramid. Clin. Nutr. 2016, 35, 638–644. [Google Scholar] [CrossRef]
- Robinson, S.M.; Manuscript, A. Improving Nutrition to Support Healthy Ageing: What Are the Opportunities for Intervention? Proc. Nutr. Soc. 2018, 77, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Host, A.; McMahon, A.T.; Walton, K.; Charlton, K. Factors Influencing Food Choice for Independently Living Older People—A Systematic Literature Review. J. Nutr. Gerontol. Geriatr. 2016, 35, 67–94. [Google Scholar] [CrossRef] [PubMed]
- Shahrin, F.I.M.; Omar, N.; Daud, Z.A.M.; Zakaria, N.F. Factors Associated with Food Choices among Elderly: A Scoping Review. Malays. J. Nutr. 2019, 25, 185–198. [Google Scholar] [CrossRef]
- Koehler, J.; Leonhaeuser, I.U. Changes in Food Preferences during Aging. Ann. Nutr. Metab. 2008, 52, 15–19. [Google Scholar] [CrossRef]
- Universidad de Chile. Informe Final Encuesta Nacional de Consumo Alimentario (ENCA). 2014, pp. 222–224. Available online: https://www.minsal.cl/sites/default/files/ENCA-INFORME_FINAL.pdf (accessed on 15 March 2021).
- Ministerio de Salud del Gobierno de Chile. Encuesta Nacional de Salud 2016–2017. Segunda Entrega de Resultados. 2018. Available online: https://www.minsal.cl/wp-content/uploads/2018/01/2-Resultados-ENS_MINSAL_31_01_2018.pdf (accessed on 15 March 2021).
- Departamento de Epidemiología Ministerio de Salud de Chile. Encuesta Nacional de Salud (ENS) 2016-2017—Diseño Muestral. Available online: http://epi.minsal.cl/wp-content/uploads/2018/05/DISEÑO-MUESTRAL-ENS-2016-2017.pdf (accessed on 16 March 2021).
- Ministerio de Salud de Chile. Norma General Técnica 148. Guías Alimentarias Para la Población Chilena. 2013. Available online: https://www.integra.cl/wp-content/uploads/2017/01/GUIAS-ALIMENTARIAS.pdf (accessed on 16 March 2020).
- Organización Panamericana de la Salud; División de promoción y protección de la salud. Salud Bienestar y Envejecimiento (SABE) en América Latina y El Caribe; EUA: Washington, DC, USA, 2001. [Google Scholar]
- Quiroga, L.P.; Albala, B.C.; Klaasen, P.G. Validación de Un Test de Tamizaje Para El Diagnóstico de Demencia Asociada a Edad, En Chile. Rev. Med. Chil. 2004, 132, 467–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanaugh, J.E.; Neath, A.A. The Akaike Information Criterion: Background, Derivation, Properties, Application, Interpretation, and Refinements. Wiley Interdiscip. Rev. Comput. Stat. 2019, 11, 1–11. [Google Scholar] [CrossRef]
- Candía, S.; Candia, P.; Mena, R.P.; Durán Agüero, S. Calidad de La Alimentación de Adultos Mayores de Santiago de Chile. Rev. Esp. Geriatr. Gerontol. 2019, 54, 147–150. [Google Scholar] [CrossRef]
- Agüero, S.D.; Candia, P.; Mena, R.P. Validación de Contenido de La Encuesta de Calidad de Alimentación Del Adulto Mayor (ECAAM). Nutr. Hosp. 2017, 34, 1311–1318. [Google Scholar]
- Dourado, D.A.Q.S.; Marucci, M.D.F.N.; Roediger, M.D.A.; Duarte, Y.A.D.O. Dietary Patterns of Elderly Persons from the City of São Paulo: Evidence from the SABE (Health, Wellbeing and Aging) Survey. Rev. Bras. Geriatr. Gerontol. 2018, 21, 731–742. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Redondo, S.; Beltrán de Miguel, B.; Gómez-Pavón, J.; Cuadrado Vives, C. Food Consumption and Risk of Malnutrition in Community-Dwelling Very Old Spanish Adults (≥80 Years). Nutr. Hosp. 2016, 33, 572–579. [Google Scholar]
- Dijkstra, S.C.; Neter, J.E.; Van Stralen, M.M.; Knol, D.L.; Brouwer, I.A.; Huisman, M.; Visser, M. The Role of Perceived Barriers in Explaining Socio-Economic Status Differences in Adherence to the Fruit, Vegetable and Fish Guidelines in Older Adults: A Mediation Study. Public Health Nutr. 2015, 18, 797–808. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Salud (MINSAL). Encuesta Nacional de Salud de Chile 2009–2010; Ministerio de Salud: Santiago, Chile, 2009–2010; Volume Tomo 1. [Google Scholar]
- Rovira, R.F. La Leche y Los Productos Lácteos: Fuentes Dietéticas de Calcio. Nutr. Hosp. 2015, 31, 1–9. [Google Scholar] [CrossRef]
- Wang, H.; Fox, C.S.; Troy, L.M.; McKeown, N.M.; Jacques, P.F. Longitudinal Association of Dairy Consumption with the Changes in Blood Pressure and the Risk of Incident Hypertension: The Framingham Heart Study. Br. J. Nutr. 2015, 114, 1887–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehghan, M.; Mente, A.; Rangarajan, S.; Sheridan, P.; Mohan, V.; Iqbal, R.; Gupta, R.; Lear, S.; Wentzel-Viljoen, E.; Avezum, A.; et al. Association of Dairy Intake with Cardiovascular Disease and Mortality in 21 Countries from Five Continents (PURE): A Prospective Cohort Study. Lancet 2018, 392, 2288–2297. [Google Scholar] [CrossRef]
- Cuesta-Triana, F.; Verdejo-Bravo, C.; Fernández-Pérez, C.; Martín-Sánchez, F.J. Effect of Milk and Other Dairy Products on the Risk of Frailty, Sarcopenia, and Cognitive Performance Decline in the Elderly: A Systematic Review. Adv. Nutr. 2019, 10, S105–S119. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.P.; Overvad, K.; Tetens, I.; Tjonneland, A.; Parner, E.T.; Jakobsen, M.U.; Dahm, C.C. Adherence to the Danish Food-Based Dietary Guidelines and Risk of Myocardial Infarction: A Cohort Study. Public Health Nutr. 2018, 21, 1286–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdugo, G.; Arias, V.; Perez-Leighton, C. Análisis Del Precio de Una Dieta Saludable y No Saludable En La Región Metropolitana de Chile. Arch. Latinoam. de Nutr. 2016, 66, 272–278. [Google Scholar]
- de Freitas, T.I.; Previdelli, Á.N.; Ferreira, M.P.D.N.; Marques, K.M.; Goulart, R.M.M.; de Aquino, R.D.C. Factors Associated with Diet Quality of Older Adults/Fatores Associados à Qualidade Da Dieta de Idosos. Rev. Nutr. VO-30 2017, 30, 297. [Google Scholar] [CrossRef] [Green Version]
- Pinto, V.; Landaeta-Díaz, L.; Castillo, O.; Villarroel, L.; Rigotti, A.; Echeverría, G. Assessment of Diet Quality in Chilean Urban Population through the Alternate Healthy Eating Index 2010: A Cross-Sectional Study. Nutrients 2019, 11, 891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, M.; Raats, M.M.; Grunert, K.G.; Lumbers, M. Factors Influencing Eating a Varied Diet in Old Age. Public Health Nutr. 2009, 12, 2421–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solar, O.; Irwin, A. A Conceptual Framework for Action on the Social Determinants of Health; WHO Document Production Services: Geneva, Switzerland, 2010. [Google Scholar]
- Dunneram, Y.; Jeewon, R. Determinants of Eating Habits among Older Adults. Prog. Nutr. 2015, 17, 274–283. [Google Scholar]
- Thorpe, M.G.; Milte, C.M.; Crawford, D.; McNaughton, S.A. Education and Lifestyle Predict Change in Dietary Patterns and Diet Quality of Adults 55 Years and Over. Nutr. J. 2019, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesnaver, E.; Keller, H.H. Social Influences and Eating Behavior in Later Life: A Review. J. Nutr. Gerontol. Geriatr. 2011, 30, 2–23. [Google Scholar] [CrossRef]
- Payette, H.; Shatenstein, B. Determinants of Healthy Eating in Community-Dwelling Elderly People. Can. J. Public Health Rev. Can. Sante’e Publique 2005, 96, S27–S31. [Google Scholar] [CrossRef]
- Zhou, X.; Perez-Cueto, F.J.A.; Dos Santos, Q.; Monteleone, E.; Giboreau, A.; Appleton, K.M.; Bjørner, T.; Bredie, W.L.P.; Hartwell, H. A Systematic Review of Behavioural Interventions Promoting Healthy Eating among Older People. Nutrients 2018, 10, 128. [Google Scholar] [CrossRef] [Green Version]
- Poscia, A.; Milovanovic, S.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Landi, F.; Moscato, U.; Magnavita, N.; Collamati, A.; Ricciardi, W. Effectiveness of Nutritional Interventions Addressed to Elderly Persons: Umbrella Systematic Review with Meta-Analysis. Eur. J. Public Health 2018, 28, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Agardh, E.E.; Östenson, C.G.; Ahlbom, A.; Andersson, T. The Magnitude of Bias in a Cross-Sectional Study on Lifestyle Factors in Relation to Type 2 Diabetes. Scand. J. Public Health 2006, 34, 665–668. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Overall | 60–79 y | ≥80 y | p-Value ‡ |
|---|---|---|---|---|
| Population represented | 3,066,214 | 2,627,745 | 438,469 | |
| Sociodemographic factors | ||||
| Female sex | 51.8 | 51.4 | 54.2 | 0.652 |
| Marital status | <0.001 | |||
| Married or living together | 59.9 | 63.6 | 37.3 | |
| Separated, divorced, or annulled | 10.8 | 11.5 | 6.4 | |
| Widower | 19.4 | 14.8 | 47.6 | |
| Single | 9.9 | 10.2 | 8.7 | |
| Residential area | 0.132 | |||
| Urban | 86.0 | 86.7 | 82.0 | |
| Rural | 14.0 | 13.3 | 18.0 | |
| Years of schooling | <0.001 | |||
| <8 y | 46.1 | 41.9 | 71.9 | |
| 8–12 y | 37.5 | 40.1 | 21.7 | |
| ≥13 y | 16.4 | 18.0 | 6.4 | |
| Household income per capita | 0.774 | |||
| <1 minimum wage | 80.8 | 80.2 | 84.4 | |
| 1 to 2 minimum wages | 14.1 | 14.4 | 12.1 | |
| >2 minimum wages | 5.1 | 5.4 | 3.5 | |
| Living alone | 19.2 | 18.2 | 24.7 | 0.106 |
| Participation in social groups | 35.9 | 35.8 | 36.3 | 0.929 |
| Someone’s caretaker | 21.6 | 24.0 | 6.5 | <0.001 |
| Health-related indicators | ||||
| Perceived health | <0.001 | |||
| Bad and very bad | 14.3 | 11.9 | 29.3 | |
| Regular | 42.4 | 43.1 | 38.2 | |
| Good and very good | 43.3 | 45.1 | 32.5 | |
| Chronic disease self-report | ||||
| Cardiovascular diseases | 73.0 | 71.6 | 81.4 | 0.082 |
| Eye disorders and diseases | 23.7 | 20.4 | 44.0 | <0.001 |
| Osteoarticular diseases | 36.3 | 35.0 | 43.6 | 0.134 |
| Multimorbidity (≥2 NCD) * | 63.2 | 60.0 | 83.1 | <0.001 |
| Nutritional status | ||||
| Underweight | 9.2 | 8.0 | 16.8 | 0.005 |
| Adequate weight | 32.3 | 31.0 | 40.2 | |
| Overweight | 20.5 | 21.1 | 16.5 | |
| Obesity | 38.0 | 39.9 | 26.5 | |
| Cognitive impairment | 4.2 | 2.3 | 15.6 | <0.001 |
| Oral prosthesis | 60.2 | 58.3 | 71.3 | 0.031 |
| Teeth or prosthesis discomfort in eating | 25.2 | 24.3 | 30.7 | 0.233 |
| Muscles/bones/joint pain in the last 7 days | 50.0 | 49.8 | 51.2 | 0.818 |
| Variables | Overall | 60–79 y | ≥80 y | p-Value ‡ |
|---|---|---|---|---|
| Health behavioral factors | ||||
| Alcohol consumption frequency | ||||
| Never | 41.5 | 39.3 | 55.2 | 0.018 |
| 1 to 4 times a month | 48.0 | 49.7 | 37.5 | |
| Two or more times a week | 10.5 | 11.0 | 7.2 | |
| Smoking status | ||||
| Never smoked | 46.1 | 43.6 | 60.8 | 0.035 |
| Quit smoking | 37.9 | 38.9 | 32.0 | |
| Current smoker | 16.0 | 17.5 | 7.2 | |
| Physical activity in the last month | ||||
| No | 89.3 | 88.3 | 95.3 | 0.016 |
| Yes | 10.7 | 11.7 | 4.7 | |
| Weight reduction intervention in the last 2 weeks | 26.6 | 29.6 | 8.9 | <0.001 |
| Lifestyles change program or intervention participation | 64.3 | 63.4 | 69.7 | 0.362 |
| Food Guidelines | ||||
| 5 servings of fruits and/or vegetables a day | 19.3 | 20.4 | 12.9 | 0.045 |
| Fish and seafood at least twice a week | 9.1 | 9.5 | 6.6 | 0.343 |
| Legumes at least twice a week | 30.6 | 30.2 | 33.3 | 0.585 |
| At least 6 glasses of water a day | 20.2 | 20.9 | 16.0 | 0.225 |
| 3 servings of dairy a day | 5.3 | 5.0 | 7.4 | 0.287 |
| Food Guidelines Compliance | ||||
| Noncompliance | 41.1 | 40.9 | 42.7 | 0.627 |
| Partial compliance | 55.0 | 55.0 | 54.8 | |
| Satisfactory compliance | 3.9 | 4.1 | 2.5 | |
| Variables | Noncompliance | Crude Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|---|
| % | PR | 95%CI | p-Value 1 | PR | 95%CI | p-Value 1 | |
| Block 1—Sociodemographic factors | |||||||
| Female sex | 43.9 | 1.16 | 0.94–1.44 | 0.162 | 1.16 | 0.94–1.43 | 0.180 |
| Marital status | |||||||
| Married or living together | 37.2 | 1.00 | - | 1.00 | - | ||
| Separated, divorced, or annulled | 46.4 | 1.25 | 0.91–1.71 | 0.168 | 1.18 | 0.86–1.60 | 0.301 |
| Widower | 51.6 | 1.39 | 1.08–1.78 | 0.010 | 1.34 | 1.04–1.71 | 0.021 |
| Single | 41.6 | 1.12 | 0.78–1.60 | 0.547 | 1.06 | 0.73–1.53 | 0.764 |
| Rural residence | 39.8 | 0.97 | 0.78–1.21 | 0.783 | |||
| Years of schooling | |||||||
| <8 y | 42.7 | 1.00 | - | 1.00 | - | ||
| 8–12 y | 34.8 | 0.82 | 0.65–1.02 | 0.073 | 0.85 | 0.68–1.06 | 0.147 |
| ≥13 y | 48.4 | 1.13 | 0.82–1.56 | 0.442 | 1.21 | 0.89–1.65 | 0.232 |
| Household income per capita | |||||||
| <1 minimum wage | 41.8 | 1.00 | - | ||||
| 1 to 2 minimum wages | 30.8 | 0.74 | 0.45–1.21 | 0.223 | |||
| >2 minimum wages | 38.0 | 0.91 | 0.48–1.71 | 0.769 | |||
| Living alone | 39.5 | 0.96 | 0.77–1.19 | 0.707 | |||
| Participation of social groups | 43.2 | 1.11 | 0.89–1.37 | 0.353 | |||
| Block 2—Health-related indicators | |||||||
| Perceived health | |||||||
| Bad, very bad, and regular | 45.0 | 1.00 | - | 1.00 | - | ||
| Good and very good | 35.8 | 0.80 | 0.64–1.00 | 0.046 | 0.84 | 0.68–1.04 | 0.117 |
| Chronic disease self-report | |||||||
| With cardiovascular diseases | 41.3 | 1.04 | 0.80–1.35 | 0.793 | |||
| With osteoarticular diseases | 46.7 | 1.24 | 1.03–1.49 | 0.025 | 1.17 | 0.97–1.41 | 0.103 |
| With eye disorders and diseases | 43.4 | 1.08 | 0.85–1.37 | 0.537 | |||
| Nutritional status | |||||||
| Adequate weight | 40.6 | 1.00 | - | 1.00 | - | ||
| Underweight | 33.9 | 0.84 | 0.56–1.25 | 0.386 | 0.82 | 0.56–1.22 | 0.335 |
| Overweight | 51.6 | 1.27 | 0.92–1.75 | 0.147 | 1.26 | 0.92–1.73 | 0.158 |
| Obesity | 36.8 | 0.91 | 0.71–1.17 | 0.448 | 0.87 | 0.258 | 0.258 |
| With Cognitive impairment | 50.6 | 1.25 | 0.73–2.13 | 0.423 | |||
| Uses oral prosthesis | 38.8 | 0.88 | 0.73–1.08 | 0.222 | |||
| Teeth or prosthesis with discomfort in eating | 37.3 | 0.89 | 0.70–1.13 | 0.321 | |||
| Block 3—Health behavioral factors | |||||||
| Alcohol consumption frequency | |||||||
| Never | 40.6 | 1.00 | - | ||||
| 1 to 4 times a month | 42.2 | 1.04 | 0.85–1.28 | 0.707 | |||
| Two or more times a week | 35.7 | 0.88 | 0.53–1.47 | 0.626 | |||
| Smoking status | |||||||
| Never smoked | 42.7 | 1.00 | - | ||||
| Quit smoking | 39.0 | 0.91 | 0.72–1.16 | 0.464 | |||
| Current smoker | 40.7 | 0.95 | 0.72–1.26 | 0.732 | |||
| Physical activity in the last month | 33.7 | 0.81 | 0.52–1.26 | 0.341 | |||
| Weight reduction intervention in the last 2 weeks | 37.4 | 1.09 | 0.87–1.36 | 0.477 | |||
| Lifestyles change program or intervention participation | 42.1 | 0.88 | 0.68–1.16 | 0.365 | |||
| Variables | Noncompliance | Crude Model | Adjusted Model | ||||
|---|---|---|---|---|---|---|---|
| % | PR | 95%CI | p-Value 1 | PR | 95%CI | p-Value 1 | |
| Block 1—Sociodemographic factors | |||||||
| Female sex | 41.7 | 0.95 | 0.59–1.55 | 0.840 | |||
| Marital status | |||||||
| Married or living together | 39.6 | 1.00 | - | ||||
| Separated, divorced, or annulled | 23.1 | 0.59 | 0.19–1.81 | 0.350 | |||
| Widower | 47.5 | 1.20 | 0.71–2.02 | 0.491 | |||
| Single | 44.1 | 1.12 | 0.47–2.66 | 0.805 | |||
| Rural residence | 51.7 | 1.27 | 0.84–1.93 | 0.262 | |||
| Years of schooling | |||||||
| <8 y | 46.2 | 1.00 | - | 1.00 | - | ||
| 8–12 y | 24.2 | 0.52 | 0.29–0.94 | 0.030 | 0.56 | 0.29–1.07 | 0.077 |
| ≥13 y | 69.0 | 1.49 | 0.74–3.00 | 0.258 | 0.94 | 0.60–1.47 | 0.783 |
| Household income per capita | |||||||
| <1 minimum wage | 39.6 | 1.00 | - | 1.00 | - | ||
| 1 to 2 minimum wages | 76.2 | 1.92 | 1.27–2.91 | 0.002 | 1.33 | 0.90–1.98 | 0.157 |
| >2 minimum wages | 2.4 | 0.06 | 0.01–0.49 | 0.005 | 0.10 | 0.02–0.61 | 0.013 |
| Living alone | 64.1 | 1.80 | 1.24–2.61 | 0.002 | 1.72 | 1.20–2.47 | 0.003 |
| Participation of social groups | 32.2 | 0.66 | 0.38–1.13 | 0.126 | 0.81 | 0.46–1.42 | 0.455 |
| Block 2—Health-related indicators | |||||||
| Perceived health | |||||||
| Bad, very bad, and regular | 42.1 | 1.00 | - | ||||
| Good and very good | 43.9 | 1.04 | 0.65–1.67 | 0.857 | |||
| Chronic disease self-report | |||||||
| With cardiovascular diseases | 36.8 | 0.54 | 0.37–0.80 | 0.002 | 0.63 | 0.43–0.93 | 0.019 |
| With osteoarticular diseases | 35.4 | 0.73 | 0.46–1.16 | 0.183 | 0.74 | 0.49–1.13 | 0.164 |
| With eye disorders and diseases | 53.3 | 1.55 | 1.00–2.40 | 0.049 | 1.53 | 1.00–2.35 | 0.048 |
| Nutritional status | |||||||
| Adequate weight | 31.3 | 1.00 | - | 1.00 | - | ||
| Underweight | 59.5 | 1.90 | 1.08–3.36 | 0.027 | 1.73 | 0.93–3.23 | 0.084 |
| Overweight | 62.2 | 1.99 | 1.10–3.58 | 0.022 | 1.29 | 0.76–2.17 | 0.339 |
| Obesity | 37.3 | 1.19 | 0.65–2.19 | 0.570 | 1.59 | 0.92–2.76 | 0.099 |
| With Cognitive impairment | 44.2 | 1.04 | 0.61–1.77 | 0.879 | |||
| Uses oral prosthesis | 41.1 | 0.88 | 0.52–1.49 | 0.642 | |||
| Teeth or prosthesis with discomfort in eating | 33.6 | 0.72 | 0.40–1.29 | 0.264 | |||
| Block 3—Health behavioral factors | |||||||
| Alcohol consumption frequency | |||||||
| Never | 44.8 | 1.00 | - | ||||
| 1 to 4 times a month | 41.4 | 0.92 | 0.54–1.56 | 0.763 | |||
| Two or more times a week | 33.1 | 0.74 | 0.34–1.61 | 0.441 | |||
| Smoking status | |||||||
| Never smoked | 31.7 | 1.00 | - | 1.00 | - | ||
| Quit smoking | 55.9 | 1.76 | 1.14–2.72 | 0.011 | 1.51 | 0.99–2.30 | 0.055 |
| Current smoker | 76.6 | 2.42 | 1.44–4.06 | 0.001 | 1.19 | 0.75–1.88 | 0.456 |
| Physical activity in the last month | 27.9 | 0.64 | 0.19–2.20 | 0.479 | |||
| Weight reduction intervention in the last 2 weeks | 36.4 | 0.68 | 0.40–1.17 | 0.167 | |||
| Lifestyles change program or intervention participation | 37.5 | 0.84 | 0.41–1.71 | 0.628 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Albuquerque-Araújo, L.; Quintiliano-Scarpelli, D.; Masferrer Riquelme, D.; Ferreira Santos, J.L. Influence of Sociodemographic, Health-Related, and Behavioral Factors on Food Guidelines Compliance in Older Adults: A Hierarchical Approach from the Chilean National Health Survey 2016–17 Data. Geriatrics 2022, 7, 47. https://doi.org/10.3390/geriatrics7020047
de Albuquerque-Araújo L, Quintiliano-Scarpelli D, Masferrer Riquelme D, Ferreira Santos JL. Influence of Sociodemographic, Health-Related, and Behavioral Factors on Food Guidelines Compliance in Older Adults: A Hierarchical Approach from the Chilean National Health Survey 2016–17 Data. Geriatrics. 2022; 7(2):47. https://doi.org/10.3390/geriatrics7020047
Chicago/Turabian Stylede Albuquerque-Araújo, Leticia, Daiana Quintiliano-Scarpelli, Dominique Masferrer Riquelme, and Jair Licio Ferreira Santos. 2022. "Influence of Sociodemographic, Health-Related, and Behavioral Factors on Food Guidelines Compliance in Older Adults: A Hierarchical Approach from the Chilean National Health Survey 2016–17 Data" Geriatrics 7, no. 2: 47. https://doi.org/10.3390/geriatrics7020047
APA Stylede Albuquerque-Araújo, L., Quintiliano-Scarpelli, D., Masferrer Riquelme, D., & Ferreira Santos, J. L. (2022). Influence of Sociodemographic, Health-Related, and Behavioral Factors on Food Guidelines Compliance in Older Adults: A Hierarchical Approach from the Chilean National Health Survey 2016–17 Data. Geriatrics, 7(2), 47. https://doi.org/10.3390/geriatrics7020047