
Home-Dwelling Older Adults’ Day-to-Day Community Interactions: A Qualitative Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Women and men aged 65 years old or more living in the community;
- Older adults with or without a probable or diagnosed slight cognitive impairment or mild-to-moderate dementia (cognitive decline in one or more areas such as memory, attention, executive function, learning or language);
- Home-dwelling older adults, living alone or not (in a house, studio or flat), in rural village or small town environments (<10,000 people), medium-sized town environments (<100,000 people) or dense urban city environments (100,000–200,000 people);
- Older adults living with or without homecare support services or the help of an informal/family caregiver;
- Older adults giving their informed consent to participate in the study;
- Older adults able to understand and speak French.
- Older adults who were hospitalised or institutionalised in a nursing home or a long-term care facility;
- Older adults with severe cognitive impairment, severe dementia or a probable or diagnosed related disease;
- Older adults who do not leave their homes;
- Older adults not domiciled in Switzerland.
3. Results
3.1. Participants’ Characteristics
3.2. Interview Results
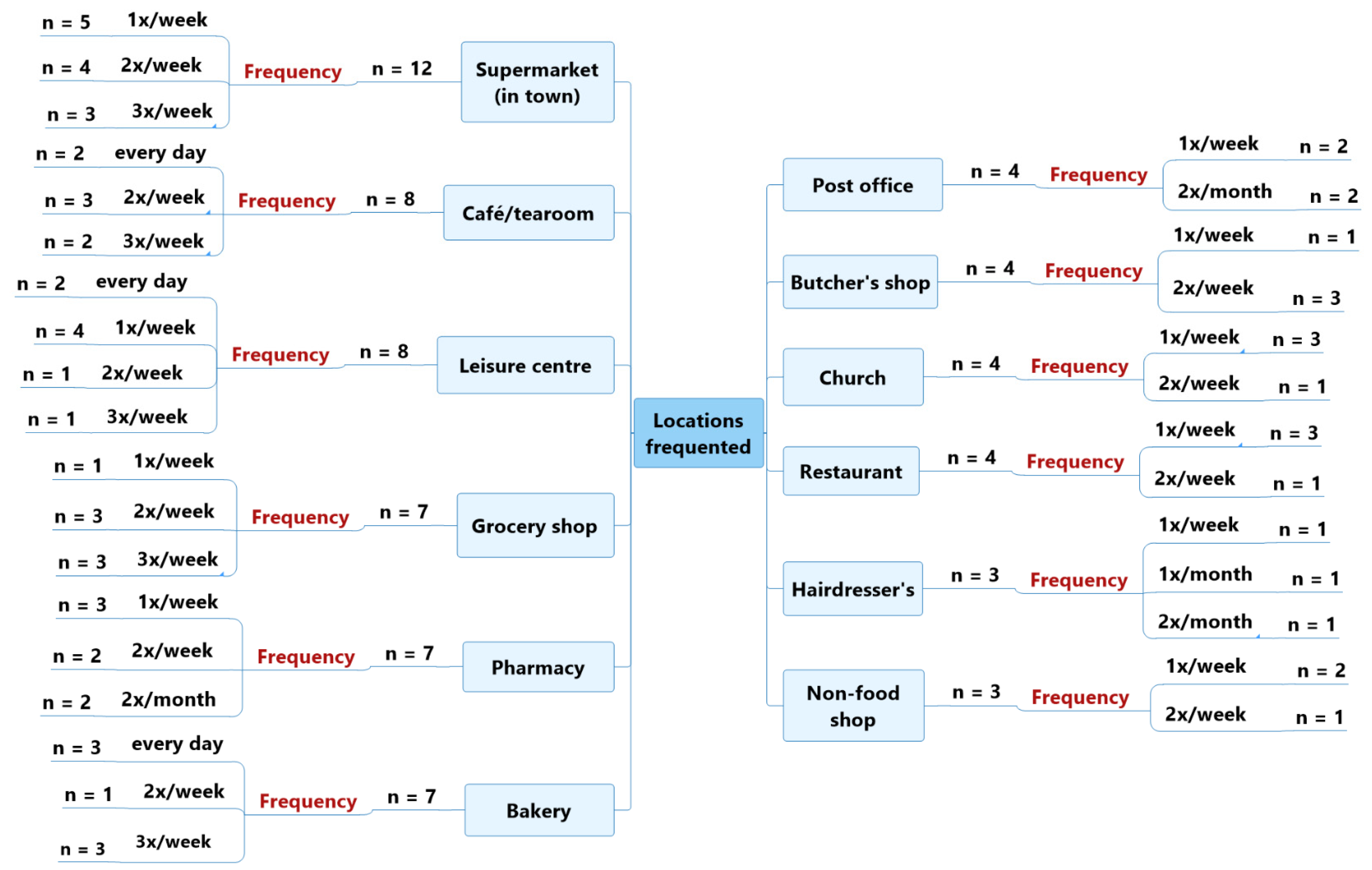
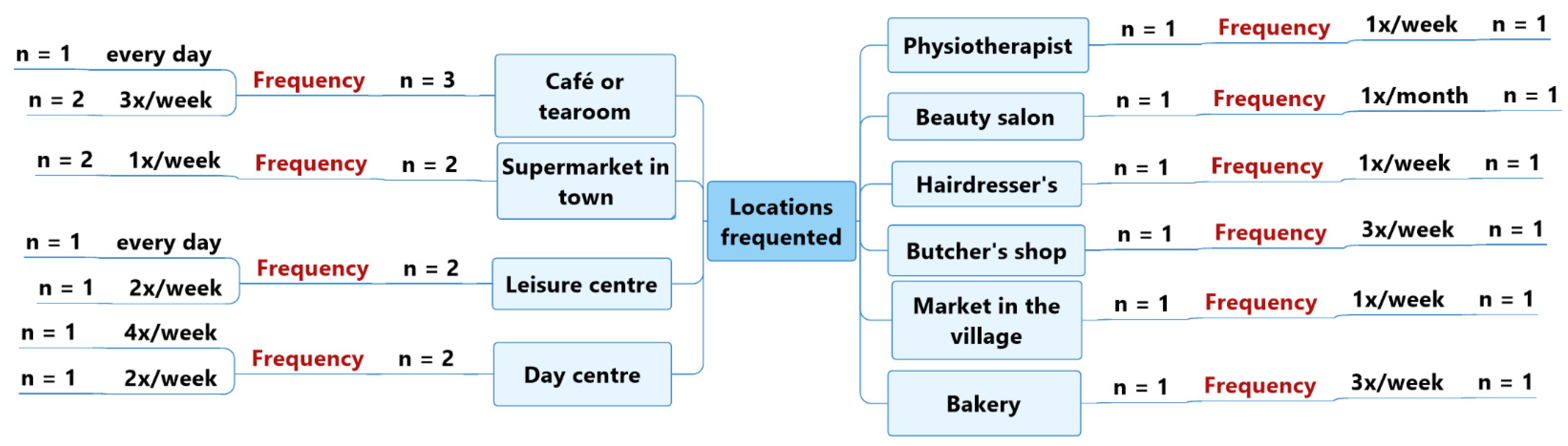
3.2.1. Theme 1: Daily Life
“I have a 45-year-old son and two grandchildren, aged 9 and 7. I am very happy to look after my grandchildren one afternoon a week. I have very good relationships with my family and friends, whom I see very often.”(Participant 5)
“I live with my daughter, who is 54 years old, since my wife died three years ago. My daughter stopped working to look after me.”(Participant 17—moderate Alzheimer’s disease)
“Every day, I usually meet my neighbours. I’m lucky; I’ve got good neighbours. They always take the time to chat with me a little, and they always offer me their help. As I walk my dog every day, I also regularly meet people I know on the street and talk to them for a few minutes.”(Participant 4)
“We have a lot of friends with whom we regularly like to go to the cinema and the theatre.”(Participant 13)
“My wife and I look after two of our grandchildren, both 3 years old, every Thursday. We are pleased to have some youngsters at home, even if it’s a lot of work because they’ve got a lot of energy.”(Participant 8)
“I often do some shopping in my village grocery shop or in a supermarket. Because they don’t have all the products that I use at the village shop, I often go to the bigger shops in town.”(Participant 10)
“None of my days is the same. I am a very busy person. My daughters often ask me to look after my grandchildren. My life is quite fast-paced.”(Participant 13)
“I like to do some shopping or have a coffee in the tea-room of the shopping centre not far from my home, five minutes’ walk away.”(Participant 11)
“Every afternoon, I do a group activity: aquafit twice a week, Tai-chi once a week, osteopathic-fitness once a week or walks.”(Participant 15)
“Every morning, on my way back from the village café, I stop to buy bread at my village bakery, and I talk to the sales ladies I know well.”(Participant 6)
“We usually go to the little cooperative shop in our neighbourhood.”(Participant 14)
“I regularly see the butcher I go to, about twice a week.”(Participant 11)
“I often go for lunch at my usual restaurant, about twice a week, and to the post office counter every two weeks to pick up orders.”(Participant 12)
“We go to church every Sunday and talk with the other participants and the priest, and we have become familiar with each other. We are like a community; we all know one another.”(Participant 14)
“I get up every day at 5:15 and have breakfast. At 6 o’clock, a friend picks me up in her car to meet our group of friends at the pool. We swim for 45 minutes, and then we always take time for a coffee in a tearoom right next to the pool.”(Participant 19—moderate vascular dementia)
“At the end of the morning, about four times a week, I attend an activity organised by the social workers in the community hall, such as gymnastics.”(Participant 20—moderate Alzheimer’s disease)
“I usually go for a walk three times a week with a friend, and we go for coffee in a tearoom near my house. I also go shopping with my daughter, once a week, in a supermarket.”(Participant 21—early-stage Alzheimer’s disease)
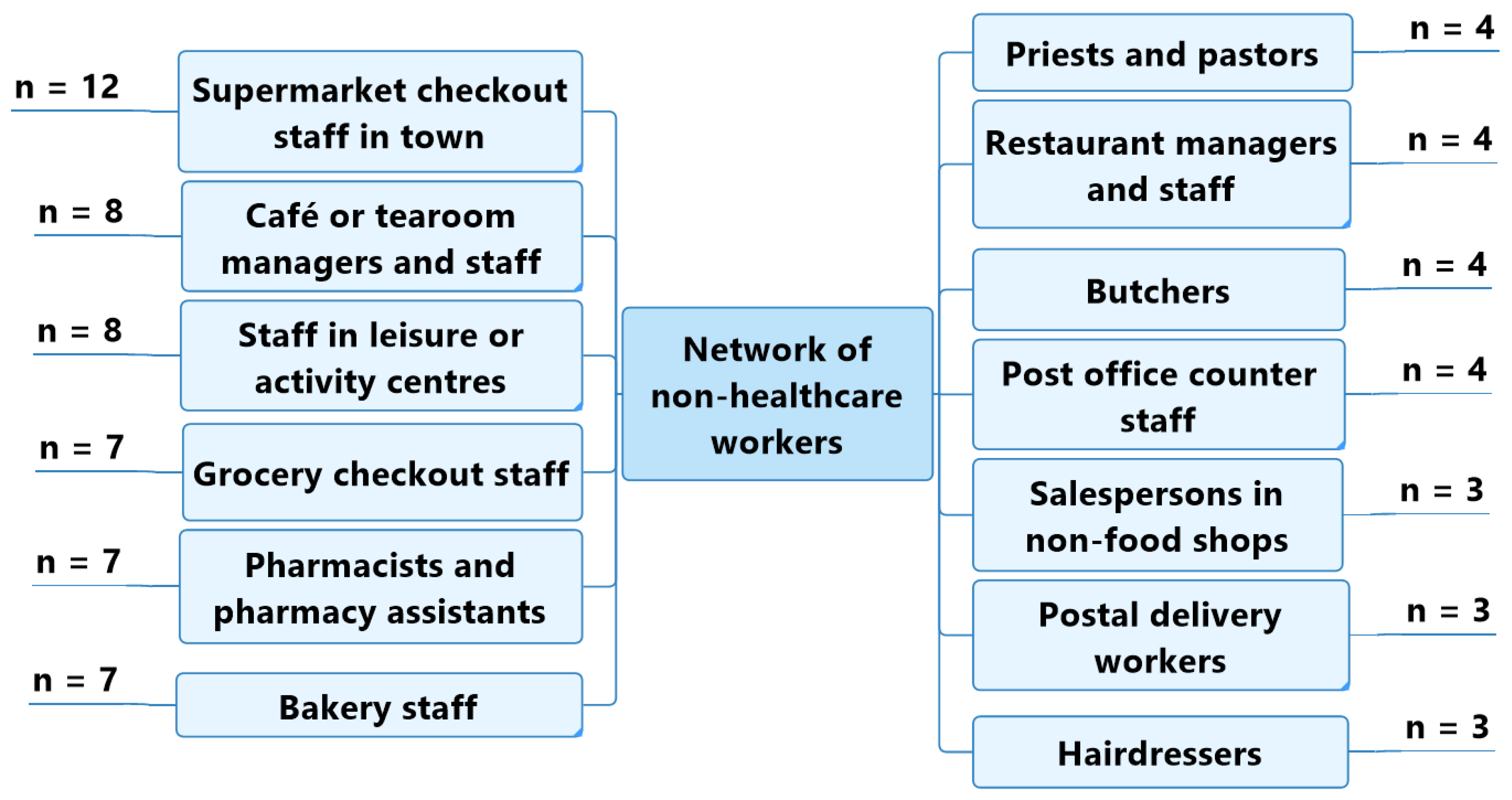
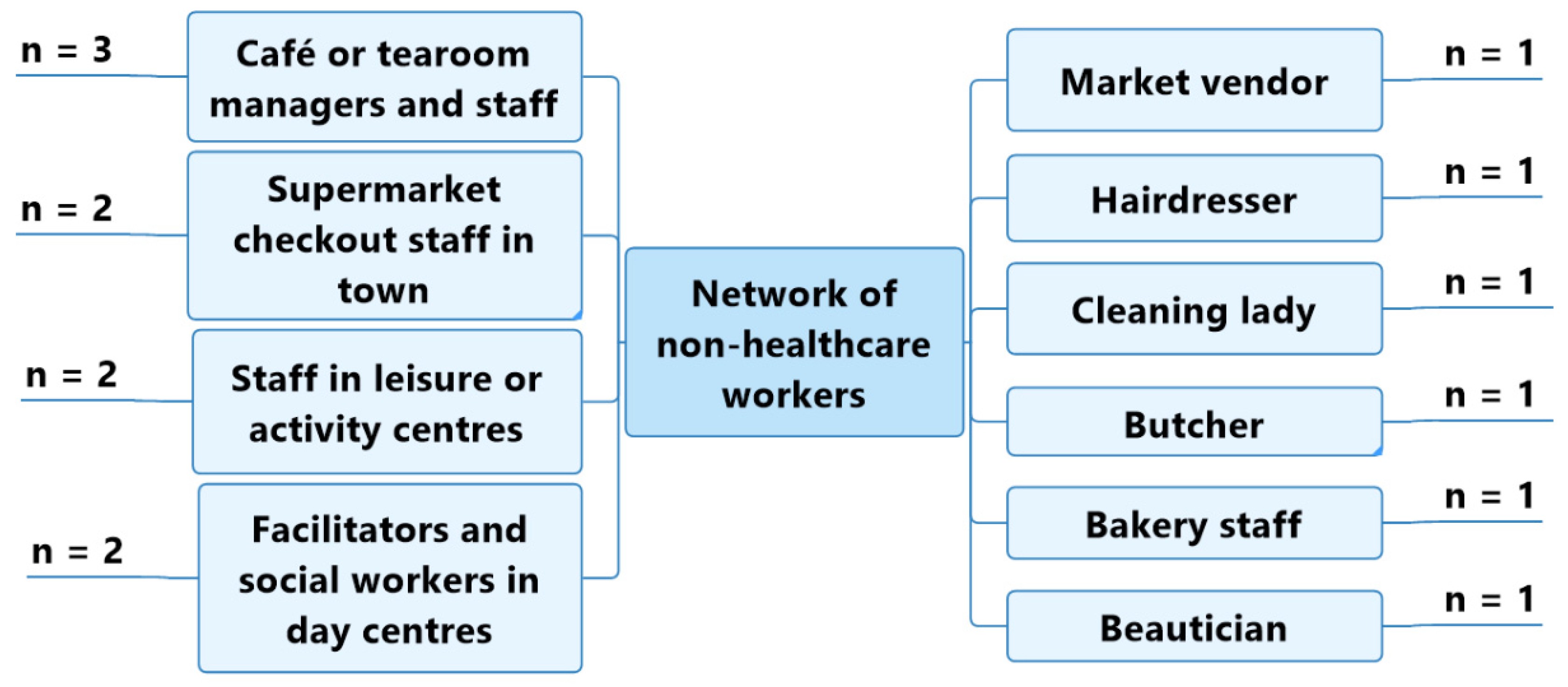
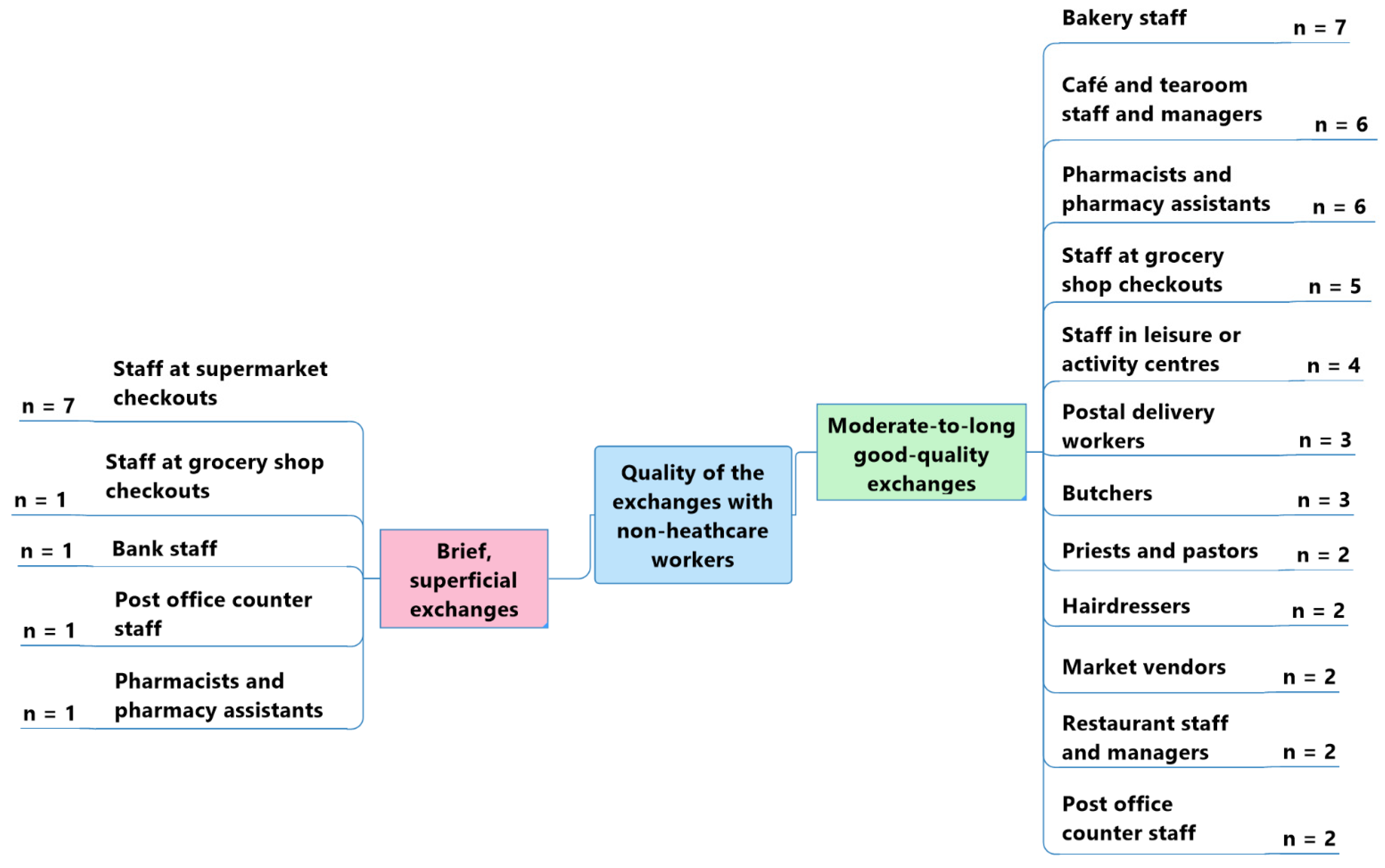
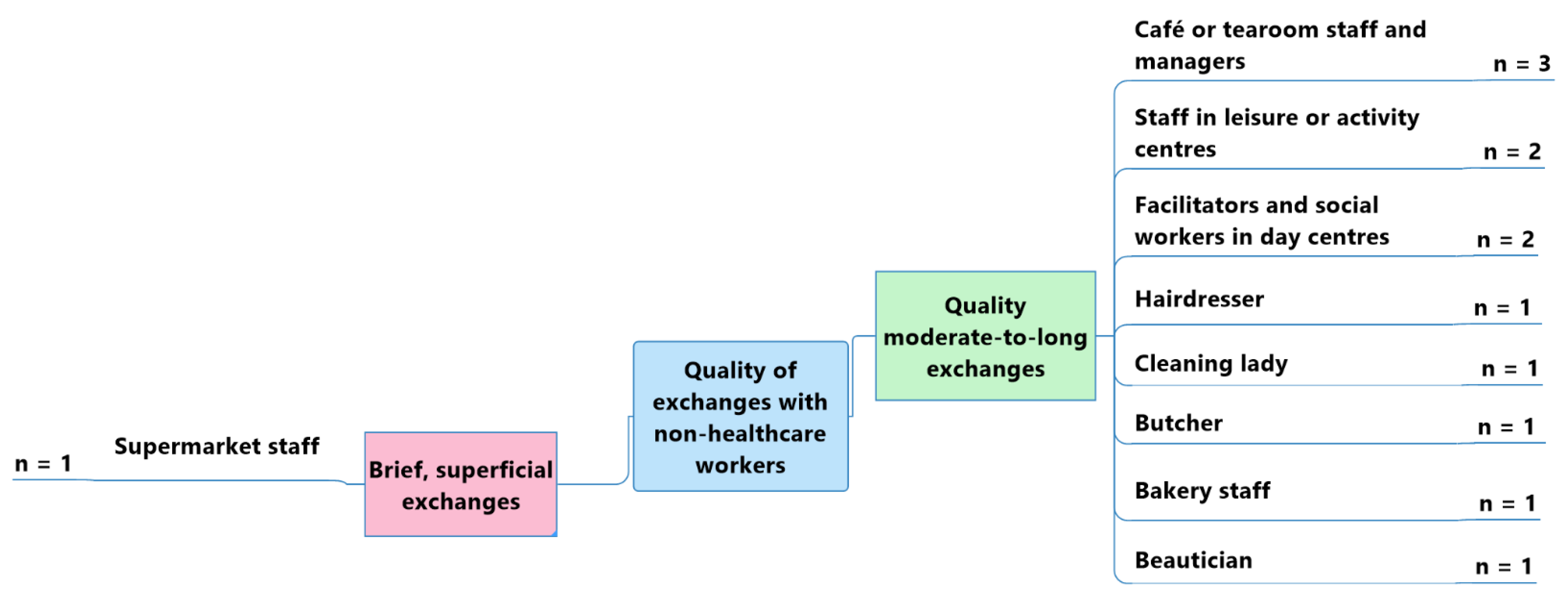
3.2.2. Theme 2: Social Networks
“I really enjoy talking to the people I meet. I think that it’s important to take the time to talk with other people; you often learn lots of things.”(Participant 9)
“I think I have excellent relations with the people in my neighbourhood, especially with the staff at the bakery and butcher’s shop, which are very close to my apartment. We all know each other and are happy to talk to each other.”(Participant 18—mild memory impairment)
“I don’t talk much with people I meet outside my house. I’m not much of a talker; I don’t like to bother people. We just talk about the weather.”(Participant 1)
“I’m a very social person. I think social relationships are what keep us alive. But I regret to see how the world has changed and become more and more stressful. People take less time to talk than they did before. All the emphasis is on money, not on human relations.”(Participant 5)
“Since I’ve lived in the city, social relations have been very different. It was different in the village. Everybody knows each other, whereas in town you’re a bit anonymous. Community life is richer in a village—I liked that. They know me well, but here in town, the checkout ladies don’t have the time.”(Participant 2)
“When you live in a village, you’ve known everybody for years. Besides, my children feel more reassured because I live here: they know that I’m well taken care of.”(Participant 7)
- Bakery sales staff (n = 7).
“There are three sales ladies at the bakery —all very kind.”(Participant 9)
- Café and tearoom staff and managers (n = 6).
“I often go for coffee with my wife at the tearoom, where we have very good relations with the staff.”(Participant 8)
- Pharmacists and pharmacy assistants (n = 6).
“With the people I meet, it’s often short discussions: we mostly talk about the weather. I sometimes have longer discussions with some people. My hairdresser and my pharmacist know me well, and we often have time for a talk.”(Participant 9)
- Grocery shop checkout staff (n = 5).
“I like talking to the checkout lady at the grocery shop near my house. It’s a bit of a change of scenery, and it cheers you up.”(Participant 7)
- Leisure or activity centre staff (n = 4).
“As I go to the pool every day, I talk very often with the three lifeguards who work there.”(Participant 8)
“The checkout ladies in my village and in the supermarkets are very kind, but I don’t stop very long to talk to them; I don’t want to disturb them. There is often a lot of people, so I just say ‘Hello’ so as not to bother them and to be quick.”(Participant 1)
[…] “I don’t talk much with sales staff and checkout ladies at the shopping centre. I don’t know them—there’s just a quick exchange of courtesies.”(Participant 12)
“I go to the day centre twice a week, and I go for coffee at a tearoom near my flat about three times a week. I get on well with the staff who work there; they are always cheerful.”(Participant 17—moderate Alzheimer’s disease)
“I know the people who work at the tennis club very well; I see them often.”(Participant 21—early-stage Alzheimer’s disease)
“The contacts we have with the supermarket staff are superficial and brief. They don’t take the time to speak, and they’re not that attentive. We’re just passing through.”(Participant 18—mild memory impairment)
3.2.3. Theme 3: Non-Life-Threatening Emergencies
“I think people in my village would notice if there were changes in my behaviour. I think that they would notice straight away if I wasn’t up on my game.”(Participant 7)
“I think the people I meet in the community would be able to detect a change in my behaviour. I think that they’d say to themselves, ‘Hey! She’s not her usual self’.”(Participant 15)
“Until now, I have not experienced any non-life-threatening emergency related to my husband’s memory impairment.”(Caregiver for participant 18—mild memory impairment)
“My mother never goes very far from her sheltered accommodation; she is very careful. As soon as she can’t see the building anymore, she retraces her steps.”(Caregiver for participant 20—moderate Alzheimer’s disease)
“My mother has never found herself in a difficult situation. She has retained a lot of her habits. She’s never wandered off on her own, and she’s never left the cooking hobs on, for example.”(Caregiver for participant 21—early-stage Alzheimer’s disease)
“My father left home and took the train to his village station. Luckily, the train’s ticket inspector noticed that he was behaving unusually and that he did not have a ticket. He had also seen him get on the train and knew which station he had boarded at. The controller then reacted very well, bringing my father in to check all the other tickets with him, and then taking him back to his starting point on the way home. There, he asked some villagers about his identity and was able to contact me directly to pick him up.”(Caregiver for participant 17—moderate Alzheimer’s disease)
“One day, my aunt got on a bus because it stopped right next to her. Luckily, the bus terminal was just two stops further, so the driver asked her where she wanted to go and noticed that she was a little confused. Luckily, she had the presence of mind to give him her telephone and ask him to call me, which the driver did, and I was able to come and collect her.”(Caregiver for participant 19—moderate vascular dementia)
“I don’t think people in the community can notice a disorder in another person. For example, if you take my dad’s situation, he’s somebody who can answer quickly. I’m scared that if he had a problem, the people opposite him might ask him some questions, think that he is just a little strange and not take things any further.”(Caregiver for participant 17—moderate Alzheimer’s disease)
4. Discussion
5. Limitations
6. Strengths
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Themes | Questions |
| Profile | - Can you describe yourself? - What is your family situation? - How would you describe your place of residence? |
| Lifestyle habits | - How would you describe one of your typical days (weekdays and weekends)? - Do you have any leisure activities? |
| Mobility | - Describe the journeys you make during the week and at weekends. - Which modes of transport do you use? - Describe the locations you frequent and how often you frequent them. |
| Meeting points | - Do you regularly meet up with people outside your home? - Who do you see most frequently outside your home? |
| Perceptions about social contacts | - How do you perceive your social contacts with others? - How would you describe your exchanges with them? Are they brief? - Are they meaningful?Do your interlocutors ask how you are? - Do you think that your interlocutors would notice a change in the state of your physical or psychological health? |
References
- World-Health-Organization. World Report on Ageing and Health; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- Dillon, C.; Serrano, C.M.; Castro, D.; Leguizamon, P.P.; Heisecke, S.L.; Taragano, F.E. Behavioral symptoms related to cognitive impairment. Neuropsychiatr. Dis. Treat. 2013, 9, 1443–1455. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.; Price, K.; Meyer, J. Home Alone with Dementia. SAGE Open 2016, 6, 2158244016664954. [Google Scholar] [CrossRef]
- Dury, R. Social isolation and loneliness in the elderly: An exploration of some of the issues. Br. J. Community Nurs. 2014, 19, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Hedman, A.; Lindqvist, E.; Nygard, L. How older adults with mild cognitive impairment relate to technology as part of present and future everyday life: A qualitative study. BMC Geriatr. 2016, 16, 73. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S.; Petersen, R.C. Mild cognitive impairment and mild dementia: A clinical perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef]
- Monod, S.; Sautebin, A. Vieillir et devenir vulnérable. Rev. Médicale Suisse 2009, 5, 2353–2357. [Google Scholar]
- Holtzman, R.E.; Rebok, G.W.; Saczynski, J.S.; Kouzis, A.C.; Wilcox Doyle, K.; Eaton, W.W. Social network characteristics and cognition in middle-aged and older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2004, 59, P278–P284. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef]
- Zunzunegui, M.V.; Alvarado, B.E.; Del Ser, T.; Otero, A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S93–S100. [Google Scholar] [CrossRef]
- Perruchoud, E.; von Gunten, A.; Ferreira, T.; Matos Queiros, A.; Verloo, H. Citizens, Neighbors, and Informal Caregivers Exposed to Challenging Behaviors and Behavioral Changes in Community-Dwelling Older Adultswith Cognitive Impairment: A Review. Health Educ. Public Health 2021, 4, 1. [Google Scholar] [CrossRef]
- Clark, A.; Campbell, S.; Keady, J.; Kullberg, A.; Manji, K.; Rummery, K.; Ward, R. Neighbourhoods as relational places for people living with dementia. Soc. Sci. Med. 2020, 252, 112927. [Google Scholar] [CrossRef] [PubMed]
- Ward, R.; Clark, A.; Campbell, S.; Graham, B.; Kullberg, A.; Manji, K.; Rummery, K.; Keady, J. The lived neighborhood: Understanding how people with dementia engage with their local environment. Int. Psychogeriatr. 2018, 30, 867–880. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Heffernan, M.; Kochan, N.A.; Draper, B.; Trollor, J.N.; Reppermund, S.; Slavin, M.J.; Sachdev, P.S. Mild cognitive impairment in a community sample: The Sydney Memory and Ageing Study. Alzheimers Dement 2013, 9, 310–317.e311. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.T.; Moniz-Cook, E.; Iliffe, S.; Campion, P.; Vernooij-Dassen, M.; Zanetti, O.; Franco, M.; Group, I. Dementia: Issues in early recognition and intervention in primary care. J. R. Soc. Med. 2003, 96, 320–324. [Google Scholar] [CrossRef]
- Apostolo, J.; Holland, C.; O’Connell, M.D.; Feeney, J.; Tabares-Seisdedos, R.; Tadros, G.; Campos, E.; Santos, N.; Robertson, D.A.; Marcucci, M.; et al. Mild cognitive decline. A position statement of the Cognitive Decline Group of the European Innovation Partnership for Active and Healthy Ageing (EIPAHA). Maturitas 2016, 83, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Promotion-Santé-Suisse. Projet “CareMENS”. Available online: https://promotionsante.ch/pds/projets-soutenus/caremens.html (accessed on 1 April 2022).
- De Chesnay, M.; Abrums, M.E. Nursing Research Using Ethnography: Qualitative Designs and Methods; online resource (374); Springer: New York, NY, USA, 2015; p. 1. [Google Scholar]
- Mayan, M.J. Essentials of Qualitative Inquiry; online resource (173 pages); Routledge: London, UK, 2016; p. 1. [Google Scholar]
- Confederation, S. Swiss State Secretariat for Education, Research and Innovation (SEFRI). Available online: https://www.sbfi.admin.ch/sbfi/fr/home.html (accessed on 1 July 2022).
- Naderifar, M.; Goli, H.; Ghaljaie, F. Snowball Sampling: A Purposeful Method of Sampling in Qualitative Research. Strides Dev. Med. Educ. 2017, 14. [Google Scholar] [CrossRef]
- Walker, J.L. The use of saturation in qualitative research. J. Cardiovasc. Nurs. 2012, 22, 37–46. [Google Scholar]
- Gauthier, B. Recherche Sociale: De la problématique à la Collecte des Données; Presses de l’Université du Québec: Québec, QC, Canada, 2009; p. 767. [Google Scholar]
- Seale, C. Researching Society and Culture, 4th ed.; Sage: London, UK, 2018; p. xi, 648 Seiten. [Google Scholar]
- Wehbe-Alamah, H.; McFarland, M. Leininger’s Ethnonursing Research Method: Historical Retrospective and Overview. J. Transcult. Nurs. 2020, 31, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Moore, T.F.; Hollett, J. Giving voice to persons living with dementia: The researcher’s opportunities and challenges. Nurs. Sci. Q. 2003, 16, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Cornwell, B.; Laumann, E.O.; Schumm, L.P. The Social Connectedness of Older Adults: A National Profile *. Am. Sociol. Rev. 2008, 73, 185–203. [Google Scholar] [CrossRef] [PubMed]
- Beuscher, L.; Grando, V.T. Challenges in conducting qualitative research with individuals with dementia. Res. Gerontol. Nurs. 2009, 2, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, Y.S.; Lincoln, Y.S.; Guba, E.G.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Beverly Hills, CA, USA, 1985; p. 416. [Google Scholar]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The use of triangulation in qualitative research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Olsen, V.; Taylor, L.; Whiteley, K.; Ellerton, A.; Kingston, P.; Bailey, J. Exploring public perceptions and understanding of dementia: Analysing narratives from the Mass Observation Project. Dementia 2020, 19, 2804–2820. [Google Scholar] [CrossRef] [PubMed]
- Owokuhaisa, J.; Rukundo, G.Z.; Wakida, E.; Obua, C.; Buss, S.S. Community perceptions about dementia in southwestern Uganda. BMC Geriatr. 2020, 20, 135. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interview N° | Gender | Age | Diagnosis |
Marital Status | Housing | Location * |
Lives Alone |
Family Caregiver |
|---|---|---|---|---|---|---|---|---|
| 1 | Woman | 82 | - | Married | House | Village | No | - |
| 2 | Woman | 68 | - | Widowed | Flat | Medium-sized town | Yes | - |
| 3 | Man | 75 | - | Married | Flat | Medium-sized town | No | - |
| 4 | Man | 83 | - | Widowed | Flat | Village | Yes | - |
| 5 | Woman | 73 | - | Married | Flat | Medium-sized town | No | - |
| 6 | Man | 80 | - | Married | House | Village | No | - |
| 7 | Woman | 91 | - | Widowed | House | Mountain village | Yes | - |
| 8 | Man | 65 | - | Married | Flat | Medium-sized town | No | - |
| 9 | Woman | 72 | - | Single | House | Medium-sized town | Yes | - |
| 10 | Man | 85 | - | Widowed | House | Village | Yes | - |
| 11 | Man | 81 | - | Widowed | Flat | Dense urban city | Yes | - |
| 12 | Man | 79 | - | Single | Flat | Dense urban city | No | - |
| 13 | Woman | 69 | - | Married | Flat | Dense urban city | No | - |
| 14 | Woman | 90 | - | Married | Flat | Dense urban city | No | - |
| 15 | Woman | 72 | - | Separated | Flat | Dense urban city | Yes | - |
| 16 | Man | 72 | - | Married | Flat | Dense urban city | No | - |
| 17 | Man | 82 | Moderate Alzheimer’s disease | Widowed | Daughter’s flat | Village | No | Daughter |
| 18 | Man | 76 | Mild memory impairment | Married | Flat | Village | Yes | Wife |
| 19 | Woman | 86 | Moderate vascular dementia | Single | Flat | Medium-sized town | Yes | Niece |
| 20 | Woman | 82 | Moderate Alzheimer’s disease | Widowed | Sheltered flat | Village | Yes | Daughters |
| 21 | Woman | 66 | Early stage Alzheimer’s disease | Widowed | House | Medium-sized town | Yes | Daughter |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perruchoud, E.; von Gunten, A.; Ferreira, T.; Queirós, A.M.; Verloo, H. Home-Dwelling Older Adults’ Day-to-Day Community Interactions: A Qualitative Study. Geriatrics 2022, 7, 82. https://doi.org/10.3390/geriatrics7040082
Perruchoud E, von Gunten A, Ferreira T, Queirós AM, Verloo H. Home-Dwelling Older Adults’ Day-to-Day Community Interactions: A Qualitative Study. Geriatrics. 2022; 7(4):82. https://doi.org/10.3390/geriatrics7040082
Chicago/Turabian StylePerruchoud, Elodie, Armin von Gunten, Tiago Ferreira, Alcina Matos Queirós, and Henk Verloo. 2022. "Home-Dwelling Older Adults’ Day-to-Day Community Interactions: A Qualitative Study" Geriatrics 7, no. 4: 82. https://doi.org/10.3390/geriatrics7040082
APA StylePerruchoud, E., von Gunten, A., Ferreira, T., Queirós, A. M., & Verloo, H. (2022). Home-Dwelling Older Adults’ Day-to-Day Community Interactions: A Qualitative Study. Geriatrics, 7(4), 82. https://doi.org/10.3390/geriatrics7040082