
The Cost Effectiveness of Coronary CT Angiography and the Effective Utilization of CT-Fractional Flow Reserve in the Diagnosis of Coronary Artery Disease

Abstract
:1. Introduction
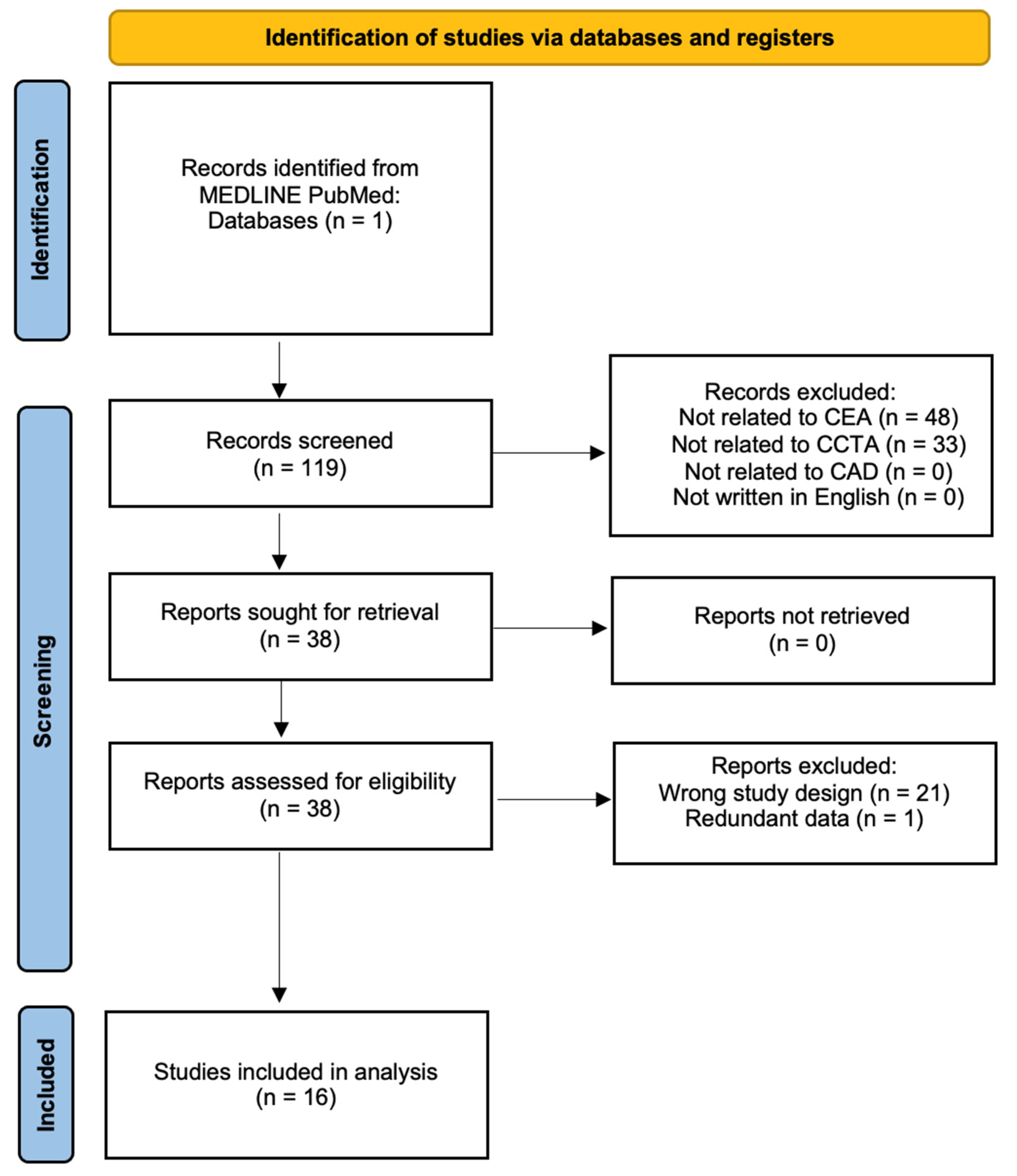
2. Materials and Methods
3. CCTA in Acute Chest Pain

{kind=link}
| Author | N | Study Population | Study Conclusion |
|---|---|---|---|
| Ladapo et al., 2008 [10] | N/A | Hypothetical patients with low-risk chest pain presenting to the ED | CCTA was cost-saving in women (decreased total cost USD 380) and associated with low incremental cost-effectiveness ratio (ICER) in men (USD 6400/QALY). This study concluded that CCTA was modestly more effective than SOC in both sexes (increased in QALYs 0.02). |
| Goehler et al., 2020 [19] | 1000 | Patients enrolled in the “Rule Out Myocardial Infarction/Ischemia Using Computer Assisted Tomography” (ROMICAT) II trial with low-intermediate risk of ACS who presented to the ED with suspicion of ACS | CCTA dominated SOC and ACC/AHA guidelines, and was cost-effective compared to expedited ED discharge (USD 49,428/QALY) |
| Hoffmann et al., 2012 [23] | 1000 | Multicenter trial with patients 40 to 74 years old with suspected ACS without ECG changes | In patients with suspected ACS, utilizing CCTA improved clinical decision making with no decrease in the total cost of care (USD 4289—CCTA group and USD 4060—standard of care, p = 0.65) |
| Litt et al., 2012 [28] | 1370 | Multicenter study with patents over 30 years old with low-to-intermediate risk of possible ACS | In comparison to the standard of care, patients in the CCTA group had reduced hospital length of stay and a higher detection of ACS |
| Goldstein et al., 2011 [29] | 699 | Multicenter randomized clinical trial across 16 EDs with randomized patient allocation suspected of ACS | Utilization of CCTA resulted in 54% reduction in time to diagnosis and 38% lower costs compared to perfusion testing (USD 2137—CCTA vs. USD 3458—MPI) |
4. CCTA in Stable Chest Pain
| Author | N | Study Population | Study Conclusion |
|---|---|---|---|
| Lee et al., 2015 [6] | 1632 | Retrospective cohort study in patients with a pretest probability between 10–90% for ACS | At a one-year follow-up, CCTA was more cost-effective in terms of life quality (0.00221 QALY) and cost (USD 513) compared to SPECT, although SPECT performed better than CCTA in patients with a pretest probability of 30–60% |
| Genders et al., 2013 [35] | 471 | Prospective cohort study in patients with stable chest pain utilizing a Markov simulation model | In patients with a pretest probability below 70%, CCTA was less expensive and more effective (cost savings EUR 444, 0.0035 QALYs gained) in 100% of simulations |
| Dewey and Hamm, 2007 [36] | N/A | Hypothetical patient cohort with a decision tree model | Utilization of CCTA was most cost-effective in patients with pretest probability between 10–50%, with CAG being most cost-effective with pretest probability above 70% |
| Bertoldi et al., 2017 [37] | N/A | Hypothetical patient cohort with a pretest probability between 20% and 70% for ACS | CCTA strategy was most cost-effective (cost-effectiveness ratio of USD 286 per correct diagnosis) |
| Bertoldi et al., 2016 [38] | N/A | Hypothetical patient cohort using the Markov simulation model | CCTA driven strategy was the most cost-effective among low-to-intermediate risk patients (0.3 QALYs gained, ICER USD 3100) * |
| Min et al., 2010 [39] | N/A | Patients with a pretest probability for ACS between 10–80%, base case being a 55–year-old male with a 30% risk of obstructive CAD | Strategies utilizing CCTA prevailed over other strategies with favorable ICERs (CCTA first USD 17,516, CCTA only USD 20,429) * |
5. Diagnostic Accuracy
6. Limitations of CCTA
7. Computed Tomography-Fractional Flow Reserve (CT-FFR)
8. Dual-Energy Computed Tomography (DECT)
9. Artificial Intelligence (AI) and the Cost-Effectiveness of CCTA
10. Conclusions and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, L.; Shah, A.; Zhao, Q.; Milentijevic, D.; Kharat, A. Economic implications of preventing major cardiovascular and limb events with rivaroxaban plus aspirin in patients with coronary or peripheral artery disease in the United States. Am. Health Drug Benefits 2020, 13, 184–190. [Google Scholar]
- Smith, S.C.; Allen, J.; Blair, S.N.; Bonow, R.O.; Brass, L.M.; Fonarow, G.C.; Grundy, S.M.; Hiratzka, L.; Jones, D.; Krumholz, H.M.; et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: Endorsed by the National Heart, Lung, and Blood Institute. Circulation 2006, 11, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- De Beule, T.; Vanhoenacker, P.; De Booij, M.; Ardies, L.; Bladt, O. Cost effectiveness of multi detector ct angiography of the coronary arteries for the diagnosis of suspected non-st elevation acute coronary syndrome (NSTE-ACS) in the emergency department. Mathematical analysis with a decision model. JBR-BTR 2010, 93, 285. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.; Simpson, A.; Bhagnani, T.; Leeper, N.J.; Murphy, B.; Nordstrom, B.; Ting, W.; Zhao, Q.; Berger, J.S. Incidence and cost of major adverse cardiovascular events and major adverse limb events in patients with chronic coronary artery disease or peripheral artery disease. Am. J. Cardiol. 2019, 123, 1893–1899. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.P.; Jang, E.J.; Kim, Y.J.; Cha, M.; Park, S.; Song, H.J.; Choi, J.E.; Shim, J.; Ahn, J.; Lee, H.J. Cost-effectiveness of coronary CT angiography in patients with chest pain: Comparison with myocardial single photon emission tomography. J. Cardiovasc. Comput. Tomogr. 2015, 9, 428–437. [Google Scholar] [CrossRef]
- Tavakol, M.; Ashraf, S.; Brener, S.J. Risks and complications of coronary angiography: A comprehensive review. Glob. J. Health Sci. 2012, 4, 65–93. [Google Scholar] [CrossRef] [PubMed]
- Skelly, A.C.; Hashimoto, R.; Buckley, D.I.; Brodt, E.D.; Noelck, N.; Totten, A.M.; Lindner, J.R.; Fu, R.; McDonagh, M. Noninvasive Testing for Coronary Artery Disease [Internet]; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2016. Available online: https://www.ncbi.nlm.nih.gov/books/NBK361133/ (accessed on 17 September 2022).
- Hajhosseiny, R.; Bustin, A.; Munoz, C.; Rashid, I.; Cruz, G.; Manning, W.J.; Prieto, C.; Botnar, R.M. Coronary Magnetic Resonance Angiography: Technical Innovations Leading Us to the Promised Land? JACC Cardiovasc. Imaging 2020, 13, 2653–2672. [Google Scholar] [CrossRef] [PubMed]
- Ladapo, J.A.; Hoffmann, U.; Bamberg, F.; Nagurney, J.T.; Cutler, D.M.; Weinstein, M.C.; Gazelle, G.S. Cost-effectiveness of coronary MDCT in the triage of patients with acute chest pain. AJR Am. J. Roentgenol. 2008, 191, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorenoi, V.; Schönermark, M.P.; Hagen, A. CT coronary angiography vs. invasive coronary angiography in CHD. GMS Health Technol. Assess. 2012, 8, Doc02. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, T.A.; Chamarti, K.A.; Tou, L.C.; Demirjian, G.A.; Noorani, S.; Zink, S.; Umair, M. The Merits, Limitations, and Future Directions of Cost-Effectiveness Analysis in Cardiac MRI with a Focus on Coronary Artery Disease: A Literature Review. J. Cardiovasc. Dev. Dis. 2022, 9, 357. [Google Scholar] [CrossRef] [PubMed]
- Pandya, A.; Yu, Y.J.; Ge, Y.; Nagel, E.; Kwong, R.Y.; Abu Bakar, R.; Grizzard, J.D.; Merkler, A.E.; Ntusi, N.; Petersen, S.E.; et al. Evidence-based cardiovascular magnetic resonance cost-effectiveness calculator for the detection of significant coronary artery disease. J. Cardiovasc. Magn. Reson. 2022, 24, 1. [Google Scholar] [CrossRef] [PubMed]
- Foldyna, B.; Szilveszter, B.; Scholtz, J.E.; Banerji, D.; Maurovich-Horvat, P.; Hoffmann, U. CAD-RADS—A new clinical decision support tool for coronary computed tomography angiography. Eur. Radiol. 2018, 28, 4. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.C.; Abbara, S.; Achenbach, S.; Agatston, A.; Berman, D.S.; Budoff, M.J.; Dill, K.E.; Jacobs, J.E.; Maroules, C.D.; Rubin, G.D.; et al. CAD-RADS™: Coronary Artery Disease—Reporting and Data System: An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. J. Am. Coll. Radiol 2016, 13, 12 Pt A. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, U.; Ferencik, M.; Udelson, J.E.; Picard, M.H.; Truong, Q.A.; Patel, M.R.; Huang, M.; Pencina, M.; Mark, D.B.; Heitner, J.F.; et al. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain: Insights from the PROMISE trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation 2017, 135, 2320–2332. [Google Scholar] [CrossRef]
- Bittner, D.O.; Mayrhofer, T.; Budoff, M.; Szilveszter, B.; Foldyna, B.; Hallett, T.R.; Ivanov, A.; Janjua, S.; Meyersohn, N.M.; Staziaki, P.V.; et al. Prognostic Value of Coronary CTA in Stable Chest Pain: CAD-RADS, CAC, and Cardiovascular Events in PROMISE. JACC Cardiovasc. Imaging. 2020, 13, 7. [Google Scholar] [CrossRef]
- Schlett, C.L.; Banerji, D.; Siegel, E.; Bamberg, F.; Lehman, S.J.; Ferencik, M.; Brady, T.J.; Nagurney, J.T.; Hoffmann, U.; Truong, Q.A. Prognostic value of CT angiography for major adverse cardiac events in patients with acute chest pain from the emergency department: 2-year outcomes of the ROMICAT trial. JACC Cardiovasc. Imaging 2011, 4, 481–491. [Google Scholar] [CrossRef] [Green Version]
- Goehler, A.; Mayrhofer, T.; Pursnani, A.; Ferencik, M.; Lumish, H.S.; Barth, C.; Karády, J.; Chow, B.; Truong, Q.A.; Udelson, J.E.; et al. Long-term health outcomes and cost-effectiveness of coronary CT angiography in patients with suspicion for acute coronary syndrome. J. Cardiovasc. Comput. Tomogr. 2020, 14, 44–54. [Google Scholar] [CrossRef]
- Redberg, R.; Katz, M.; Grady, D. Diagnostic tests: Another frontier for less is more: Or why talking to your patient is a safe and effective method of reassurance. Arch. Intern Med. 2011, 171, 619. [Google Scholar] [CrossRef] [PubMed]
- Than, M.; Cullen, L.; Reid, C.M.; Lim, S.H.; Aldous, S.; Ardagh, M.W.; Peacock, W.F.; Parsonage, W.A.; Ho, H.F.; Ko, H.F.; et al. A 2-h diagnostic protocol to assess patients with chest pain symptoms in the Asia-Pacific region (ASPECT): A prospective observational validation study. Lancet 2011, 377, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Rübenthaler, J.; Nörenberg, D.; Huber, T.; Kunz, W.G.; Sommer, W.H.; Schoenberg, S.O.; Janssen, S.; Overhoff, D.; Froelich, M.F. Cost-effectiveness of stress CTP versus CTA in detecting obstructive CAD or in-stent restenosis in stented patients. Eur. Radiol. 2020, 31, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Truong, Q.A.; Schoenfeld, D.A.; Chou, E.T.; Woodard, P.K.; Nagurney, J.T.; Pope, J.H.; Hauser, T.H.; White, C.S.; Weiner, S.G.; et al. Coronary CT angiography versus standard evaluation in acute chest pain. N. Engl. J. Med. 2012, 367, 299–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.H.; Aufderheide, T.P.; Ruthazer, R.; Woolard, R.H.; Feldman, J.A.; Beshansky, J.R.; Griffith, J.L.; Selker, H.P. Missed diagnoses of acute cardiac ischemia in the emergency department. N. Engl. J. Med. 2000, 342, 1163–1170. [Google Scholar] [CrossRef]
- Swap, C.J.; Nagurney, J.T. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA 2005, 294, 2623–2629. [Google Scholar] [CrossRef]
- Aziz, M.U.; Singh, S. Computed tomography of coronary artery atherosclerosis: A review. J. Med. Imaging Radiat. Sci. 2021, 52, S19–S39. [Google Scholar] [CrossRef]
- Litt, H.I.; Gatsonis, C.; Snyder, B.; Singh, H.; Miller, C.D.; Entrikin, D.W.; Leaming, J.M.; Gavin, L.J.; Pacella, C.B.; Hollander, J.E. CT angiography for safe discharge of patients with possible acute coronary syndromes. N. Engl. J. Med. 2012, 366, 1393–1403. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, J.A.; Chinnaiyan, K.M.; Abidov, A.; Achenbach, S.; Berman, D.S.; Hayes, S.W.; Hoffmann, U.; Lesser, J.R.; Mikati, I.A.; O’Neil, B.J.; et al. The CT-STAT (Coronary Computed Tomographic Angiography for Systematic Triage of Acute Chest Pain Patients to Treatment) trial. J. Am. Coll. Cardiol. 2011, 58, 1414–1422. [Google Scholar] [CrossRef]
- Nielsen, L.H.; Ortner, N.; Nørgaard, B.L.; Achenbach, S.; Leipsic, J.; Abdulla, J. The diagnostic accuracy and outcomes after coronary computed tomography angiography vs. conventional functional testing in patients with stable angina pectoris: A systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Imaging 2014, 5, 961–971. [Google Scholar] [CrossRef]
- Jørgensen, M.E.; Andersson, C.; Nørgaard, B.L.; Abdulla, J.; Shreibati, J.B.; Top-Pedersen, C.; Gislason, G.H.; Shaw, R.E.; Hlatky, M.A. Functional testing or coronary computed tomography angiography in patients with stable coronary artery disease. J. Am. Coll. Cardiol. 2017, 69, 1761–1770. [Google Scholar] [CrossRef]
- Karády, J.; Taron, J.; Kammerlander, A.A.; Hoffmann, U. Outcomes of anatomical vs. functional testing for coronary artery disease: Lessons from the major trials. Herz 2020, 45, 421–430. [Google Scholar] [CrossRef]
- Darlington, M.; Gueret, P.; Laissy, J.P.; Pierucci, A.F.; Maoulida, H.; Quelen, C.; Niarra, R.; Chatellier, G.; Durand-Zaleski, I. Cost-effectiveness of computed tomography coronary angiography versus conventional invasive coronary angiography. Eur. J. Health Econ. 2015, 16, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Halpern, E.J.; Savage, M.P.; Fischman, D.L.; Levin, D.C. Cost-effectiveness of coronary CT angiography in evaluation of patients without symptoms who have positive stress test results. AJR Am. J. Roentgenol. 2010, 194, 1257–1262. [Google Scholar] [CrossRef] [PubMed]
- Genders, T.S.S.; Ferket, B.S.; Dedic, A.; Galema, T.W.; Mollet, N.R.; Feyter, P.J.; Fleischmann, K.E.; Nieman, K.; Hunink, M.G. Coronary computed tomography versus exercise testing in patients with stable chest pain: Comparative effectiveness and costs. Int. J. Cardiol. 2013, 167, 1268–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, M.; Hamm, B. Cost effectiveness of coronary angiography and calcium scoring using CT and stress MRI for diagnosis of coronary artery disease. Eur. Radiol. 2007, 17, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Bertoldi, E.G.; Stella, S.F.; Rohde, L.E.P.; Polanczyk, C.A. Cost-effectiveness of anatomical and functional test strategies for stable chest pain: Public health perspective from a middle-income country. BMJ Open 2017, 7, e012652. [Google Scholar] [CrossRef] [Green Version]
- Bertoldi, E.G.; Stella, S.F.; Rohde, L.E.; Polanczyk, C.A. Long-term cost-effectiveness of diagnostic tests for assessing stable chest pain: Modeled analysis of anatomical and functional strategies. Clin. Cardiol. 2016, 39, 249–256. [Google Scholar] [CrossRef]
- Min, J.K.; Gilmore, A.; Budoff, M.J.; Berman, D.S.; O’Day, K. Cost-effectiveness of coronary CT angiography versus myocardial perfusion spect for evaluation of patients with chest pain and no known coronary artery disease. Radiology 2010, 254, 801–808. [Google Scholar] [CrossRef]
- Goeree, R.; Blackhouse, G.; Bowen, J.M.; O’Reilly, D.; Sutherland, S.; Hopkins, R.; Chow, B.; Freeman, M.; Provost, Y.; Dennie, C.; et al. Cost-effectiveness of 64-slice CT angiography compared to conventional coronary angiography based on a coverage with evidence development study in Ontario. Expert Rev. Pharmacoecon. Outcomes Res. 2013, 13, 675–690. [Google Scholar] [CrossRef]
- Stocker, T.J.; Deseive, S.; Leipsic, J.; Hadamitzky, M.; Chen, M.Y.; Rubinshtein, R.; Heckner, M.; Bax, J.J.; Fang, X.; Grove, E.L.; et al. Reduction in radiation exposure in cardiovascular computed tomography imaging: Results from the Prospective multicenter registry on radiation dose estimates of cardiac CT angiography in daily practice in 2017 (Protection VI). Eur. Heart J. 2018, 39, 3715–3723. [Google Scholar] [CrossRef] [Green Version]
- Richards, C.E.; Dorman, S.; John, P.; Davies, A.; Evans, S.; Ninan, T.; Martin, D.; Kannoly, S.; Roberts-Davies, G.; Ramsey, M.; et al. Low-radiation and high image quality coronary computed tomography angiography in “real-world” unselected patients. World J. Radiol. 2018, 10, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Gimelli, A.; Achenbach, S.; Buechel, R.R.; Edvardsen, T.; Francone, M.; Gaemperli, O.; Hacker, M.; Hyafil, F.; Kaufmann, P.A.; Lancellotti, P.; et al. Strategies for radiation dose reduction in nuclear cardiology and cardiac computed tomography imaging: A report from the European Association of Cardiovascular Imaging (EACVI), the Cardiovascular Committee of European Association of Nuclear Medicine (EANM), and the European Society of Cardiovascular Radiology (ESCR). Eur. Heart J. 2018, 39, 286–296. [Google Scholar] [CrossRef]
- Miller, J.M.; Rochitte, C.E.; Dewey, M.; Arbab-Zadeh, A.; Niinuma, H.; Gottlieb, I.; Paul, N.; Clouse, M.E.; Shapiro, E.P.; Hoe, J.; et al. Diagnostic performance of coronary angiography by 64-row CT. N. Engl. J. Med. 2008, 359, 2324–2336. [Google Scholar] [CrossRef] [Green Version]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Z.; Almutairi, A.M. Diagnostic accuracy of 64 multislice CT angiography in the assessment of coronary in-stent restenosis: A meta-analysis. Eur. J. Radiol. 2010, 73, 266–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijboom, W.B.; Van Mieghem, C.A.; van Pelt, N.; Weustink, A.; Pugliese, F.; Mollet, N.R.; Boersma, E.; Regar, E.; van Geuns, R.J.; de Jaegere, P.J.; et al. Comprehensive assessment of coronary artery stenoses: Computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina. J. Am. Coll. Cardiol. 2008, 52, 636–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, B.K.; Erglis, A.; Doh, J.H.; Daniels, D.V.; Jegere, S.; Kim, H.; Dunning, A.; DeFrance, T.; Lansky, A.; Leipsic, J.; et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J. Am. Coll. Cardiol. 2011, 58, 1989–1997. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, B.; Wang, S.; Zhao, S.; Lu, M. Computed tomography angiography-derived fractional flow reserve (CT-FFR) for the detection of myocardial ischemia with invasive fractional flow reserve as reference: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 712–725. [Google Scholar] [CrossRef]
- Danad, I.; Szymonifka, J.; Twisk, J.W.R.; Norgaard, B.L.; Zarins, C.K.; Knaapen, P.; Min, J.K. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: A meta-analysis. Eur. Heart J. 2017, 38, 991–998. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, J.A.; Lipinski, M.J.; Flors, L.; Shaw, P.W.; Kramer, C.M.; Salerno, M. Meta-analysis of diagnostic performance of coronary computed tomography angiography, computed tomography perfusion, and computed tomography-fractional flow reserve in functional myocardial ischemia assessment versus invasive fractional flow reserve. Am. J. Cardiol. 2015, 116, 1469–1478. [Google Scholar] [CrossRef] [Green Version]
- Ihdayhid, A.R.; Norgaard, B.L.; Gaur, S.; Leipsic, J.; Nerlekar, N.; Osawa, K.; Miyoshi, T.; Jensen, J.M.; Kimura, T.; Shiomi, H.; et al. Prognostic value and risk continuum of noninvasive fractional flow reserve derived from coronary CT angiography. Radiology 2019, 292, 343–351. [Google Scholar] [CrossRef]
- Min, J.K.; Koo, B.K.; Erglis, A.; Doh, J.; Daniels, D.V.; Jegere, S.; Kim, H.; Dunning, A.; Defrance, T.; Leipsic, J. Effect of image quality on diagnostic accuracy of noninvasive fractional flow reserve: Results from the prospective multicenter international DISCOVER-FLOW study. J. Cardiovasc. Comput. Tomogr. 2012, 6, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Wang, X.; Wu, T.; Yang, Z.; Li, S.; Li, Y.; He, F.; Zhang, M.; Yang, C.; Jia, S.; et al. Clinical application of computed tomography angiography and fractional flow reserve computed tomography in patients with coronary artery disease: A meta-analysis based on pre- and post-test probability. Eur. J. Radiol. 2021, 139, 109712. [Google Scholar] [CrossRef]
- Kay, F.U. Dual-energy CT and coronary imaging. Cardiovasc. Diagn. Ther. 2022, 10, 4. [Google Scholar] [CrossRef]
- Tarkowski, P.; Czekajska-Chehab, E. Dual-Energy Heart CT: Beyond Better Angiography-Review. J. Clin. Med. 2021, 10, 5193. [Google Scholar] [CrossRef]
- Nieman, K.; Balla, S. Dynamic CT myocardial perfusion imaging. J. Cardiovasc. Comput. Tomogr. 2020, 14, 4. [Google Scholar] [CrossRef]
- Assen, M.V.; Vonder, M.; Pelgrim, G.J.; Doeberitz, P.L.; Vliegenthart, R. Computed tomography for myocardial characterization in ischemic heart disease: A state-of-the-art review. Eur. Radiol. Exp. 2020, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Muñoz, A.; Valente, F.; Dux-Santoy, L.; Guala, A.; Teixidó-Turà, G.; Galián-Gay, L.; Gutiérrez, L.; Fernández-Galera, R.; Casas, G.; González-Alujas, T.; et al. Diagnostic value of quantitative parameters for myocardial perfusion assessment in patients with suspected coronary artery disease by single- and dual-energy computed tomography myocardial perfusion imaging. IJC Heart Vasc. 2021, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Pontone, G.; Baggiano, A.; Andreini, D.; Guaricci, A.I.; Guglielmo, M.; Muscogiuri, G.; Fusini, L.; Soldi, M.; Del Torto, A.; Mushtaq, S.; et al. Dynamic Stress Computed Tomography Perfusion With a Whole-Heart Coverage Scanner in Addition to Coronary Computed Tomography Angiography and Fractional Flow Reserve Computed Tomography Derived. JACC Cardiovasc. Imaging. 2019, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- van Assen, M.; Muscogiuri, G.; Caruso, D.; Lee, S.J.; Laghi, A.; De Cecco, C.N. Artificial intelligence in cardiac radiology. Radiol. Med. 2020, 125, 1186–1199. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Van Assen, M.; Tesche, C.; De Cecco, C.N.; Chiesa, M.; Scafuri, S.; Guglielmo, M.; Baggiano, A.; Fusini, L.; Guaricci, A.I.; et al. Artificial intelligence in coronary computed tomography angiography: From anatomy to prognosis. Biomed. Res. Int. 2020, 2020, 6649410. [Google Scholar] [CrossRef] [PubMed]
- Tesche, C.; de Cecco, C.N.; Baumann, S.; Renker, M.; McLaurin, T.W.; Duguay, T.M.; Bayer, R.R.; Steinberg, D.H.; Grant, K.L.; Canstein, C.; et al. Coronary CT angiography-derived fractional flow reserve: Machine learning algorithm versus computational fluid dynamics modeling. Radiology 2018, 288, 64–72. [Google Scholar] [CrossRef] [Green Version]
- von Knebel Doeberitz, P.L.; De Cecco, C.N.; Schoepf, U.J.; Duguay, T.M.; Albrecht, M.H.; van Assen, M.; Bauer, M.J.; Savage, R.H.; Pannell, J.T.; De Santis, D.; et al. Coronary CT angiography-derived plaque quantification with artificial intelligence CT fractional flow reserve for the identification of lesion-specific ischemia. Eur. Radiol. 2019, 29, 2378–2387. [Google Scholar] [CrossRef]
- Coenen, A.; Kim, Y.H.; Kruk, M.; Tesche, C.; De Geer, J.; Kurata, A.; Lubbers, M.L.; Daemen, J.; Itu, L.; Rapaka, S.; et al. Diagnostic accuracy of a machine-learning approach to coronary computed tomographic angiography-based fractional flow reserve: Result from the MACHINE consortium. Circ. Cardiovasc. Imaging 2018, 11, e007217. [Google Scholar] [CrossRef] [Green Version]
- van Rosendael, A.R.; Maliakal, G.; Kolli, K.K.; Beecy, A.; Al’Aref, S.J.; Dwivedi, A.; Singh, G.; Panday, M.; Kumar, A.; Ma, X.; et al. Maximization of the usage of coronary CTA derived plaque information using a machine learning based algorithm to improve risk stratification; insights from the CONFIRM registry. J. Cardiovasc. Comput. Tomogr. 2018, 12, 204–209. [Google Scholar] [CrossRef]
- Motwani, M.; Dey, D.; Berman, D.S.; Germano, G.; Achenbach, S.; Al-Mallah, M.H.; Andreini, D.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; et al. Machine learning for prediction of all-cause mortality in patients with suspected coronary artery disease: A 5-year multicentre prospective registry analysis. Eur. Heart J. 2017, 38, 500–507. [Google Scholar] [CrossRef] [Green Version]
- Tesche, C.; Bauer, M.J.; Baquet, M.; Hedels, B.; Straube, F.; Hartl, S.; Gray, H.N.; Jochheim, D.; Aschauer, T.; Rogowski, S.; et al. Improved long-term prognostic value of coronary CT angiography-derived plaque measures and clinical parameters on adverse cardiac outcome using machine learning. Eur. Radiol. 2021, 31, 486–493. [Google Scholar] [CrossRef]
- Cademartiri, F.; Malagò, R.; Belgrano, M.; Alberghina, F.; Maffei, E.; La Grutta, L.; Palumbo, A.A.; Runza, G.; Mollet, N.R.; Midiri, M.; et al. Spectrum of collateral findings in multislice CT coronary angiography. Radiol. Med. 2007, 112, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Goehler, A.; McMahon, P.M.; Lumish, H.S.; Wu, C.C.; Munshi, V.; Gilmore, M.; Chung, J.H.; Ghoshhajra, B.B.; Mark, D.; Truong, Q.A.; et al. Cost-effectiveness of follow-up of pulmonary nodules incidentally detected on cardiac computed tomographic angiography in patients with suspected coronary artery disease. Circulation 2014, 130, 668–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karády, J.; Mayrhofer, T.; Ivanov, A.; Foldyna, B.; Lu, M.T.; Ferencik, M.; Pursnani, A.; Salerno, M.; Udelson, J.E.; Mark, D.B.; et al. Cost-effectiveness analysis of anatomic vs functional index testing in patients with low-risk stable chest pain. JAMA Netw. Open 2020, 3, e2028312. [Google Scholar] [CrossRef]
- Douglas, P.S.; Hoffmann, U.; Patel, M.R.; Mark, D.B.; Al-Khalidi, H.R.; Cavanaugh, B.; Cole, J.; Dolor, R.J.; Fordyce, C.B.; Huang, M.; et al. Outcomes of anatomical versus functional testing for coronary artery disease. N. Engl. J. Med. 2015, 372, 1291–1300. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burch, R.A.; Siddiqui, T.A.; Tou, L.C.; Turner, K.B.; Umair, M. The Cost Effectiveness of Coronary CT Angiography and the Effective Utilization of CT-Fractional Flow Reserve in the Diagnosis of Coronary Artery Disease. J. Cardiovasc. Dev. Dis. 2023, 10, 25. https://doi.org/10.3390/jcdd10010025
Burch RA, Siddiqui TA, Tou LC, Turner KB, Umair M. The Cost Effectiveness of Coronary CT Angiography and the Effective Utilization of CT-Fractional Flow Reserve in the Diagnosis of Coronary Artery Disease. Journal of Cardiovascular Development and Disease. 2023; 10(1):25. https://doi.org/10.3390/jcdd10010025
Chicago/Turabian StyleBurch, Rex A., Taha A. Siddiqui, Leila C. Tou, Kiera B. Turner, and Muhammad Umair. 2023. "The Cost Effectiveness of Coronary CT Angiography and the Effective Utilization of CT-Fractional Flow Reserve in the Diagnosis of Coronary Artery Disease" Journal of Cardiovascular Development and Disease 10, no. 1: 25. https://doi.org/10.3390/jcdd10010025
APA StyleBurch, R. A., Siddiqui, T. A., Tou, L. C., Turner, K. B., & Umair, M. (2023). The Cost Effectiveness of Coronary CT Angiography and the Effective Utilization of CT-Fractional Flow Reserve in the Diagnosis of Coronary Artery Disease. Journal of Cardiovascular Development and Disease, 10(1), 25. https://doi.org/10.3390/jcdd10010025