
Relationship between Cognitive Function and Sway of Body in Standing Posture: A Cross-Sectional Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sway Measurement Equipment
2.3. Cognitive Assessment Protocol
2.4. Sway Test Protocol
2.5. Data Analysis
3. Results
3.1. The Participant Characteristics
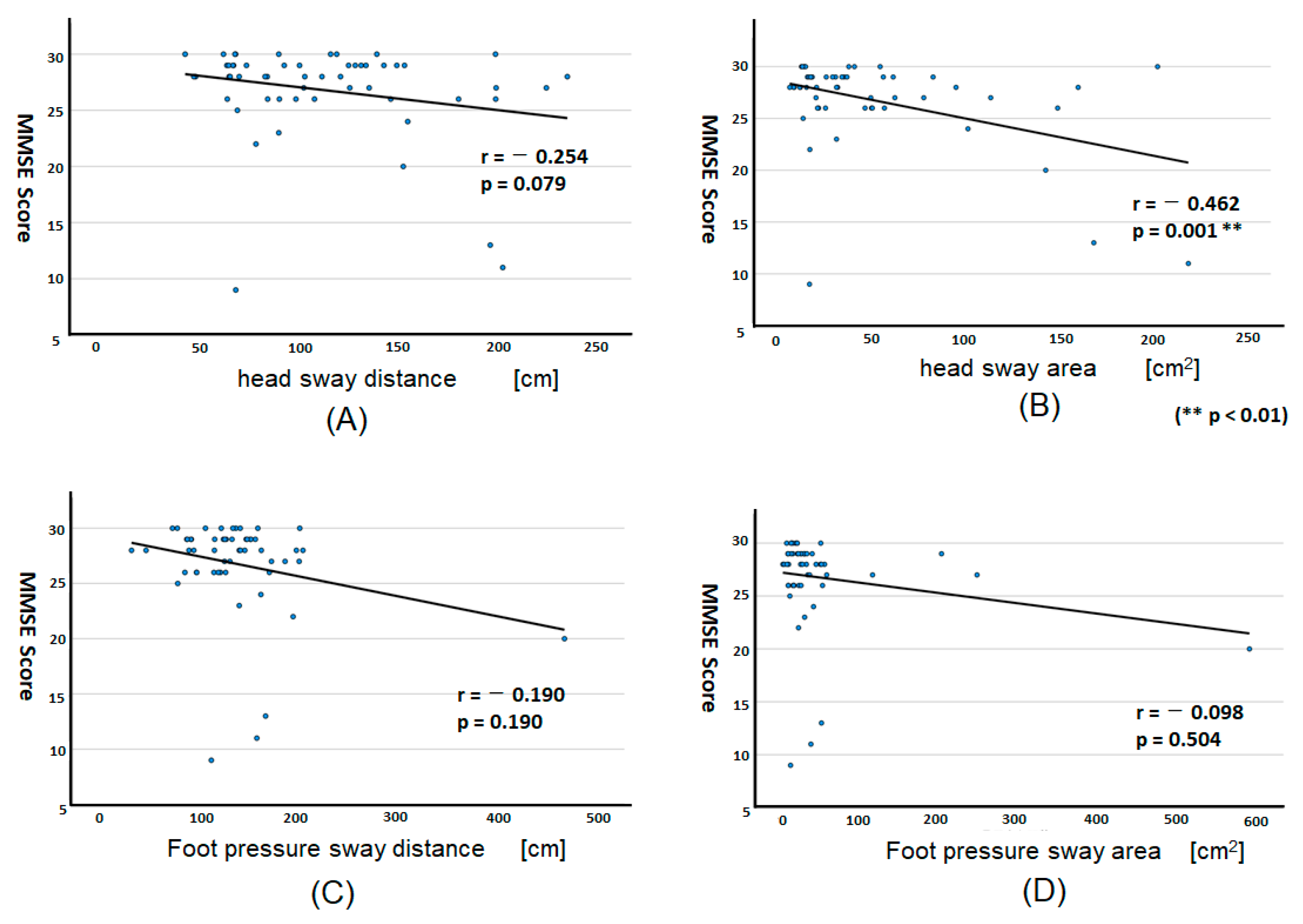
3.2. MMSE Scores and Sway Test Standing on One-Leg
3.3. MMSE Scores and Sway Test Standing on Two-Legs
3.4. Sway Test Standing in the Difference between EO and EC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Allan, L.M.; Ballard, C.G.; Burn, D.J.; Kenny, R.A. Prevalence and severity of gait disorders in Alzheimer’s and non-Alzheimer’s dementias. J. Am. Geriatr. Soc. 2005, 53, 1681–1687. [Google Scholar] [CrossRef] [PubMed]
- Buracchio, T.; Dodge, H.H.; Howieson, D.; Wasserman, D.; Kaye, J. The trajectory of gait speed preceding mild cognitive impairment. Arch. Neurol. 2010, 67, 980–986. [Google Scholar] [CrossRef]
- Cheng, P.; Tan, L.; Ning, P.; Li, L.; Gao, Y.; Wu, Y.; Schwebel, D.C.; Chu, H.; Yin, H.; Hu, G. Comparative Effectiveness of Published Interventions for Elderly Fall Prevention: A Systematic Review and Network Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 498. [Google Scholar] [CrossRef] [Green Version]
- Verghese, J.; Robbins, M.; Holtzer, R.; Zimmerman, M.; Wang, C.; Xue, X.; Lipton, R.B. Gait dysfunction in mild cognitive impairment syndromes. J. Am. Geriatr. Soc. 2008, 56, 1244–1251. [Google Scholar] [CrossRef]
- Xu, W.; Chen, T.; Shan, Q.; Hu, B.; Zhao, M.; Deng, X.; Zuo, J.; Hu, Y.; Fan, L. Sarcopenia Is Associated with Cognitive Decline and Falls but Not Hospitalization in Community-Dwelling Oldest Old in China: A Cross-Sectional Study. Med. Sci. Monit. 2020, 26, e919894. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Hirai, H.W.; Wong, S.Y.; Kwok, T.C. Cognitive Tests to Detect Dementia: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2015, 175, 1450–1458. [Google Scholar] [CrossRef] [Green Version]
- Deschamps, T.; Beauchet, O.; Annweiler, C.; Cornu, C.; Mignardot, J.B. Postural control and cognitive decline in older adults: Position versus velocity implicit motor strategy. Gait Posture 2014, 39, 628–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horak, F.B.; Wrisley, D.M.; Frank, J. The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits. Phys. Ther. 2009, 89, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Pieruccini-Faria, F.; Muir-Hunter, S.W.; Montero-Odasso, M. Do depressive symptoms affect balance in older adults with mild cognitive impairment? Results from the “gait and brain study”. Exp. Gerontol. 2018, 108, 106–111. [Google Scholar] [CrossRef]
- Shin, B.M.; Han, S.J.; Jung, J.H.; Kim, J.E.; Fregni, F. Effect of mild cognitive impairment on balance. J. Neurol. Sci. 2011, 305, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Larkin, P.A.; Cook, A.C.; Gear, J.; Singer, J. Decrease in timed balance test scores with aging. Phys. Ther. 1984, 64, 1067–1070. [Google Scholar] [CrossRef] [PubMed]
- Kido, T.; Tabara, Y.; Igase, M.; Ochi, N.; Uetani, E.; Nagai, T.; Yamamoto, M.; Taguchi, K.; Miki, T.; Kohara, K. Postural Instability Is Associated with Brain Atrophy and Cognitive Impairment in the Elderly: The J-SHIPP study. Dement. Geriatr. Cogn. Disord. 2010, 29, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Szczygieł, E.; Fudacz, N.; Golec, J.; Golec, E. The impact of the position of the head on the functioning of the human body: A systematic review. Int. J. Occup. Med. Environ. Health 2020, 17, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Kaufer, D.I.; Williams, C.S.; Braaten, A.J.; Gill, K.; Zimmerman, S.; Sloane, P.D. Cognitive screening for dementia and mild cognitive impairment in assisted living: Comparison of 3 tests. J. Am. Med. Dir. Assoc. 2008, 9, 586–593. [Google Scholar] [CrossRef]
- Saxton, J.; Morrow, L.; Eschman, A.; Archer, G.; Luther, J.; Zuccolotto, A. Computer assessment of mild cognitive impairment. Postgrad Med. 2009, 121, 177–185. [Google Scholar] [CrossRef]
- Tariq, S.H.; Tumosa, N.; Chibnall, J.T.; Perry, M.H., III; Morley, J.E. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder: A pilot study. Am. J. Geriatr. Psychiatry 2006, 14, 900–910. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Magasi, S.R.; Bubela, D.J.; Wang, Y.C.; Gershon, R.C. Grip and knee extension muscle strength reflect a common construct among adults. Muscle Nerve. 2012, 46, 555–558. [Google Scholar] [CrossRef] [Green Version]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing. 2006, 35 (Suppl. S2), ii7–ii11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyama, A.; Takeda, S.; Ito, Y.; Nakajima, T.; Takami, Y.; Takeya, Y.; Yamamoto, K.; Sugimoto, K.; Shimizu, H.; Shimamura, M.; et al. Novel Method for Rapid Assessment of Cognitive Impairment Using High-Performance Eye-Tracking Technology. Sci. Rep. 2019, 9, 12932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, N.E.; Kegelmeyer, D.A.; Kloos, A.D.; Linder, S.; Park, A.; Kataki, M.; Adeli, A.; Agrawal, P.; Scharre, D.W.; Kostyk, S.K. Motor performance differentiates individuals with Lewy body dementia, Parkinson’s and Alzheimer’s disease. Gait Posture 2016, 50, 1–7. [Google Scholar] [CrossRef]
- Beauchet, O.; Annweiler, C.; Callisaya, M.L.; De Cock, A.M.; Helbostad, J.L.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.P.; Blumen, H.M.; Verghese, J.; et al. Poor Gait Performance and Prediction of Dementia: Results From a Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 482–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telenius, E.W.; Engedal, K.; Bergland, A. Effect of a high-intensity exercise program on physical function and mental health in nursing home residents with dementia: An assessor blinded randomized controlled trial. PLoS ONE 2015, 10, e0126102. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Two-Legs (n = 103) Mean ± SD | One-Leg (n = 54) Mean ± SD | p Value | |
|---|---|---|---|
| Age | 77.52 ± 6.90 | 75.4 ± 6.11 | 0.057 |
| Sex (male = 0/female = 1) | 0.9 ± 0.30 | 0.93 ± 0.26 | 0.610 |
| BMI | 22.54 ± 3.32 | 21.9 ± 3.44 | 0.258 |
| Grip strength | 23.27 ± 6.33 | 24.46 ± 5.77 | 0.260 |
| Fatigue on the day of assessment | 0.57 ± 0.67 | 0.53 ± 0.69 | 0.686 |
| Sleep quality | 1.64 ± 0.71 | 1.78 ± 0.76 | 0.249 |
| MMSE score | 26.22 ± 3.96 | 26.8 ± 4.37 | 0.402 |
| MMSE Subscale | Partial Correlation Coefficient | |||||||
|---|---|---|---|---|---|---|---|---|
| Head Sway | Foot Pressure Sway | |||||||
| Distance | p Value | Area | p Value | Distance | p Value | Area | p Value | |
| Orientation to time | −0.242 | 0.093 | −0.464 ** | 0.001 | −0.148 | 0.309 | −0.050 | 0.732 |
| Orientation to place | −0.267 | 0.064 | −0.509 ** | 0.001 | −0.384 ** | 0.006 | −0.295 * | 0.039 |
| Immediate memory | 0.170 | 0.242 | 0.124 | 0.396 | −0.109 | 0.457 | 0.052 | 0.723 |
| Serial sevens | −0.289 * | 0.044 | −0.438 ** | 0.002 | −0.085 | 0.559 | −0.143 | 0.326 |
| Delayed memory | −0.201 | 0.165 | −0.295 * | 0.040 | −0.205 | 0.159 | −0.098 | 0.504 |
| Naming | −0.341 * | 0.016 | −0.492 ** | 0.001 | −0.101 | 0.491 | −0.033 | 0.820 |
| Repetition | −0.171 | 0.239 | −0.335 * | 0.019 | −0.076 | 0.602 | 0.113 | 0.438 |
| Oral instructions | 0.129 | 0.378 | 0.067 | 0.648 | 0.120 | 0.411 | 0.209 | 0.149 |
| Writing instructions | −0.341 * | 0.016 | −0.492 ** | 0.001 | −0.101 | 0.491 | −0.033 | 0.820 |
| Spontaneous writing | 0.072 | 0.621 | 0.035 | 0.814 | 0.095 | 0.515 | 0.128 | 0.382 |
| Copy a design | −0.317 * | 0.027 | −0.179 | 0.218 | −0.080 | 0.585 | −0.330 * | 0.021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naito, T.; Suzuki, Y.; Yamasue, K.; Saito, K.; Umemura, M.; Kojima, N.; Kim, H.; Osuka, Y.; Ishikawa, Y.; Tochikubo, O. Relationship between Cognitive Function and Sway of Body in Standing Posture: A Cross-Sectional Study. Geriatrics 2023, 8, 29. https://doi.org/10.3390/geriatrics8020029
Naito T, Suzuki Y, Yamasue K, Saito K, Umemura M, Kojima N, Kim H, Osuka Y, Ishikawa Y, Tochikubo O. Relationship between Cognitive Function and Sway of Body in Standing Posture: A Cross-Sectional Study. Geriatrics. 2023; 8(2):29. https://doi.org/10.3390/geriatrics8020029
Chicago/Turabian StyleNaito, Takao, Yume Suzuki, Kotaro Yamasue, Kyoko Saito, Masanari Umemura, Narumi Kojima, Hunkyung Kim, Yosuke Osuka, Yoshihiro Ishikawa, and Osamu Tochikubo. 2023. "Relationship between Cognitive Function and Sway of Body in Standing Posture: A Cross-Sectional Study" Geriatrics 8, no. 2: 29. https://doi.org/10.3390/geriatrics8020029
APA StyleNaito, T., Suzuki, Y., Yamasue, K., Saito, K., Umemura, M., Kojima, N., Kim, H., Osuka, Y., Ishikawa, Y., & Tochikubo, O. (2023). Relationship between Cognitive Function and Sway of Body in Standing Posture: A Cross-Sectional Study. Geriatrics, 8(2), 29. https://doi.org/10.3390/geriatrics8020029