

Association between Psychiatric Disorders and the Incidence of Heart Failure in Women

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Elements
2.2. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
3.2.1. Incidence of HF
3.2.2. Length of Stay
3.2.3. Cost of Care
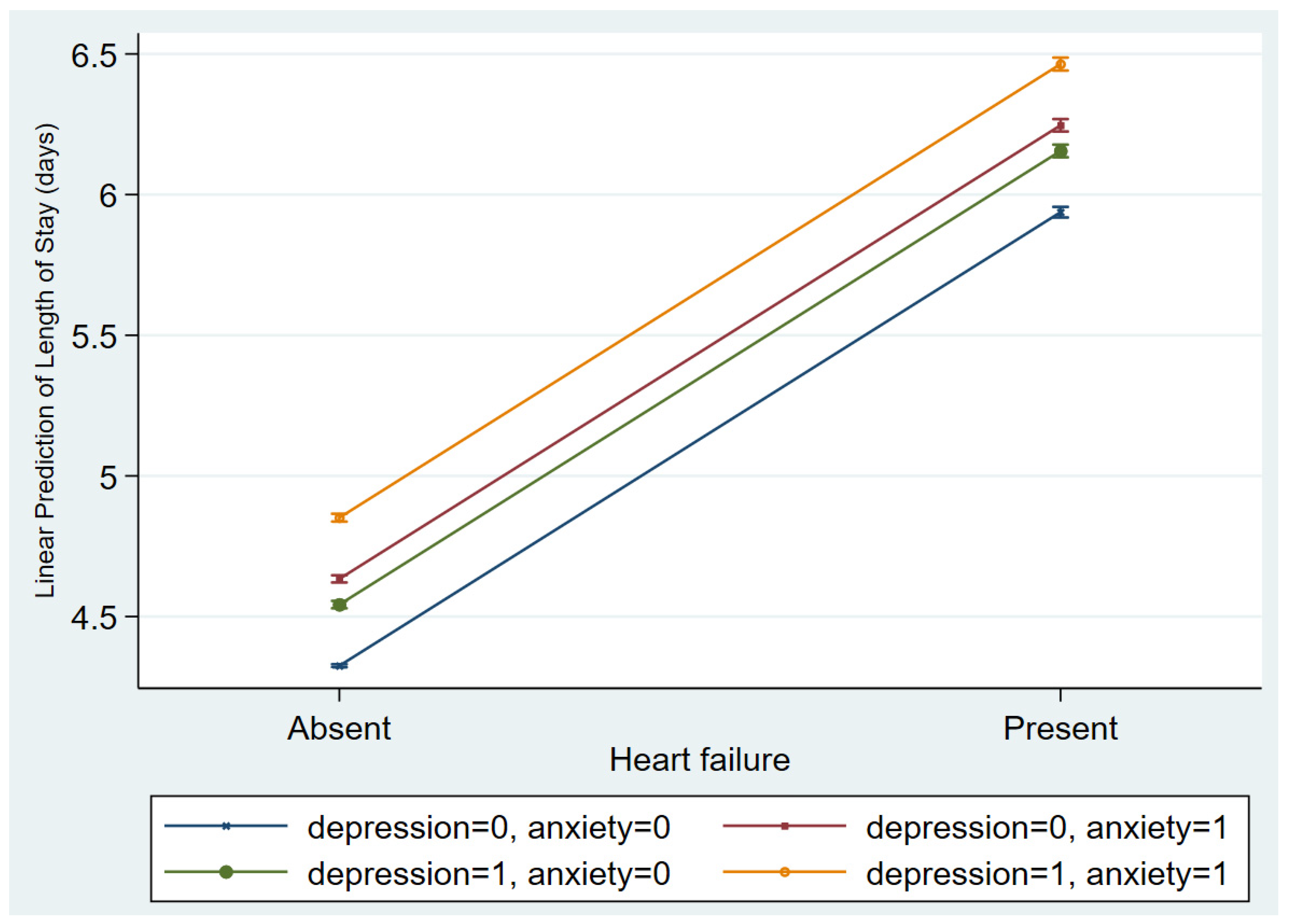
3.3. Influence of Depression and Anxiety on Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Di Palo, K.E. Psychological Disorders in Heart Failure. Cardiol. Clin. 2022, 40, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Beristianos, M.H.; Yaffe, K.; Cohen, B.; Byers, A.L. PTSD and Risk of Incident Cardiovascular Disease in Aging Veterans. Am. J. Geriatr. Psychiatry 2016, 24, 192–200. [Google Scholar] [CrossRef]
- Leander, M.; Lampa, E.; Rask-Andersen, A.; Franklin, K.; Gislason, T.; Oudin, A.; Svanes, C.; Torén, K.; Janson, C. Impact of anxiety and depression on respiratory symptoms. Respir. Med. 2014, 108, 1594–1600. [Google Scholar] [CrossRef] [PubMed]
- Redeker, N.S. Somatic symptoms explain differences in psychological distress in heart failure patients vs a comparison group. Prog. Cardiovasc. Nurs. 2006, 21, 182–189. [Google Scholar] [CrossRef]
- DeJongh, B.; Birkeland, K.; Brenner, M. Managing Comorbidities in Patients with Chronic Heart Failure: First, Do No Harm. Am. J. Cardiovasc. Drugs 2015, 15, 171–184. [Google Scholar] [CrossRef]
- Silver, M.A. Depression and heart failure: An overview of what we know and don’t know. Cleve. Clin. J. Med. 2010, 77, S7–S11. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, T.; Reis, V.A.; Linke, S.E.; Greenberg, B.H.; Mills, P.J. Depression in Heart Failure: A Meta-Analytic Review of Prevalence, Intervention Effects, and Associations With Clinical Outcomes. J. Am. Coll. Cardiol. 2006, 48, 1527–1537. [Google Scholar] [CrossRef]
- Bordoni, B.; Marelli, F.; Morabito, B.; Sacconi, B. Depression and anxiety in patients with chronic heart failure. Future Cardiol. 2018, 14, 115–119. [Google Scholar] [CrossRef]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender Differences in Depression in Representative National Samples: Meta-Analyses of Diagnoses and Symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Mendes de Leon, C.F.; Krumholz, H.M.; Seeman, T.S.; Vaccarino, V.; Williams, C.S.; Kasl, S.V.; Berkman, L.F. Depression and Risk of Coronary Heart Disease in Elderly Men and Women: New Haven EPESE, 1982–1991. Arch. Intern. Med. 1998, 158, 2341–2348. [Google Scholar] [CrossRef]
- Gottlieb, S.S.; Khatta, M.; Friedmann, E.; Einbinder, L.; Katzen, S.; Baker, B.; Marshall, J.; Minshall, S.; Robinson, S.; Fisher, M.L.; et al. The influence of age, gender, and race on the prevalence of depression in heart failure patients. J. Am. Coll. Cardiol. 2004, 43, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Gaffey, A.E.; Cavanagh, C.E.; Rosman, L.; Wang, K.; Deng, Y.; Sims, M.; O’Brien, E.C.; Chamberlain, A.M.; Mentz, R.J.; Glover, L.M.; et al. Depressive Symptoms and Incident Heart Failure in the Jackson Heart Study: Differential Risk Among Black Men and Women. J. Am. Heart Assoc. 2022, 11, e022514. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Hastings, M.H.; Rhee, J.; Trager, L.E.; Roh, J.D.; Rosenzweig, A. Targeting Age-Related Pathways in Heart Failure. Circ. Res. 2020, 126, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Larson, M.G.; Leip, E.P.; Beiser, A.; D’Agostino, R.B.; Kannel, W.B.; Murabito, J.M.; Vasan, R.S.; Benjamin, E.J.; Levy, D. Lifetime Risk for Developing Congestive Heart Failure. Circulation 2002, 106, 3068–3072. [Google Scholar] [CrossRef] [PubMed]
- NHLBI, NIH. Heart Failure—Causes and Risk Factors. Available online: https://www.nhlbi.nih.gov/health/heart-failure/causes (accessed on 8 April 2023).
- WHO. World Mental Health Report: Transforming Mental Health for All—Executive Summary. Available online: https://www.who.int/publications-detail-redirect/9789240050860 (accessed on 18 June 2023).
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef]
- Carroll, D.; Phillips, A.C.; Gale, C.R.; Batty, G.D. Generalized anxiety and major depressive disorders, their comorbidity and hypertension in middle-aged men. Psychosom. Med. 2010, 72, 16–19. [Google Scholar] [CrossRef]
- Yu, M.; Zhang, X.; Lu, F.; Fang, L. Depression and Risk for Diabetes: A Meta-Analysis. Can. J. Diabetes 2015, 39, 266–272. [Google Scholar] [CrossRef]
- Heiskanen, T.H.; Niskanen, L.K.; Hintikka, J.J.; Koivumaa-Honkanen, H.T.; Honkalampi, K.M.; Haatainen, K.M.; Viinamäki, H.T. Metabolic syndrome and depression: A cross-sectional analysis. J. Clin. Psychiatry 2006, 67, 1422–1427. [Google Scholar] [CrossRef]
- Kawachi, I.; Sparrow, D.; Vokonas, P.S.; Weiss, S.T. Decreased heart rate variability in men with phobic anxiety (data from the Normative Aging Study). Am. J. Cardiol. 1995, 75, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, S.-X.; Liu, Y.; Rodriguez, F.; Watson, K.E.; Dreyer, R.P.; Khera, R.; Murugiah, K.; D’Onofrio, G.; Spatz, E.S.; et al. Sex-Specific Risk Factors Associated With First Acute Myocardial Infarction in Young Adults. JAMA Netw. Open 2022, 5, e229953. [Google Scholar] [CrossRef] [PubMed]
- Emdin, C.A.; Odutayo, A.; Wong, C.X.; Tran, J.; Hsiao, A.J.; Hunn, B.H.M. Meta-Analysis of Anxiety as a Risk Factor for Cardiovascular Disease. Am. J. Cardiol. 2016, 118, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Allabadi, H.; Probst-Hensch, N.; Alkaiyat, A.; Haj-Yahia, S.; Schindler, C.; Kwiatkowski, M.; Zemp, E. Mediators of gender effects on depression among cardiovascular disease patients in Palestine. BMC Psychiatry 2019, 19, 284. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.A.; Kasl, S.V.; Heiat, A.; Abramson, J.L.; Krumholz, H.M.; Vaccarino, V. Depression and risk of heart failure among the elderly: A prospective community-based study. Psychosom. Med. 2002, 64, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Dewan, P.; Rørth, R.; Jhund, P.S.; Shen, L.; Raparelli, V.; Petrie, M.C.; Abraham, W.T.; Desai, A.S.; Dickstein, K.; Køber, L.; et al. Differential Impact of Heart Failure With Reduced Ejection Fraction on Men and Women. J. Am. Coll. Cardiol. 2019, 73, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Haedtke, C.A.; Moser, D.K.; Pressler, S.J.; Chung, M.L.; Wingate, S.; Goodlin, S.J. Influence of depression and gender on symptom burden among patients with advanced heart failure: Insight from the pain assessment, incidence and nature in heart failure study. Heart Lung 2019, 48, 201–207. [Google Scholar] [CrossRef]
- Levy, D.; Kenchaiah, S.; Larson, M.G.; Benjamin, E.J.; Kupka, M.J.; Ho, K.K.L.; Murabito, J.M.; Vasan, R.S. Long-term trends in the incidence of and survival with heart failure. N. Engl. J. Med. 2002, 347, 1397–1402. [Google Scholar] [CrossRef]
- Moraska, A.R.; Chamberlain, A.M.; Shah, N.D.; Vickers, K.S.; Rummans, T.A.; Dunlay, S.M.; Spertus, J.A.; Weston, S.A.; McNallan, S.M.; Redfield, M.M.; et al. Depression, healthcare utilization, and death in heart failure: A community study. Circ. Heart Fail. 2013, 6, 387–394. [Google Scholar] [CrossRef]
- Gustad, L.T.; Bjerkeset, O.; Strand, L.B.; Janszky, I.; Salvesen, Ø.; Dalen, H. Cardiac function associated with previous, current and repeated depression and anxiety symptoms in a healthy population: The HUNT study. Open Heart 2016, 3, e000363. [Google Scholar] [CrossRef]
- Dessotte, C.A.M.; Silva, F.S.; Furuya, R.K.; Ciol, M.A.; Hoffman, J.M.; Dantas, R.A.S. Somatic and cognitive-affective depressive symptoms among patients with heart disease: Differences by sex and age. Rev. Lat. Am. Enferm. 2015, 23, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R.; Gan, D.R.Y.; Wister, A.V.; Cosco, T.D. Age and sex trends in depressive symptoms across middle and older adulthood: Comparison of the Canadian Longitudinal Study on Aging to American and European cohorts. J. Affect. Disord. 2021, 295, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Girgus, J.S.; Yang, K.; Ferri, C.V. The Gender Difference in Depression: Are Elderly Women at Greater Risk for Depression Than Elderly Men? Geriatrics 2017, 2, 35. [Google Scholar] [CrossRef] [PubMed]
- Roest, A.M.; Zuidersma, M.; de Jonge, P. Myocardial infarction and generalised anxiety disorder: 10-year follow-up. Br. J. Psychiatry 2012, 200, 324–329. [Google Scholar] [CrossRef]
- Celano, C.M.; Millstein, R.A.; Bedoya, C.A.; Healy, B.C.; Roest, A.M.; Huffman, J.C. Association between anxiety and mortality in patients with coronary artery disease: A meta-analysis. Am. Heart J. 2015, 170, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, E.; Thomas, S.A.; Liu, F.; Morton, P.G.; Chapa, D.; Gottlieb, S.S. Sudden Cardiac Death in Heart Failure Trial Investigators Relationship of depression, anxiety, and social isolation to chronic heart failure outpatient mortality. Am. Heart J. 2006, 152, 940.e1–940.e8. [Google Scholar] [CrossRef] [PubMed]
- Pelle, A.J.; Pedersen, S.S.; Schiffer, A.A.; Szabó, B.; Widdershoven, J.W.; Denollet, J. Psychological distress and mortality in systolic heart failure. Circ. Heart Fail. 2010, 3, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.S.; Foraker, R.E.; Girton, R.A.; Mansfield, A.J. Posttraumatic stress disorder and incident heart failure among a community-based sample of US veterans. Am. J. Public Health 2015, 105, 757–763. [Google Scholar] [CrossRef]
- Tsuchihashi-Makaya, M.; Kato, N.; Chishaki, A.; Takeshita, A.; Tsutsui, H. Anxiety and poor social support are independently associated with adverse outcomes in patients with mild heart failure. Circ. J. 2009, 73, 280–287. [Google Scholar] [CrossRef]
- Schlauch, R.W.; Reich, P.; Kelly, M.J. Leaving the hospital against medical advice. N. Engl. J. Med. 1979, 300, 22–24. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Arnott, C.; Beale, A.L.; Chandramouli, C.; Hilfiker-Kleiner, D.; Kaye, D.M.; Ky, B.; Santema, B.T.; Sliwa, K.; Voors, A.A. Sex differences in heart failure. Eur. Heart J. 2019, 40, 3859–3868c. [Google Scholar] [CrossRef] [PubMed]
- Köhler-Forsberg, O.; Buttenschøn, H.N.; Tansey, K.E.; Maier, W.; Hauser, J.; Dernovsek, M.Z.; Henigsberg, N.; Souery, D.; Farmer, A.; Rietschel, M.; et al. Association between C-reactive protein (CRP) with depression symptom severity and specific depressive symptoms in major depression. Brain Behav. Immun. 2017, 62, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Birur, B.; Amrock, E.M.; Shelton, R.C.; Li, L. Sex Differences in the Peripheral Immune System in Patients with Depression. Front. Psychiatry 2017, 8, 108. [Google Scholar] [CrossRef]
- Nymo, S.H.; Hulthe, J.; Ueland, T.; McMurray, J.; Wikstrand, J.; Askevold, E.T.; Yndestad, A.; Gullestad, L.; Aukrust, P. Inflammatory cytokines in chronic heart failure: Interleukin-8 is associated with adverse outcome. Results from CORONA. Eur. J. Heart Fail. 2014, 16, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Rodríguez, O.; Sheridan, S.C.; Lundevaller, E.H.; Schumann, B. Effect of extreme hot and cold weather on cause-specific hospitalizations in Sweden: A time series analysis. Environ. Res. 2021, 193, 110535. [Google Scholar] [CrossRef] [PubMed]
- Dib, P.; Zhang, Y.; Ihnat, M.A.; Gallucci, R.M.; Standifer, K.M. TNF-Alpha as an Initiator of Allodynia and Anxiety-Like Behaviors in a Preclinical Model of PTSD and Comorbid Pain. Front. Psychiatry 2021, 12, 721999. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Krishnan, R.; Kuchibhatla, M.; Cuffe, M.S.; Martsberger, C.; Arias, R.M.; O’Connor, C.M.; SADHART-CHF Investigators. Characteristics of depression remission and its relation with cardiovascular outcome among patients with chronic heart failure (from the SADHART-CHF Study). Am. J. Cardiol. 2011, 107, 545–551. [Google Scholar] [CrossRef]
- Pizzi, C.; Rutjes, A.W.; Costa, G.M.; Fontana, F.; Mezzetti, A.; Manzoli, L. Meta-analysis of selective serotonin reuptake inhibitors in patients with depression and coronary heart disease. Am. J. Cardiol. 2011, 107, 972–979. [Google Scholar] [CrossRef]
- Sherwood, A.; Blumenthal, J.A.; Trivedi, R.; Johnson, K.S.; O’Connor, C.M.; Adams, K.F.; Dupree, C.S.; Waugh, R.A.; Bensimhon, D.R.; Gaulden, L.; et al. Relationship of depression to death or hospitalization in patients with heart failure. Arch. Intern. Med. 2007, 167, 367–373. [Google Scholar] [CrossRef]
- Fosbøl, E.L.; Gislason, G.H.; Poulsen, H.E.; Hansen, M.L.; Folke, F.; Schramm, T.K.; Olesen, J.B.; Bretler, D.M.; Abildstrøm, S.Z.; Sørensen, R.; et al. Prognosis in heart failure and the value of {beta}-blockers are altered by the use of antidepressants and depend on the type of antidepressants used. Circ. Heart Fail. 2009, 2, 582–590. [Google Scholar] [CrossRef]
- Zwas, D.R.; Keren, A.; Amir, O.; Gotsman, I. Treatment of Heart Failure Patients with Anxiolytics Is Associated with Adverse Outcomes, with and without Depression. J. Clin. Med. 2020, 9, 3967. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, R.D.; Dierker, L.C.; Wu, M.; Galea, S.; Hoven, C.W.; Weinberger, A.H. Trends in U.S. Depression Prevalence From 2015 to 2020: The Widening Treatment Gap. Am. J. Prev. Med. 2022, 63, 726–733. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Females [6,394,136 (56.6%)] | Females [6,394,136 (56.6%)] | |||||
|---|---|---|---|---|---|---|
| No Depression [5,388,939 (84.3%)] | Had Depression [1,005,197 (15.7%)] | p-Value | No Anxiety [5,320,276 (83.2%)] | Had Anxiety [1,073,860 (16.8%)] | p-Value | |
| Age, years [median (IQR)] | 58 (33–74) | 62 (45–74) | <0.001 | 58 (33–75) | 60 (42–73) | <0.001 |
| Age Category (years) | <0.001 | <0.001 | ||||
| 18–34 | 1,434,356 (27.0) | 177,936 (16.6) | 1,434,356 (27.0) | 177,936 (16.6) | ||
| 35–44 | 558,661 (10.5) | 117,582 (11.0) | 558,661 (10.5) | 117,582 (10.9) | ||
| 45–54 | 439,208 (8.3) | 139,414 (13.0) | 439,208 (8.3) | 139,414 (13.0) | ||
| 55–64 | 690,721 (13.0) | 199,489 (18.6) | 690,721 (13.0) | 199,489 (18.6) | ||
| 65–74 | 864,243 (16.2) | 205,548 (19.1) | 864,243 (16.2) | 205,548 (19.1) | ||
| 75–84 | 778,950 (14.6) | 150,305 (14.0) | 778,950 (14.6) | 150,305 (14.0) | ||
| >84 | 554,137 (10.4) | 83,586 (7.8) | 554,137 (10.4) | 83,586 (7.8) | ||
| RACE | <0.001 | <0.001 | ||||
| White | 3,379,569 (62.7) | 772,621 (76.9) | 3,305,850 (62.1) | 846,340 (78.8) | ||
| Black | 904,606 (16.8) | 114,813 (11.4) | 911,207 (17.1) | 108,212 (10.1) | ||
| Hispanic | 704,218 (13.1) | 77,485 (7.7) | 703,214 (13.2) | 78,489 (7.3) | ||
| Asian or Pacific Islander | 190,684 (3.5) | 11,865 (1.2) | 190,893 (3.6) | 11,656 (1.1) | ||
| Native American | 38,432 (0.7) | 7059 (0.7) | 38,946 (0.7) | 6545 (0.6) | ||
| Other | 171,430 (3.2) | 21,354 (2.1) | 170,166 (3.2) | 22,618 (2.1) | ||
| ADMISSION TYPE | <0.001 | <0.001 | ||||
| Non-elective | 3,981,484 (74.0) | 804,523 (80.1) | 3,931,609 (74.0) | 854,398 (79.6) | ||
| Elective | 1,401,308 (26.0) | 199,589 (19.9) | 1,382,557 (26.0) | 218,340 (20.4) | ||
| HOSPITAL REGION | <0.001 | <0.001 | ||||
| Northeast | 975,705 (18.1) | 185,338 (18.4) | 953,939 (17.9) | 207,104 (19.3) | ||
| Midwest | 1,111,782 (20.6) | 261,775 (26.0) | 1,096,589 (20.6) | 276,968 (25.8) | ||
| South | 2,221,005 (41.2) | 387,300 (38.5) | 2,183,130 (41.0) | 425,175 (39.6) | ||
| West | 1,080,447 (20.1) | 170,784 (17.0) | 1,086,618 (20.4) | 164,613 (15.3) | ||
| HOSPITAL TEACHING STATUS | <0.001 | <0.001 | ||||
| Rural | 471,112 (8.7) | 93,233 (9.3) | 462,512 (8.7) | 101,833 (9.5) | ||
| Urban, non-teaching | 991,235 (18.4) | 179,933 (17.9) | 971,702 (18.3) | 199,466 (18.6) | ||
| Urban, teaching | 3,926,592 (72.9) | 732,031 (72.8) | 3,886,062 (73.0) | 772,561 (71.9) | ||
| HOSPITAL BED SIZE | <0.001 | <0.001 | ||||
| Small | 1,208,930 (22.4) | 228,944 (22.8) | 1,190,008 (22.4) | 247,866 (23.1) | ||
| Medium | 1,561,732 (29.0) | 285,360 (28.4) | 1,538,962 (28.9) | 308,130 (28.7) | ||
| Large | 2,618,277 (48.6) | 490,893 (48.8) | 2,591,306 (48.7) | 517,864 (48.2) | ||
| PAYER TYPE | <0.001 | <0.001 | ||||
| Medicare | 2,321,932 (43.1) | 529,841 (52.8) | 2,318,538 (43.6) | 533,235 (49.7) | ||
| Medicaid | 1,141,455 (21.2) | 181,767 (18.1) | 1,121,433 (21.1) | 201,789 (18.8) | ||
| Private Insurance | 1,606,098 (29.8) | 240,672 (24.0) | 1,566,912 (29.5) | 279,858 (26.1) | ||
| Self-pay | 185,493 (3.4) | 28,913 (2.9) | 182,091 (3.4) | 32,315 (3.0) | ||
| No Charge | 13,734 (0.3) | 2337 (0.2) | 13,375 (0.2) | 2696 (0.2) | ||
| Other | 114,621 (2.1) | 20,626 (2.0) | 112,380 (2.1) | 22,867 (2.1) | ||
| MEDIAN HOUSEHOLD INCOME | <0.001 | <0.001 | ||||
| 0–25th percentile | 1,624,419 (30.6) | 293,420 (29.6) | 1,608,211 (30.6) | 309,628 (29.2) | ||
| 26–50th percentile | 1,378,154 (25.9) | 268,425 (27.1) | 1,359,903 (25.9) | 286,676 (27.1) | ||
| 51st–75th percentile | 1,256,270 (23.6) | 241,350 (24.3) | 1,240,376 (23.6) | 257,244 (24.3) | ||
| 76–100th percentile | 1,055,985 (19.9) | 187,889 (19.0) | 1,038,966 (19.8) | 204,908 (19.4) | ||
| Disposition | <0.001 | <0.001 | ||||
| Home, self-care | 3,583,700 (66.5) | 579,843 (57.7) | 3,514,904 (66.1) | 648,639 (60.4) | ||
| Short term hospital | 85,770 (1.6) | 17,532 (1.7) | 84,712 (1.6) | 18,590 (1.7) | ||
| Skilled Nursing Facility | 758,434 (14.1) | 200,273 (19.9) | 773,911 (14.5) | 184,796 (17.2) | ||
| Home Healthcare | 772,904 (14.3) | 177,161 (17.6) | 765,361 (14.4) | 184,704 (17.2) | ||
| Against Medical Advice | 63,524 (1.2) | 13,973 (1.4) | 59,049 (1.1) | 18,448 (1.7) | ||
| Died | 123,557 (2.3) | 16,335 (1.6) | 121,372 (2.3) | 18,520 (1.7) | ||
| Comorbid Conditions | ||||||
| Alcohol abuse | 123,180 (2.3) | 60,480 (6.0) | <0.001 | 122,985 (2.3) | 60,675 (5.6) | <0.001 |
| Chronic pulmonary disease | 1,043,437 (19.4) | 299,148 (29.8) | <0.001 | 1,013,514 (19.0) | 329,071 (30.6) | <0.001 |
| Diabetes | 1,288,256 (23.9) | 286,539 (28.5) | <0.001 | 1,308,977 (24.6) | 265,818 (24.7) | 0.27 |
| Drug abuse | 198,811 (3.7) | 76,090 (7.6) | <0.001 | 186,445 (3.5) | 88,456 (8.2) | <0.001 |
| HIV/AIDS | 18,661 (0.4) | 4404 (0.4) | 0.29 | 19,180 (0.4) | 3885 (0.4) | 1 |
| Hypertension | 2,475,902 (45.9) | 583,291 (58.0) | <0.001 | 2,462,571 (46.3) | 596,622 (55.6) | <0.001 |
| Liver Disease | 170,084 (3.2) | 47,371 (4.7) | <0.001 | 166,632 (3.1) | 50,823 (4.7) | <0.001 |
| Leukemia | 28,022 (0.5) | 5912 (0.6) | 0.37 | 27,603 (0.5) | 6331 (0.6) | 0.32 |
| Lymphoma | 40,090 (0.7) | 7912 (0.8) | 0.64 | 39,626 (0.7) | 8376 (0.8) | 0.72 |
| Metastatic Cancer | 153,648 (2.9) | 26,982 (2.7) | 0.002 | 146,876 (2.8) | 33,754 (3.1) | <0.001 |
| Obesity | 1,012,895 (18.8) | 248,753 (24.7) | <0.001 | 1,010,840 (19.0) | 250,808 (23.4) | <0.001 |
| Peripheral vascular disease | 273,137 (5.1) | 61,054 (6.1) | <0.001 | 272,413 (5.1) | 61,778 (5.7) | <0.001 |
| Renal failure | 790,839 (14.7) | 169,589 (16.9) | <0.001 | 805,266 (15.1) | 155,162 (14.4) | <0.001 |
| Rheumatoid diseases | 188,387 (3.5) | 51,875 (5.2) | <0.001 | 188,948 (3.5) | 51,314 (4.8) | <0.001 |
| Solid tumor, no metastasis | 124,028 (2.3) | 25,017 (2.5) | <0.001 | 121,119 (2.3) | 27,926 (2.6) | <0.001 |
| Smoking | 1,340,089 (24.9) | 369,799 (36.8) | <0.001 | 1,296,001 (24.4) | 413,887 (38.5) | <0.001 |
| Pregnancy | 1,345,273 (25.0) | 66,289 (6.6) | <0.001 | 1,326,307 (24.9) | 85,255 (7.9) | <0.001 |
| Charlson Comorbidity Index | <0.001 | <0.001 | ||||
| 0 | 2,318,099 (43.0) | 297,338 (29.6) | 2,279,355 (42.8) | 336,082 (31.3) | ||
| 1 | 973,464 (18.1) | 222,911 (22.2) | 947,080 (17.8) | 249,295 (23.2) | ||
| ≥2 | 2,097,376 (38.9) | 484,948 (48.2) | 2,093,841 (39.4) | 488,483 (45.5) | ||
| Females [6,394,136 (56.6%)] | Males [4,898,702 (43.4%)] | |||||
|---|---|---|---|---|---|---|
| Outcomes | No Depression 5,388,939 (84.3%) | Had Depression 1,005,197 (15.7%) | p-Value | No Depression 4,300,724 (87.8%) | Had Depression 597,978 (12.2%) | p-Value |
| Acute HF | 356,739 (6.6) | 66,363 (6.6) | 0.51 | 418,888 (9.7) | 43,629 (7.3) | <0.001 |
| Takotsubo cardiomyopathy | 10,395 (0.2) | 2783 (0.3) | 0.03 | 2656 (0.1) | 389 (0.1) | 0.34 |
| Length of stay, days [MD (IQR)] | 3 (2–5) | 3 (2–6) | <0.001 | 3 (2–6) | 4 (2–7) | <0.001 |
| Cost of care, US Dollars [MD (IQR)] | 7944 (4668–14,553) | 9003 (5216–16,034) | <0.001 | 10,552 (5923–19,582) | 9025 (4986–17,049) | <0.001 |
| Outcomes | No Anxiety 5,320,276 (83.2%) | Had Anxiety 1,073,860 (16.8%) | p-Value | No Anxiety 4,329,053 (88.4%) | Had Anxiety 569,649 (11.6%) | p-Value |
| Acute HF | 353,308 (6.6) | 69,794 (6.5) | 0.32 | 421,119 (9.7) | 41,398 (7.3) | <0.001 |
| Takotsubo cardiomyopathy | 9823 (0.2) | 3355 (0.3) | 0.02 | 2649 (0.1) | 396 (0.1) | 0.52 |
| Length of stay, days [MD (IQR)] | 3 (2–6) | 3 (2–5) | <0.001 | 3 (2–6) | 4 (2–7) | <0.001 |
| Cost of care, US Dollars [MD (IQR)] | 8914 (5229–15,880) | 7945 (4657–14,568) | <0.001 | 10,552 (5923–19,582) | 9202 (5108–17,470) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antwi-Amoabeng, D.; Neelam, V.; Ulanja, M.B.; Beutler, B.D.; Gbadebo, T.D.; Sugathan, P. Association between Psychiatric Disorders and the Incidence of Heart Failure in Women. J. Cardiovasc. Dev. Dis. 2023, 10, 491. https://doi.org/10.3390/jcdd10120491
Antwi-Amoabeng D, Neelam V, Ulanja MB, Beutler BD, Gbadebo TD, Sugathan P. Association between Psychiatric Disorders and the Incidence of Heart Failure in Women. Journal of Cardiovascular Development and Disease. 2023; 10(12):491. https://doi.org/10.3390/jcdd10120491
Chicago/Turabian StyleAntwi-Amoabeng, Daniel, Vijay Neelam, Mark Bilinyi Ulanja, Bryce David Beutler, Tokunbo David Gbadebo, and Prasanna Sugathan. 2023. "Association between Psychiatric Disorders and the Incidence of Heart Failure in Women" Journal of Cardiovascular Development and Disease 10, no. 12: 491. https://doi.org/10.3390/jcdd10120491
APA StyleAntwi-Amoabeng, D., Neelam, V., Ulanja, M. B., Beutler, B. D., Gbadebo, T. D., & Sugathan, P. (2023). Association between Psychiatric Disorders and the Incidence of Heart Failure in Women. Journal of Cardiovascular Development and Disease, 10(12), 491. https://doi.org/10.3390/jcdd10120491