
Evaluation of Exercise Mobile Applications for Adults with Cardiovascular Disease Risk Factors

Abstract
:1. Introduction
2. Methods
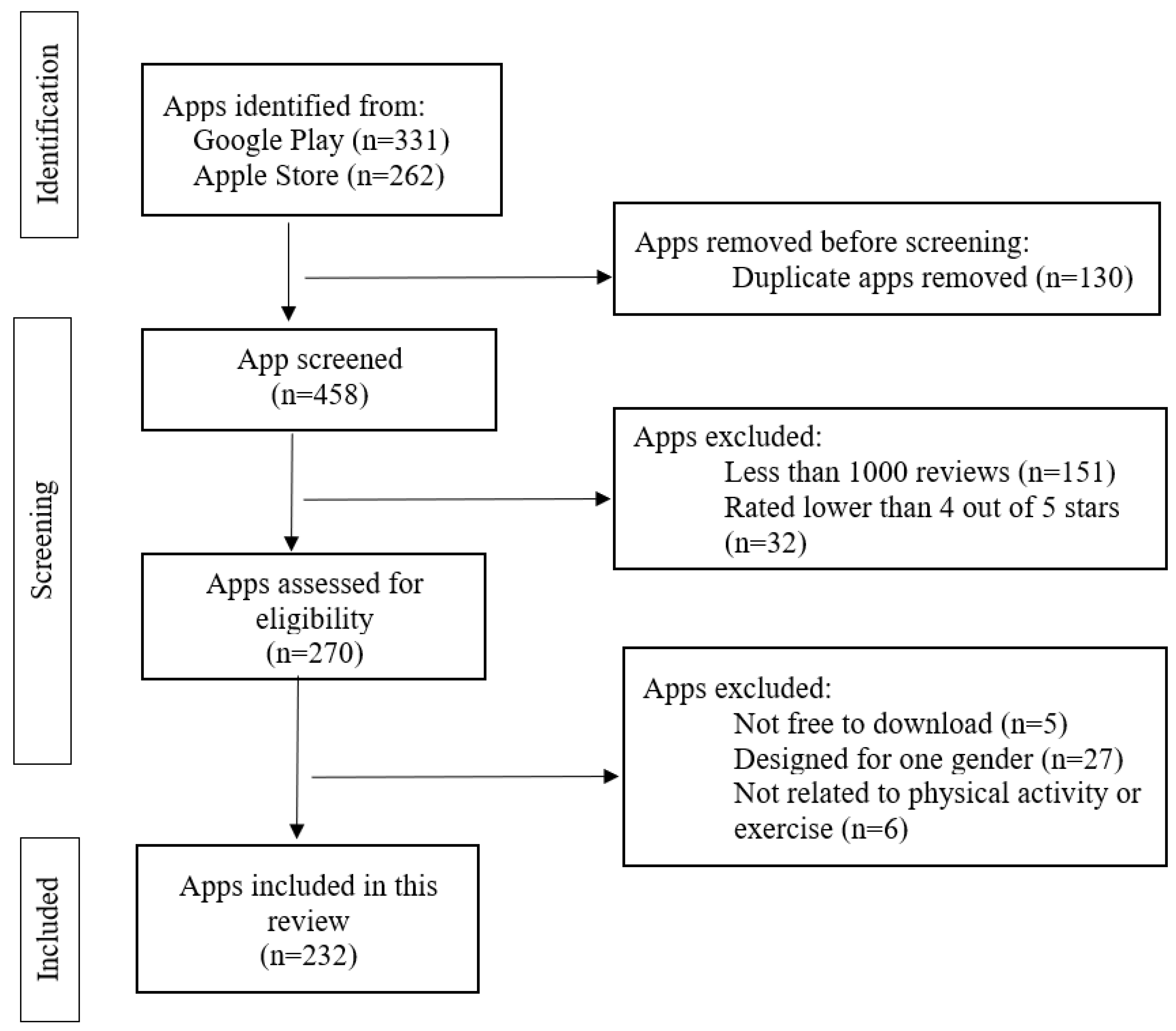
2.1. Search Strategy and Methods
2.2. Data Extraction and Coding
2.3. Statistical Analysis
3. Results
3.1. The Scientific Evidence Base
3.2. The Preparticipation Health Screening Protocol
3.3. The Cardiovascular Disease Risk Factor Profile
3.4. Prioritization of the Chronic Diseases or Health Conditions
3.5. Framing the Exercise Plans by the FITT ExRx
3.6. Special Considerations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Adult Physical Inactivity Prevalence Maps by Race/Ethnicity. Available online: https://www.cdc.gov/physicalactivity/data/inactivity-prevalence-maps/index.html (accessed on 29 July 2022).
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R. Physical Activity and Cardiovascular Disease: How Much Is Enough? AJLM 2009, 3, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart Disease and Stroke Statistics—2023 Update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Powell, K.E.; King, A.C.; Buchner, D.M.; Campbell, W.W.; DiPietro, L.; Erickson, K.I.; Hilman, C.H.; Jakicic, J.M.; Janz, K.F.; Katzmarzyk, P.T.; et al. Physical Activity Guidelines Advisory Committee. In 2018 Physical Activity Guidelines Advisory Committee Scientific Report; Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Thompson, P.D.; Eijsvogels, T.M.H. New Physical Activity Guidelines: A Call to Activity for Clinicians and Patients. JAMA 2018, 320, 1983–1984. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.C.; Paul, M.; Hayden, B.B.; Paul, K.W. Prevention and Control of Hypertension: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1278–1293. [Google Scholar]
- Kraus, W.E.; Powell, K.E.; Haskell, W.L.; Janz, K.F.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L.; et al. Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease. Med. Sci. Sports Exerc. 2019, 51, 1270–1281. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. BJSM 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Barnes, P.; Schoenborn, C. Trends in Adults Receiving a Recommendation for Exercise or Other Physical Activity from a Physician or Other Health Professional. NCHS Data Brief 2012, 86, 1–8. [Google Scholar]
- Selvaraj, C.S.; Abdullah, N. Physically active primary care doctors are more likely to offer exercise counselling to patients with cardiovascular diseases: A cross-sectional study. BMC Prim. Care 2022, 23, 59. [Google Scholar] [CrossRef]
- Hansen, D.; Ruiz, G.R.; Doherty, P.; Iliou, M.-C.; Vromen, T.; Hinton, S.; Frederix, I.; Wilhelm, M.; Schmid, J.-P.; Abreu, A.; et al. Do Clinicians Prescribe Exercise Similarly in Patients with Different Cardiovascular Diseases? Findings from the EAPC EXPERT Working Group Survey. Eur. J. Prev. Cardiol. 2018, 25, 682–691. [Google Scholar] [CrossRef]
- Research and Market. Fitness App Market Size, Share & Trends Analysis Report by Type (Exercise & Weight Loss, Diet & Nutrition, Activity Tracking), by Platform (Android, iOS), by Device, by Region, and Segment Forecasts, 2022–2030; Grand View Research: San Francisco, CA, USA, 2022; Chapter 2. [Google Scholar]
- Romeo, A.; Edney, S.; Plotnikoff, R.; Curtis, R.; Ryan, J.; Sanders, I.; Crozier, A.; Maher, C. Smartphone Apps Increase Physical Activity? Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e12053. [Google Scholar] [CrossRef] [PubMed]
- Daryabeygi-Khotbehsara, R.; Islam, S.M.S.; Dunstan, D.; McVicar, J.; Abdelrazek, M.; Maddison, R. Smartphone-Based Interventions to Reduce Sedentary Behavior and Promote Physical Activity Using Integrated Dynamic Models: Systematic Review. J. Med. Internet Res. 2021, 23, e26315. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. 2016, 13, 127. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Arena, R.; Riebe, D.W.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Baltimore, ML, USA, 2013. [Google Scholar]
- Thompson, W.; Gordon, N.; Pescatello, L.S. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Lippincott Williams & Wilkins: Baltimore, ML, USA, 2009. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Breton, E.R.; Fuemmeler, B.F.; Abroms, L.C. Weight loss—There is an app for that! But does it adhere to evidence-informed practices? Transl. Behav. Med. 2011, 1, 523–529. [Google Scholar] [CrossRef]
- Azar, J.; Lesser, I.; Laing, Y. Mobile applications for weight management: Theory-based content analysis. Am. J. Prev. Med. 2013, 45, 583–589. [Google Scholar] [CrossRef]
- Gustavo, C.M.; Marina, B.P.; Hopin, L. Smartphone apps for the self-management of low back pain: A systematic review. Best Pract. Res. Clin. Rheumatol. 2016, 30, 1098–1109. [Google Scholar]
- Haskins, B.L.; Lesperance, D.; Gibbons, P.; Boudreaux, E.D. A systematic review of smartphone applications for smoking cessation. Trans. Behav. Med. 2017, 7, 292–299. [Google Scholar] [CrossRef]
- American College of Sports Medicine; Gary, L. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- American Heart Association Life’s Essential 8. Available online: https://www.heart.org/en/healthy-living/healthy-lifestyle/lifes-essential-8 (accessed on 22 April 2023).
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. What Exercise Professionals Need to Know. ACSMs Health Fit. J. 2016, 20, 22–27. [Google Scholar]
- Simple Design Ltd. 7 Minute Workout. Simple Design Ltd., 1.363.112. 23 June 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.popularapp.sevenmins&hl=en_US&gl=US (accessed on 23 June 2021).
- EM Digital LLC. Jillian Michaels | The Fitness App. EM Digital LLC, 4.2.10. 1 September 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.emdigital.jillianmichaels&hl=en_US&gl=US (accessed on 1 September 2021).
- The National Exercise & Sports Trainers Association. Available online: https://www.nestacertified.com/ (accessed on 22 April 2023).
- Deborah, R.; Jonathan, K.E.; Gary, L.; Meir, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Gymclan Health & Fitness Services. Fitpaa 💪 Weight Loss/Gain, Bodybuilding, Six Pack. Gymclan Health & Fitness Services, 4.0.71. 1 September 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.gymclan (accessed on 1 September 2021).
- ASICS Digital, Inc. Runkeeper—GPS Track Run Walk. ASICS Digital, Inc. 1.03. Google Play. 1 September 2021. Available online: https://play.google.com/store/apps/details?id=com.fitnesskeeper.runkeeper.pro&hl=en_US&gl=US (accessed on 1 September 2021).
- Nike, Inc. Nike Training Club: Fitness. Nike, Inc., 6.21.0. 1 September 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.nike.ntc&hl=en_US&gl=US (accessed on 1 September 2021).
- Ratsev, V. Back Pain Relief Exercises at Home. Vladimir Ratsev. 1.0.99. 23 June 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.vratsev.bpex&hl=en_US&gl=US (accessed on 23 June 2021).
- Riebe, D.; Franklin, B.A.; Thompson, P.D.; Garber, C.E.; Whitfield, G.P.; Magal, M.; Pescatello, L.S. Updating ACSM’s Recommendations for Exercise Preparticipation Health Screening. Med. Sci. Sports Exerc. 2015, 47, 2473–2479. [Google Scholar] [CrossRef]
- FitOn. FitOn Workouts & Fitness Plans. FitOn, 5.5.0. 23 June 2021. Google Play. Available online: https://play.google.com/store/apps/details?id=com.fiton.android&hl=en_US&gl=US (accessed on 23 June 2021).
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary. Circulation 2018, 73, 3168–3209. [Google Scholar]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [PubMed]
- Karmali, K.N.; Lloyd-Jones, D.M. Implementing cardiovascular risk prediction in clinical practice: The future is now. J. Am. Heart Assoc. 2017, 6, 006019. [Google Scholar] [CrossRef] [PubMed]
- Karmali, K.N.; Lloyd-Jones, D.M.; van der Leeuw, J.; Goff, D.C., Jr.; Yusuf, S.; Zanchetti, A.; Glasziou, P.; Jackson, R.; Woodward, M.; Rodgers, A.; et al. Blood pressure-lowering treatment strategies based on cardiovascular risk versus blood pressure: A meta-analysis of individual participant data. PLoS Med. 2018, 15, e1002538. [Google Scholar] [CrossRef]
- Billinger, S.A.; Boyne, P.; Coughenour, E.; Dunning, K.; Mattlage, A. Does aerobic exercise and the FITT principle fit into stroke recovery? Curr. Neurol. Neurosci. Rep. 2015, 15, 519. [Google Scholar] [CrossRef]
- Grace, B.; Lucas, C.T.; Shetgiri, R.; Cardenas, K.; de la Garza, G.P.; Pak, Y.; Yee, J.K. Physical Activity Counseling and Documentation by Pediatric Residents in Primary Care: Before and after Introduction of the FITT Principle. Clin. Pediatr. 2022, 62, 449–455. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services. Physical Activity Guidelines Advisory Committee Report, 2008: To the Secretary of Health and Human Services; U.S. Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]
- Pescatello, L.S.; Wu, Y.; Panza, G.A.; Zaleski, A.; Guidry, M. Development of a Novel Clinical Decision Support System for Exercise Prescription among Patients with Multiple Cardiovascular Disease Risk Factors. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 5, 193–203. [Google Scholar] [CrossRef]


{kind=link}
| Questions and Answers | Number of Apps | Percentage of Apps | Notes |
|---|---|---|---|
| Question 1: Did the app specify the scientific foundation upon which the app was based? | |||
| A. Scientific evidence or guidelines from professional organizations. | n = 1 | 0.4% | |
| B. Expert’ or professional’ opinion. | n = 10 | 4.3% | |
| C. Neither A nor B. | n = 221 | 95.3% | |
| Question 2: Did the app include an exercise preparticipation health screening function for users? | |||
| A. The app included an exercise preparticipation health screening function. | n = 0 | 0% | |
| B. The app recommended the user consult with professionals about preparticipation health screening in the legal disclaimer. | n = 80 | 34.5% | |
| C. The app had no information on exercise preparticipation health screening. | n = 152 | 65.5% | |
| Question 3: Did the app build a CVD risk factor profile for users? | |||
| A. The app collected a comprehensive CVD risk factor user profile. | n = 1 | 0.4% | |
| B. The app collected some information on the CVD risk factor profile, but it was not comprehensive. | n = 90 | 38.8% | Information was collected on: Age: n = 82, 35.3% BMI: n = 74, 31.9% Baseline activity: n = 40, 17.2% |
| C. The app did not collect any CVD risk factor profile information. | n = 142 | 61.2% | |
| Question 4: Did the app’s exercise plan focus on one or more of the user’s chronic disease(s) and/or health condition(s)? | |||
| A. The exercise plan focused on one chronic disease or health condition based on the health information collected from the users. | n = 1 | 0.4% | |
| B. The exercise plan focused on a named disease or health condition regardless of the chronic disease or health conditions information collected from the users. | n = 8 | 3.4% | |
| C. The exercise plan focused on body image or athletic performance. * | n = 155 | 66.8% | Exercise plan focused on: Body image: n = 71, 45.8% Weight loss: n = 124, 80.0% Athletic performance: n = 44, 27.1% Injury recovery: n = 7, 4.5% |
| D. The exercise plan did not have a clear focus regardless of the information collected from the user, if any. | n = 69 | 29.7% | |
| Question 5: Did the app provide recommendations for all four types of exercise (i.e., aerobic, resistance, neuromotor and flexibility)? # | |||
| A. The app provided recommendations all four types of exercise. | n = 10 | 4.3% | |
| B. The app provided exercise recommendations for aerobic and/or resistance exercise only. | n = 173 | 70.7% | Exercise recommendations were provided for: Both aerobic and resistance exercise: n = 80, 46.2%. Only aerobic or only resistance exercise: n = 93, 53.8% |
| C. The app provided various options and let the users choose which type of exercise to perform. | n = 49 | 21.1% | |
| D. The app provided no information about exercise types. | n = 0 | 0% | |
| Question 6: Did the app provide the FIT information for each type of exercise recommended? § | |||
| A. The app provided a comprehensive FIT information for each type of exercise recommended. | n = 42 | 18.1% | |
| B. The app provided some but not all the FIT information for each type of exercise recommended. | n = 116 | 50.0% | |
| C. The app provided no FIT information for each type of exercise recommended. | n = 74 | 31.9% | |
| Question 7: Did the exercise app provide special considerations to ensure safety and maximize the health benefits of exercise? | |||
| A. The app provided a comprehensive list of special considerations for CVD Risk Factor(s), Existing Disease(s), and/or Health Condition(s) for users. | n = 0 | 0% | |
| B. The app listed some but not all special considerations for CVD Risk Factor(s), Existing Disease(s), and/or Health Condition(s) for users. | n = 3 | 1.3% | |
| C. The app had no information regarding special considerations for CVD Risk Factor(s), Existing Disease(s), and/or Health Condition(s) for users | n = 229 | 98.7% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Wu, Y.; Bushey, E.L.; Pescatello, L.S. Evaluation of Exercise Mobile Applications for Adults with Cardiovascular Disease Risk Factors. J. Cardiovasc. Dev. Dis. 2023, 10, 477. https://doi.org/10.3390/jcdd10120477
Chen S, Wu Y, Bushey EL, Pescatello LS. Evaluation of Exercise Mobile Applications for Adults with Cardiovascular Disease Risk Factors. Journal of Cardiovascular Development and Disease. 2023; 10(12):477. https://doi.org/10.3390/jcdd10120477
Chicago/Turabian StyleChen, Shiqi, Yin Wu, Erica L. Bushey, and Linda S. Pescatello. 2023. "Evaluation of Exercise Mobile Applications for Adults with Cardiovascular Disease Risk Factors" Journal of Cardiovascular Development and Disease 10, no. 12: 477. https://doi.org/10.3390/jcdd10120477
APA StyleChen, S., Wu, Y., Bushey, E. L., & Pescatello, L. S. (2023). Evaluation of Exercise Mobile Applications for Adults with Cardiovascular Disease Risk Factors. Journal of Cardiovascular Development and Disease, 10(12), 477. https://doi.org/10.3390/jcdd10120477