
Higher Incidence of Cancer Therapy-Related Cardiac Dysfunction in the COVID-19 Era: A Single Cardio-Oncology Center Experience

Abstract
:1. Introduction
2. Methods
3. Results
- 7 patients (4 patients with breast cancer and 3 patients with lymphoma) developed CTRCD earlier during anticancer treatment with anthracyclines after a median period of 1 year; these patients have not performed previous radiotherapy or chemotherapy; their median age was 65 ± 10 years old; 3 patients had arterial hypertension and 1 patient had diabetes as cardiovascular risk factors; only electrocardiogram and focus echocardiogram without GLS measurement were performed before starting chemotherapy in these patients.
- only 1 patient (a 68 years old women with arterial hypertension) with breast cancer and previous chemotherapy with high doses of anthracyclines, had late cardiotoxicity developing CTRCD 2 years after the end of the treatment.
- 1 patient with lymphoma (a 72 year old man), who developed early CTRCD after anthracycline treatment was hospitalized for COVID-19 pneumonia during the second wave; 4 patients who developed CTRCD had asymptomatic COVID-19 infection and were isolated.
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Lisi, D.; Leggio, G.; Vitale, G.; Arrotti, S.; Iacona, R.; Inciardi, R.M.; Nobile, D.; Bonura, F.; Novo, G.; Russo, A.; et al. Chemotherapy cardiotoxicity: Cardioprotective drugs and early identification of cardiac dysfunction. J. Cardiovasc. Med. 2016, 17, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Mercurio, V.; Cuomo, A.; Dessalvi, C.C.; Deidda, M.; Di Lisi, D.; Novo, G.; Manganaro, R.; Zito, C.; Santoro, C.; Ameri, P.; et al. Redox Imbalances in Ageing and Metabolic Alterations: Implications in Cancer and Cardiac Diseases. An Overview from the Working Group of Cardiotoxicity and Cardioprotection of the Italian Society of Cardiology (SIC). Antioxidants 2020, 9, 641. [Google Scholar] [CrossRef]
- Bonura, F.; Di Lisi, D.; Novo, S.; D’Alessandro, N. Timely Recognition of Cardiovascular Toxicity by Anticancer Agents: A Common Objective of the Pharmacologist, Oncologist and Cardiologist. Cardiovasc. Toxicol. 2011, 12, 93–107. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the Eu-ropean Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Munoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R.; et al. 2016 ESC position paper on cancer treatments and cardiovascular toxicity de-veloped under the auspices of the ESC Committee for Practice Guidelines: The Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology. Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Santoro, M.; Mancuso, S.; Accurso, V.; Di Lisi, D.; Novo, G.; Siragusa, S. Cardiovascular Issues in Tyrosine Kinase Inhibitors Treatments for Chronic Myeloid Leu-kemia: A Review. Front. Physiol. 2021, 12, 675811. [Google Scholar] [CrossRef]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Semeraro, G.C.; Cipolla, C.M.; Cardinale, D.M. Role of Cardiac Biomarkers in Cancer Patients. Cancers 2021, 13, 5426. [Google Scholar] [CrossRef]
- Di Lisi, D.; Bonura, F.; Macaione, F.; Peritore, A.; Meschisi, M.; Cuttitta, F.; Novo, G.; Novo, S. Chemotherapy-induced cardiotoxicity: Role of the tissue Doppler in the early diagnosis of left ventricular dysfunction. Anticancer. Drugs 2011, 22, 468–472. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Poulin, F.; Lim, K.D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll. Cardiol. 2014, 63, 2751–2768. [Google Scholar] [CrossRef]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Tan, T.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Assessment of Echocardiography and Biomarkers for the Extended Prediction of Cardiotoxicity in Patients Treated With Anthracyclines, Taxanes, and Trastuzumab. Circ. Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plana, J.C.; Thavendiranathan, P.; Bucciarelli-Ducci, C.; Lancellotti, P. Multi-Modality Imaging in the Assessment of Cardiovascular Toxicity in the Cancer Patient. JACC Cardiovasc. Imaging 2018, 11, 1173–1186. [Google Scholar] [CrossRef] [PubMed]
- Galán-Arriola, C.; Lobo, M.; Vílchez-Tschischke, J.P.; López, G.J.; de Molina-Iracheta, A.; Pérez-Martínez, C.; Agüero, J.; Fernández-Jiménez, R.; Martín-García, A.; Oliver, E.; et al. Serial Magnetic Resonance Imaging to Identify Early Stages of Anthracycline-Induced Cardiotoxicity. J. Am. Coll. Cardiol. 2019, 73, 779–791. [Google Scholar] [CrossRef]
- Di Lisi, D.; Manno, G.; Novo, G. Subclinical Cardiotoxicity: The Emerging Role of Myocardial Work and Other Imaging Techniques. Curr. Probl. Cardiol. 2021, 46, 100818. [Google Scholar] [CrossRef]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [PubMed]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Calvillo-Argüelles, O.; Abdel-Qadir, H.; Ky, B.; Liu, J.E.; Lopez-Mattei, J.C.; Amir, E.; Thavendiranathan, P. Modified Routine Cardiac Imaging Surveillance of Adult Cancer Patients and Survivors During the COVID-19 Pandemic. JACC: CardioOncol. 2020, 2, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Bisceglia, I.; Gabrielli, D.; Canale, M.L.; Gallucci, G.; Parrini, I.; Turazza, F.M.; Russo, G.; Maurea, N.; Quagliariello, V.; Lestuzzi, C.; et al. ANMCO POSITION PAPER: Cardio-oncology in the COVID era (CO and CO). Eur. Heart J. Suppl. 2021, 23, C128–C153. [Google Scholar] [CrossRef]
- Kitahara, S.; Fujino, M.; Honda, S.; Asaumi, Y.; Kataoka, Y.; Otsuka, F.; Nakanishi, M.; Tahara, Y.; Ogata, S.; Onozuka, D.; et al. COVID-19 pandemic is associated with mechanical complications in patients with ST-elevation myocardial infarction. Open Heart 2021, 8, e001497. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef] [PubMed]
- Italia, L.; Tomasoni, D.; Bisegna, S.; Pancaldi, E.; Stretti, L.; Adamo, M.; Metra, M. COVID-19 and Heart Failure: From Epidemiology During the Pandemic to Myocardial Injury, Myocarditis, and Heart Failure Sequelae. Front. Cardiovasc. Med. 2021, 8, 867. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Cenko, E.; Badimon, L.; Bugiardini, R.; Claeys, M.J.; De Luca, G.; de Wit, C.; Derumeaux, G.; Dorobantu, M.; Duncker, D.J.; Eringa, E.C.; et al. Cardiovascular disease and COVID-19: A consensus paper from the ESC Working Group on Coronary Pathophysiology & Microcirculation, ESC Working Group on Thrombosis and the Association for Acute CardioVascular Care (ACVC), in collaboration with the European Heart Rhythm Association (EHRA). Cardiovasc. Res. 2021, 117, 2705–2729. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Before COVID-19 Pandemic (June–August 2019) | During COVID-19 Pandemic (June–August 2021) | p Value | |
|---|---|---|---|
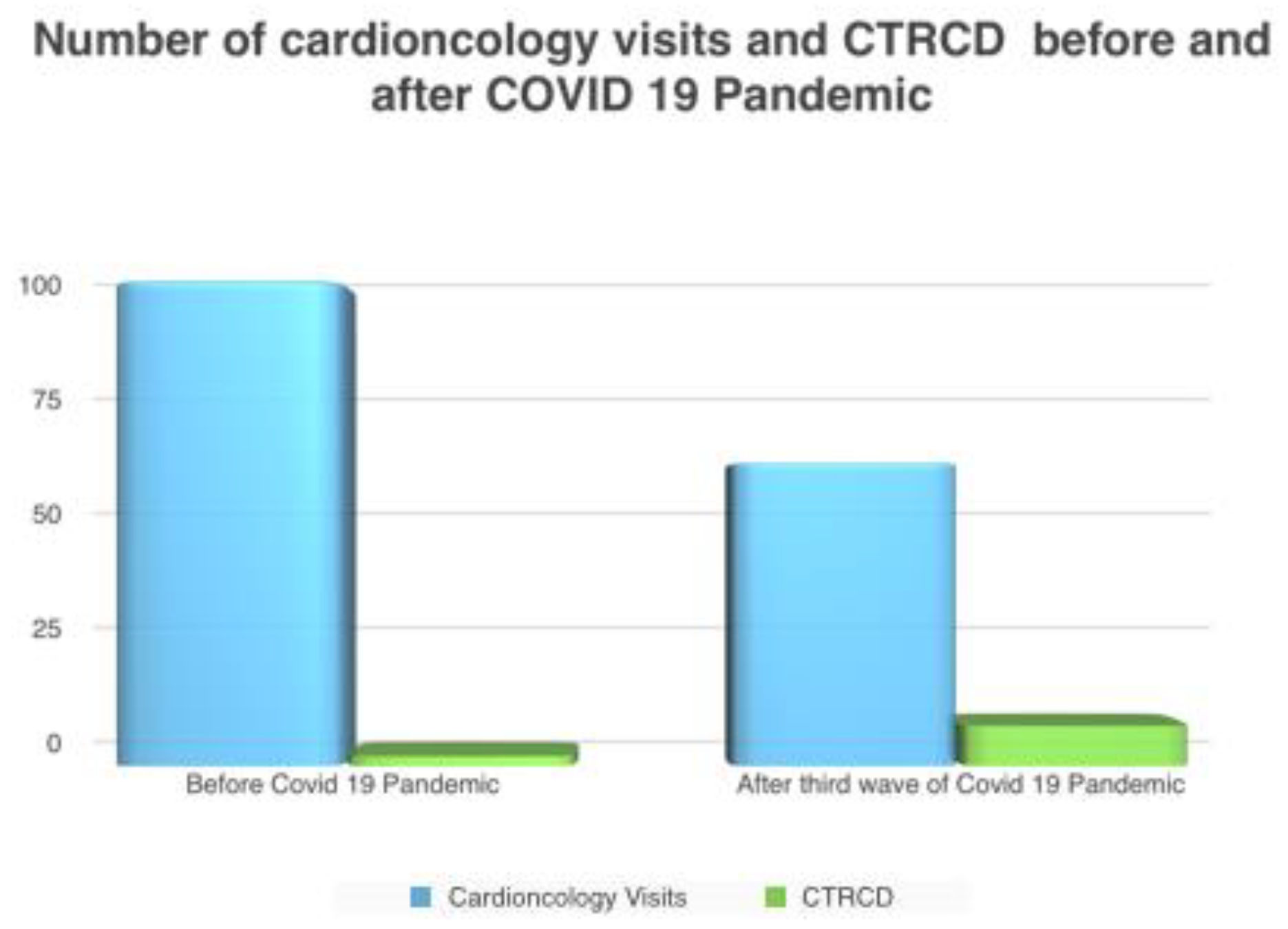
| Outpatient visits with transthoracic echocardiography | 96 | 60 | |
| Median age (years old) | 52 ± 9.4 | 65 ± 5 | p < 0.0001 |
| n. female (%) | 49 (52%) | 39 (66%) | 0.08 |
| BMI, kg/m2 | 24 ± 3.9 | 25 ± 5 | 0.16 |
| Arterial hypertension n° pts (%) | 19 (20%) | 13 (22%) | 0.76 |
| Dyslipidemia n° pts (%) | 24 (25%) | 15 (25%) | 1 |
| Diabetes n° pts (%) | 17 (18%) | 13 (22%) | 0.54 |
| Smoke n° pts (%) | 52 (55%) | 32 (54%) | 0.9 |
| ACEI or ARB treatment | 14 (15%) | 10 (16%) | 0.86 |
| Beta blockers | 5 (5%) | 5 (8%) | 0.45 |
| Statin | 24 (25%) | 15 (25%) | 1 |
| Solid tumor n° (%) | 58 (60%) | 30 (50%) | 0.22 |
| Hematological tumor n° (%) | 38 (40%) | 30 (50%) | 0.22 |
| Previous chemotherapy | 20 (21%) | 15 (25%) | 0.56 |
| Previous radiotherapy | 20 (21%) | 10 (16%) | 0.44 |
| Baseline visit n° pts (%) | 40 (41%) | 30 (50%) | 0.27 |
| Follow-up visits n° pts (%) | 56 (59%) | 30 (50%) | 0.27 |
| Median duration of chemotherapy treatment (months ± DS) | 12 ± 4 | 12 ± 2 | 1 |
| Chemotherapy-related cardiac dysfunction (n° pts) | 2 (2%) | 8 (13%) | 0.0058 |
| Pre COVID-19 | COVID-19 Era | |||
|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | |
| Cardiological evaluation | yes | every 3 months | no | no |
| Electrocardiogram | yes | every 3 months | yes | every 6 months |
| Echocardiogram | Yes with ECG monitoring and GLS Measurement | every 3 months | Yeswithout GLS measurement and without ECG monitoring to reduce exposition time and contact | every 6 months or 12 months if clinical stability |
| Nt pro BNP, Troponin measurement | yes | every 3 months | no | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Lisi, D.; Madaudo, C.; Di Fazio, L.; Gulotta, A.; Triolo, O.F.; Galassi, A.R.; Incorvaia, L.; Russo, A.; Novo, G. Higher Incidence of Cancer Therapy-Related Cardiac Dysfunction in the COVID-19 Era: A Single Cardio-Oncology Center Experience. J. Cardiovasc. Dev. Dis. 2023, 10, 23. https://doi.org/10.3390/jcdd10010023
Di Lisi D, Madaudo C, Di Fazio L, Gulotta A, Triolo OF, Galassi AR, Incorvaia L, Russo A, Novo G. Higher Incidence of Cancer Therapy-Related Cardiac Dysfunction in the COVID-19 Era: A Single Cardio-Oncology Center Experience. Journal of Cardiovascular Development and Disease. 2023; 10(1):23. https://doi.org/10.3390/jcdd10010023
Chicago/Turabian StyleDi Lisi, Daniela, Cristina Madaudo, Luca Di Fazio, Antonino Gulotta, Oreste Fabio Triolo, Alfredo Ruggero Galassi, Lorena Incorvaia, Antonio Russo, and Giuseppina Novo. 2023. "Higher Incidence of Cancer Therapy-Related Cardiac Dysfunction in the COVID-19 Era: A Single Cardio-Oncology Center Experience" Journal of Cardiovascular Development and Disease 10, no. 1: 23. https://doi.org/10.3390/jcdd10010023
APA StyleDi Lisi, D., Madaudo, C., Di Fazio, L., Gulotta, A., Triolo, O. F., Galassi, A. R., Incorvaia, L., Russo, A., & Novo, G. (2023). Higher Incidence of Cancer Therapy-Related Cardiac Dysfunction in the COVID-19 Era: A Single Cardio-Oncology Center Experience. Journal of Cardiovascular Development and Disease, 10(1), 23. https://doi.org/10.3390/jcdd10010023