
Health Consequences of Falls among Older Adults in India: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Methodological Quality Assessment
2.5. Data Extraction
2.6. Data Synthesis
3. Results
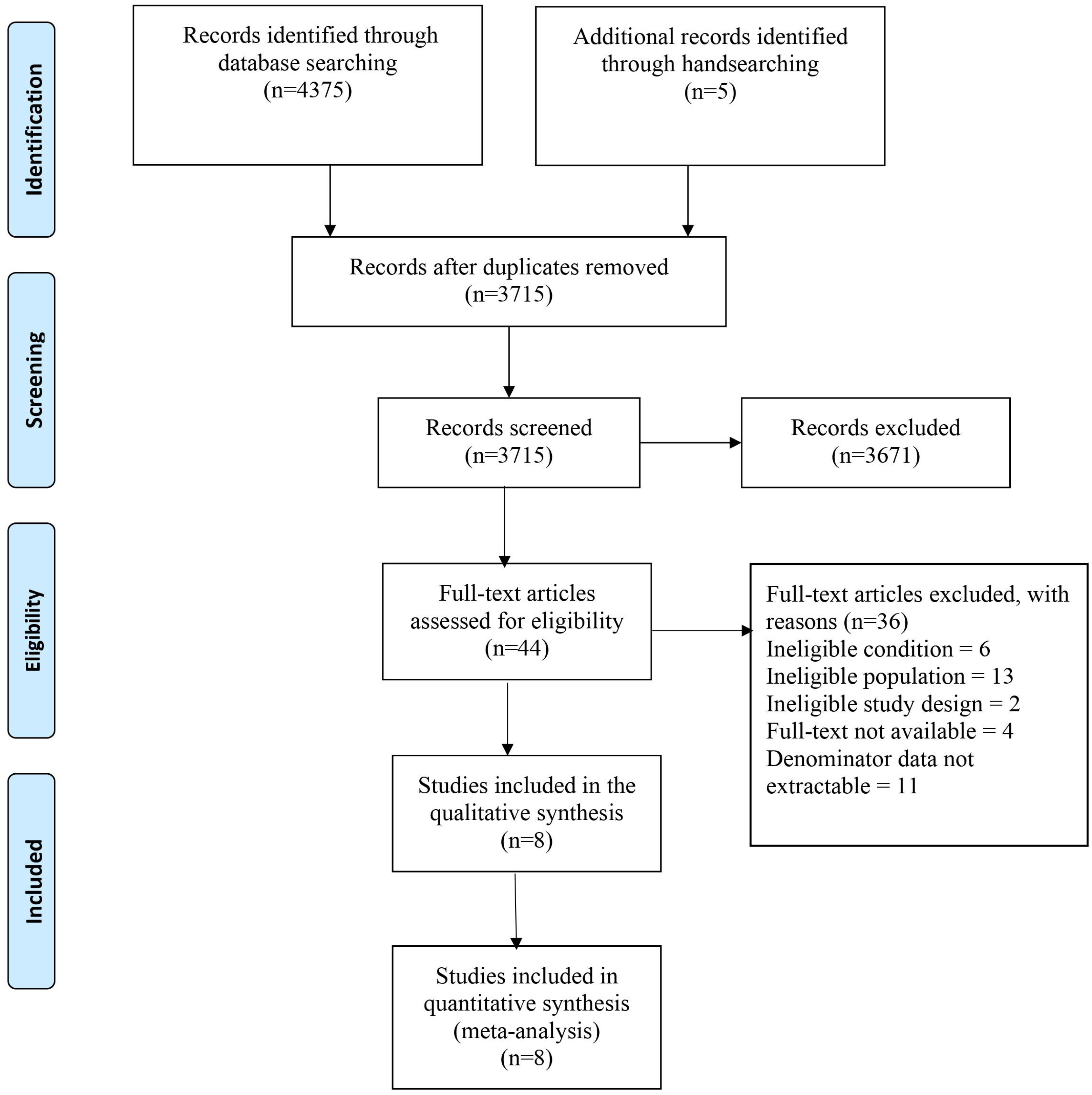
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Methodological Quality of the Included Studies
3.4. Meta-Analysis
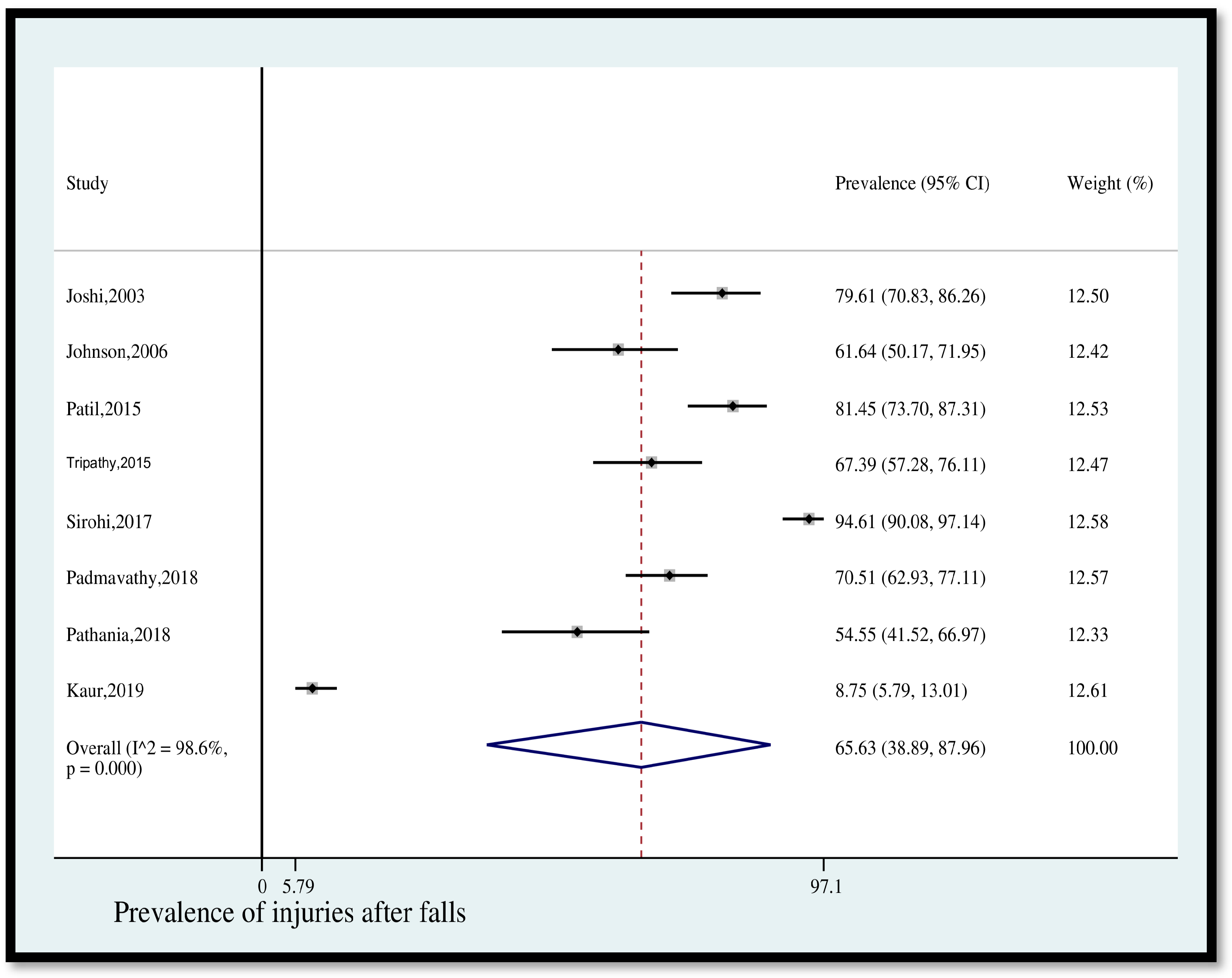
- Prevalence of injuries after falls
- 2.
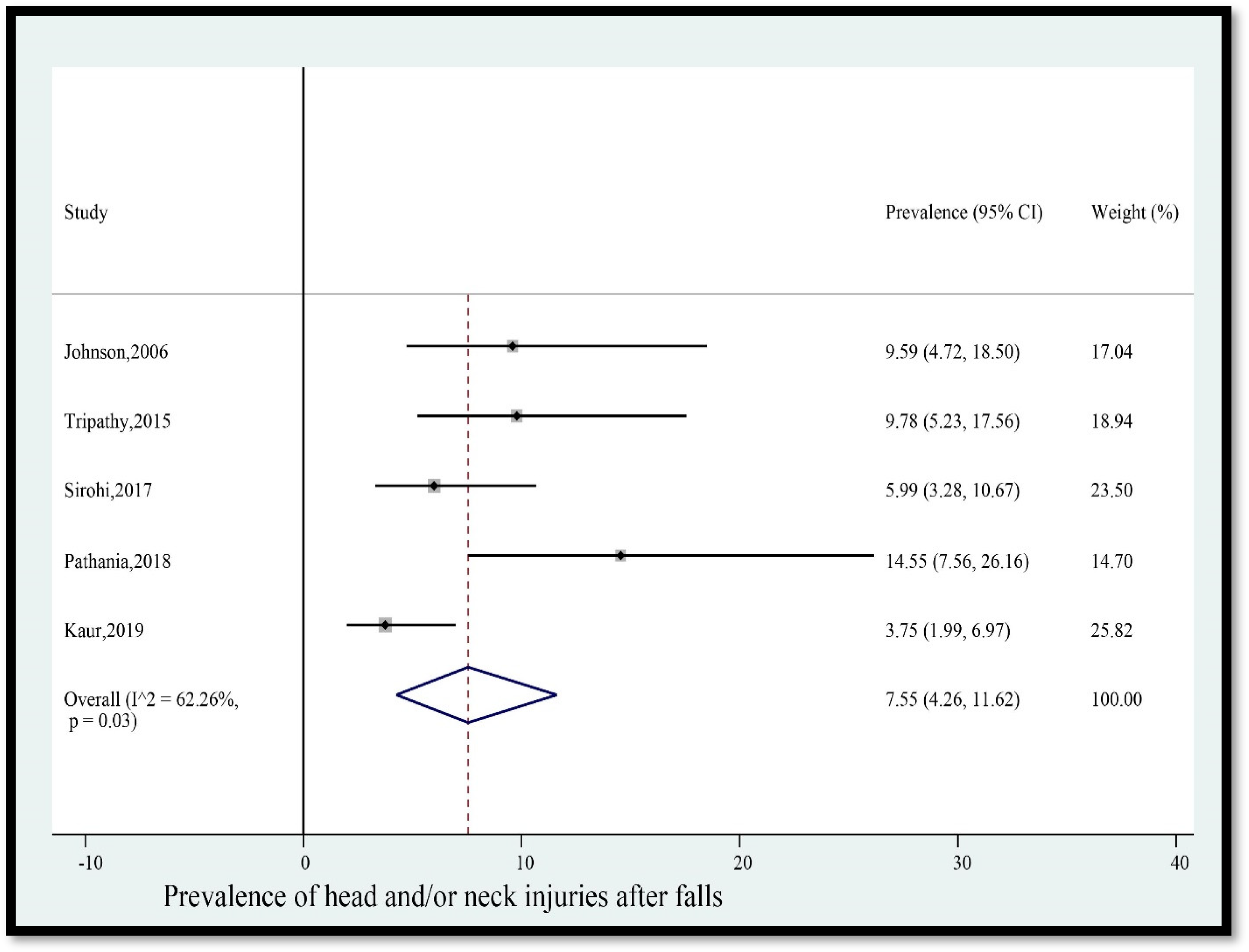
- Prevalence of head and/or neck injuries after falls
- 3.
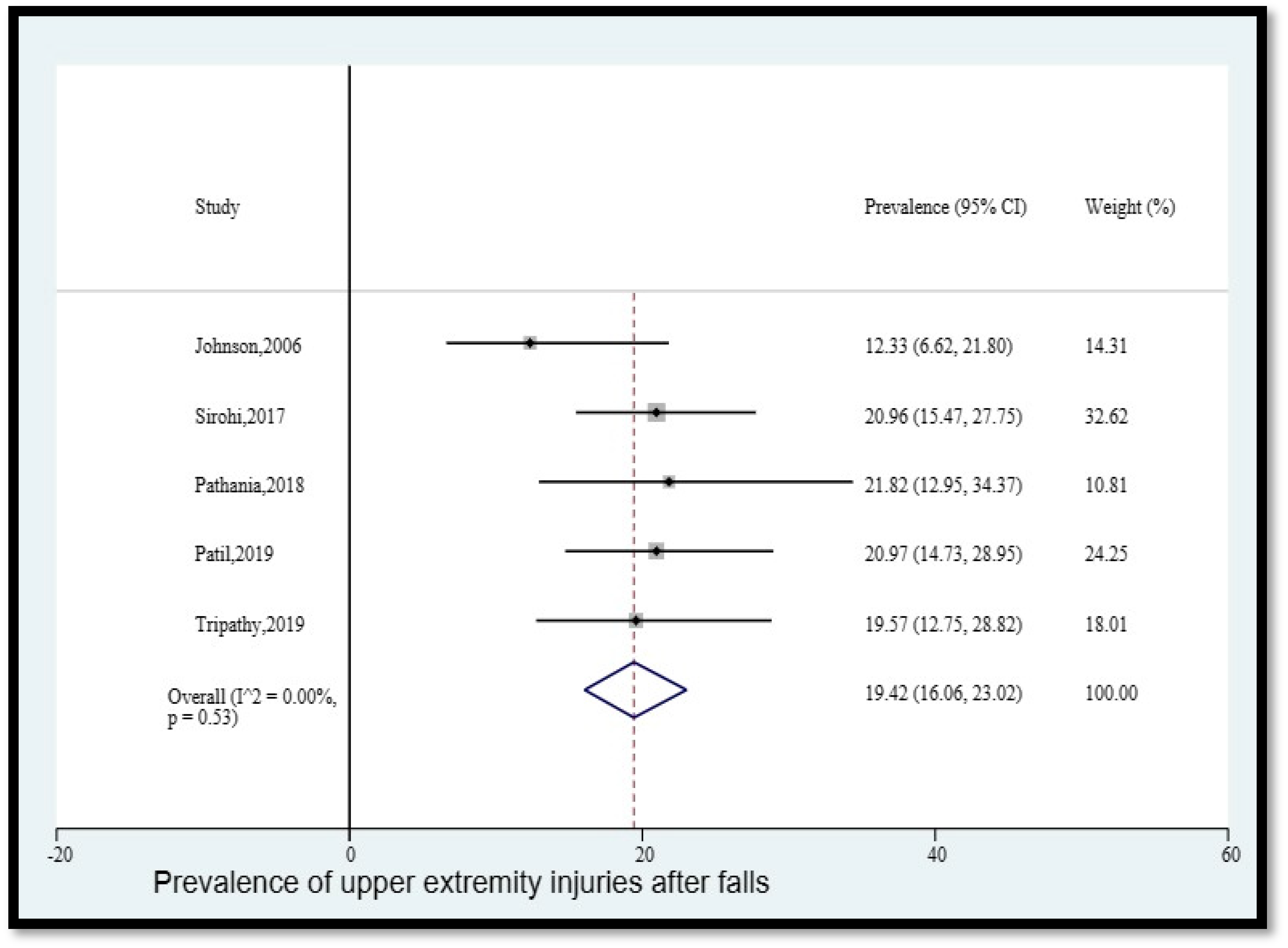
- Prevalence of upper extremity injuries after falls
- 4.
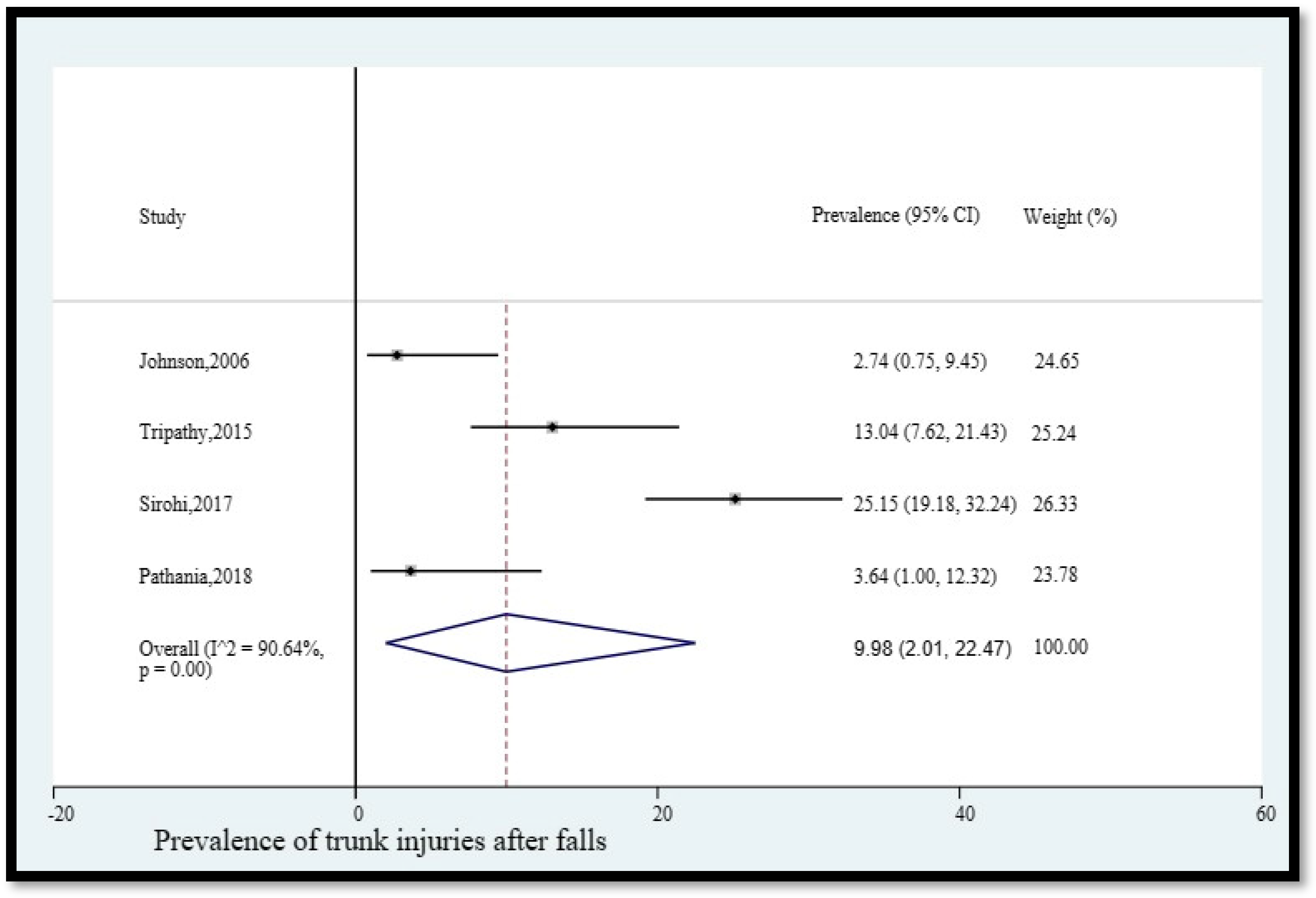
- Prevalence of trunk injuries after falls
- 5.
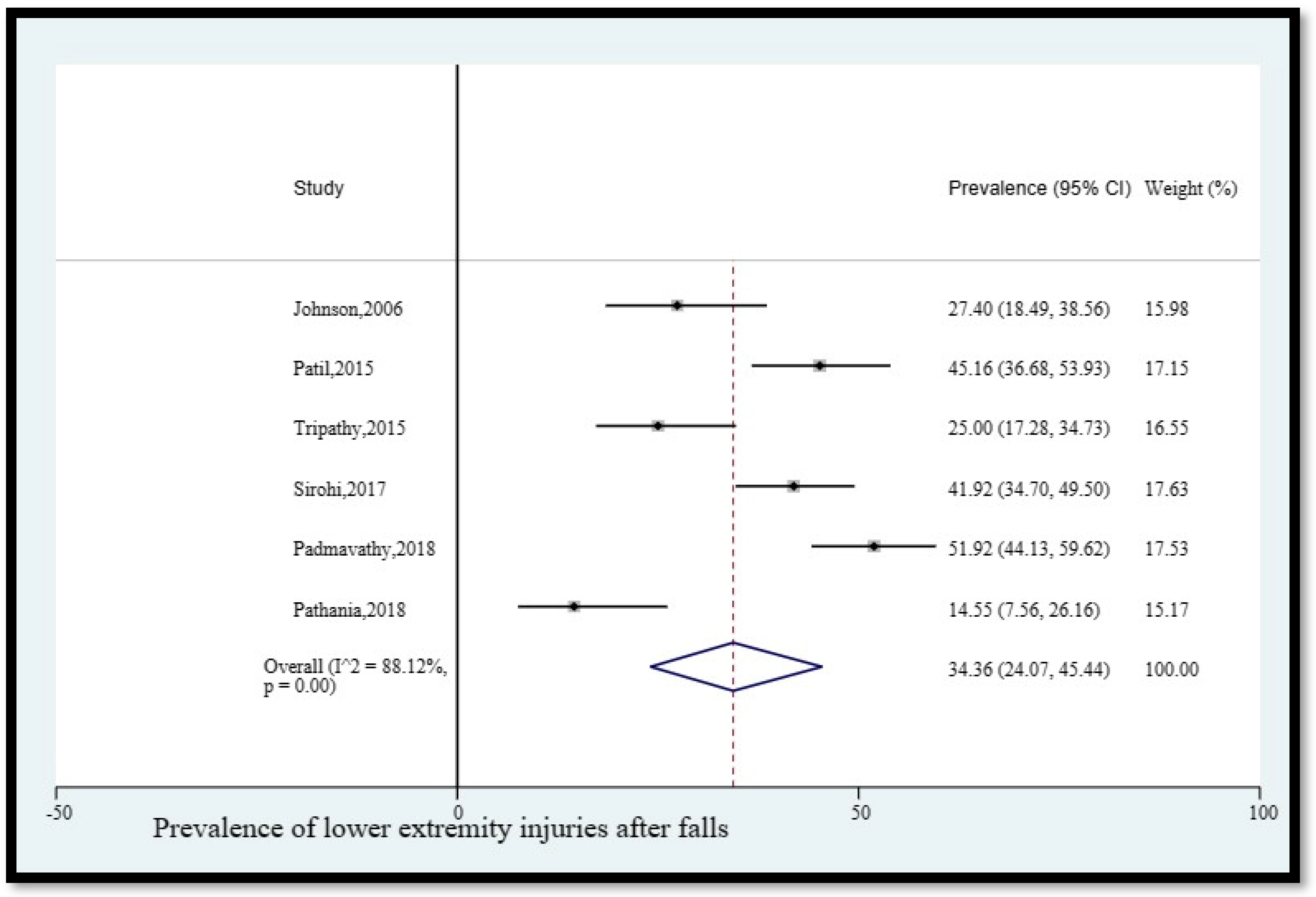
- Prevalence of lower extremity injuries after falls
- 6.
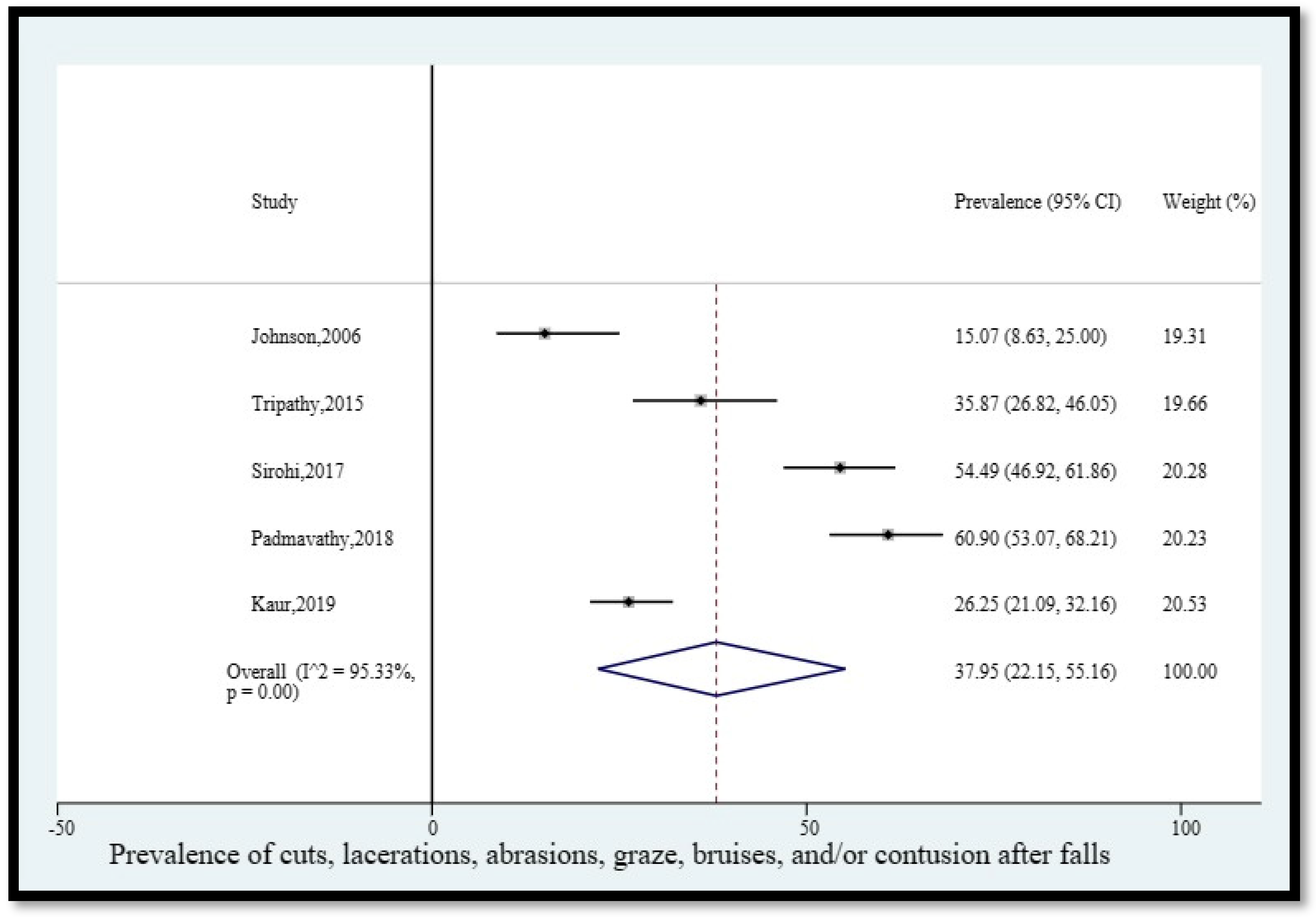
- Prevalence of cuts, lacerations, grazes, bruises, and/or contusions after falls
- 7.
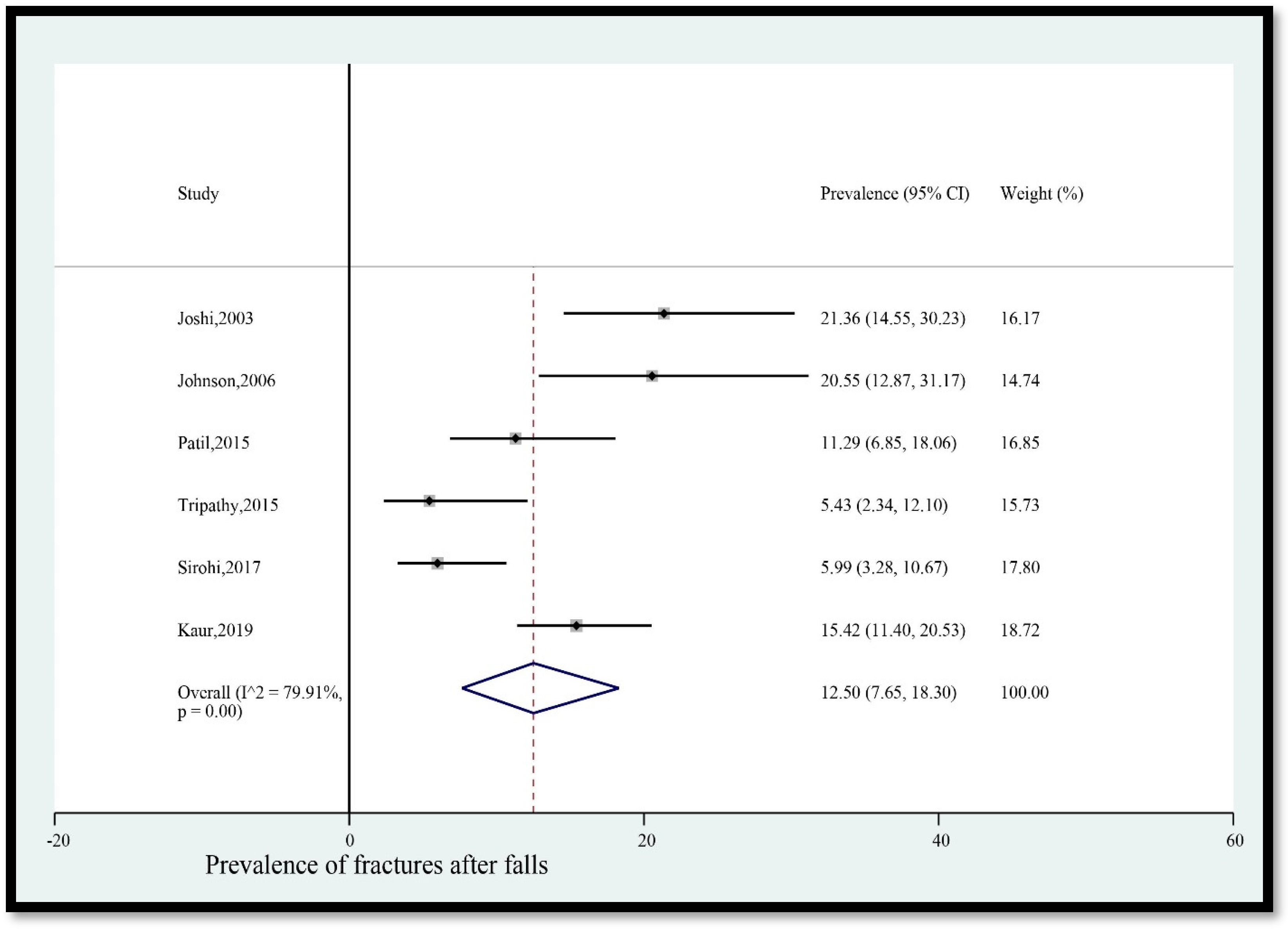
- Prevalence of fractures after falls
- 8.
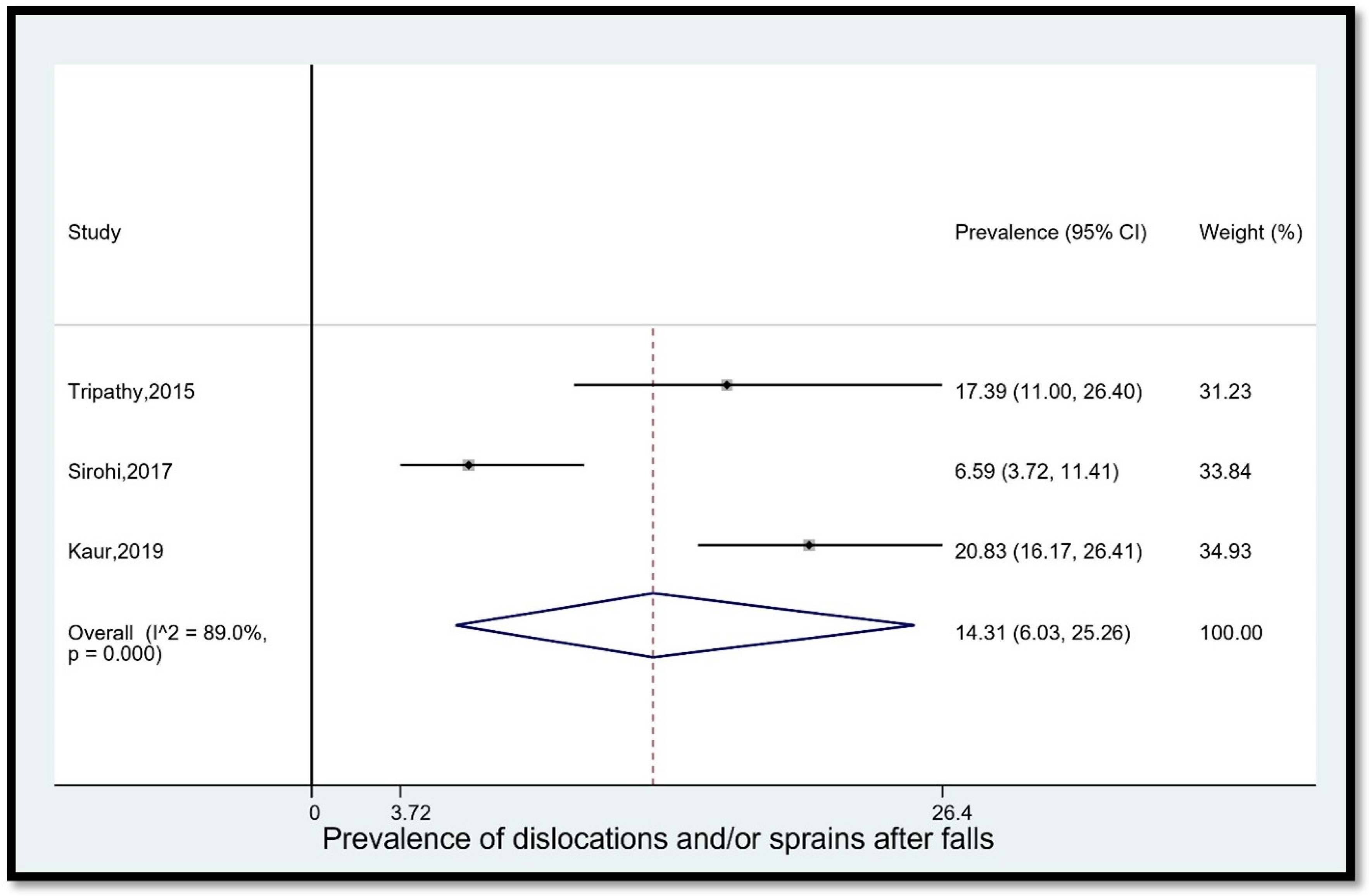
- Prevalence of dislocations and/or sprains after falls
- 9.
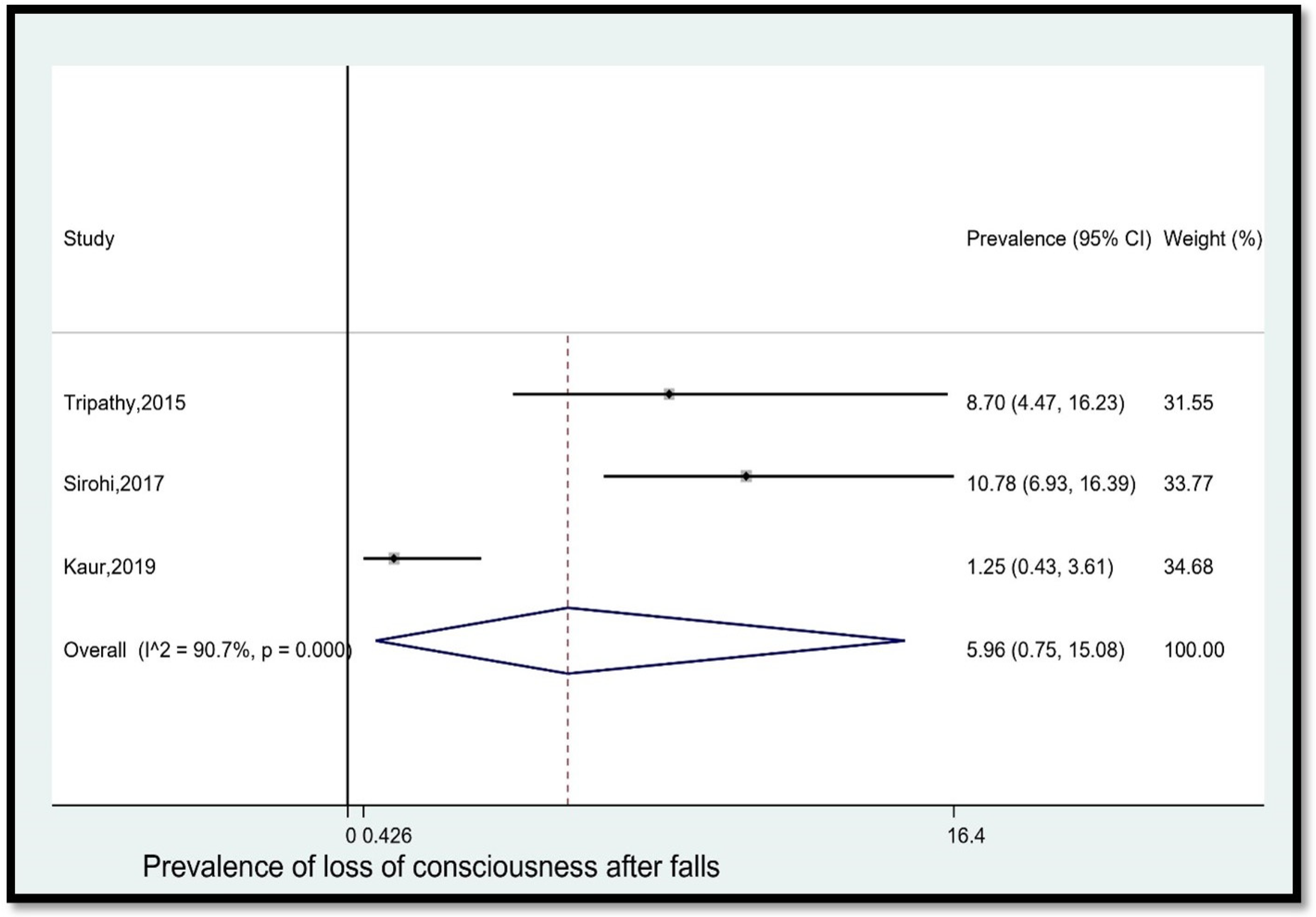
- Prevalence of loss of consciousness after falls
- 10.
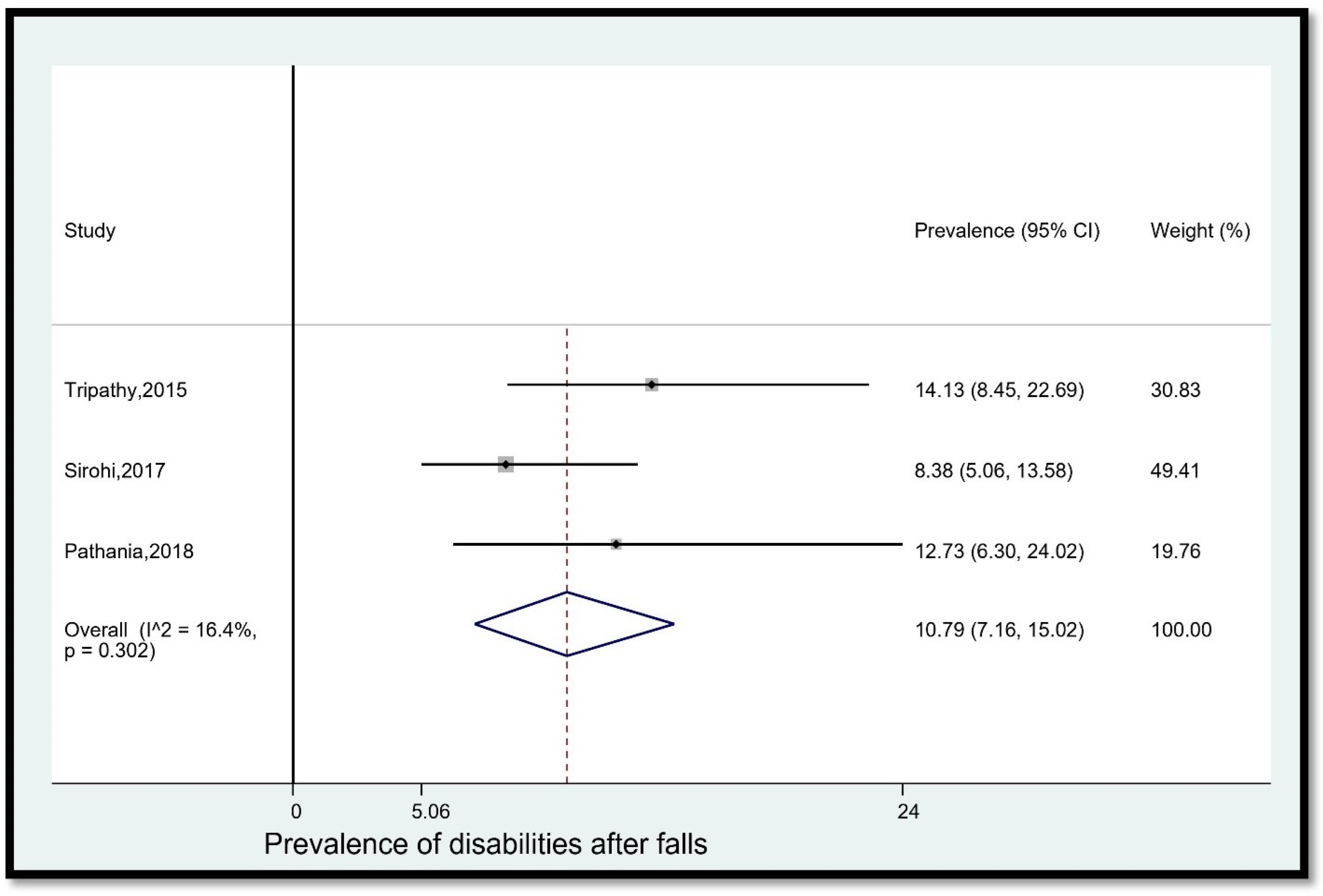
- Prevalence of disabilities after falls
- 11.
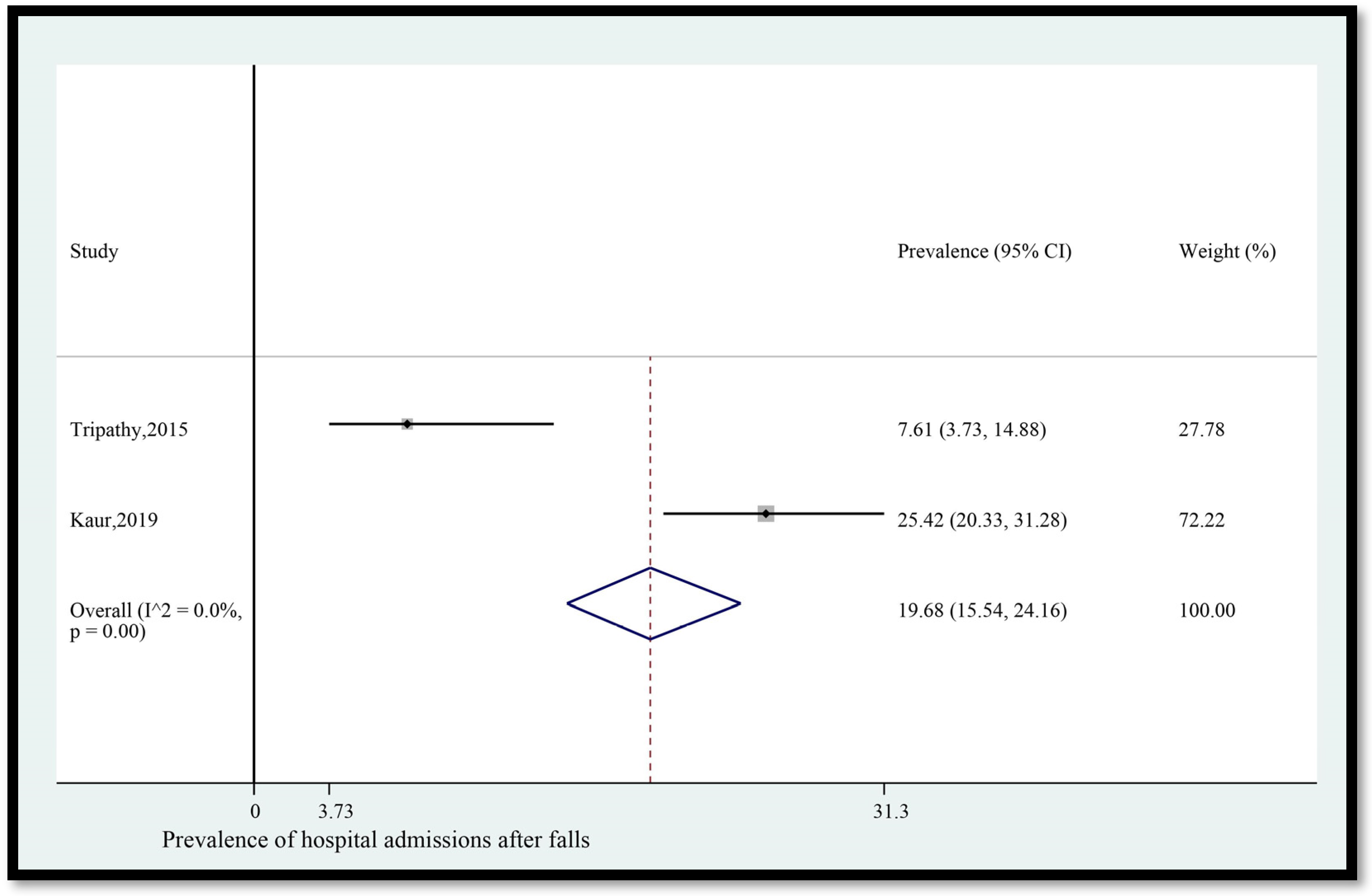
- Prevalence of hospital admissions after falls
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategies
- 1
- exp Accidental falls/
- 2
- (Fall* or fell* or slip* or trip* or stumble*).mp.
- 3
- exp Gait/
- 4
- exp Postural balance/
- 5
- 1 or 2 or 3 or 4
- 6
- exp Morbidity/
- 7
- exp Mortality/
- 8
- exp Wounds/ and injuries/
- 9
- exp Death/
- 10
- exp Hospitalization/
- 11
- exp Patient admission/
- 12
- exp Patient readmission/
- 13
- exp Length of stay/
- 14
- (Consequence* or impact* or outcome* or implicat* or effect* or morbidit* or injur* or trauma or morbidit* or mortalit* or death* or hospitali* or admission or readmission or length of stay).mp.
- 15
- 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14
- 16
- exp Adult/ or Adult.mp.
- 17
- exp India/
- 18
- (India* or Bharat* or Hindustan*).mp.
- 19
- 17 or 18
- 20
- 5 and 14 and 16 and 19
- 1
- exp falling/
- 2
- (Accidental fall* or slip* or trip* or stumble* or fell).mp.
- 3
- exp gait/
- 4
- (Gait or balance).mp.
- 5
- 1 or 2 or 3 or 4
- 6
- exp morbidity/
- 7
- exp mortality/
- 8
- exp wound/
- 9
- exp injury/
- 10
- exp Death/
- 11
- exp Hospitalization/
- 12
- exp Patient admission/
- 13
- exp Patient readmission/
- 14
- exp Length of stay/
- 15
- (Consequence* or impact* or outcome* or implicat* or effect* or morbidit* or injur* or trauma or morbidit* or mortalit* or death* or hospitali* or admission or readmission or length of stay).mp.
- 16
- 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15
- 17
- exp Adult/ or Adult.mp.
- 18
- exp India/
- 19
- (India* or Bharat* or Hindustan*).mp.
- 20
- 18 or 19
- 21
- 5 and 16 and 17 and 20
- 1
- exp Falls/
- 2
- (fall* or fell or slip* or trip* or stumble*).mp.
- 3
- exp Gait/
- 4
- (Balance or gait).mp.
- 5
- 1 or 2 or 3 or 4
- 6
- exp Morbidity/
- 7
- (Death and dying).mp.
- 8
- exp Wounds/ and injuries/
- 9
- Death.mp.
- 10
- Patient admission.mp.
- 11
- Patient readmission.mp.
- 12
- exp Length of stay/
- 13
- (Consequence* or impact* or outcome* or implicat* or effect* or morbidit* or injur* or trauma or morbidit* or mortalit* or death* or hospitali* or admission or readmission or length of stay).mp.
- 14
- 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13
- 15
- exp Adult/ or Adult.mp.
- 16
- (India* or Bharat* or Hindustan*).mp.
- 17
- 5 and 14 and 15 and 16
- S1
- (MH “Accidental falls”) OR “fall”
- S2
- “Slip* or trip* or stumble* or fell”
- S3
- (MH “Outcomes (health care)”) OR “consequence or effect or outcome or impact”
- S4
- (MH “India”) OR “India*”
- S5
- S1 OR S2
- S6
- S3 AND S4 AND S5
Appendix B. Excluded Studies Following Full-Text Screening
| Study | Reason for Exclusion |
| Subhashraj K, Ravindran C. Maxillofacial intervention in trauma patients aged 60 years and older. Indian Journal of Dental Research. 2008;19(2):109–11. | Ineligible condition |
| Ahuja K, Sen S, Dhanwal D. Risk factors and epidemiological profile of hip fractures in Indian population: a case-control study. Osteoporosis Sarcopenia. 2017;3(3):138–48. | Ineligible condition |
| Lalwani S, Mathur P, Kumar M, et al. Profile of fatal geriatric trauma at a level 1 trauma centre of India. Journal of Patient Safety and Infection Control. 2018;6(2):51–3. | Ineligible condition |
| Abhilash KPP, Tephilah R, Pradeeptha S, et al. Injury patterns and outcomes of trauma in the geriatric population presenting to the emergency department in a tertiary care hospital of south India. Journal of Emergencies, Trauma, and Shock. 2019;12(3):198–202. | Ineligible condition |
| Prinja S, Jagnoor J, Sharma D, et al. Out-of-pocket expenditure and catastrophic health expenditure for hospitalization due to injuries in public sector hospitals in north India. PLoS One. 2019;14(11): e0224721. | Ineligible condition |
| Lahiri A, Jha SS, Chakraborty A. Elders suffering recurrent injurious falls: causal analysis from a rural tribal community in the eastern part of India. Rural Remote Health. 2020;20(4):6042. | Ineligible condition |
| Singh JK, Lateef M, Khan MA, et al. Clinical study of maxillofacial trauma in Kashmir. Indian Journal of Otolaryngology and Head and Neck Surgery. 2005;57(1):24–7. | Ineligible population |
| Dhingra N, Yunus Mhod, Sinha SN, et al. Trauma patients in an Indian hospital. Journal of the Royal Society of Health. 1990;110(2):67–9. | Ineligible population |
| Kohli A, Banerjee KK. Pattern of injuries in fatal falls from buildings. Medicine, Science and the Law. 2006;46(4):335–41. | Ineligible population |
| Venkatesh VT, Kumar MV, Jagannatha SR, et al. Pattern of skeletal injuries in cases of falls from a height. Medicine, Science and the Law. 2007;47(4):330–4. | Ineligible population |
| Bither S, Mahindra U, Halli R, et al. Incidence and pattern of mandibular fractures in rural population: a review of 324 patients at a tertiary hospital in Loni, Maharashtra, India. Dental Traumatology. 2008;24(4):468–70. | Ineligible population |
| Behera C, Rautji R, Dogra TD. Patterns of injury seen in deaths from accidental falls down a staircase: a study from south Delhi. Medicine, Science and the Law. 2009;49(2):127–31. | Ineligible population |
| Sachdeva S, Menon S. Magnitude of unintentional injuries: record-based hospital study. Indian Pediatrics. 2009;46(5):439. | Ineligible population |
| Gosavi SV, Deshmukh PR. Epidemiology of injuries in rural Wardha, central India. Medical Journal Armed Forces India. 2014;70(4):380–2. | Ineligible population |
| Lalwani S, Singh V, Trikha V, et al. Mortality profile of patients with traumatic spinal injuries at a level I trauma care centre in India. Indian Journal of Medical Research. 2014;140(1):40–5. | Ineligible population |
| Mathur N, Jain S, Kumar N, et al. Spinal cord injury: scenario in an Indian state. Spinal Cord. 2015;53(5):349–52. | Ineligible population |
| Ghiya MN, Murty S, Shetty N, et al. A descriptive study of hand injuries presenting to the adult emergency department of a tertiary care center in urban India. Journal of Emergencies, Trauma and Shock. 2017;10(1):19–25. | Ineligible population |
| Shreedhara K, Gouda C, Sidramappa. A study on pattern of injuries in fatal cases of fall from height in the rural areas of Mandya district. Medico-Legal Update. 2018;18(2):151–4. | Ineligible population |
| Das B. Prevalence of work-related occupational injuries and its risk factors among brickfield workers in West Bengal, India. International Journal of Industrial Ergonomics. 2020;80:103052. | Ineligible population |
| Jagnoor J, Suraweera W, Keay L, et al. Childhood and adult mortality from unintentional falls in India. Bulletin of the World Health Organization. 2011;89(10):733–40. | Ineligible study design |
| Ahuja R, Singh K, Gani R, et al. Fatal trauma: death analysis from September 2011 to December 2013, at Fortis hospital, Noida, India. International Journal of Emergency Medicine. 2015;8(1). | Ineligible study design |
| Patel JC. Falls in elderly. Indian Journal of Medical Sciences. 2000;54(8):350–2. | Full-text not available |
| Sharma R, All L, Ubbot M. The epidemiology of fractures and dislocations at district hospital Kathua (Jammu and Kashmir). JK Practitioner. 2007; 14:114–7. | Full-text not available |
| Thirunaaukarasu D, Srikanth S, Susiganeshkumar E, et al. Unintentional injuries: burden and risk factors in rural areas of Puducherry. Indian Journal of Medical specialities. 2013;4(2):229–33. | Full-text not available |
| Singhal D. A study of head injury and its pattern in Surat region: a prospective study. International Journal of Medical Toxicology and Legal Medicine. 2019;22(1):53–5. | Full-text not available |
| Cardona M, Joshi R, Ivers RQ, et al. The burden of fatal and non-fatal injury in rural India. Injury Prevention. 2008;14(4):232–7. | Denominator data not extractable |
| Dandona R, Kumar GA, Ivers R, et al. Characteristics of non-fatal fall injuries in rural India. Injury Prevention. 2010;16(3):166. | Denominator data not extractable |
| Gulati D, Aggarwal AN, Kumar S, et al. Skeletal injuries following unintentional fall from height. Ulusal travma ve Acil Cerrahi Dergisi. 2012;18)2):141–6. | Denominator data not extractable |
| Jagnoor J, Keay L, Ganguli A, et al. Fall related injuries: a retrospective medical review study in North India. Injury. 2012;43(12):1996–2000. | Denominator data not extractable |
| Vidua R. How much safe are our elders in south Delhi. Journal of Forensic Medicine and Toxicology. 2012;29:113–6. | Denominator data not extractable |
| Weihsin H, Thadani S, Agrawal M, et al. Causes and incidence of maxillofacial injuries in India: 12-year retrospective study of 4437 patients in a tertiary hospital in Gujarat. British Journal of Oral and Maxillofacial Surgery. 2014;52(8):693–6. | Denominator data not extractable |
| Dash SK, Panigrahi R, Palo N, et al. Fragility hip fractures in elderly patients in Bhubaneswar, India (2012–2014): a prospective multicenter study of 1031 elderly patients. Geriatric Orthopaedic Surgery and Rehabilitation. 2015;6(1):11–5. | Denominator data not extractable |
| Joseph A, Bagavandas M. Non-fatal home injuries among the elderly in Tamil Nadu, India. Indian Journal of Community Medicine. 2019;44(1):81–4. | Denominator data not extractable |
| Kulshrestha V, Sood M, Kumar S, et al. Outcomes of fast-track multidisciplinary care of hip fractures in veterans: a geriatric hip fracture program report. Clinics in Orthopedic Surgery. 2019;11(4):388–95. | Denominator data not extractable |
| Naveen Kumar T, Jagannatha SR, Venkatesha VT. Rise in deaths due to fall from height: a 3-year retrospective study. Medico-Legal Update.2019;19(2):113–6. | Denominator data not extractable |
| George J, Sharma V, Farooque K, et al. Factors associated with delayed surgery in elderly hip fractures in India. Archives of Osteoporosis. 2021;16(1):7. | Denominator data not extractable |
References
- International Classification of Diseases. ICD-10 Version: 2019 [Internet]. Available online: https://icd.who.int/browse10/2019/en#/W00-W19 (accessed on 24 March 2023).
- Gibson, M.J.; Andres, R.O.; Kennedy, T.E.; Coppard, L.C. Kellogg International Work Group on the prevention of falls by the elderly. The prevention of falls in later life. Dan. Med. Bull. 1987, 34, 1–24. [Google Scholar]
- Lord, S.R. Pathophysiology of falls, balance and fall prevention. Proc. Physiol. Soc. 2015, 33, SA06. Available online: https://www.physoc.org/abstracts/pathophysiology-of-falls-balance-and-fall-prevention/ (accessed on 24 March 2023).
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Milat, A.J.; Watson, W.L.; Monger, C.; Barr, M.; Giffin, M.; Reid, M. Prevalence, circumstances and consequences of falls among community-dwelling older people: Results of the 2009 NSW falls prevention baseline survey. N. S. W. Public Health Bull. 2011, 22, 43–48. [Google Scholar] [CrossRef]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, M.S.; Singh, V.; Chatterjee, P.; Dwivedi, S.N.; Dey, A.B. Prevalence and predictors of falls in a health-seeking older population: An outpatient-based study. Aging Med. (Milton) 2020, 3, 25–31. [Google Scholar] [CrossRef]
- Kaur, R.; Kalaivani, M.; Goel, A.D.; Goswami, A.K.; Nongkynrih, B.; Gupta, S.K. Burden of falls among elderly persons in India: A systematic review and meta-analysis. Natl. Med. J. India 2020, 33, 195–200. [Google Scholar] [CrossRef]
- Joseph, A.; Kumar, D.; Bagavandas, M. A review of epidemiology of fall among elderly in India. Indian J. Community Med. 2019, 44, 166–168. [Google Scholar]
- Biswas, I.; Adebusoye, B.; Chattopadhyay, K. Risk factors for falls among older adults in India: A systematic review and meta-analysis. Health Sci. Rep. 2022, 5, e637. [Google Scholar] [CrossRef]
- Joshi, K.; Kumar, R.; Avasthi, A. Morbidity profile and its relationship with disability and psychological distress among elderly people in northern India. Int. J. Epidemiol. 2003, 32, 978–987. [Google Scholar] [CrossRef]
- Johnson, S.J. Frequency and nature of falls among older women in India. Asia Pac. J. Public Health 2006, 18, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Suryanarayana, S.P.; Rajaram, D. Circumstances and consequences of falls in community-living elderly in north Bangalore, Karnataka. J. Krishna Inst. Med. Sci. Univ. 2015, 4, 27–35. [Google Scholar]
- Tripathy, N.K.; Jagnoor, J.; Patro, B.K.; Dhillon, M.S.; Kumar, R. Epidemiology of falls among older adults: A cross sectional study from Chandigarh, India. Injury 2015, 46, 1801–1805. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Chapter 5: Systematic reviews of prevalence and incidence. In: Aromataris E, Munn Z (Editors). JBI Manual for Evidence Synthesis. JBI 2020. Available online: https://doi.org/10.46658/JBIMES-20-06 (accessed on 12 April 2023).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. Available online: http://www.prisma-statement.org/ (accessed on 12 April 2023). [CrossRef]
- Government of India. Ministry of Statistics and Programme Implementation. National Statistics Office. Social Statistics Division. Available online: www.mospi.gov.in (accessed on 17 March 2023).
- United Nations High Commissioner for Refugees. Older Persons. Available online: https://emergency.unhcr.org/entry/43935/older-persons (accessed on 17 March 2023).
- Endnote X9.3 Clarivate Analytics, PA, USA [Internet]. Endnote. 2017. Available online: http://endnote.com/ (accessed on 26 November 2020).
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid.-Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Stata Statistical Software: Release 16; [Internet]; StataCorp LLC: College Station, TX, USA, 2017; Available online: https://www.stata.com/company/ (accessed on 26 November 2020).
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef]
- Migliavaca, C.B.; Stein, C.; Colpani, V.; Barker, T.H.; Ziegelmann, P.K.; Munn, Z.; Falavigna, M.; Prevalence Estimates Reviews—Systematic Review Methodology Group (PERSyst). Meta-analysis of prevalence: I2 statistic and how to deal with heterogeneity. Res. Synth. Methods 2022, 13, 363–367. [Google Scholar] [CrossRef]
- Sirohi, A.; Kaur, R.; Goswami, A.K.; Mani, K.; Nongkynrih, B.; Gupta, S.K. A study of falls among elderly persons in a rural area of Haryana. Indian J. Public Health 2017, 61, 99–104. [Google Scholar]
- Padmavathy, L.; Dongre, A.R. Characteristics of fall among older people in rural Puducherry. Indian J. Community Med. 2018, 43, 327–328. [Google Scholar]
- Pathania, A.; Haldar, P.; Kant, S.; Gupta, S.; Pandav, C.; Bachani, D. Prevalence of fall, and determinants of repeat incidents of fall in older persons living in old age homes in the National Capital Territory of Delhi, India. Natl. Med. J. India 2018, 31, 329–333. [Google Scholar]
- Kaur, M.; Kaur, J.; Devgun, P.; Sharma, S. Post fall health consequences among elderly. IOSR J. Nurs. Health Sci. (IOSR-JNHS) 2019, 7, 34–37. [Google Scholar]
- Facts about Falls [Internet]. Center for Disease Control and Prevention. Center for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/falls/facts.html (accessed on 20 November 2022).
- Schwendimann, R.; Bühler, H.; De Geest, S.; Milisen, K. Falls and consequent injuries in hospitalized patients: Effects of an interdisciplinary falls prevention program. BMC Health Serv. Res. 2006, 6, 69. [Google Scholar] [CrossRef]
- Aranda-Gallardo, M.; Morales-Asencio, J.M.; Enriquez de Luna-Rodriguez, M.; Vazquez-Blanco, M.J.; Morilla-Herrera, J.C.; Rivas-Ruiz, F.; Toribio-Montero, J.C.; Canca-Sanchez, J.C. Characteristics, consequences and prevention of falls in institutionalised older adults in the province of Malaga (Spain): A prospective, cohort, multicentre study. BMJ Open 2018, 8, e020039. [Google Scholar] [CrossRef]
- Singh, A.; Tetreault, L.; Kalsi-Ryan, S.; Nouri, A.; Fehlings, M.G. Global prevalence and incidence of traumatic spinal cord injury. Clin. Epidemiol. 2014, 6, 309–331. [Google Scholar]
- Dsouza, S.; Rajashekar, B.; Dsouza, H.; Kumar, K.B. Falls in Indian older adults: A barrier to active ageing. Asian J. Gerontol. 2014, 9, 33–40. [Google Scholar]
- Krishnaswamy, B.; Gnanasambandam, U. Falls in Older People. National/Regional Review, India. Available online: https://reliva.in/wp-content/uploads/2019/11/SEARO.pdf (accessed on 20 November 2022).
- Vaapio, S.S.; Salminen, M.J.; Ojanlatva, A.; Kivelä, S.-L. Quality of life as an outcome of fall prevention interventions among the aged: A systematic review. Eur. J. Public Health 2009, 19, 7–15. [Google Scholar] [CrossRef]
- Pfortmueller, C.; Lindner, G.; Exadaktylos, A.K. Reducing fall risk in the elderly: Risk factors and fall prevention: A systematic review. Minerva Med. 2014, 105, 275–281. [Google Scholar]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of interventions for preventing falls in older adults: A systematic review and meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef]
- NICE. Falls in Older People: Assessing Risk and Prevention of Falls. NICE Clinical Guideline 161 [CG161]. 2013. Available online: https://www.nice.org.uk/Guidance/CG161 (accessed on 28 May 2021).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Study Design | Study Period | Indian State | Study Setting | Rural/Urban | Sex | Definition of Falls | Data Collection on Falls | Number of Falls | Data Collection on Health Consequences of Falls | Health Consequences of Falls and Numbers |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Joshi, 2003 [11] | Cross- sectional | 1999–2000 | Haryana | Community | Rural and urban | Male and female | Ending up on the floor or ground unintentionally | Self-reported by family members, medical records, physical Examination | 103 | Self-reported by participants | Fractures = 21 Other fall-related injuries = 82 |
| Johnson, 2006 [12] | Cross- sectional | 2002 | Kerala | Community and institutionalized long-term care (LTC) facilities (nursing homes) | Urban | Female | Not defined | Self-reported by participants | 73 | Self-reported by participants | Injuries sustained: pain = 25 fractures = 15 minor (cuts, bruises) = 11 Area of injury: head injury = 7 back/neck injury = 7 chest injury = 2 hand/arm injury = 9 hip injury = 3 leg/knee/ankle injury = 17 |
| Patil, 2015 [13] | Cross- sectional | 2010–2011 | Karnataka | Community | Urban | Male and female | Inadvertently coming to rest on the ground, floor, or other lower level excluding intentional change in position to rest on furniture, wall, or other objects | Self-reported by participants and physical Examination | 124 | Self-reported by participants and medical records | Fall-related injuries = 101 Head/back/face injuries = 19 Upper limb injuries = 26 Lower limb injuries = 56 Bruises/internal injuries = 49 Sprains/grazes/cuts/others = 38 Fractures = 14 |
| Tripathy, 2015 [14] | Cross- sectional | 2011–2012 | Punjab | Community | Urban | Male and female | Not defined | Self-reported by participants and physical examination | 92 | Self-reported by participants and physical examination | Fall-related injury = 62 Head/neck injury = 9 Trunk injury = 4 Upper extremity injury = 18 Spine injury = 8 Lower extremity injury = 23 Cut/bruise/abrasion = 33 Dislocation/sprain = 16 Fracture = 5 Loss of consciousness after falls = 8 Disability = 13 Hospital admission = 7 |
| Sirohi, 2017 [24] | Cross- sectional | 2015 | Haryana | Community | Rural | Male and female | An event that results in a person coming to rest inadvertently on the ground or floor or other lower level | Self-reported by participants and medical records | 167 | Self-reported by participants | Head injuries = 10 Upper extremity injuries = 35 Spine injuries = 17 Pelvis injuries = 25 Lower extremity injuries = 70 Internal injuries = 1 Cut/laceration/abrasion/bruise = 91 Joint dislocation/sprain = 11 Fractures = 10 Loss of consciousness after fall = 18 Disability due to fall = 14 |
| Padmavathy, 2018 [25] | Cross- sectional | 2017 | Puducherry | Community | Rural | Male and female | Not defined | Medical records and self-reported by carers | 156 | Medical records and self-reported by carers | Head and neck and upper extremity injury = 29 Lower extremity injury = 81 Contusion = 95 |
| Pathania, 2018 [26] | Cross- sectional | 2015 | Delhi | Residential care (old age home) | Urban | Male and female | An event which resulted in a person coming to rest inadvertently on the ground or floor or other lower level | Self-reported by participants | 55 | Self-reported by participants | Fall-related injuries = 30 Head injury = 7 Neck injury = 1 Upper limb injury = 12 Spine injury = 2 Lower limb injury = 8 Disability after fall = 7 |
| Kaur, 2019 [27] | Cross- sectional | 2016–2017 | Punjab | Community | Rural and urban | Male and female | Not defined | Self-reported by participants | 240 | Self-reported by participants | Head injury = 9 Internal injuries = 12 Bruises/cuts = 63 Dislocation of joints = 11 Sprains = 39 Fractures = 37 Loss of consciousness after fall = 3 Post-fall syndrome = 6 Hospitalization = 61 |
| Author and Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Total % of “Yes” to Critical Appraisal Questions |
|---|---|---|---|---|---|---|---|---|---|---|
| Joshi, 2003 [11] | Y | Y | N | Y | Y | Y | U | Y | Y | 78 |
| Johnson, 2006 [12] | Y | U | U | Y | Y | U | Y | Y | U | 56 |
| Patil, 2015 [13] | Y | Y | N | Y | Y | U | U | Y | Y | 67 |
| Tripathy, 2015 [14] | Y | Y | N | Y | Y | U | Y | Y | Y | 78 |
| Sirohi, 2017 [24] | Y | Y | N | Y | Y | U | Y | Y | Y | 78 |
| Padmavathy, 2018 [25] | Y | U | U | Y | Y | U | Y | Y | U | 56 |
| Pathania, 2018 [26] | Y | Y | N | Y | Y | U | U | Y | Y | 67 |
| Kaur, 2019 [27] | Y | Y | N | Y | Y | U | U | Y | U | 56 |
| Total % of “yes” to each critical appraisal question | 100 | 75 | 0 | 100 | 100 | 13 | 50 | 100 | 63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biswas, I.; Adebusoye, B.; Chattopadhyay, K. Health Consequences of Falls among Older Adults in India: A Systematic Review and Meta-Analysis. Geriatrics 2023, 8, 43. https://doi.org/10.3390/geriatrics8020043
Biswas I, Adebusoye B, Chattopadhyay K. Health Consequences of Falls among Older Adults in India: A Systematic Review and Meta-Analysis. Geriatrics. 2023; 8(2):43. https://doi.org/10.3390/geriatrics8020043
Chicago/Turabian StyleBiswas, Isha, Busola Adebusoye, and Kaushik Chattopadhyay. 2023. "Health Consequences of Falls among Older Adults in India: A Systematic Review and Meta-Analysis" Geriatrics 8, no. 2: 43. https://doi.org/10.3390/geriatrics8020043
APA StyleBiswas, I., Adebusoye, B., & Chattopadhyay, K. (2023). Health Consequences of Falls among Older Adults in India: A Systematic Review and Meta-Analysis. Geriatrics, 8(2), 43. https://doi.org/10.3390/geriatrics8020043