



A Novel Approach to Assess Balneotherapy Effects on Musculoskeletal Diseases—An Open Interventional Trial Combining Physiological Indicators, Biomarkers, and Patients’ Health Perception

 ,
,  , ,
, ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
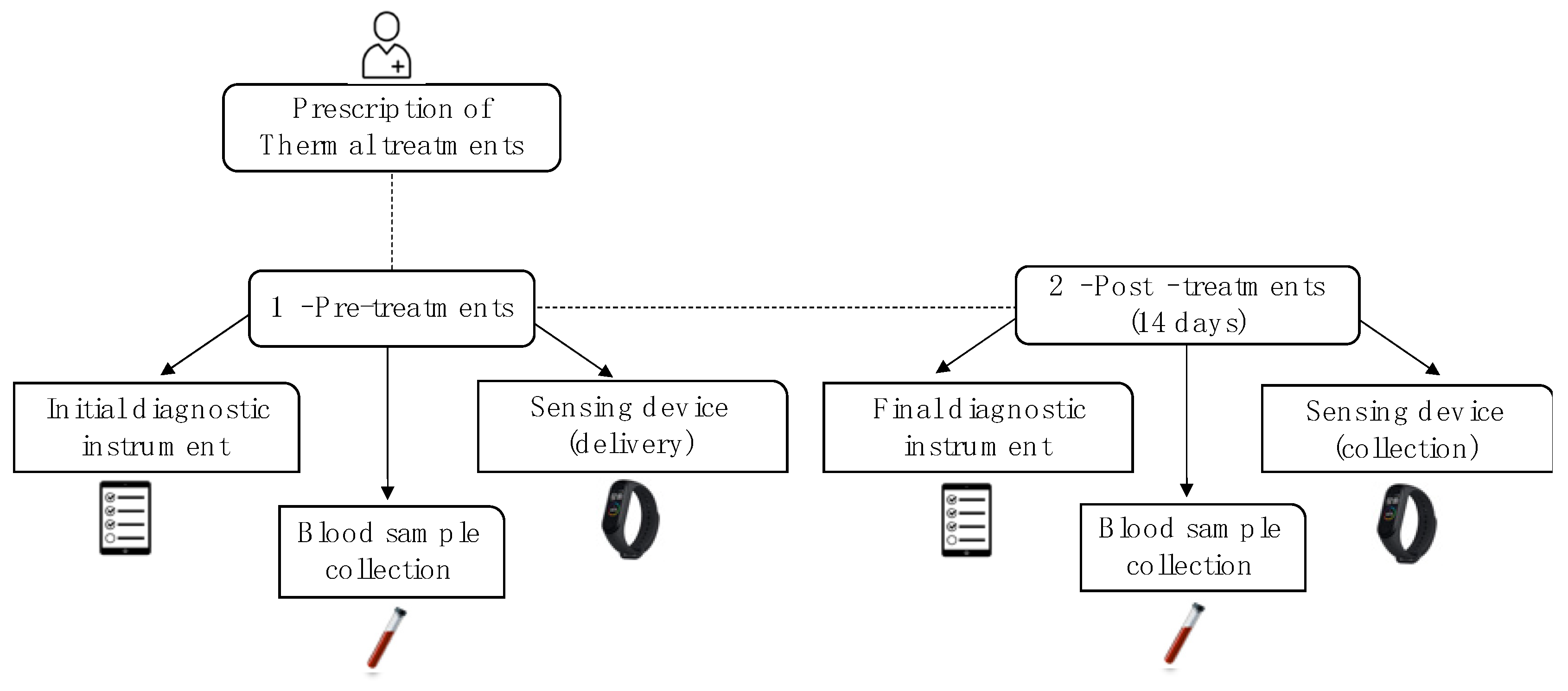
2.1. Study Design, Patients, and Sample Collection
2.2. Balneotherapy

{kind=link}
{kind=link}
{kind=link}
| Physicochemical Properties | |
|---|---|
| Conductivity (to 20 °C) | 2320 µS/cm |
| pH (to 20 °C) | 6.9 |
| Dry residue to 180 °C | 1744 mg/L |
| Hardness (to p.p. 105 CaCO3) | 7.4 mg/L CaCO3 |
| Alkalinity (mL/L de HCl 0.1 M) | 288.9 mL/L HCl 0.1 M |
| Anions | mg/L |
| HCO3− | 1762 |
| Cl− | 36 |
| SO42− | 21 |
| F− | 8.3 |
| PO43− | 0.22 |
| Cations | mg/L |
| Na+ | 623 |
| K+ | 65 |
| Ca2+ | 22 |
| Mg2+ | 5.5 |
| Fe2+ | 0.17 |
| Mineral concentration (mg/L) | 2625 |
| CO2 dissolved (mg/L) | 600 |
2.3. Instruments
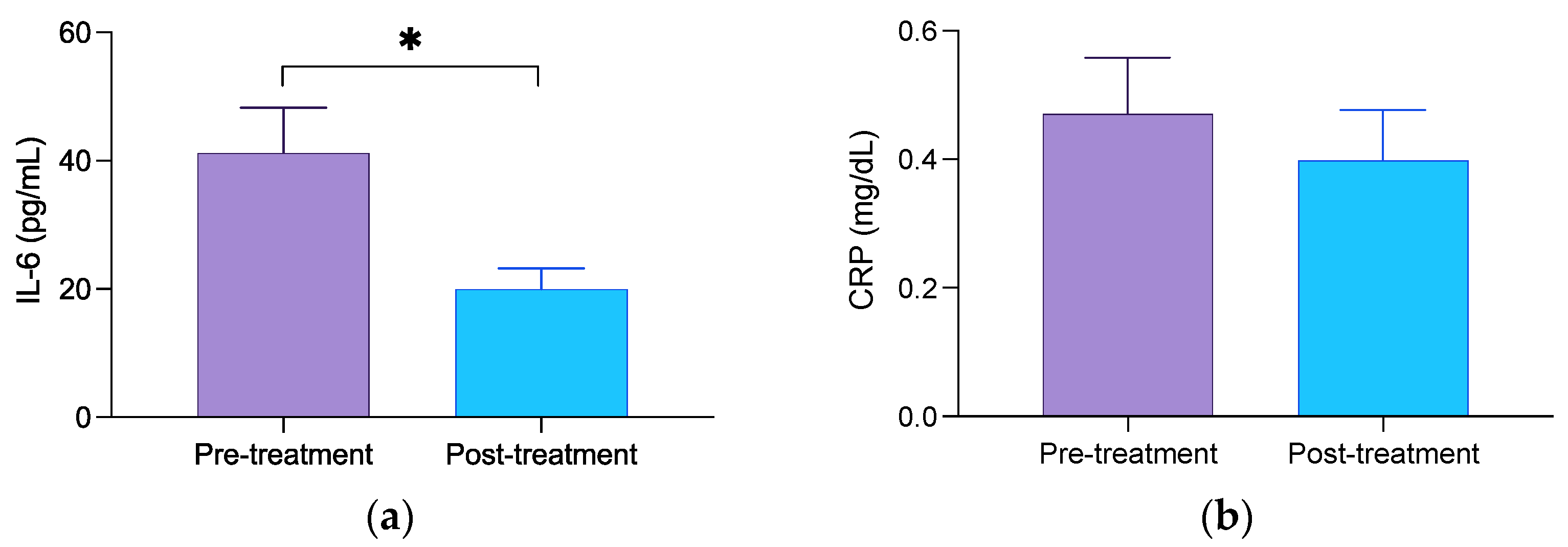
2.4. Determination of Circulating Concentration of Inflammatory Biomarkers
2.5. Wearable Sensing Device
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef]
- Williams, A.; Kamper, S.J.; Wiggers, J.H.; O’brien, K.M.; Lee, H.; Wolfenden, L.; Yoong, S.L.; Robson, E.; McAuley, J.H.; Hartvigsen, J.; et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. 2018, 16, 167. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Bernetti, A.; Mangone, M.; Alviti, F.; Paolucci, T.; Attanasi, C.; Murgia, M.; Di Sante, L.; Agostini, F.; Vitale, M.; Paoloni, M. Spa therapy and rehabilitation of musculoskeletal pathologies: A proposal for best practice in Italy. Int. J. Biometeorol. 2020, 64, 905–914. [Google Scholar] [CrossRef]
- Kamioka, H.; Nobuoka, S.; Iiyama, J. Overview of Systematic Reviews with Meta-Analysis Based on Randomized Controlled Trials of Balneotherapy and Spa Therapy from 2000 to 2019. Int. J. Gen. Med. 2020, 13, 429–442. [Google Scholar] [CrossRef]
- Cantista, P.; Maraver, F. Balneotherapy for knee osteoarthritis in S. Jorge: A randomized controlled trial. Int. J. Biometeorol. 2020, 64, 1027–1038. [Google Scholar] [CrossRef]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: Evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef]
- Gutenbrunner, C.; Bender, T.; Cantista, P.; Karagülle, Z. A proposal for a worldwide definition of health resort medicine, balneology, medical hydrology and climatology. Int. J. Biometeorol. 2010, 54, 495–507. [Google Scholar] [CrossRef]
- Carbajo, J.M.; Maraver, F. Sulphurous Mineral Waters: New Applications for Health. Evid. Based Complement. Alternat Med. 2017, 2017, 8034084. [Google Scholar] [CrossRef]
- Galvez, I.; Torres-Piles, S.; Ortega-Rincon, E. Balneotherapy, Immune System, and Stress Response: A Hormetic Strategy? Int. J. Mol. Sci. 2018, 19, 1687. [Google Scholar] [CrossRef]
- Karaarslan, F.; Ozkuk, K.; Karabulut, S.S.; Bekpinar, S.; Karagulle, M.Z.; Erdogan, N. How does spa treatment affect cardiovascular function and vascular endothelium in patients with generalized osteoarthritis? A pilot study through plasma asymmetric di-methyl arginine (ADMA) and L-arginine/ADMA ratio. Int. J. Biometeorol. 2018, 62, 833–842. [Google Scholar] [CrossRef]
- Ortega, E.; Gálvez, I.; Hinchado, M.D.; Guerrero, J.; Martín-Cordero, L.; Torres-Piles, S. Anti-inflammatory effect as a mechanism of effectiveness underlying the clinical benefits of pelotherapy in osteoarthritis patients: Regulation of the altered inflammatory and stress feedback response. Int. J. Biometeorol. 2017, 61, 1777–1785. [Google Scholar] [CrossRef]
- Vela-Anero, Á.; Hermida-Gómez, T.; Gato-Calvo, L.; Vaamonde-García, C.; Díaz-Prado, S.; Meijide-Faílde, R.; Blanco, F.; Burguera, E. Long-term effects of hydrogen sulfide on the anabolic-catabolic balance of articular cartilage in vitro. Nitric Oxide 2017, 70, 42–50. [Google Scholar] [CrossRef]
- Harzy, T.; Ghani, N.; Akasbi, N.; Bono, W.; Nejjari, C. Short- and long-term therapeutic effects of thermal mineral waters in knee osteoarthritis: A systematic review of randomized controlled trials. Clin. Rheumatol. 2009, 28, 501–507. [Google Scholar] [CrossRef]
- Santos, I.; Cantista, P.; Vasconcelos, C. Balneotherapy in rheumatoid arthritis-a systematic review. Int. J. Biometeorol. 2016, 60, 1287–1301. [Google Scholar] [CrossRef]
- Özkurt, S.; Dönmez, A.; Karagülle, M.Z.; Uzunoglu, E.; Turan, M.; Erdoğan, N. Balneotherapy in fibromyalgia: A single blind randomized controlled clinical study. Rheumatol. Int. 2012, 32, 1949–1954. [Google Scholar] [CrossRef]
- Balogh, Z.; Ördögh, J.; Gász, A.; Német, L.; Bender, T. Effectiveness of balneotherapy in chronic low back pain—A randomized single-blind controlled follow-up study. Forsch. Komplement. Klass. Nat. 2005, 12, 196–201. [Google Scholar] [CrossRef]
- Pittler, M.H.; Karagülle, M.Z.; Ernst, E. Spa therapy and balneotherapy for treating low back pain: Meta-analysis of randomized trials. Rheumatology 2006, 45, 880–884. [Google Scholar] [CrossRef]
- Cheleschi, S.; Tenti, S.; Seccafico, I.; Gálvez, I.; Fioravanti, A.; Ortega, E. Balneotherapy year in review 2021: Focus on the mechanisms of action of balneotherapy in rheumatic diseases. Environ. Sci. Pollut. Res. Int. 2022, 29, 8054–8073. [Google Scholar] [CrossRef]
- Giannitti, C.; De Palma, A.; Pascarelli, N.A.; Cheleschi, S.; Giordano, N.; Galeazzi, M.; Fioravanti, A. Can balneotherapy modify microRNA expression levels in osteoarthritis? A comparative study in patients with knee osteoarthritis. Int. J. Biometeorol. 2017, 61, 2153–2158. [Google Scholar] [CrossRef]
- Galvez, I.; Torres-Piles, S.; Ortega, E. Innate/inflammatory bioregulation and clinical effectiveness of whole-body hyperthermia (balneotherapy) in elderly patients with osteoarthritis. Int. J. Hyperth. 2018, 35, 340–347. [Google Scholar] [CrossRef]
- Antonelli, M.; Donelli, D.; Fioravanti, A. Effects of balneotherapy and spa therapy on quality of life of patients with knee osteoarthritis: A systematic review and meta-analysis. Rheumatol. Int. 2018, 38, 1807–1824. [Google Scholar] [CrossRef]
- Castelli, L.; Galasso, L.; Mulè, A.; Ciorciari, A.; Fornasini, F.; Montaruli, A.; Roveda, E.; Esposito, F. Sleep and spa therapies: What is the role of balneotherapy associated with exercise? A systematic review. Front. Physiol. 2022, 13, 964232. [Google Scholar] [CrossRef]
- Bestaş, E.; Dündar, Ü.; Köken, T.; Koca, B.; Yeşil, H. The comparison of effects of balneotherapy, water-based and land-based exercises on disease activity, symptoms, sleep quality, quality of life and serum sclerostin level in patients with ankylosing spondylitis: A prospective, randomized study. Arch. Rheumatol. 2022, 37, 159–168. [Google Scholar] [CrossRef]
- Masiero, S. Thermal rehabilitation and osteoarticular diseases of the elderly. Aging Clin. Exp. Res. 2008, 20, 189–194. [Google Scholar] [CrossRef]
- Batterham, S.I.; Heywood, S.; Keating, J.L. Systematic review and meta-analysis comparing land and aquatic exercise for people with hip or knee arthritis on function, mobility and other health outcomes. BMC Musculoskelet. Disord. 2011, 12, 123. [Google Scholar] [CrossRef]
- (DGEG). Direção Geral de Energia e Geologia-D.G.d.E.e.G. 2023. Available online: https://www.dgeg.gov.pt (accessed on 15 February 2023).
- Chaves, T.D. 2023. Available online: https://www.termasdechaves.com/ (accessed on 15 February 2023).
- Ferreira, P.L.; Antunes, P.; Ferreira, L.; Pereira, L. EQ-5D-5L valuation study for Portugal. Qual. Life Res. 2017, 26, 87. [Google Scholar]
- Ferreira, P.L.; Pereira, L.N.; Antunes, P.; Ferreira, L.N. EQ-5D-5L Portuguese population norms. Eur. J. Health Econ. 2023, 1–10. [Google Scholar] [CrossRef]
- Pereira, M.; Melo, C.; Gameiro, S.; Canavarro, M.C. Estudos psicométricos da versão em Português Europeu do índice de qualidade de vida EUROHIS-QOL-8. Laboratório De Psicol. 2011, 9, 109–123. [Google Scholar] [CrossRef]
- Karagülle, M.; Kardeş, S.; Dişçi, R.; Gürdal, H.; Karagülle, M.Z. Spa therapy for elderly: A retrospective study of 239 older patients with osteoarthritis. Int. J. Biometeorol. 2016, 60, 1481–1491. [Google Scholar] [CrossRef]
- Santos, I.; Cantista, P.; Vasconcelos, C.; Amado, J.C. Balneotherapy and Rheumatoid Arthritis: A Randomized Control Trial. Isr. Med. Assoc. J. 2016, 18, 474–478. [Google Scholar]
- Miller-Mendes, M.; Gomes, A.A.; Ruivo Marques, D.; Clemente, V.; Azevedo, M.H.P. BaSIQS—Basic scale on insomnia complaints and quality of sleep: Reliability, norms, validity, and accuracy studies, based on clinical and community samples. Chronobiol. Int. 2019, 36, 644–656. [Google Scholar] [CrossRef]
- de la Casa Pérez, A.; Latorre Román, P.Á.; Muñoz Jiménez, M.; Lucena Zurita, M.; Laredo Aguilera, J.A.; Párraga Montilla, J.A.; Cabrera Linares, J.C. Is the Xiaomi Mi Band 4 an Accuracy Tool for Measuring Health-Related Parameters in Adults and Older People? An Original Validation Study. Int. J. Environ. Res. Public. Health 2022, 19, 1593. [Google Scholar] [CrossRef]
- Gandek, B.; Sinclair, S.J.; Kosinski, M.; Ware, J.E., Jr. Psychometric evaluation of the SF-36 health survey in Medicare managed care. Health Care Financ. Rev. 2004, 25, 5–25. [Google Scholar]
- McHorney, C.A. Health Status Assessement Methods For Adults: Past Accomplishments and Future Challenges. Annu. Rev. Public Health 1999, 20, 309–335. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep health: Can we define it? Does it matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef]
- Gáti, T.; Tefner, I.K.; Kovács, L.; Hodosi, K.; Bender, T. The effects of the calcium-magnesium-bicarbonate content in thermal mineral water on chronic low back pain: A randomized, controlled follow-up study. Int. J. Biometeorol. 2018, 62, 897–905. [Google Scholar] [CrossRef]
- Pereira, S.; Silva, J.; Marques, C.; Galvão, A.; Alve, M.J. Thermalism as A Determinant of Quality of Life and Sleep: A Novel Approach to The Sector Using SF-36v2 and Pittsburgh Index. Front. Med. Case Rep. 2021, 2, 1–14. [Google Scholar] [CrossRef]
- Ortega, E.; Garcia, J.; Bote, M.E.; Martín-Cordero, L.; Escalante, Y.; Saavedra, J.M.; Northoff, H.; Giraldo, E. Exercise in fibromyalgia and related inflammatory disorders: Known effects and unknown chances. Exerc. Immunol. Rev. 2009, 15, 42–65. [Google Scholar]
- Oyama, J.-I.; Kudo, Y.; Maeda, T.; Node, K.; Makino, N. Hyperthermia by bathing in a hot spring improves cardiovascular functions and reduces the production of inflammatory cytokines in patients with chronic heart failure. Heart Vessel. 2013, 28, 173–178. [Google Scholar] [CrossRef]
- Oláh, M.; Koncz, A.; Fehér, J.; Kálmánczhey, J.; Oláh, C.; Balogh, S.; Nagy, G.; Bender, T. The effect of balneotherapy on C-reactive protein, serum cholesterol, triglyceride, total antioxidant status and HSP-60 levels. Int. J. Biometeorol. 2010, 54, 249–254. [Google Scholar] [CrossRef]
- Oláh, M.; Koncz, Á.; Fehér, J.; Kálmánczhey, J.; Oláh, C.; Nagy, G.; Bender, T. The effect of balneotherapy on antioxidant, inflammatory, and metabolic indices in patients with cardiovascular risk factors (hypertension and obesity)—A randomised, controlled, follow-up study. Contemp. Clin. Trials 2011, 32, 793–801. [Google Scholar] [CrossRef]
- Fioravanti, A.; Adamczyk, P.; Pascarelli, N.A.; Giannitti, C.; Urso, R.; Tołodziecki, M.; Ponikowska, I. Clinical and biochemical effects of a 3-week program of diet combined with spa therapy in obese and diabetic patients: A pilot open study. Int. J. Biometeorol. 2015, 59, 783–789. [Google Scholar] [CrossRef]
- Fioravanti, A.; Karagülle, M.; Bender, T.; Karagülle, M.Z. Balneotherapy in osteoarthritis: Facts, fiction and gaps in knowledge. Eur. J. Integr. Med. 2017, 9, 148–150. [Google Scholar] [CrossRef]
- Rapolienė, L.; Razbadauskas, A.; Mockevičienė, D.; Varžaitytė, L.; Skarbalienė, A. Balneotherapy for musculoskeletal pain: Does the mineral content matter? Int. J. Biometeorol. 2020, 64, 965–979. [Google Scholar] [CrossRef]
- Morer, C.; Roques, C.-F.; Françon, A.; Forestier, R.; Maraver, F. The role of mineral elements and other chemical compounds used in balneology: Data from double-blind randomized clinical trials. Int. J. Biometeorol. 2017, 61, 2159–2173. [Google Scholar] [CrossRef]
- Carbajo, J.M.; Maraver, F. Salt water and skin interactions: New lines of evidence. Int. J. Biometeorol. 2018, 62, 1345–1360. [Google Scholar] [CrossRef]
- de Zambotti, M.; Cellini, N.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Wearable Sleep Technology in Clinical and Research Settings. Med. Sci. Sport. Exerc. 2019, 51, 1538–1557. [Google Scholar] [CrossRef]
- Pino-Ortega, J.; Gomez-Carmona, C.D.; Rico-Gonzalez, M. Accuracy of Xiaomi Mi Band 2.0, 3.0 and 4.0 to measure step count and distance for physical activity and healthcare in adults over 65 years. Gait Posture 2021, 87, 6–10. [Google Scholar] [CrossRef]
- Concheiro-Moscoso, P.; Groba, B.; Martínez-Martínez, F.J.; Miranda-Duro, M.D.C.; Nieto-Riveiro, L.; Pousada, T.; Pereira, J. Use of the Xiaomi Mi Band for sleep monitoring and its influence on the daily life of older people living in a nursing home. Digit. Health 2022, 8, 20552076221121162. [Google Scholar] [CrossRef]



| Total (n = 28) | |
|---|---|
| Age (mean ± SD) | 56.07 ± 9.641 |
| Gender, n (%) | |
| Male | 6 (21.4) |
| Female | 22 (78.6) |
| Marital status, n (%) | |
| Single | 2 (7.2) |
| Married/Consensual union | 22 (78.6) |
| Divorced/widower | 4 (14.2) |
| Education, n (%) | |
| Less than high school | 12 (42.9) |
| High school | 6 (21.4) |
| Graduated | 10 (35.7) |
| Employment status, n (%) | |
| Unemployed | 1 (3.7) |
| Pensioner/Retired | 5 (17.9) |
| Employed | 17 (60.7) |
| Self-employed | 5 (17.9) |
| Private household, n (%) | |
| 1 | 2 (7.1) |
| 2 | 14 (50.0) |
| 3 | 10 (35.8) |
| 4 | 2 (7.1) |
| Instruments | Pre-Treatment | Post-Treatment | Difference (95% CI) | Effect Size (d) | p-Value |
|---|---|---|---|---|---|
| 5Q-5D-5L | 0.780 (±0.236) | 0.917 (±0.114) | 0.137 (0.062, 0.208) | 0.980 | <0.001 |
| EQ-VAS | 67.857 (±17.020) | 81.786 (±10.560) | 13.929 (7.081, 20.775) | 0.789 | <0.001 |
| EUROHIS-QOL | 68.192 (±12.149) | 72.545 (±9.711) | 4.353 (0.842, 7.864) | 0.581 | 0.017 |
| B-IPQ | 37.536 (±6.010) | 28.643 (±4.653) | −8.893 (−13.209, −4.577) | 0.799 | <0.001 |
| BaSIQS | 13.071 (±8.750) | 9.107 (±9.708) | −3.964 (−5.769, −2.159) | 0.852 | <0.001 |
| HAQ-DI | 0.268 (±0.431) | 0.112 (±0.305) | −0.156 (−0.292, −0.021) | 0.747 | 0.019 |
| Week-1 | Week-2 | p-Value | |
|---|---|---|---|
| Number of steps | 9900.541 (±4276.198) | 9498.555 (±4508.623) | 0.399 |
| Heart rate | 72.172 (±6.316) | 71.146 (±6.243) | 0.557 |
| Deep sleep (minutes) | 93.714 (±34.961) | 99.429 (±38.159) | 0.290 |
| Light sleep (minutes) | 352.311 (±56.664) | 362.979 (±53.320) | 0.225 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, J.; Martins, J.; Nicomédio, C.; Gonçalves, C.; Palito, C.; Gonçalves, R.; Fernandes, P.O.; Nunes, A.; Alves, M.J. A Novel Approach to Assess Balneotherapy Effects on Musculoskeletal Diseases—An Open Interventional Trial Combining Physiological Indicators, Biomarkers, and Patients’ Health Perception. Geriatrics 2023, 8, 55. https://doi.org/10.3390/geriatrics8030055
Silva J, Martins J, Nicomédio C, Gonçalves C, Palito C, Gonçalves R, Fernandes PO, Nunes A, Alves MJ. A Novel Approach to Assess Balneotherapy Effects on Musculoskeletal Diseases—An Open Interventional Trial Combining Physiological Indicators, Biomarkers, and Patients’ Health Perception. Geriatrics. 2023; 8(3):55. https://doi.org/10.3390/geriatrics8030055
Chicago/Turabian StyleSilva, Jani, José Martins, Cristina Nicomédio, Catarina Gonçalves, Cátia Palito, Ramiro Gonçalves, Paula Odete Fernandes, Alcina Nunes, and Maria José Alves. 2023. "A Novel Approach to Assess Balneotherapy Effects on Musculoskeletal Diseases—An Open Interventional Trial Combining Physiological Indicators, Biomarkers, and Patients’ Health Perception" Geriatrics 8, no. 3: 55. https://doi.org/10.3390/geriatrics8030055
APA StyleSilva, J., Martins, J., Nicomédio, C., Gonçalves, C., Palito, C., Gonçalves, R., Fernandes, P. O., Nunes, A., & Alves, M. J. (2023). A Novel Approach to Assess Balneotherapy Effects on Musculoskeletal Diseases—An Open Interventional Trial Combining Physiological Indicators, Biomarkers, and Patients’ Health Perception. Geriatrics, 8(3), 55. https://doi.org/10.3390/geriatrics8030055